
Is It Time to Supersede the Diagnostic Term “Melanoma In Situ with Regression?” A Narrative Review




{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
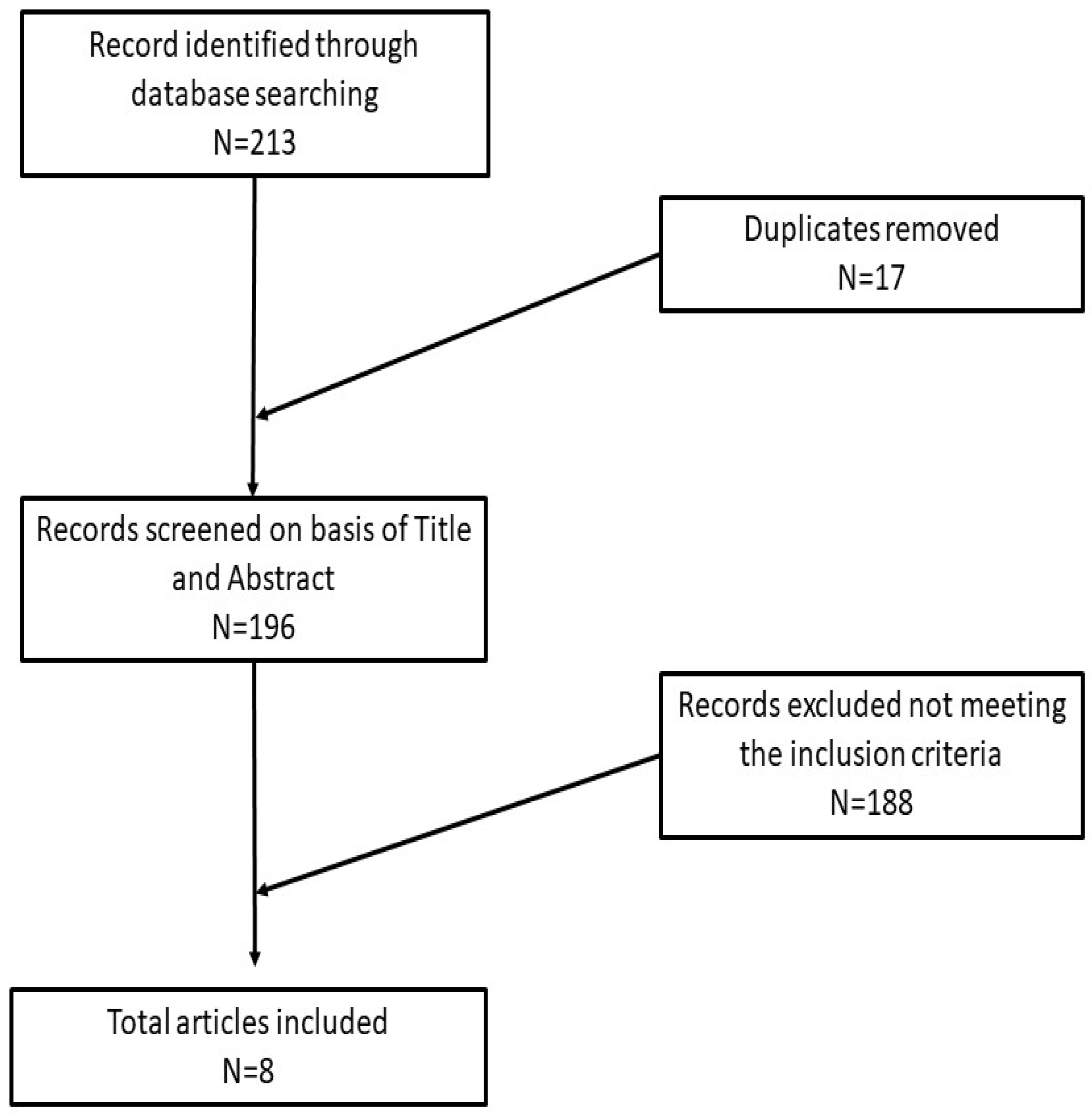
2. Materials and Methods
3. Results
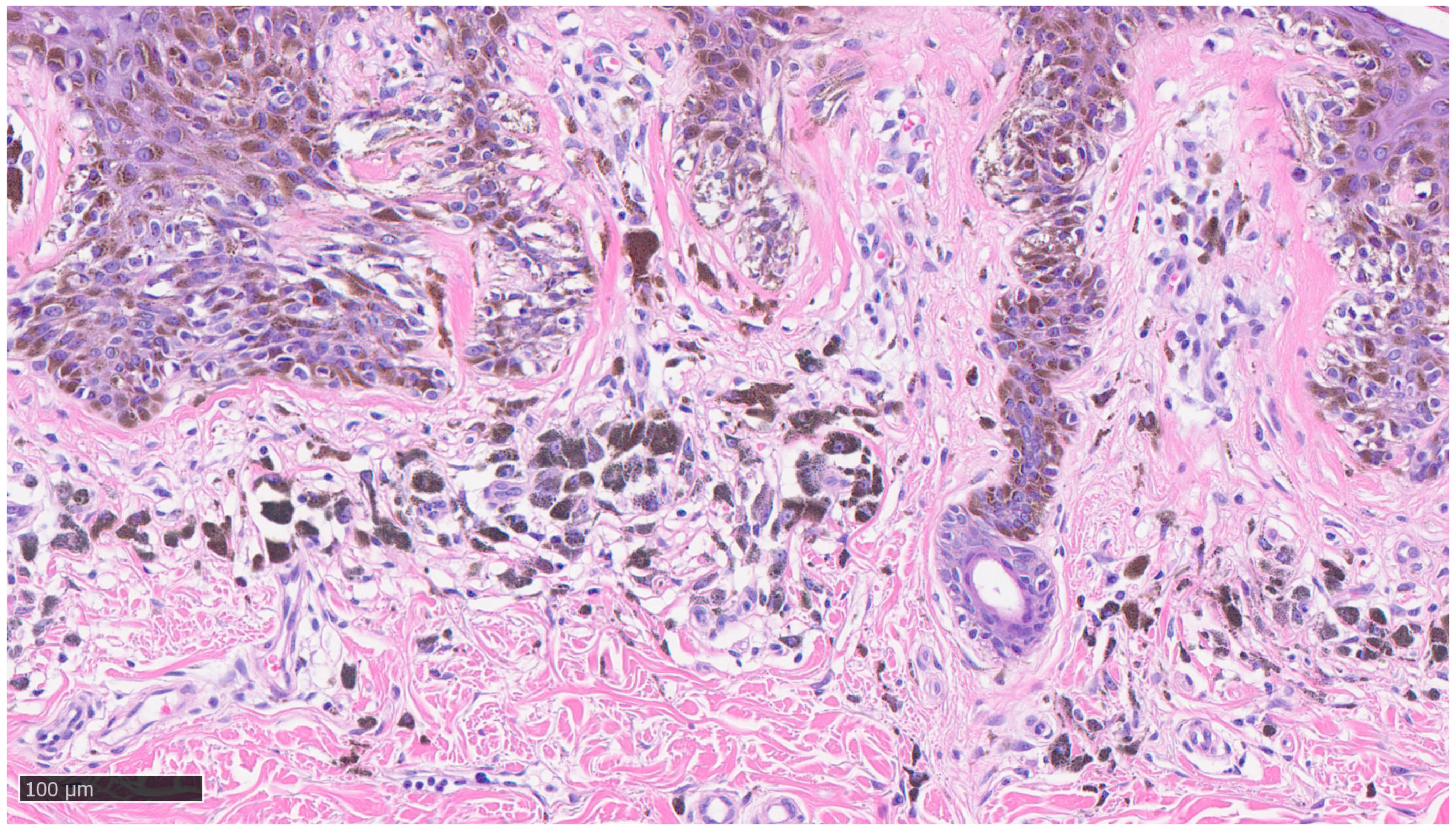
3.1. Histological Features of MIS and Regression
3.2. Prognostic Information
3.3. Treatment
3.4. Conclusive Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lowe, L. Metastatic melanoma and rare melanoma variants: A review. Pathology 2023, 55, 236–244. [Google Scholar] [CrossRef]
- Rashid, S.; Shaughnessy, M.; Tsao, H. Melanoma classification and management in the era of molecular medicine. Dermatol. Clin. 2023, 41, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Ramírez, D.; Ojeda-Vila, T.; Ríos-Martín, J.J.; Nieto-Garcia, M.-A.; Ferrándiz, L. Association between tumor size and Breslow’s thickness in malignant melanoma: A cross-sectional, multicenter study. Melanoma Res. 2015, 25, 450–452. [Google Scholar] [CrossRef]
- Available online: https://documents.cap.org/protocols/cp-skin-melanoma-biopsy-20-4110.pdf (accessed on 15 December 2022).
