
Histopathologic Aspects of Malignancy-Associated Granuloma Annulare: A Single Institution Experience



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Case–Control Study
3.2. Clinical Characteristics
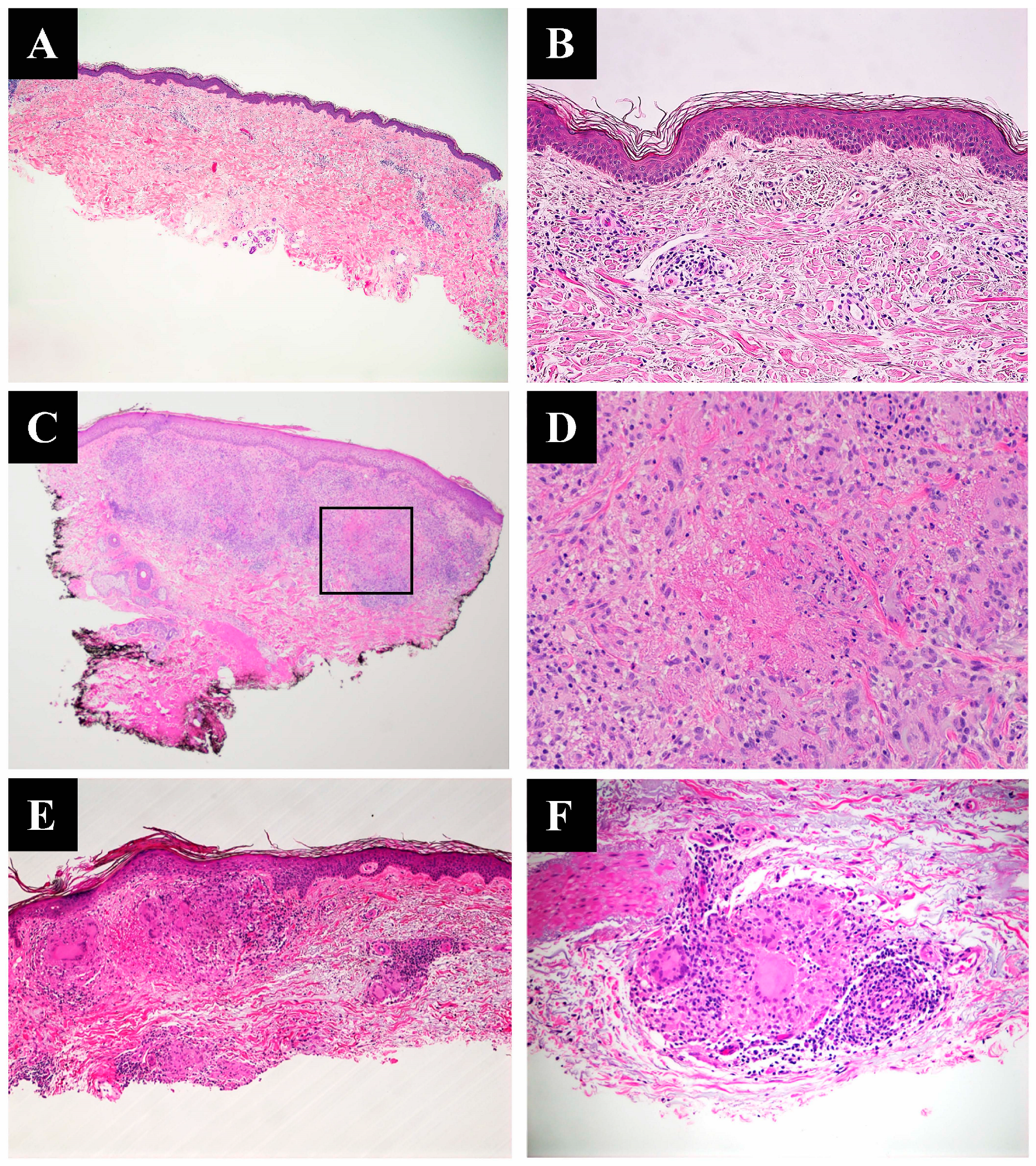
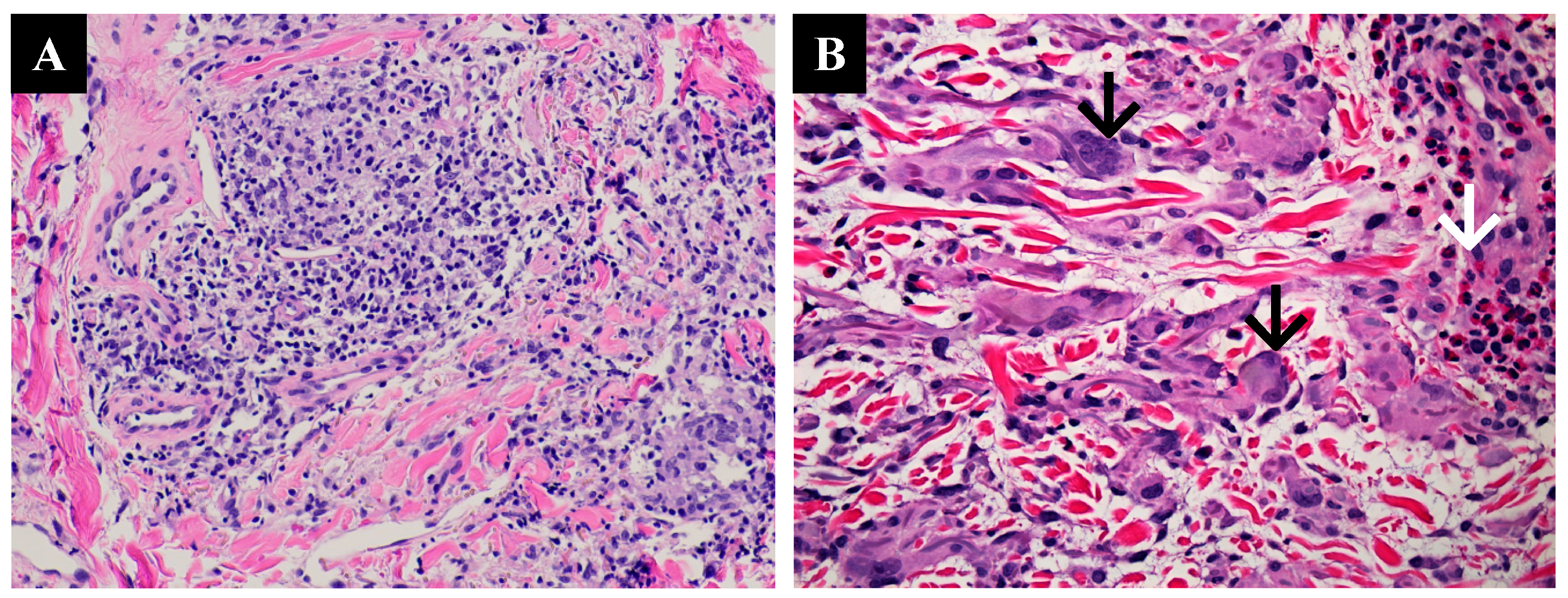
3.3. Histopathological Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Umbert, P.; Winkelmann, R.K. Histologic, ultrastructural and histochemical studies of granuloma annulare. Arch. Dermatol. 1977, 113, 1681–1686. [Google Scholar] [CrossRef]
- Muhlbauer, J.E. Granuloma annulare. J. Am. Acad. Dermatol. 1980, 3, 217–230. [Google Scholar] [CrossRef]
- Cyr, P.R. Diagnosis and management of granuloma annulare. Am. Fam. Physician. 2006, 74, 1729–1734. [Google Scholar]
- Dabski, K.; Winkelmann, R.K. Generalized granuloma annulare: Histopathology and immunopathology. Systematic review of 100 cases and comparison with localized granuloma annulare. J. Am. Acad. Dermatol. 1989, 20, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Thornsberry, L.A.; English, J.C., 3rd. Etiology, diagnosis, and therapeutic management of granuloma annulare: An update. Am. J. Clin. Dermatol. 2013, 14, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Piette, E.W.; Rosenbach, M. Granuloma annulare: Pathogenesis, disease associations and triggers, and therapeutic options. J. Am. Acad. Dermatol. 2016, 75, 467–479. [Google Scholar] [CrossRef]
- Fayyazi, A.; Schweyer, S.; Eichmeyer, B.; Herms, J.; Hemmerlein, B.; Radzun, H.J.; Berger, H. Expression of IFNgamma, coexpression of TNFalpha and matrix metalloproteinases and apoptosis of T lymphocytes and macrophages in granuloma annulare. Arch. Dermatol. Res. 2000, 292, 384–390. [Google Scholar] [CrossRef]
- Buechner, S.A.; Winkelmann, R.K.; Banks, P.M. Identification of T-cell subpopulations in granuloma annulare. Arch. Dermatol. 1983, 119, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Dabski, K.; Winkelmann, R.K. Generalized granuloma annulare: Clinical and laboratory findings in 100 patients. J. Am. Acad. Dermatol. 1989, 20, 39–47. [Google Scholar] [CrossRef]
