Recovery from Idiopathic Facial Paralysis (Bell’s Palsy) Using Photobiomodulation in Patients Non-Responsive to Standard Treatment: A Case Series Study

 , and
, and 
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Patients’ Information and Eligibility
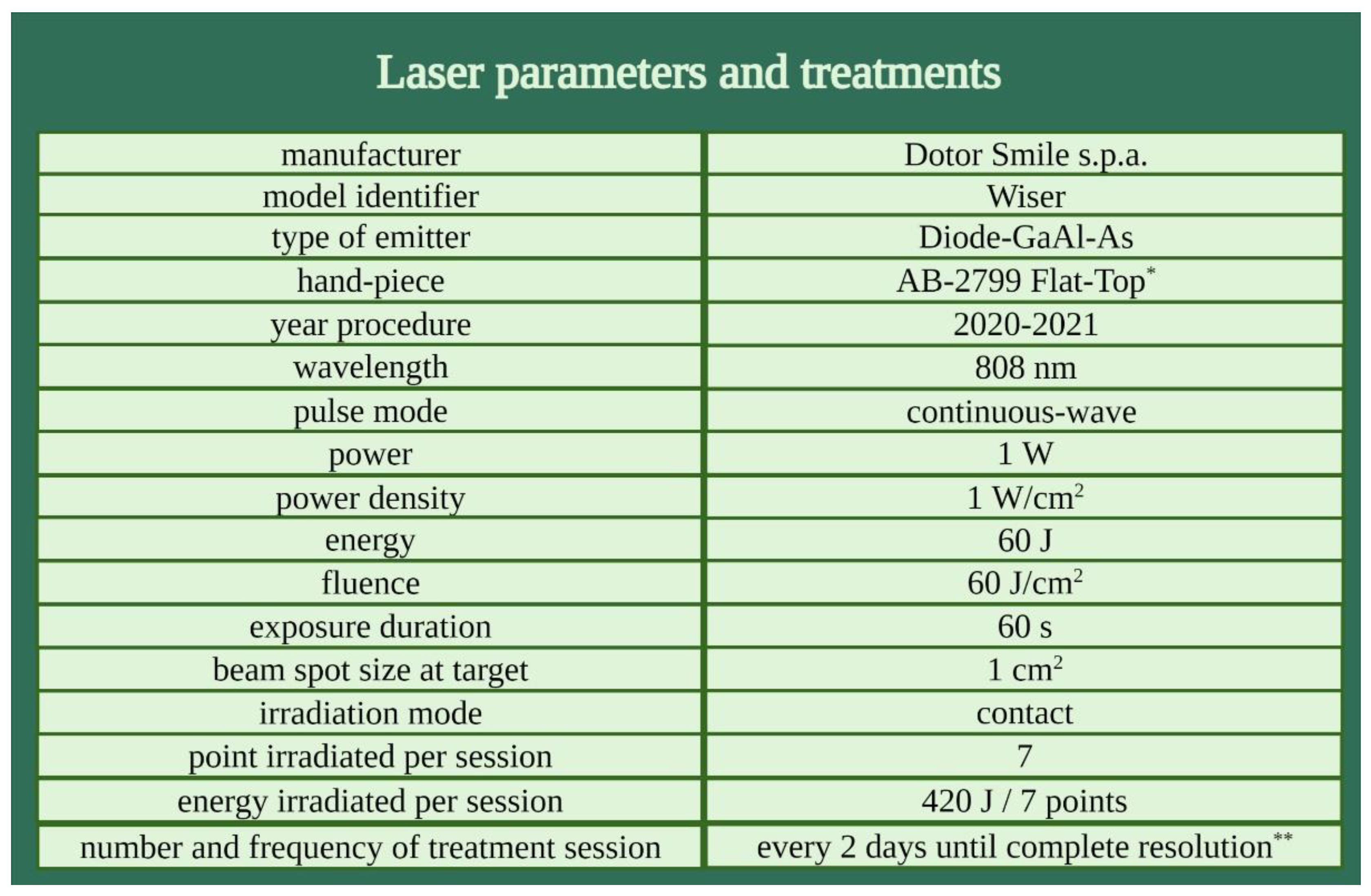
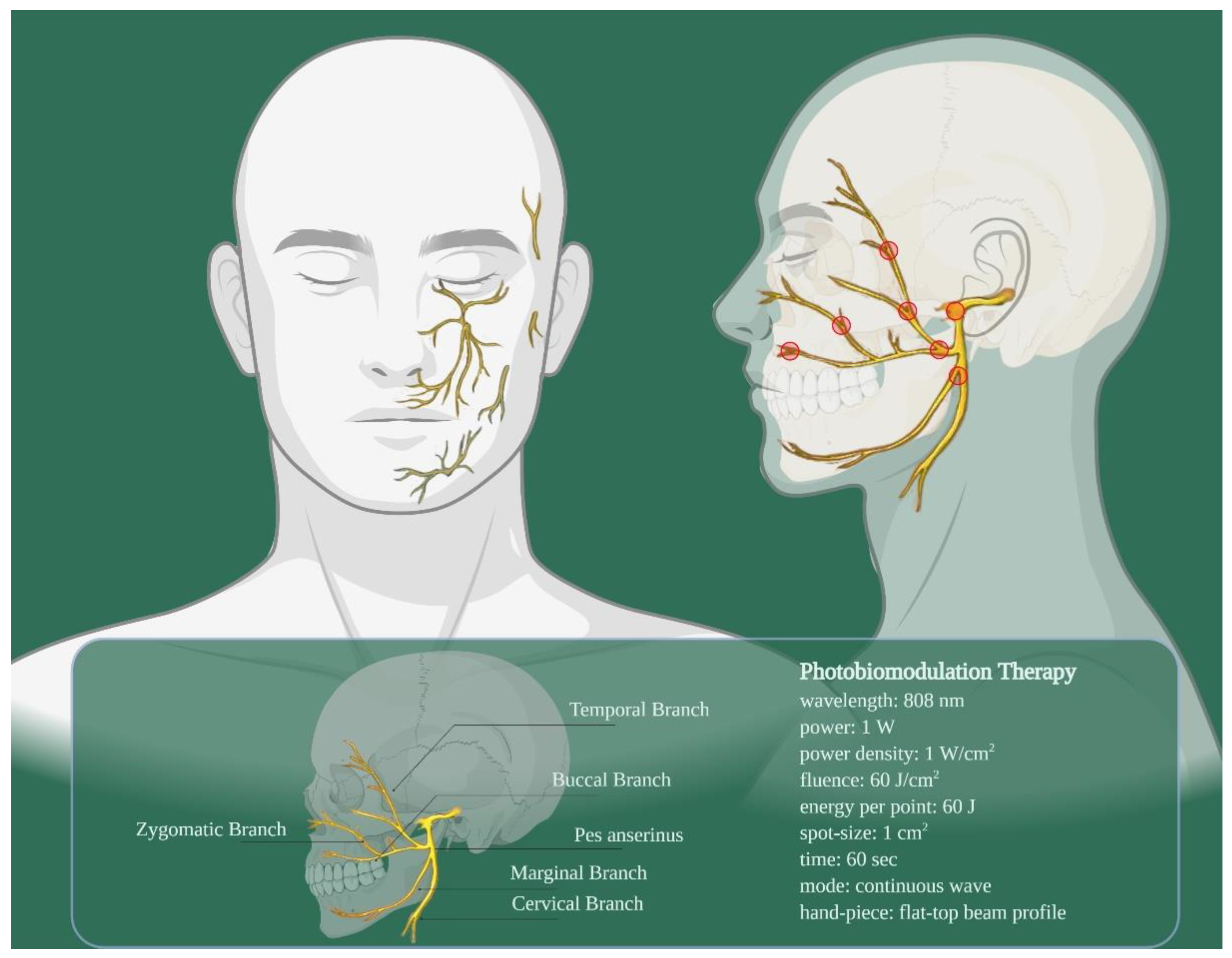
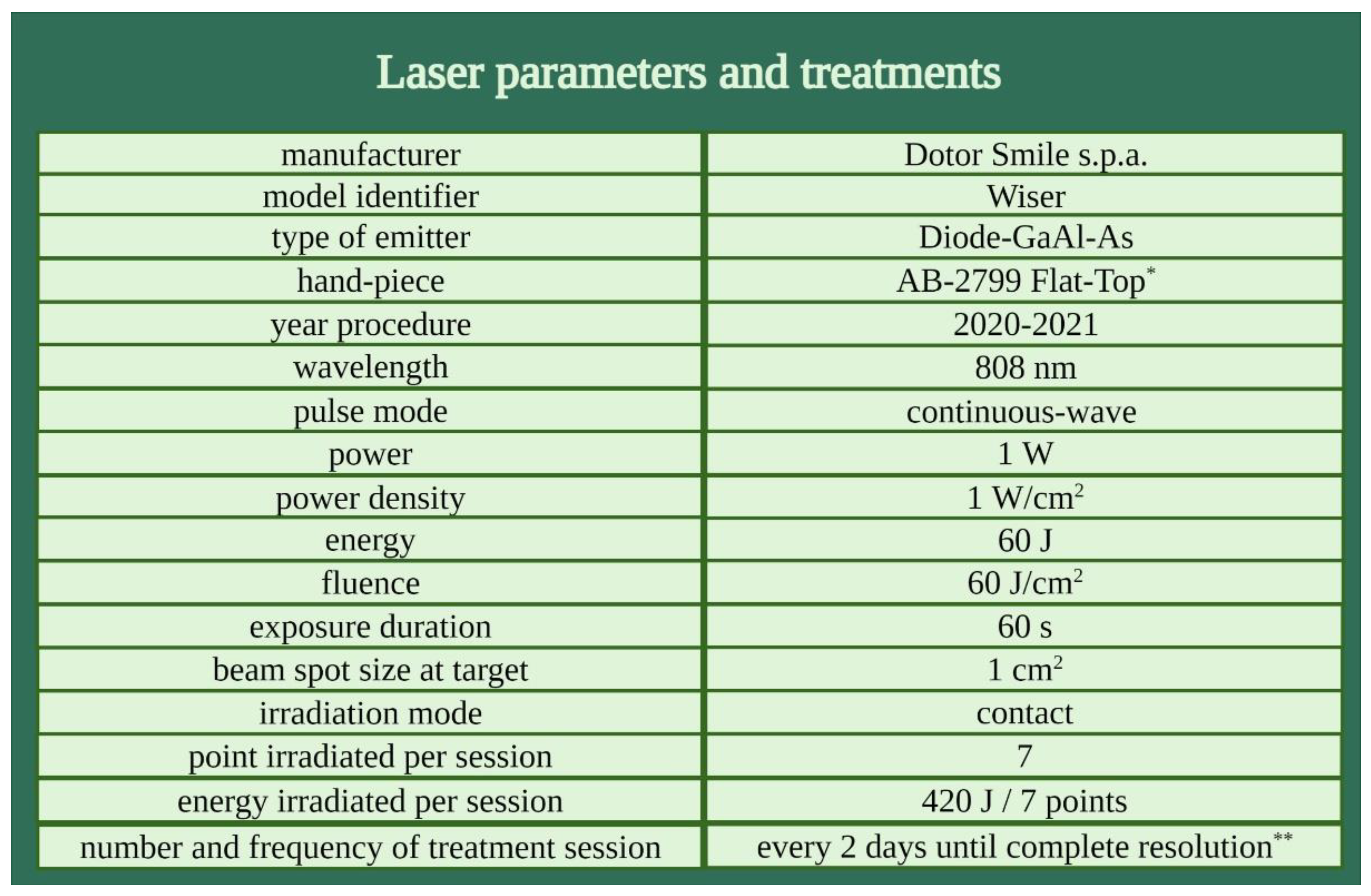
2.2. Procedures
2.3. Outcomes
3. Results
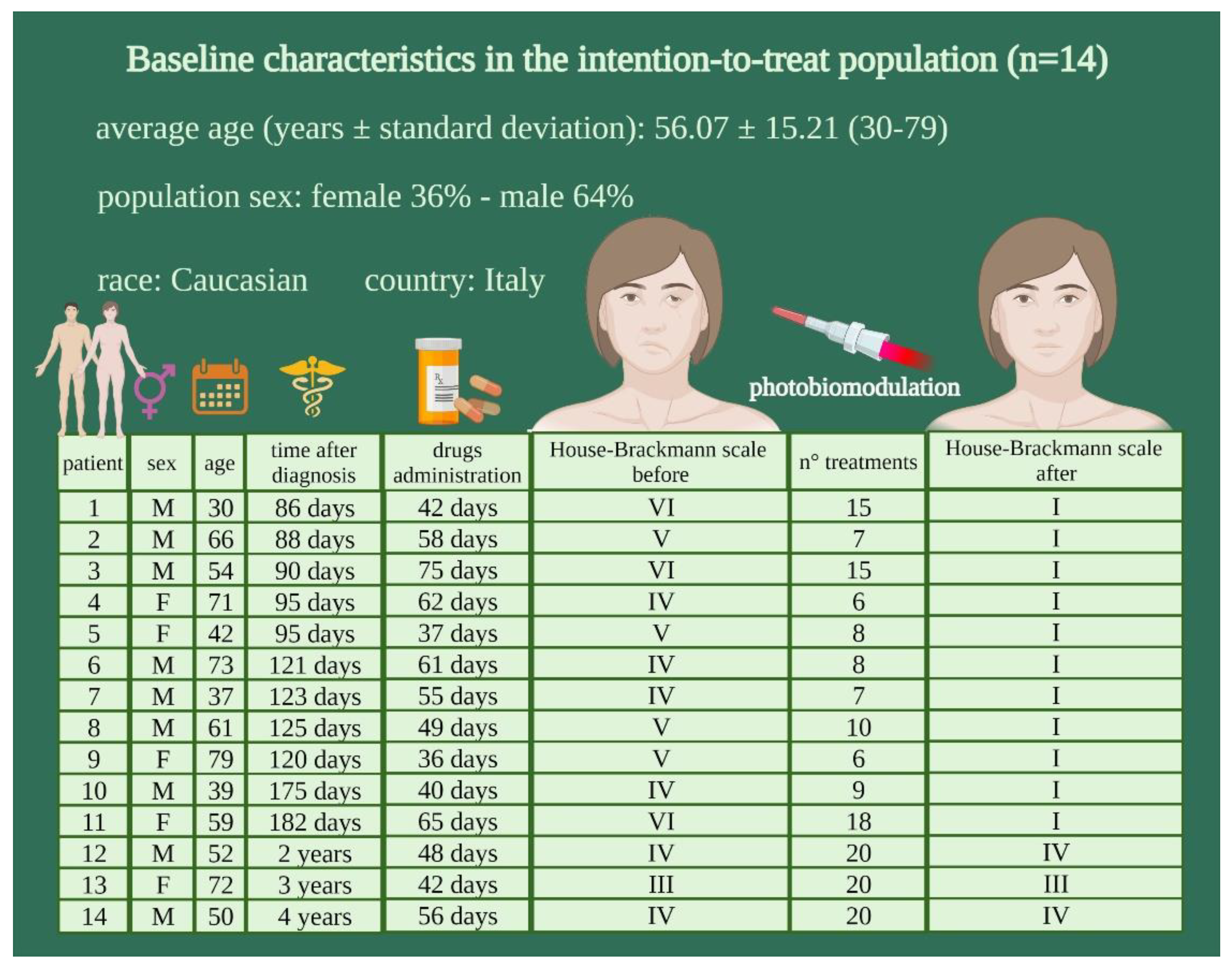
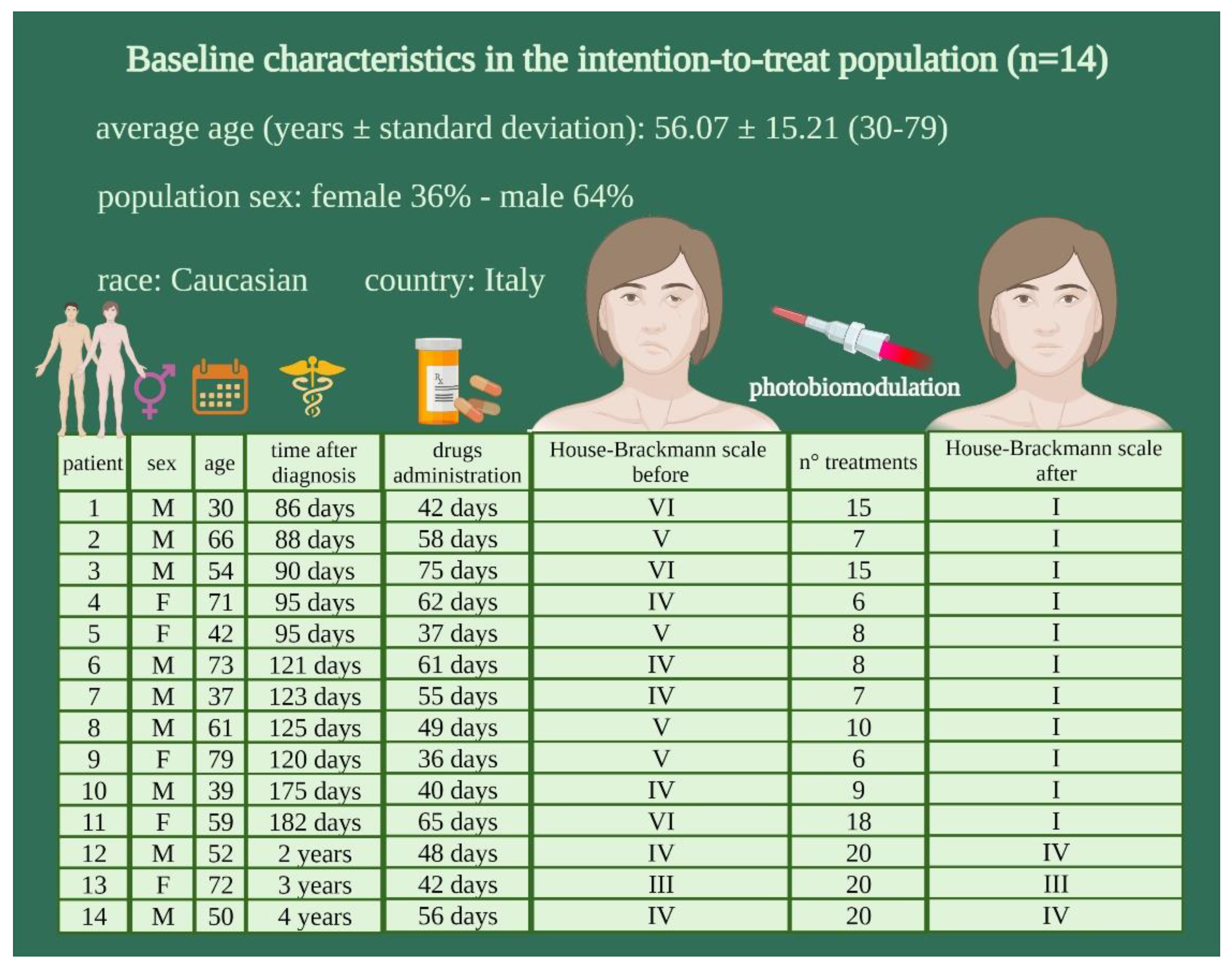
3.1. Participants
3.2. Primary and Secondary Endpoints Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pouwels, S.; Beurskens, C.H.; Luijmes, R.E.; Ingels, K.J. Clinical importance of smiling in patients with a peripheral facial palsy. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 1305–1306. [Google Scholar] [CrossRef]
- Zhang, W.; Xu, L.; Luo, T.; Wu, F.; Zhao, B.; Li, X. The etiology of Bell’s palsy: A review. J. Neurol. 2020, 267, 1896–1905. [Google Scholar] [CrossRef] [Green Version]
- Nellis, J.C.; Ishii, M.; Byrne, P.J.; Boahene, K.D.O.; Dey, J.K.; Ishii, L.E. Association among facial paralysis, depression, and of quality of life in facial plastic surgery patients. JAMA Facial Plast. Surg. 2017, 19, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Tiemstra, J.D.; Khatkhate, N. Bell’s palsy: Diagnosis and management. Am. Fam. Physician 2007, 76, 997–1002. [Google Scholar]
- Yoo, M.C.; Soh, Y.; Chon, J.; Lee, J.H.; Jung, J.; Kim, S.S.; You, M.W.; Byun, J.Y.; Kim, S.H.; Yeo, S.G. Evaluation of actors associated with favorable outcomes in adults with Bell palsy. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 256–263. [Google Scholar] [CrossRef]
- Heckmann, J.G.; Urban, P.P.; Pitz, S.; Guntinas-Lichius, O.; Gágyor, I. The diagnosis and treatment of idiopathic facial paresis (Bell’s palsy). Deutsches Ärzteblatt Int. 2019, 116, 692–702. [Google Scholar]
- Jabor, M.A.; Gianoli, G. Management of Bell’s palsy. J. State Med. Soc. 1996, 148, 279–283. [Google Scholar]