- Slominski, A.; Wortsman, J.; Carlson, A.J.; Matsuoka, L.Y.; Balch, C.M.; Mihm, M.C. Malignant Melanoma. Arch. Pathol. Lab. Med. 2001, 125, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.-J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final Version of 2009 AJCC Melanoma Staging and Classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef]
- Nicola, T.; Sarah, S.; Siwei, Z.; Stewart, M. Lymphovascular invasion: Assessment and prognostic impact in melanoma and breast cancer. Histol. Histopathol. 2015, 30, 1001–1009. [Google Scholar] [CrossRef]
- Frydenlund, N.; Mahalingam, M. Desmoplastic Melanoma, Neurotropism, and Neurotrophin Receptors—What We Know and What We Do Not. Adv. Anat. Pathol. 2015, 22, 227–241. [Google Scholar] [CrossRef]
- Cartron, A.M.; Aldana, P.C.; Khachemoune, A. Reporting regression in primary cutaneous melanoma. Part 1: History, histological criteria and pathogenesis. Clin. Exp. Dermatol. 2021, 46, 28–33. [Google Scholar] [CrossRef]
- Knackstedt, T.; Knackstedt, R.W.; Couto, R.; Gastman, B. Malignant Melanoma: Diagnostic and Management Update. Plast. Reconstr. Surg. 2018, 142, 202e–216e. [Google Scholar] [CrossRef]
- Roncati, L.; Piscioli, F.; Pusiol, T.; Maiorana, A. Microinvasive Radial Growth Phase of Cutaneous Melanoma: A Histopatho-logical and Immunohistochemical Study with Diagnostic Implications. Acta Dermatovenerol. Croat. 2017, 25, 39–45. [Google Scholar] [PubMed]
- Sumner, W.C. Spontaneous regression of melanoma. Cancer 1953, 6, 1040–1043. [Google Scholar] [CrossRef]
- Cartron, A.M.; Aldana, P.C.; Khachemoune, A. Reporting regression in primary cutaneous melanoma. Part 2: Prognosis, Evaluation and Management. Clin. Exp. Dermatol. 2020, 45, 818–823. [Google Scholar] [CrossRef]
- Shai, A.; Avinoach, I.; Sagi, A. Metastatic Malignant Melanoma with Spontaneous and Complete Regression of the Primary Lesion. Case report and review of the literature. J. Dermatol. Surg. Oncol. 1994, 20, 342–345. [Google Scholar] [CrossRef]
- Elston, D.M.; Stratman, E.J.; Miller, S.J. Skin biopsy: Biopsy issues in specific diseases. J. Am. Acad. Dermatol. 2016, 74, 1–16. [Google Scholar] [PubMed]
- Bayer-Garner, I.B.; Ivan, D.; Schwartz, M.R.; Tschen, J.A. The Immunopathology of Regression in Benign Lichenoid Keratosis, Keratoacanthoma and Halo Nevus. Clin. Med. Res. 2004, 2, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Aung, P.P.; Nagarajan, P.; Prieto, V.G. Regression in primary cutaneous melanoma: Etiopathogenesis and clinical significance. Lab. Investig. 2017, 97, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Nichita, L.; Zurac, S.; Bastian, A. Comparative analysis of CEACAM1 expression in thin melanomas with and without regression. Oncol. Lett. 2019, 17, 4149–4154. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Wu, S. Tissue inhibitor of metalloproteinase 2 inhibits activation of the β-catenin signaling in melanoma cells. Cell Cycle 2015, 14, 1666–1674. [Google Scholar] [CrossRef]
- Higgins, H.W.; Lee, K.C.; Galan, A.; Leffell, D.J. Melanoma in situ: Part I. Epidemiology, screening, and clinical features. J. Am. Acad. Dermatol. 2020, 73, 181–190. [Google Scholar] [CrossRef]
- WHO. Classification of Tumors, 4th ed.; Elder, D.E., Massi, D., Scolyer, R.A., Willemze, R., Eds.; WHO: Geneva, Switzerland, 2018; Volume 11. [Google Scholar]
- Ramji, R.; Oakley, A.; Rademaker, M. Morphological evolution in melanoma in situ using revised pattern analysis. Pigment. Cell Melanoma Res. 2021, 34, 163–173. [Google Scholar] [CrossRef]
- Available online: https://snlg.iss.it/wp-content/uploads/2022/04/LG-411-SIAPEC-IAP.pdf (accessed on 15 December 2022).