- Yun, J.H.; Lee, J.Y.; Kim, M.K.; Seo, Y.J.; Kim, M.H.; Cho, K.H.; Kim, M.B.; Lee, W.S.; Lee, K.H.; Kim, Y.C.; et al. Clinical and pathological features of generalized granuloma annulare with their correlation: A retrospective multicenter study in Korea. Ann. Dermatol. 2009, 21, 113–119. [Google Scholar] [CrossRef]
- Barbieri, J.S.; Rodriguez, O.; Rosenbach, M.; Margolis, D. Incidence and Prevalence of Granuloma Annulare in the United States. JAMA Dermatol. 2021, 157, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Hogan, D.J.; Sanusi, I.D.; Smoller, B.R. Granuloma annulare and malignant neoplasms. Am. J. Dermatopathol. 2003, 25, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Mangold, A.R.; Cumsky, H.J.; Costello, C.; Xie, D.Y.; Buras, M.; Nelson, S.A.; DiCaudo, D.J.; Sekulic, A.; Pittelkow, M.R. Clinical and histopathologic features of paraneoplastic granuloma annulare in association with solid organ malignancies: A case-control study. J. Am. Acad. Dermatol. 2018, 79, 913–920.e911. [Google Scholar] [CrossRef] [PubMed]
- Housman, T.S.; Feldman, S.; Williford, P.M.; Fleischer, A.B.; Goldman, N.D.; Acostamadiedo, J.M.; Chen, G. Skin cancer is among the most costly of all cancers to treat for the Medicare population. J. Am. Acad. Dermatol. 2003, 48, 425–429. [Google Scholar] [CrossRef]
- Müller, C.S.L.; Vogt, T. Granuloma annulare—Is it a paraneoplastic condition for malignant lymphoma? J. Dtsch. Dermatol. Ges. 2021, 19, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Min, M.S.; Lebwohl, M. Treatment of recalcitrant granuloma annulare (GA) with adalimumab: A single-center, observational study. J. Am. Acad. Dermatol. 2016, 74, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Charollais, R.; Aubin, F.; Roche-Kubler, B.; Puzenat, E. Two cases of granuloma annulare under anti-PD1 therapy. Ann. Dermatol. Venereol. 2018, 145, 116–119. [Google Scholar] [CrossRef]
- Dahl, M.V.; Ullman, S.; Goltz, R.W. Vasculitis in granuloma annulare: Histopathology and direct immunofluorescence. Arch. Dermatol. 1977, 113, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Harman, R.R. Hodgkin’s disease, seminoma of testicle and widespread granuloma annulare. Br. J. Dermatol. 1977, 97 (Suppl. S15), 50–51. [Google Scholar] [CrossRef]
- Barksdale, S.K.; Perniciaro, C.; Halling, K.C.; Strickler, J.G. Granuloma annulare in patients with malignant lymphoma: Clinicopathologic study of thirteen new cases. J. Am. Acad. Dermatol. 1994, 31, 42–48. [Google Scholar] [CrossRef]