- Zandian, A.; Osiro, S.; Hudson, R.; Ali, I.M.; Matusz, P.; Tubbs, S.R.; Loukas, M. The neurologist’s dilemma: A comprehensive clinical review of Bell’s palsy, with emphasis on current management trends. Med. Sci. Monit. 2014, 20, 83–90. [Google Scholar] [PubMed] [Green Version]
- Finkensieper, M.; Volk, G.F.; Guntinas-Lichius, O. Erkrankungen des nervus facialis. Laryngo-Rhino-Otologie 2012, 91, 121–142. [Google Scholar] [CrossRef]
- Murakami, S.; Mizobuchi, M.; Nakashiro, Y.; Doi, T.; Hato, N.; Yanagihara, N. Bell palsy and herpes simplex virus: Identification of viral DNA in endoneurial fluid and muscle. Ann. Intern. Med. 1996, 124, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, P.G. Herpes simplex virus type 1 and Bell’s palsy—A current assessment of the controversy. J. Neurovirol. 2010, 16, 1–5. [Google Scholar] [CrossRef]
- Numthavaj, P.; Thakkinstian, A.; Dejthevaporn, C.; Attia, J. Corticosteroid and antiviral therapy for Bell’s palsy: A network meta-analysis. BMC Neurol. 2011, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Jung, J.; Lee, J.H.; Byun, J.Y.; Park, M.S.; Yeo, S.G. Delayed facial nerve decompression for Bell’s palsy. Eur. Arch. Otorhinolaryngol. 2016, 273, 1755–1760. [Google Scholar] [CrossRef]
- Gantz, B.J.; Rubinstein, J.T.; Gidley, P.; Woodworth, G.G. Surgical management of Bell’s palsy. Laryngoscope 1999, 109, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.; Yu, H.; Rao, X.; Wu, J.; Gou, Y.; Cui, H.; Huang, X.; Wang, L. Efficacy of manipulative acupuncture therapy monitored by LSCI technology in patients with severe Bell’s palsy: A randomized controlled trial. Evid. Based Complement. Altern. Med. 2020, 2020, 6531743. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.B.; Huang, B.; Zhang, C.Y.; Du, P.; Yuan, Q.; Bi, G.J.; Zhang, G.B.; Xie, M.J.; Luo, X.; Huang, G.Y.; et al. Effectiveness of strengthened stimulation during acupuncture for the treatment of Bell palsy: A randomized controlled trial. CMAJ Can. Med. Assoc. J. 2013, 185, 473–479. [Google Scholar] [CrossRef] [Green Version]
