
Rehabilitation of Worn Dentition with Direct Resin Composite Restorations: A Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
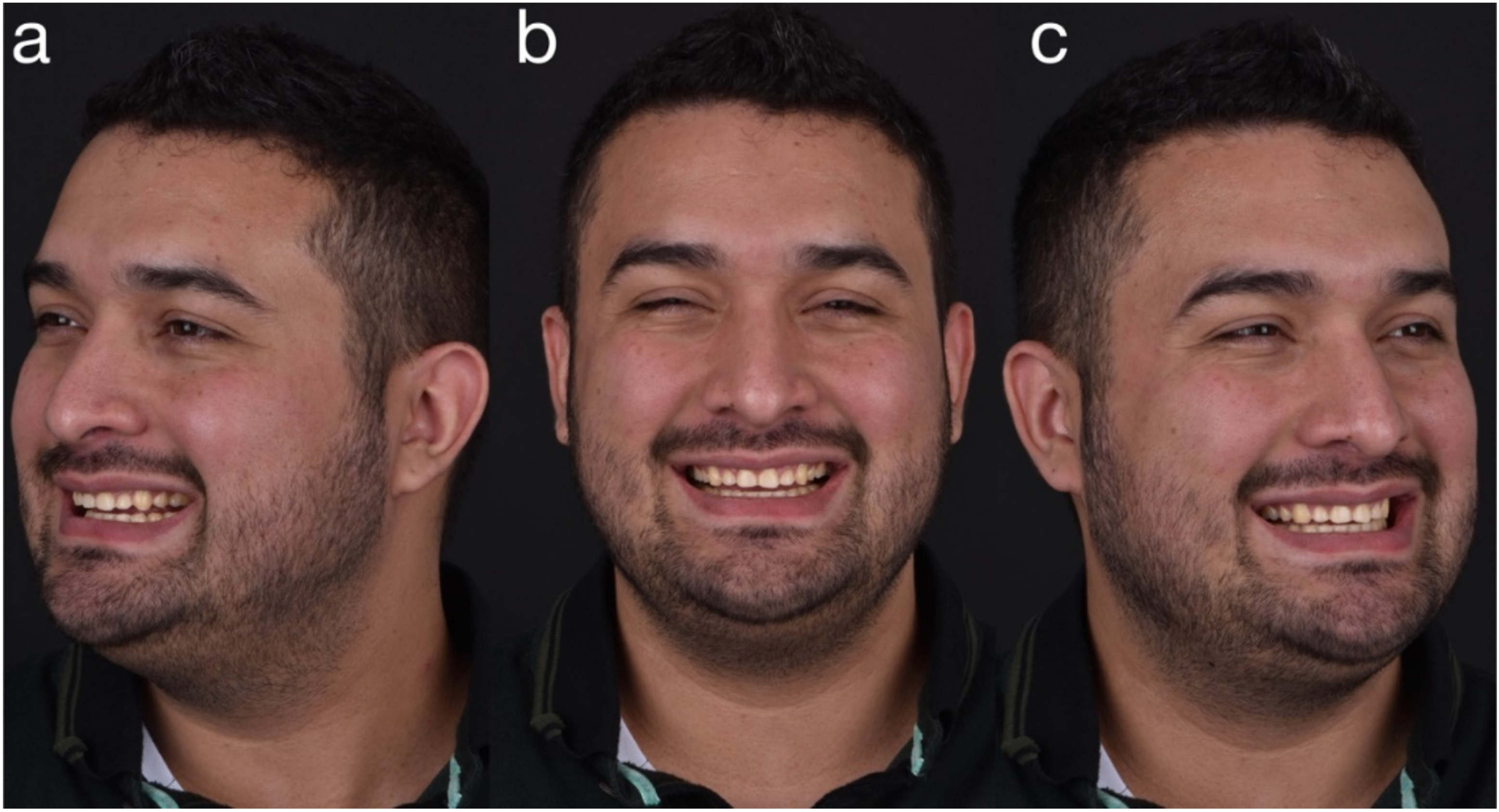
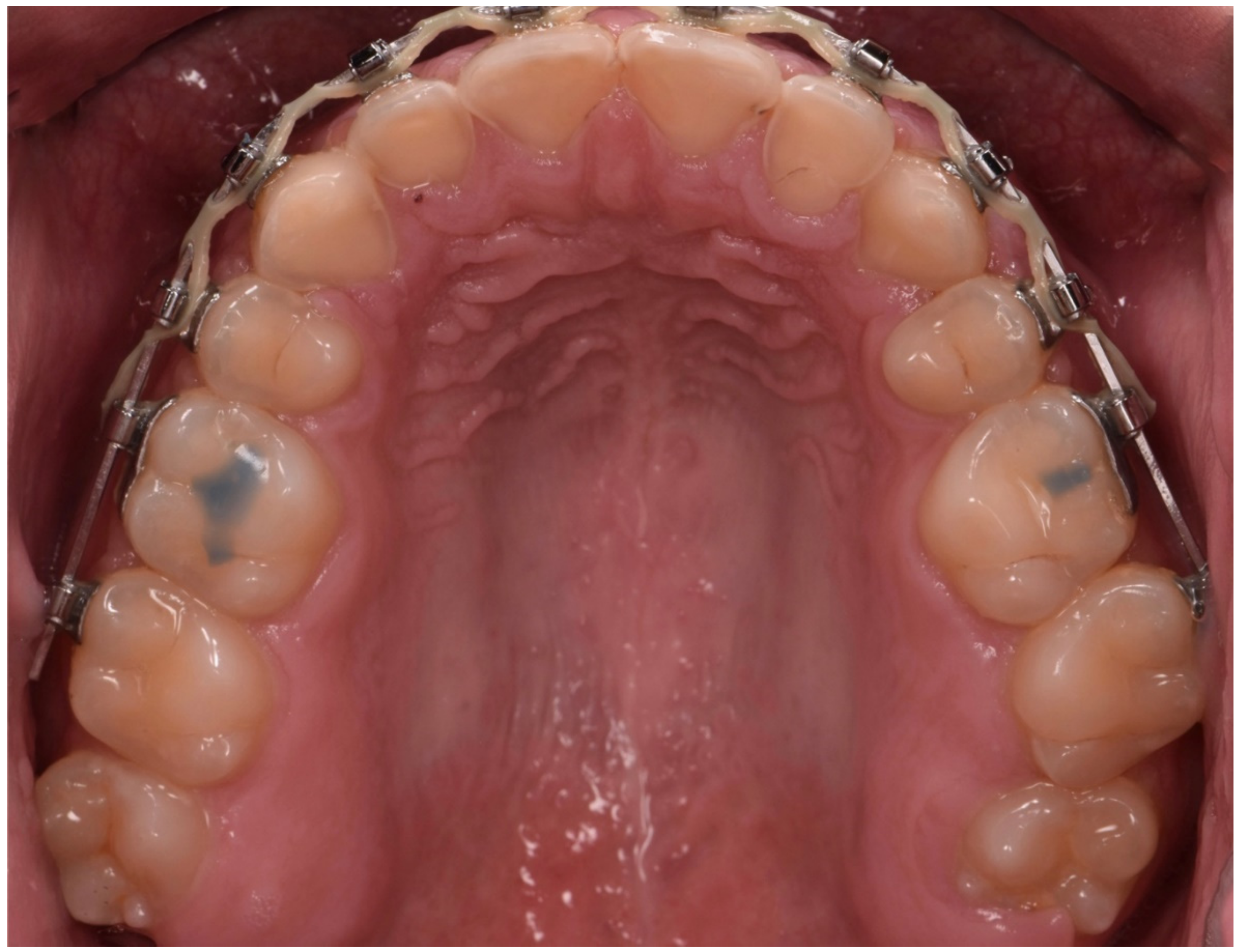
2. Clinical Report
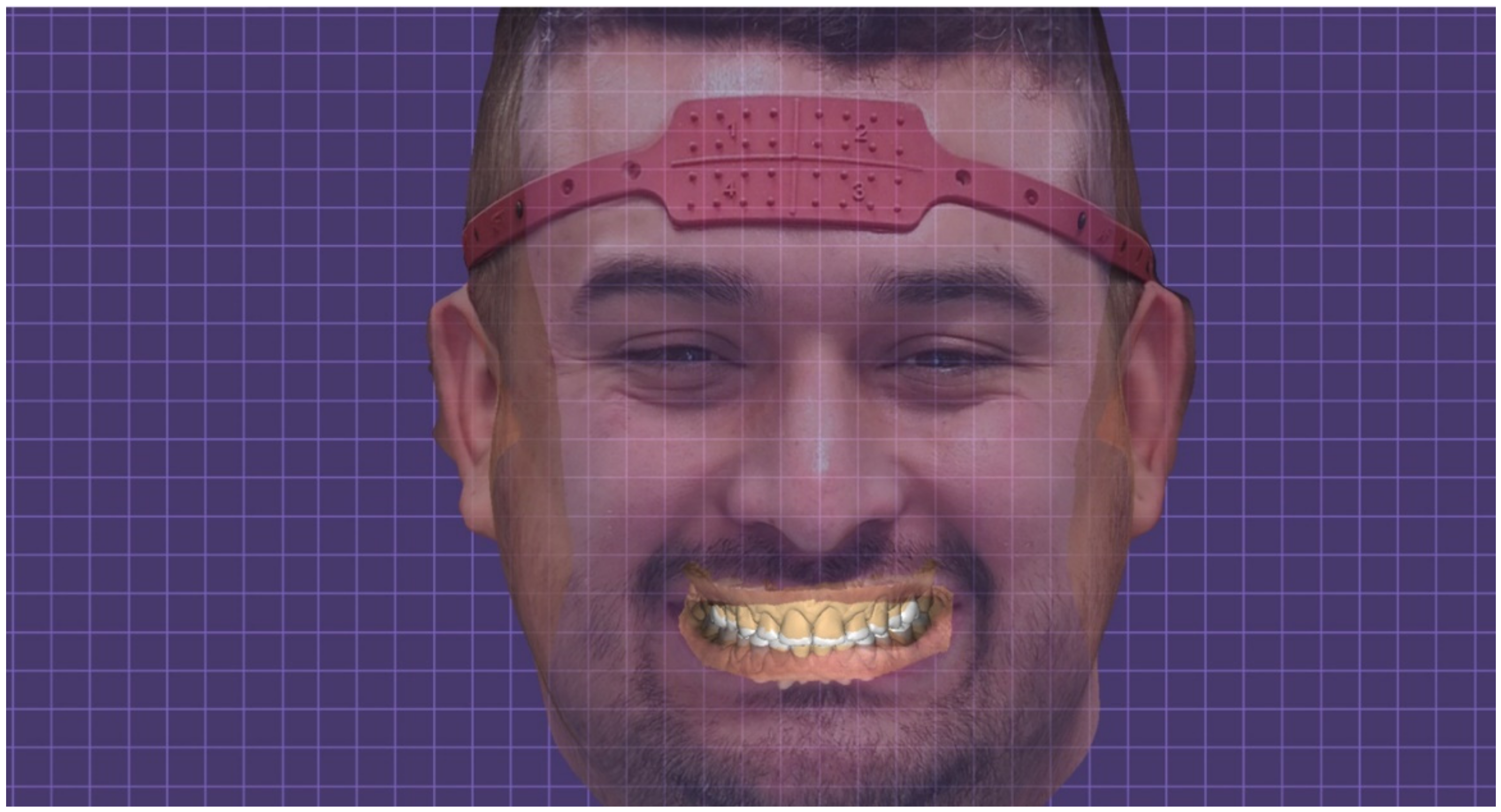
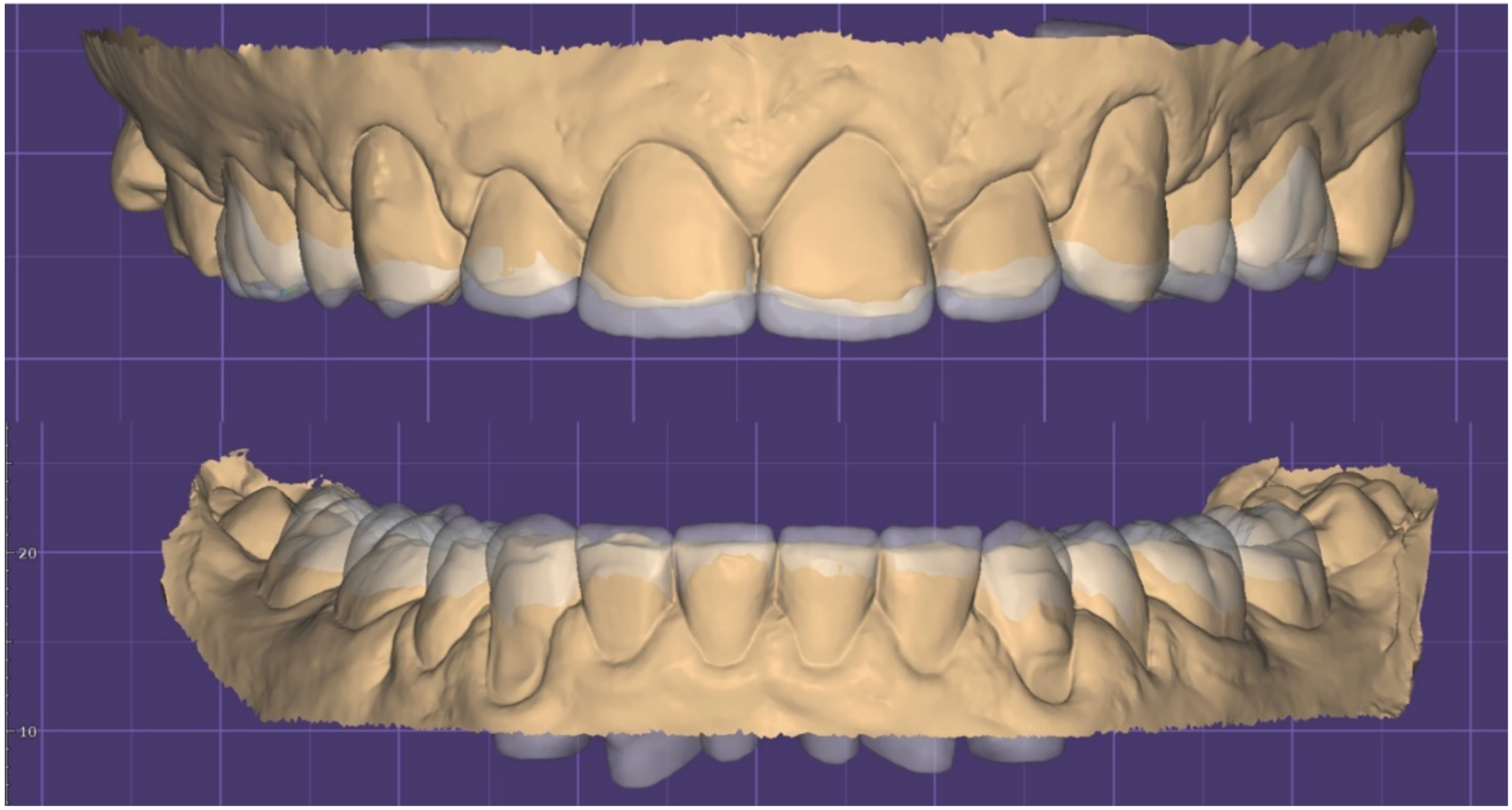
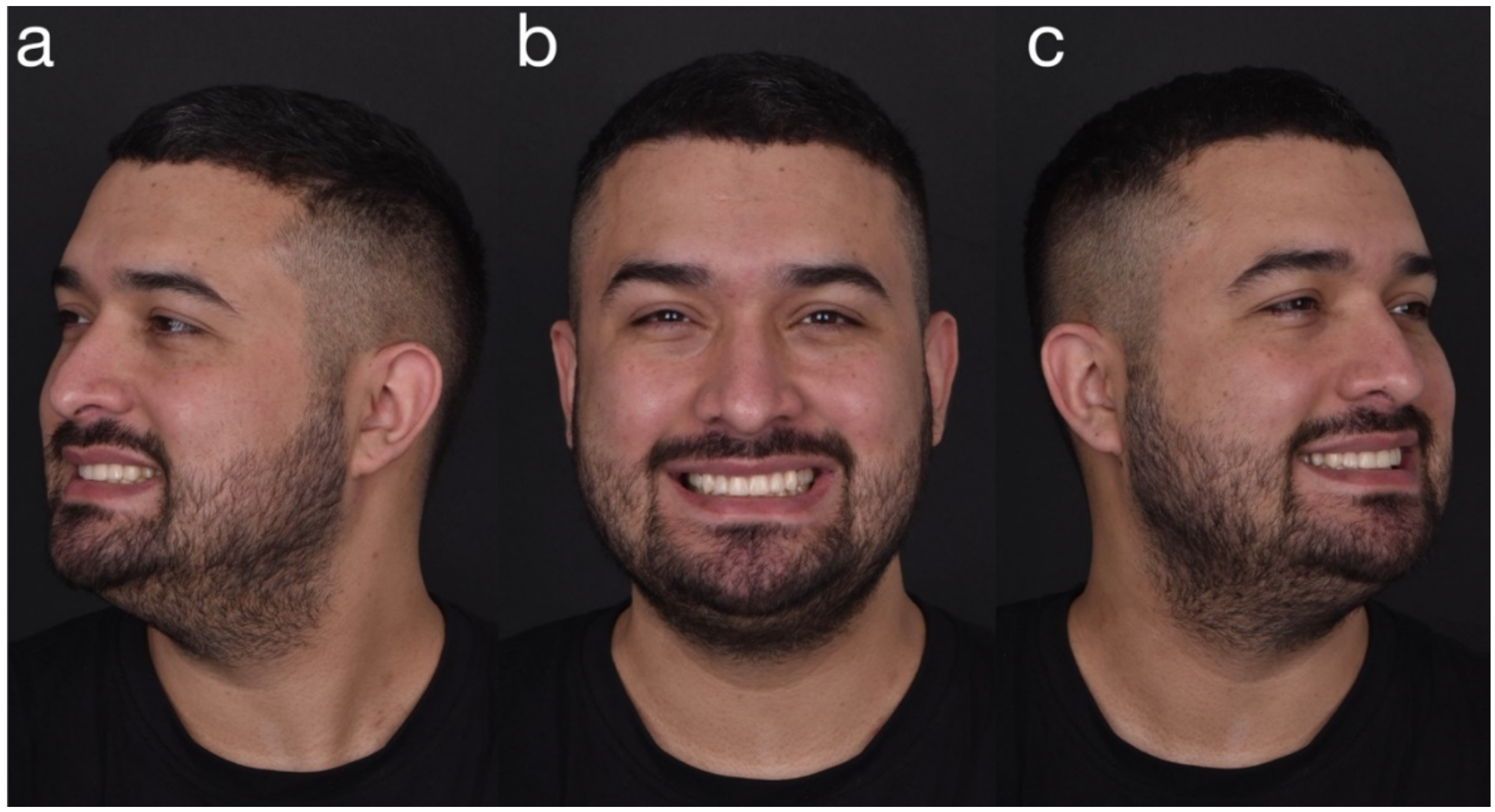
2.1. Planning Phase
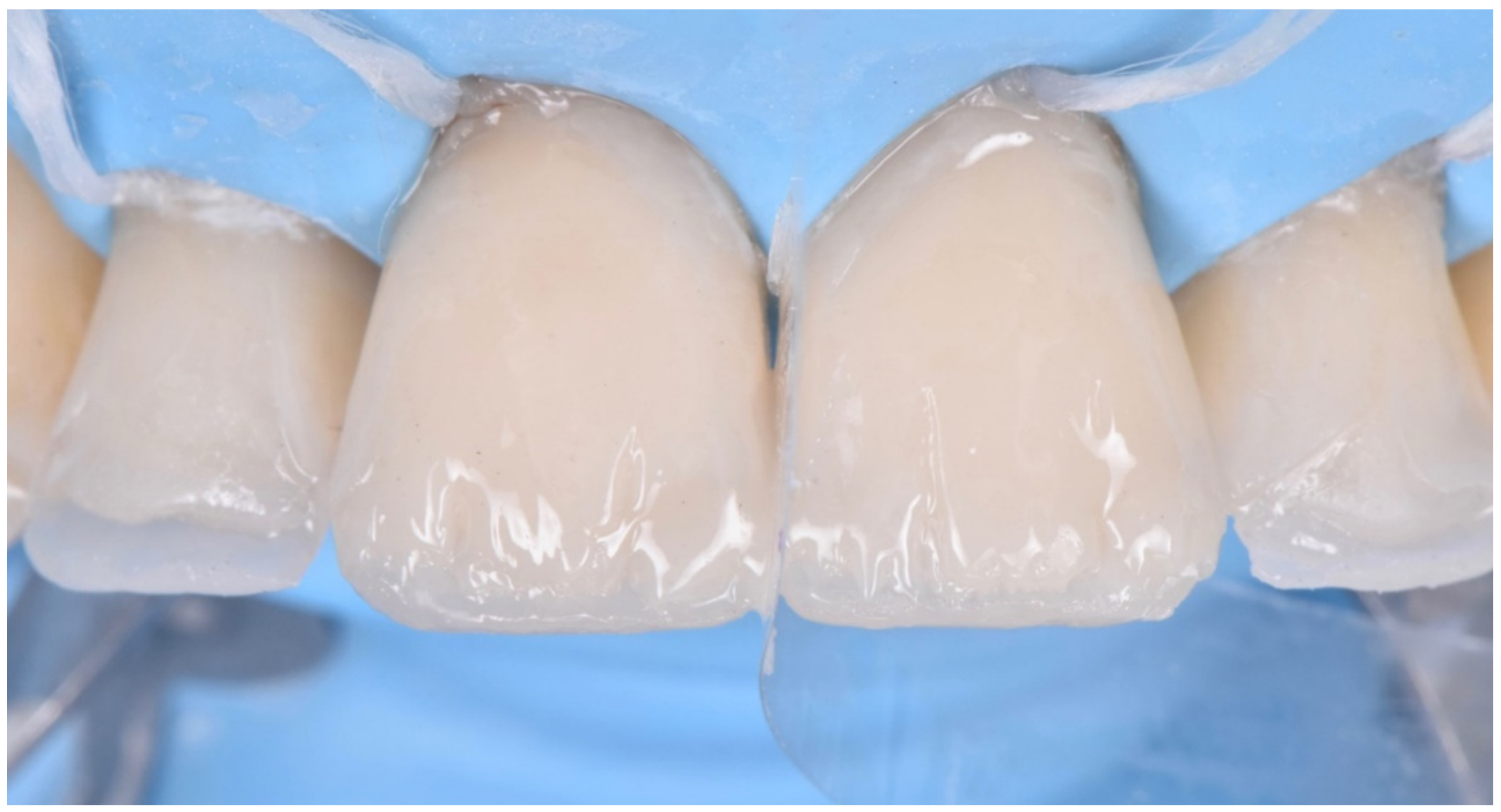
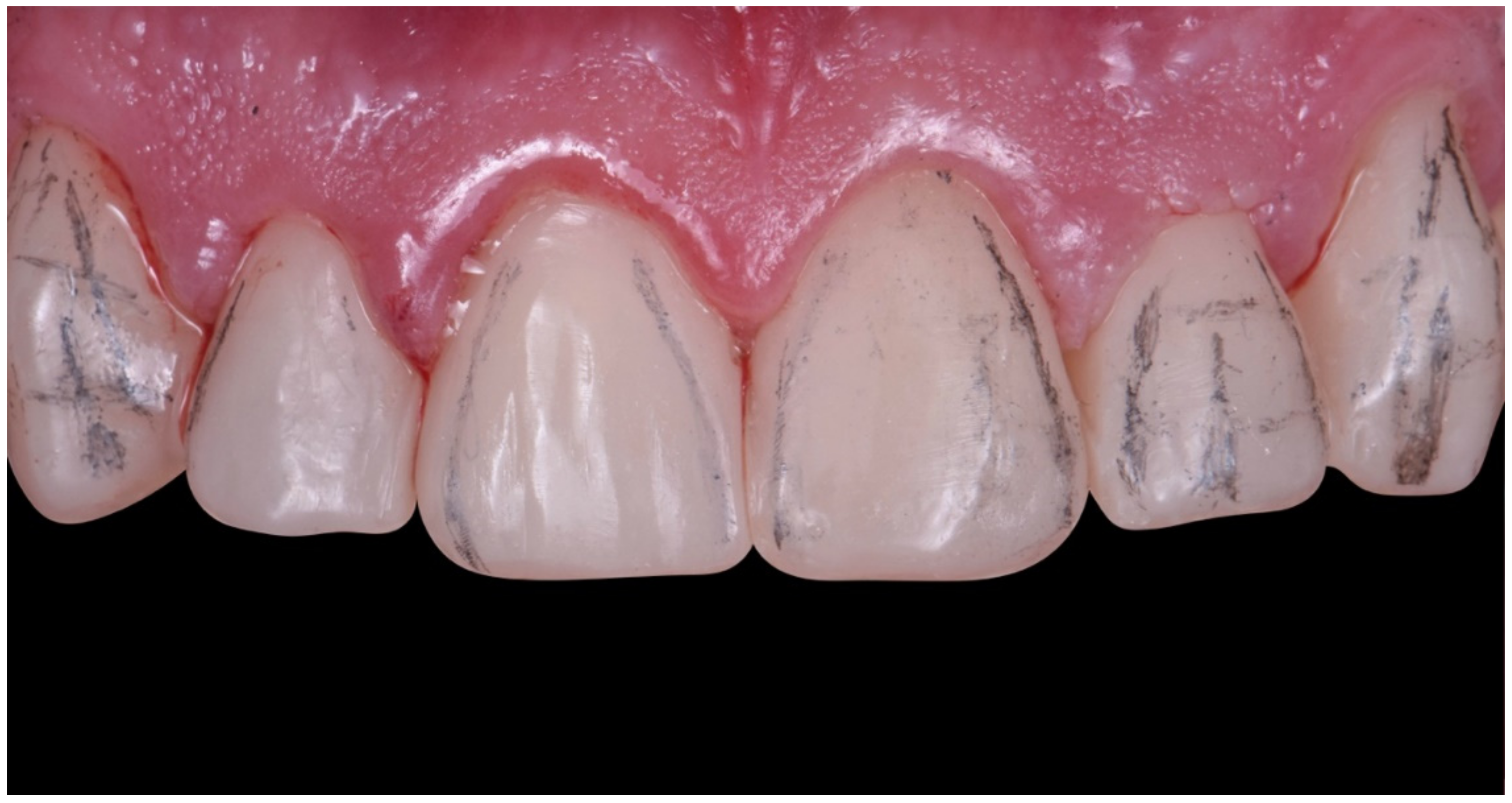
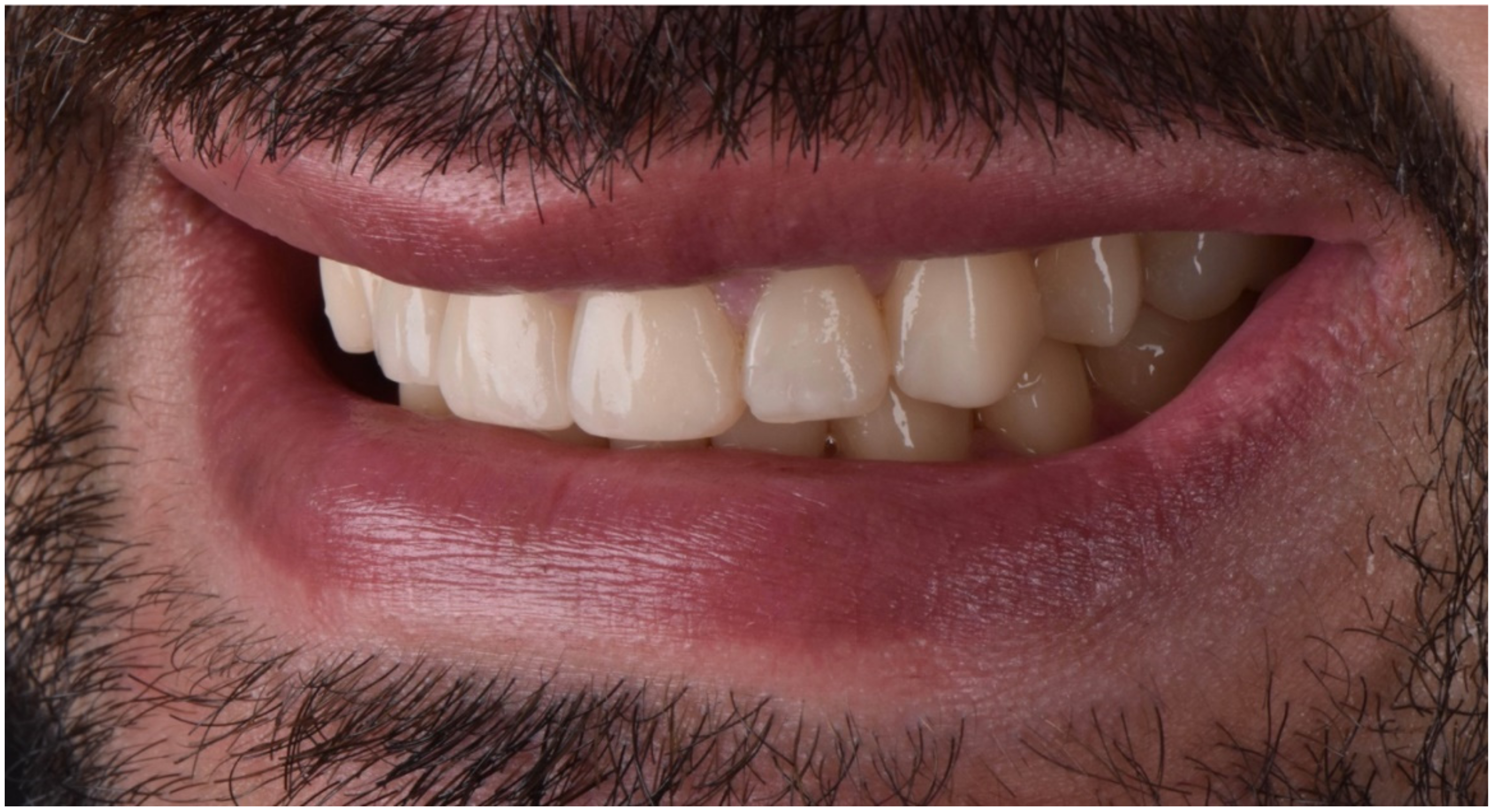
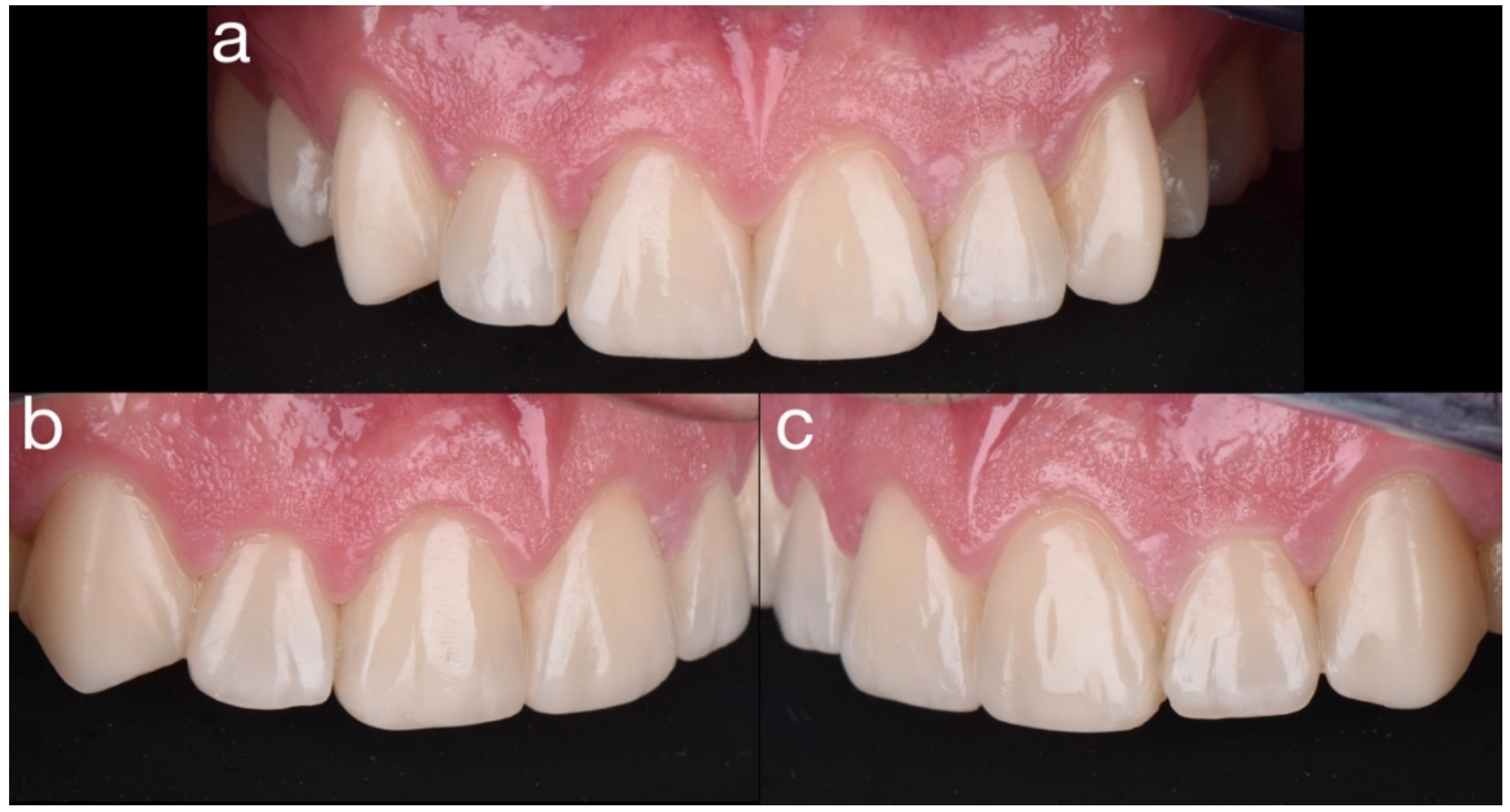
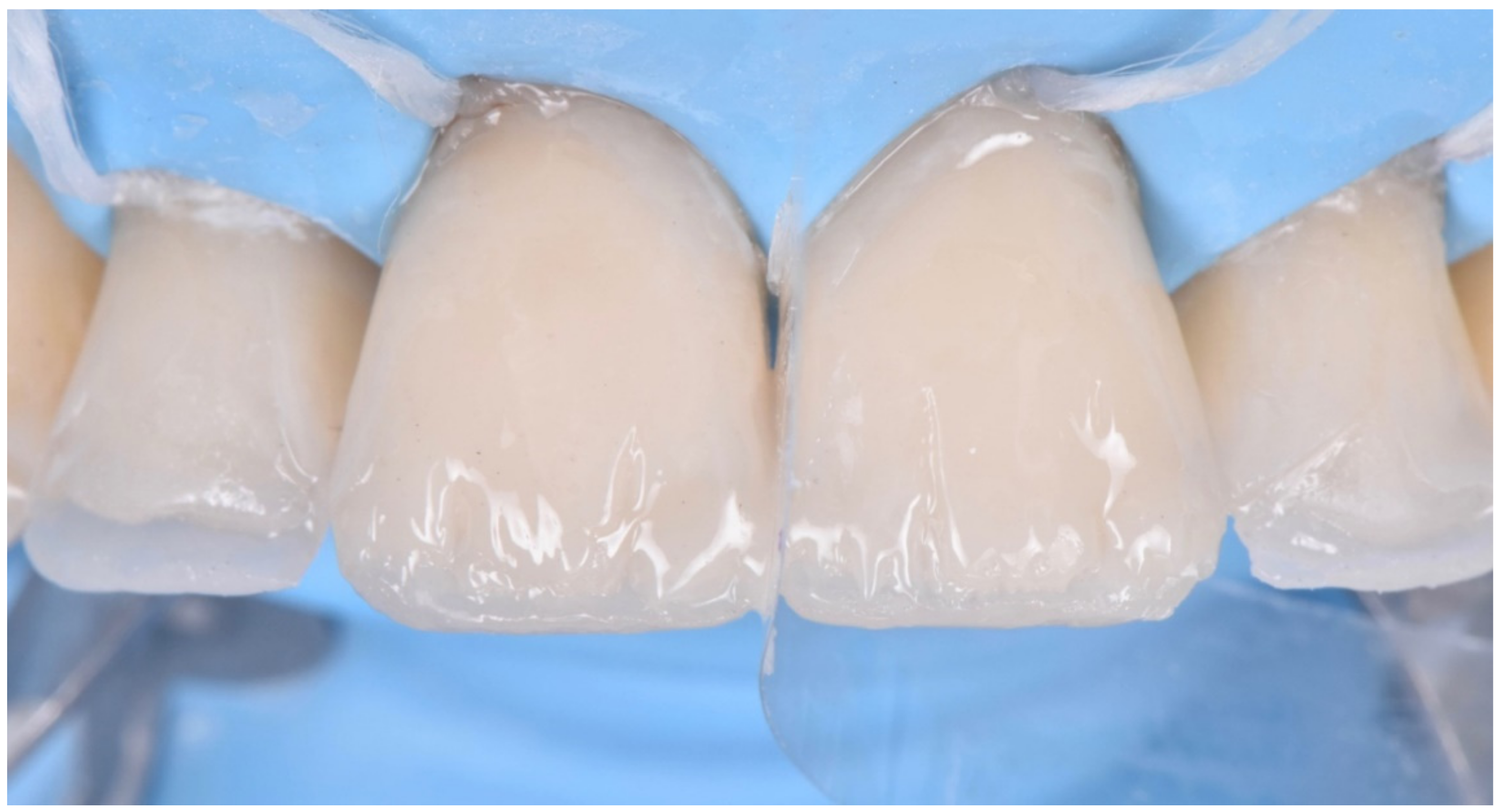
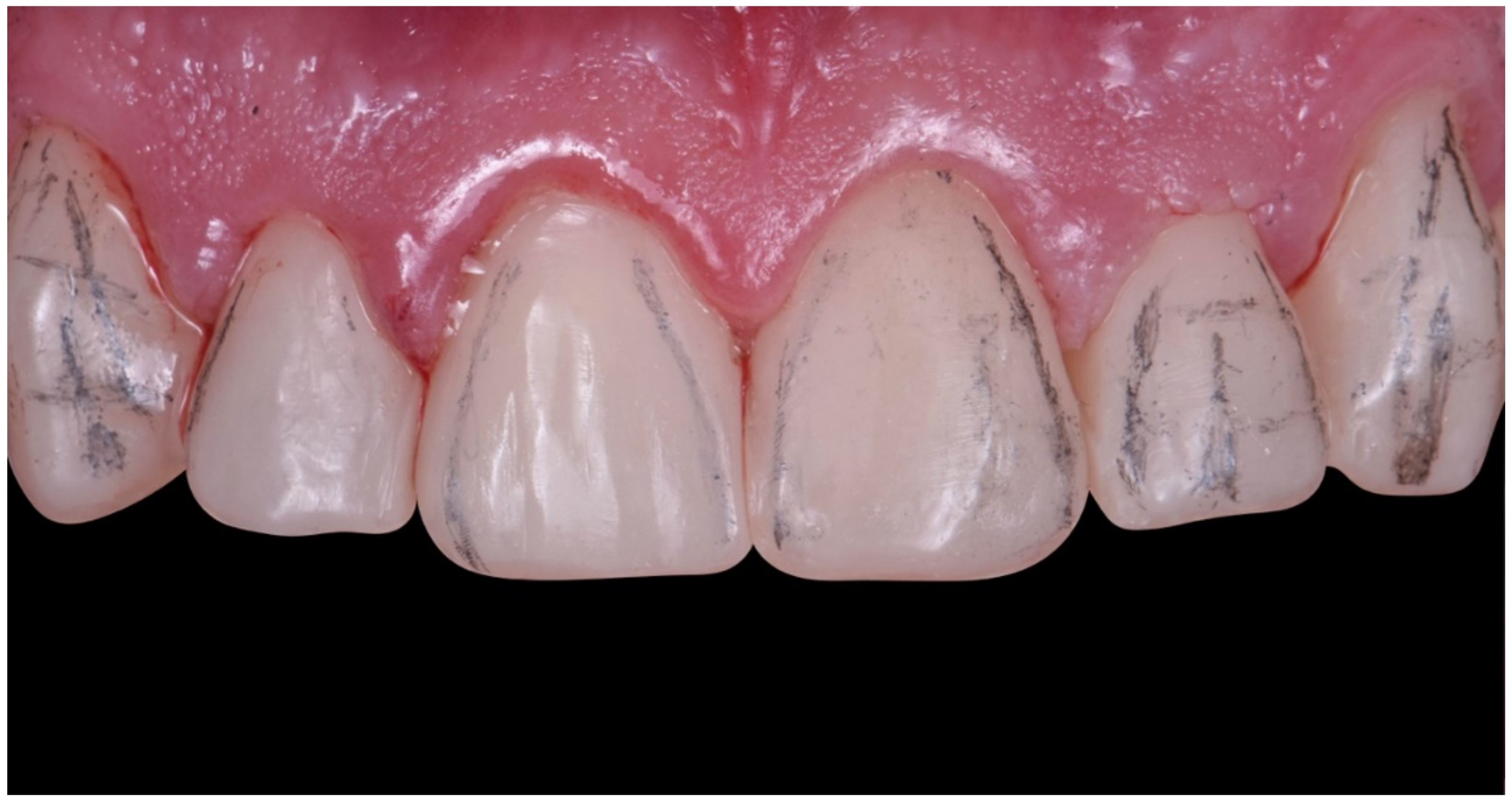
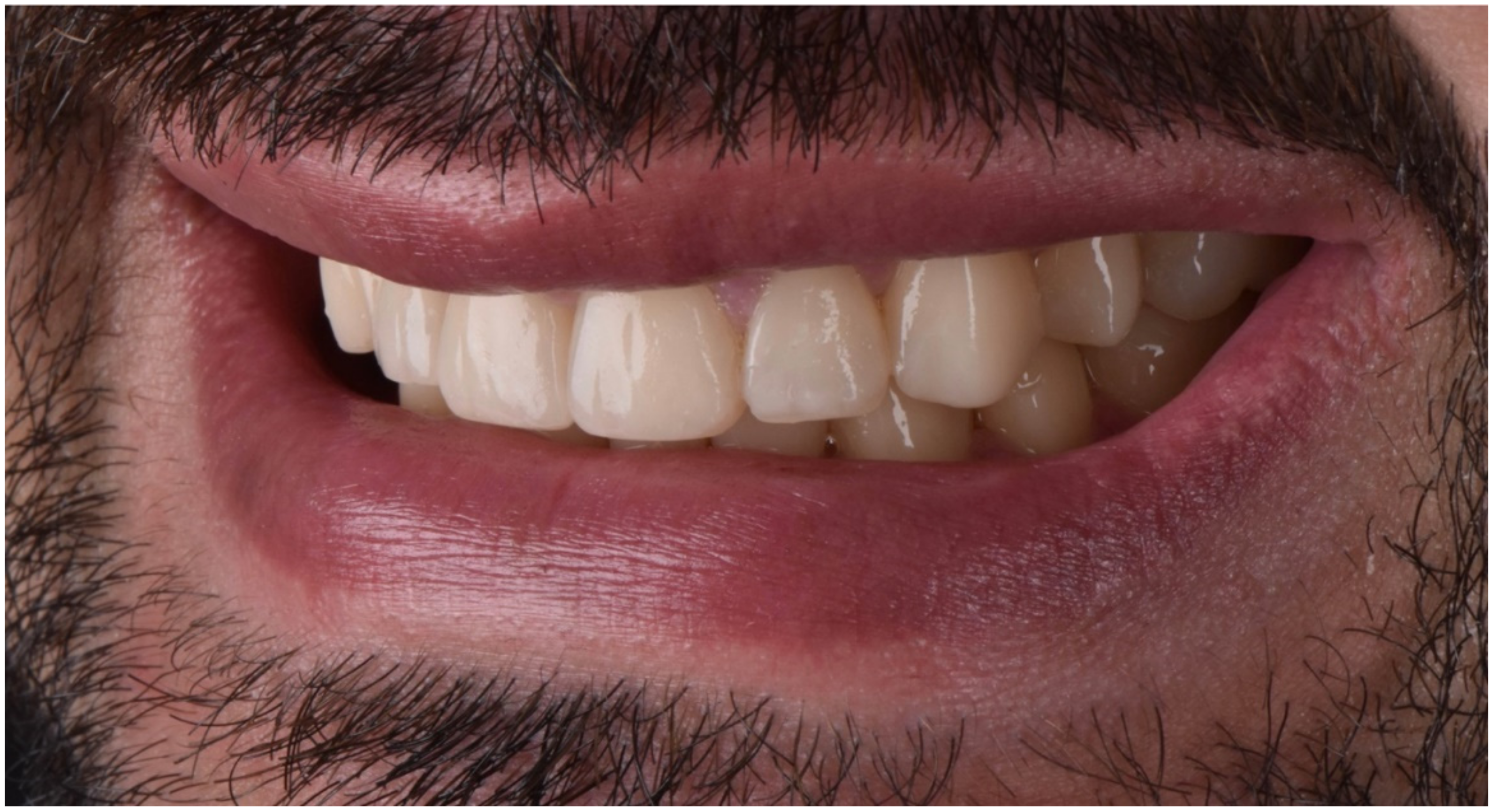
2.2. Restorative Phase
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Almeida e Silva, J.S.; Baratieri, L.N.; Araujo, E.; Widmer, N. Dental erosion: Understanding this pervasive condition. J. Esthet. Restor. Dent. 2011, 23, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.; O’Toole, S. Tooth wear and aging. Aust. Dent. J. 2019, 64, S59–S62. [Google Scholar] [CrossRef] [PubMed]