- Slingluff, C.L., Jr.; Vollmer, R.T.; Reintgen, D.S.; Seigler, H.F. Lethal “Thin” Malignant Melanoma. Identifying patients at risk. Ann. Surg. 1988, 208, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, K.; Ronan, S.G.; Eng, A.M.; Briele, H.A.; Shioura, N.N.; Das Gupta, T.K. Thin malignant melanomas with regression and metas-tases. Arch Dermatol. 1987, 123, 1326–1330. [Google Scholar]
- Blessing, K.; McLaren, K. Histological regression in primary cutaneous melanoma: Recognition, prevalence and significance. Histopathology 1992, 20, 315–322. [Google Scholar] [CrossRef]
- Schou, G. Survival with primary cutaneous malignant melanoma, evaluated from 2012 cases. A multivariate regression analysis. Virchows Arch. A Pathol. Anat. Histopathol. 1985, 406, 179–195. [Google Scholar] [CrossRef]
- Morris, K.T.; Busam, K.J.; Bero, S.; Patel, A.; Brady, M.S. Primary Cutaneous Melanoma with Regression Does not Require a Lower Threshold for Sentinel Lymph Node Biopsy. Ann. Surg. Oncol. 2008, 15, 316–322. [Google Scholar] [CrossRef]
- Ribero, S.; Quaglino, P.; Osella-Abate, S.; Sanlorenzo, M.; Senetta, R.; Macrì, L.; Savoia, P.; Macripò, G.; Sapino, A.; Bernengo, M. Relevance of multiple basin drainage and primary histologic regression in prognosis of trunk melanoma patients with negative sentinel lymph nodes. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 1132–1137. [Google Scholar] [CrossRef]
- Higgins, H.W.; Lee, K.C.; Galan, A.; Leffell, D.J. Melanoma in situ: Part II. Histopathology, treatment, and clinical management. J. Am. Acad. Dermatol. 2015, 73, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Elder, D.; Murphy, G. Melanocytic Tumors of the Skin (AFIP Atlas of Tumor Pathology), 4th ed.; ARP Press: Washington, DC, USA, 2010. [Google Scholar]
- Massi, G.; LeBoit, P. Histological Diagnosis of Nevi and Melanoma, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Plaza, J.A.; Prieto, V.G. Pathology of Pigmented Skin Lesions; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Cartron, A.M.; Aldana, P.C.; Khachemoune, A. Reporting regression with melanoma in situ: Reappraisal of a potential paradox. Arch. Dermatol. Res. 2021, 313, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Barnhill, R. Pathology of Malignant Melanoma; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar]
- Available online: https://documents.cap.org/protocols/Skin.Melanoma.Bx_4.3.1.0.REL_CAPCP.pdf (accessed on 15 December 2022).
- Kang, S.; Barnhill, R.L.; Mihm, M.C.; Sober, A.J. Histologic regression in malignant melanoma: An interobserver concordance study. J. Cutan. Pathol. 1993, 20, 126–129. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colagrande, A.; Ingravallo, G.; Cazzato, G. Is It Time to Supersede the Diagnostic Term “Melanoma In Situ with Regression?” A Narrative Review. Dermatopathology 2023, 10, 120-127. https://doi.org/10.3390/dermatopathology10010018
Colagrande A, Ingravallo G, Cazzato G. Is It Time to Supersede the Diagnostic Term “Melanoma In Situ with Regression?” A Narrative Review. Dermatopathology. 2023; 10(1):120-127. https://doi.org/10.3390/dermatopathology10010018
Chicago/Turabian StyleColagrande, Anna, Giuseppe Ingravallo, and Gerardo Cazzato. 2023. "Is It Time to Supersede the Diagnostic Term “Melanoma In Situ with Regression?” A Narrative Review" Dermatopathology 10, no. 1: 120-127. https://doi.org/10.3390/dermatopathology10010018
APA StyleColagrande, A., Ingravallo, G., & Cazzato, G. (2023). Is It Time to Supersede the Diagnostic Term “Melanoma In Situ with Regression?” A Narrative Review. Dermatopathology, 10(1), 120-127. https://doi.org/10.3390/dermatopathology10010018