- Javaherian, M.; Attarbashi Moghaddam, B.; Bashardoust Tajali, S.; Dabbaghipour, N. Efficacy of low-level laser therapy on management of Bell’s palsy: A systematic review. Lasers Med. Sci. 2020, 35, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Ravera, S.; Colombo, E.; Pasquale, C.; Benedicenti, S.; Solimei, L.; Signore, A.; Amaroli, A. Mitochondrial bioenergetic, photobiomodulation and trigeminal branches nerve damage, what’s the connection? A review. Int. J. Mol. Sci. 2021, 22, 4347. [Google Scholar] [CrossRef]
- Ravera, S.; Ferrando, S.; Agas, D.; De Angelis, N.; Raffetto, M.; Sabbieti, M.G.; Signore, A.; Benedicenti, S.; Amaroli, A. 1064 nm Nd:YAG laser light affects transmembrane mitochondria respiratory chain complexes. J. Biophotonics 2019, 12, e201900101. [Google Scholar] [CrossRef]
- Amaroli, A.; Pasquale, C.; Zekiy, A.; Utyuzh, A.; Benedicenti, S.; Signore, A.; Ravera, S. Photobiomodulation and oxidative stress: 980 nm diode laser light regulates mitochondrial activity and reactive oxygen species production. Oxid. Med. Cell Longev. 2021, 2021, 6626286. [Google Scholar] [CrossRef]
- Hamblin, M.; Demidova, T. Mechanisms of low level light therapy. Proc. SPIE 2006, 6140, 614001. [Google Scholar]
- Karu, T.I. Molecular mechanism of the therapeutic effect of low-intensity laser irradiation. Dokl. Akad. Nauk. SSSR 1986, 291, 1245–1249. [Google Scholar]
- Amaroli, A.; Ravera, S.; Parker, S.; Panfoli, I.; Benedicenti, A.; Benedicenti, S. An 808-nm diode laser with a flat-top handpiece positively photobiomodulates mitochondria activities. Photomed. Laser Surg. 2016, 34, 564–571. [Google Scholar] [CrossRef]
- Hanna, R.; Agas, D.; Benedicenti, S.; Ferrando, S.; Laus, F.; Cuteri, V.; Lacava, G.; Sabbieti, M.G.; Amaroli, A. A comparative study between the effectiveness of 980 nm photobiomodulation delivered by hand-piece with gaussian vs. flat-top profiles on osteoblasts maturation. Front. Endocrinol. 2019, 10, 92. [Google Scholar] [CrossRef] [Green Version]
- Amaroli, A.; Arany, P.; Pasquale, C.; Benedicenti, S.; Bosco, A.; Ravera, S. Improving consistency of photobiomodulation therapy: A novel flat-top beam hand-piece versus standard gaussian probes on mitochondrial activity. Int. J. Mol. Sci. 2021, 22, 7788. [Google Scholar] [CrossRef]