- Loomans, B.; Opdam, N.; Attin, T.; Bartlett, D.; Edelhoff, D.; Frankenberger, R.; Benic, G.; Ramseyer, S.; Wetselaar, P.; Sterenborg, B.; et al. Severe tooth wear: European consensus statement on management guidelines. J. Adhes. Dent. 2017, 19, 111–119. [Google Scholar] [PubMed]
- Lussi, A.; Ganss, C. (Eds.) Erosive Tooth Wear from Diagnosis to Therapy; Karger Medical and Scientific Publishers: Basel, Switzerland, 2014. [Google Scholar]
- Carvalho, T.S.; Lussi, A. Chapter 9: Acidic beverages and foods associated with dental erosion and erosive tooth wear. Monogr. Oral Sci. 2019, 28, 91–98. [Google Scholar]
- O’Toole, S.; Mullan, F. The role of the diet in tooth wear. Br. Dent. J. 2018, 224, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Mesko, M.E.; Sarkis-Onofre, R.; Cenci, M.; Opdam, N.J.; Loomans, B.; Pereira-Cenci, T. Rehabilitation of severely worn teeth: A systematic review. J. Dent. 2016, 48, 9–15. [Google Scholar] [CrossRef]
- Calamita, M.; Calamita, M.; Coachman, C.; Sesma, N.; Kois, J. Occlusal vertical dimension. IJED 2019, 14, 166–182. [Google Scholar]
- Muts, E.-J.; Van Pelt, H.; Edelhoff, D.; Krejci, I.; Cune, M. Tooth wear: A systematic review of treatment options. J. Prosthet. Dent. 2014, 112, 752–759. [Google Scholar] [CrossRef]
- Lee, H.; Fehmer, V.; Kwon, K.-R.; Burkhardt, F.; Pae, A.; Sailer, I. Virtual diagnostics and guided tooth preparation for the minimally invasive rehabilitation of a patient with extensive tooth wear: A validation of a digital workflow. J. Prosthet. Dent. 2020, 123, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Loomans, B.; Opdam, N. A guide to managing tooth wear: The Radboud philosophy. Br. Dent. J. 2018, 224, 348–356. [Google Scholar] [CrossRef]