- Amaroli, A.; Ravera, S.; Parker, S.; Panfoli, I.; Benedicenti, A.; Benedicenti, S. 808-nm laser therapy with a flat-top handpiece photobiomodulates mitochondria activities of Paramecium primaurelia (Protozoa). Lasers Med. Sci. 2016, 31, 741–747. [Google Scholar] [CrossRef]
- Ferrando, S.; Agas, D.; Mirata, S.; Signore, A.; De Angelis, N.; Ravera, S.; Utyuzh, A.S.; Parker, S.; Sabbieti, M.G.; Benedicenti, S.; et al. The 808 nm and 980 nm infrared laser irradiation affects spore germination and stored calcium homeostasis: A comparative study using delivery hand-pieces with standard (Gaussian) or flat-top profile. J. Photochem. Photobiol. 2019, 199, 111627. [Google Scholar] [CrossRef] [PubMed]
- Amaroli, A.; Ferrando, S.; Pozzolini, M.; Gallus, L.; Parker, S.; Benedicenti, S. The earthworm Dendrobaena veneta (Annelida): A new experimental-organism for photobiomodulation and wound healing. Eur. J. Histochem. 2018, 62, 2867. [Google Scholar] [CrossRef] [PubMed]
- Abdel Hamid, M.A.; Zaied, A.A.; Zayet, M.K.; Abdelmageed, H.; Hassan, E.A.; Amaroli, A. Efficacy of flat-top hand-piece using 980 nm diode laser photobiomodulation on socket healing after extraction: Split-mouth experimental model in dogs. J. Photochem. Photobiol. 2021, 97, 627–633. [Google Scholar] [CrossRef]
- Pasquale, C.; Colombo, E.; Benedicenti, S.; Signore, A.; Amaroli, A. 808-Nm near-infrared laser photobiomodulation versus switched-off laser placebo in major aphthae management: A randomized double-blind controlled trial. Appl. Sci. 2021, 11, 4717. [Google Scholar] [CrossRef]
- Fini Storchi, I.; Frosecchi, M.; Bovis, F.; Zekiy, A.; Benedicenti, S.; Amaroli, A.; Convissar, R.A. Snoring and sleep-related symptoms: A novel non-invasive 808 nm wavelength diode laser non-ablative outpatient treatment. A prospective pilot-study on 45 patients. Photonics 2021, 8, 69. [Google Scholar] [CrossRef]
- Baugh, R.F.; Basura, G.J.; Ishii, L.E.; Schwartz, S.R.; Drumheller, C.M.; Burkholder, R.; Deckard, N.A.; Dawson, C.; Driscoll, C.; Gillespie, M.B.; et al. Clinical practice guideline: Bell’s palsy. Otolaryngol. Head Neck Surg. 2013, 149 (Suppl. 3), S1–S27. [Google Scholar] [CrossRef] [PubMed]
- Lacombe, H. Evaluation de la paralysie faciale périphérique: Échelle de House-Brackmann [Evaluation of peripheral facial palsy: The House-Brackmann scale]. Revue Neurol. 2000, 156, 806–808. [Google Scholar]
- Gronseth, G.S.; Paduga, R. Evidence-based guideline update: Steroids and antivirals for bell palsy: Report of the guideline development Subcommittee of the American Academy of neurology. Neurology 2012, 79, 2209–2213. [Google Scholar] [CrossRef] [PubMed]
- Leclère, F.M.; Magalon, G.; Philandrianos, C.; Unglaub, F.; Servell, P.; Mordon, S. Prospective ex-vivo study on thermal effects in human skin phototypes II, IV and VI: A comparison between the 808, 1064, 1210 and 1320-nm diode laser. J. Cosmet. Laser Ther. 2012, 14, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Prud’hon, S.; Kubis, N. Bell’s palsy. Rev. Med. Interne 2019, 40, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Delgado Castillo, M.; Sanchez del Rio, M.; de Jesús Díaz García, A.; González Quevedo, A.; Sánchez López, J.V. Usefulness of magnetic field and laser for the treatment of idiopathic peripheral facial palsy. Fisioterapia 2013, 35, 252–257. [Google Scholar] [CrossRef]
- Teixeira, L.J.; Valbuza, J.S.; Prado, G.F. Physical therapy for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst. Rev. 2011, 12, CD006283. [Google Scholar] [CrossRef]
- Tanganeli, J.P.C.; de Oliveira, S.S.I.; da Silva, T.; Fernandes, K.P.S.; Motta, L.J.; Bussadori, S.K. Complete and fast recovery from idiopathic facial paralysis using laser-photobiomodulation. Case Rep. Dent. 2020, 2020, 9867693. [Google Scholar] [CrossRef]
- Kumar, S. Effect of class IV LASER on Bell’s palsy: A case series. Indian J. Phys. Ther. Res. 2019, 1, 55–58. [Google Scholar]
- Aghamohamdi, D.; Fakhari, S.; Farhoudi, M.; Farzin, H. The Efficacy of low-level laser therapy in the treatment of Bell’s palsy in diabetic patients. J. Lasers Med. Sci. 2020, 11, 310–315. [Google Scholar] [CrossRef]