- Van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Saratti, C.M.; Merheb, C.; Franchini, L.; Rocca, G.T.; Krejci, I. Full-mouth rehabilitation of a severe tooth wear case: A digital, esthetic and functional approach. Int. J. Esthet. Dent. 2020, 15, 242–262. [Google Scholar] [PubMed]
- Saratti, C.M.; Del Curto, F.; Rocca, G.T.; Krejci, I. Vertical dimension augmentation with a full digital approach: A multiple chairside sessions case report. Int. J. Comput. Dent. 2017, 20, 423–438. [Google Scholar] [PubMed]
- Del Curto, F.; Saratti, C.M.; Krejci, I. CAD/CAM-based chairside restorative technique with composite resin for full-mouth adhesive rehabilitation of excessively worn dentition. Int. J. Esthet. Dent. 2018, 13, 50–64. [Google Scholar]
- Wetselaar, P.; Wetselaar-Glas, M.J.; Katzer, L.D.; Ahlers, M.O.; Wetselaar-Glas, M.M. Diagnosing tooth wear, a new taxonomy based on the revised version of the Tooth Wear Evaluation System (TWES 2.0). J. Oral Rehabil. 2020, 47, 703–712. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Saratti, C.M.; Rocca, G.T.; Vaucher, P.; Awai, L.; Papini, A.; Zuber, S.; Di Bella, E.; Dietschi, D.; Krejci, I. Functional assessment of the stomatognathic system. Part 1: The role of static elements of analysis. Quintessence Int. 2021, 52, 920–932. [Google Scholar]
- Saratti, C.M.; Rocca, G.T.; Vaucher, P.; Awai, L.; Papini, A.; Zuber, S.; Di Bella, E.; Dietschi, D.; Krejci, I. Functional assessment of the stomatognathic system. Part 2: The role of dynamic elements of analysis. Quintessence Int. 2022, 53, 90–102. [Google Scholar]
- Bracco, P.; Deregibus, A.; Piscetta, R. Effects of different jaw relations on postural stability in human subjects. Neurosci. Lett. 2004, 356, 228–230. [Google Scholar] [CrossRef]
- Dietschi, D.; Saratti, C.M. Interceptive treatment of tooth wear: A revised protocol for the full molding technique. Int. J. Esthet. Dent. 2020, 15, 264–286. [Google Scholar]
- Patcas, R.; Zinelis, S.; Eliades, G.; Eliades, T. Surface and interfacial analysis of sandblasted and acid-etched enamel for bonding orthodontic adhesives. AJO-DO 2015, 147, S64–S75. [Google Scholar] [CrossRef] [PubMed]
- Dietschi, N.F., Jr. Shading concepts and layering techniques to master direct anterior composite restorations: An update. Br. Dent. J. 2016, 221, 765–771. [Google Scholar] [CrossRef]
- Goldstein, G.; Goodacre, C.; MacGregor, K. Occlusal Vertical Dimension: Best Evidence Consensus Statement. J. Prosthodont. 2021, 30, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Abduo, J. Safety of increasing vertical dimension of occlusion: A systematic review. Quintessence Int. 2012, 43, 369–380. [Google Scholar] [PubMed]
- Julià-Sánchez, S.; Álvarez-Herms, J.; Cirer-Sastre, R.; Corbi, F.; Burtscher, M. The influence of dental occlusion on dynamic balance and muscular tone. Front. Physiol. 2020, 10, 1626. [Google Scholar] [CrossRef] [PubMed]
- Lepidi, L.; Galli, M.; Grammatica, A.; Joda, T.; Wang, H.; Li, J. Indirect Digital Workflow for Virtual Cross-Mounting of Fixed Implant-Supported Prostheses to Create a 3D Virtual Patient. J. Prosthodont. 2021, 30, 177–182. [Google Scholar] [CrossRef]
- Mehta, S.B.; Bronkhorst, E.M.; Lima, V.P.; Crins, L.; Bronkhorst, H.; Opdam, N.J.; Huysmans, M.-C.D.; Loomans, B.A. The effect of pre-treatment levels of tooth wear and the applied increase in the vertical dimension of occlusion (VDO) on the survival of direct resin composite restorations. J. Dent. 2021, 111, 103712. [Google Scholar] [CrossRef]
- Vajani, D.; Tejani, T.H.; Milosevic, A. Direct composite resin for the management of tooth wear: A systematic review. Clin. Cosmet. Investig. Dent. 2020, 12, 465–475. [Google Scholar] [CrossRef]



















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blasi Beriain, M.; Rocca, G.T.; Franchini, L.; Dietschi, D.; Saratti, C.M. Rehabilitation of Worn Dentition with Direct Resin Composite Restorations: A Case Report. Dent. J. 2022, 10, 51. https://doi.org/10.3390/dj10040051
Blasi Beriain M, Rocca GT, Franchini L, Dietschi D, Saratti CM. Rehabilitation of Worn Dentition with Direct Resin Composite Restorations: A Case Report. Dentistry Journal. 2022; 10(4):51. https://doi.org/10.3390/dj10040051
Chicago/Turabian StyleBlasi Beriain, Marta, Giovanni Tommaso Rocca, Leonardo Franchini, Didier Dietschi, and Carlo Massimo Saratti. 2022. "Rehabilitation of Worn Dentition with Direct Resin Composite Restorations: A Case Report" Dentistry Journal 10, no. 4: 51. https://doi.org/10.3390/dj10040051
APA StyleBlasi Beriain, M., Rocca, G. T., Franchini, L., Dietschi, D., & Saratti, C. M. (2022). Rehabilitation of Worn Dentition with Direct Resin Composite Restorations: A Case Report. Dentistry Journal, 10(4), 51. https://doi.org/10.3390/dj10040051