- Ordahan, B.; Karahan, A.Y. Role of low-level laser therapy added to facial expression exercises in patients with idiopathic facial (Bell’s) palsy. J. Lasers Med. Sci. 2017, 32, 931–936. [Google Scholar] [CrossRef]
- Koyuncu, O.O.; Perlman, D.H.; Enquist, L.W. Efficient retrograde transport of pseudorabies virus within neurons requires local protein synthesis in axons. Cell Host Microbe 2013, 13, 54–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koyuncu, O.O.; Song, R.; Greco, T.M.; Cristea, I.M.; Enquist, L.W. The number of alphaherpesvirus particles infecting axons andthe axonal protein repertoire determines the outcome of neuronal infection. mBio 2015, 6, e00276-15. [Google Scholar] [CrossRef] [Green Version]
- Fang, F.; Liu, C.Y.; Zhang, J.; Zhu, L.; Qian, Y.X.; Yi, J.; Xiang, Z.H.; Wang, H.; Jiang, H. Involvement of MAPK ERK activation in upregulation of water channel protein aquaporin 1 in a mouse model of Bell’s palsy. J. Mol. Neurosci. 2015, 56, 164–176. [Google Scholar] [CrossRef]
- Masub, N.; Austin, E.; Huang, A.; Jagdeo, J. High-fluence light emitting diode-red light inhibits cell cycle progression in human dermal fibroblasts. J. Biophotonics 2021, 14, e202000359. [Google Scholar] [CrossRef]
- Louzeiro, G.C.; Teixeira, D.D.S.; Cherubini, K.; de Figueiredo, M.A.Z.; Salum, F.G. Does laser photobiomodulation prevent hyposalivation in patients undergoing head and neck radiotherapy? A systematic review and meta-analysis of controlled trials. Crit. Rev. Oncol. Hematol. 2020, 156, 103115. [Google Scholar] [CrossRef]
- Luo, G.Y.; Sun, L.; Wei, E.X.; Tan, X.; Liu, T.C. The effects of low-intensity He-Ne laser irradiation on erythrocyte metabolism. Lasers Med. Sci. 2015, 30, 2313–2318. [Google Scholar] [CrossRef]
- Grewal, D.S. Bell’s palsy-tertiary ischemia: An etiological factor in residual facial palsy. Indian J. Otolaryngol. Head Neck Surg. 2018, 70, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Dong, Y.; Lu, Y.; Zhang, W.; Brann, D.W.; Zhang, Q. Photobiomodulation for global cerebral ischemia: Targeting mitochondrial dynamics and functions. Mol. Neurobiol. 2019, 56, 1852–1869. [Google Scholar] [CrossRef] [PubMed]
- Amaroli, A.; Ravera, S.; Baldini, F.; Benedicenti, S.; Panfoli, I.; Vergani, L. Photobiomodulation with 808-nm diode laser light promotes wound healing of human endothelial cells through increased reactive oxygen species production stimulating mitochondrial oxidative phosphorylation. Lasers Med. Sci. 2019, 34, 495–504. [Google Scholar] [CrossRef]
- Colombo, E.; Signore, A.; Aicardi, S.; Zekiy, A.; Utyuzh, A.; Benedicenti, S.; Amaroli, A. Experimental and clinical applications of red and near-infrared photobiomodulation on endothelial dysfunction:a review. Biomedicines 2021, 9, 274. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, H.; Mitsukawa, N.; Itoh, M.; Otsuka, N. A view of the therapy for Bell’s palsy based on molecular biological analyses of facial muscles. J. Int. Adv. Otol. 2017, 13, 414–416. [Google Scholar] [CrossRef]
- Persson, A.K.; Kim, I.; Zhao, P.; Estacion, M.; Black, J.A.; Waxman, S.G. Sodium channels contribute to degeneration of dorsal root ganglion neurites induced by mitochondrial dysfunction in an in vitro model of axonal injury. J. Neurosci. 2013, 33, 19250–19261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaroli, A.; Parker, S.; Dorigo, G.; Benedicenti, A.; Benedicenti, S. Paramecium: A promising non-animal bioassay to study the effect of 808 nm infrared diode laser photobiomodulation. Photomed. Laser Surg. 2015, 33, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Amaroli, A.; Ferrando, S.; Benedicenti, S. Photobiomodulation affects key cellular pathways of all life-forms: Considerations on old and new laser light targets and the calcium issue. Photochem. Photobiol. 2019, 95, 455–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaroli, A.; Agas, D.; Laus, F.; Cuteri, V.; Hanna, R.; Sabbieti, M.G.; Benedicenti, S. The effects of photobiomodulation of 808 nm diode laser therapy at higher fluence on the in vitro osteogenic differentiation of bone marrow stromal cells. Front. Physiol. 2018, 9, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaroli, A.; Ferrando, S.; Hanna, R.; Gallus, L.; Benedicenti, A.; Scarfì, S.; Pozzolini, M.; Benedicenti, S. The photobiomodulation effect of higher-fluence 808-nm laser therapy with a flat-top handpiece on the wound healing of the earthworm Dendrobaena veneta: A brief report. Lasers Med. Sci. 2018, 33, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Amaroli, A.; Marcoli, M.; Venturini, A.; Passalacqua, M.; Agnati, L.F.; Signore, A.; Raffetto, M.; Maura, G.; Benedicenti, S.; Cervetto, C. Near-infrared laser photons induce glutamate release from cerebrocortical nerve terminals. J. Biophotonics 2018, 11, e201800102. [Google Scholar] [CrossRef]
- Mathes, T.; Pieper, D. Clarifying the distinction between case series and cohort studies in systematic reviews of comparative studies: Potential impact on body of evidence and workload. BMC Med. Res. Methodol. 2017, 17, 107. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasquale, C.; Utyuzh, A.; Mikhailova, M.V.; Colombo, E.; Amaroli, A. Recovery from Idiopathic Facial Paralysis (Bell’s Palsy) Using Photobiomodulation in Patients Non-Responsive to Standard Treatment: A Case Series Study. Photonics 2021, 8, 341. https://doi.org/10.3390/photonics8080341
Pasquale C, Utyuzh A, Mikhailova MV, Colombo E, Amaroli A. Recovery from Idiopathic Facial Paralysis (Bell’s Palsy) Using Photobiomodulation in Patients Non-Responsive to Standard Treatment: A Case Series Study. Photonics. 2021; 8(8):341. https://doi.org/10.3390/photonics8080341
Chicago/Turabian StylePasquale, Claudio, Anatoliy Utyuzh, Maria Vladimirovna Mikhailova, Esteban Colombo, and Andrea Amaroli. 2021. "Recovery from Idiopathic Facial Paralysis (Bell’s Palsy) Using Photobiomodulation in Patients Non-Responsive to Standard Treatment: A Case Series Study" Photonics 8, no. 8: 341. https://doi.org/10.3390/photonics8080341
APA StylePasquale, C., Utyuzh, A., Mikhailova, M. V., Colombo, E., & Amaroli, A. (2021). Recovery from Idiopathic Facial Paralysis (Bell’s Palsy) Using Photobiomodulation in Patients Non-Responsive to Standard Treatment: A Case Series Study. Photonics, 8(8), 341. https://doi.org/10.3390/photonics8080341