- Stewart, K.A.; Cooper, P.H.; Greer, K.E.; Kersh, C.R. Granuloma annulare temporally associated with carcinoma of the breast. J. Am. Acad. Dermatol. 1989, 21 Pt 1, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Akyol, M.; Kiliçarslan, H.; Göze, F.; Emre, S. Granuloma annulare associated with prostate carcinoma. J. Eur. Acad. Dermatol. Venereol. 2003, 17, 464–465. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.R. Granuloma annulare associated with malignancy. South Med. J. 1997, 90, 1056–1059. [Google Scholar] [CrossRef] [PubMed]
- Vassileva, S.; Krasteva, M.; Marina, S.; Tsankov, N. Widespread granuloma annulare and cervical adenocarcinoma. Int. J. Dermatol. 1992, 31, 819. [Google Scholar] [CrossRef]
- Chiu, M.L.; Tang, M.B. Generalized granuloma annulare associated with gastrointestinal stromal tumour: Case report and review of clinical features and management. Clin. Exp. Dermatol. 2008, 33, 469–471. [Google Scholar] [CrossRef]
- Mestre, T.; Rodrigues, A.M.; Cardoso, J. Disseminated granuloma annulare and hepatocellular carcinoma: Association or coincidence? BMJ Case Rep. 2014, 2014, bcr2014205883. [Google Scholar] [CrossRef]
- Shimizu, S.; Yasui, C.; Tsuchiya, K. Atypical generalized granuloma annulare associated with two visceral cancers. J. Am. Acad. Dermatol. 2006, 54 (Suppl. S5), S236–S238. [Google Scholar] [CrossRef]
- Vedula, S.; Agha, I.; Luber, A.J. Paraneoplastic Granuloma Annulare Associated with Metastatic Lung Cancer. Skinmed 2021, 19, 387–389. [Google Scholar]
- Cho, S.I.; Yu, D.A.; Lee, J.H.; Cho, K.H.; Mun, J.H. Paraneoplastic Generalized Granuloma Annulare in a Patient with Hepatocellular Carcinoma. Ann. Dermatol. 2018, 30, 503–504. [Google Scholar] [CrossRef]
- Möst, J.; Spötl, L.; Mayr, G.; Gasser, A.; Sarti, A.; Dierich, M.P. Formation of multinucleated giant cells in vitro is dependent on the stage of monocyte to macrophage maturation. Blood 1997, 89, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Brooks, P.J.; Glogauer, M.; McCulloch, C.A. An Overview of the Derivation and Function of Multinucleated Giant Cells and Their Role in Pathologic Processes. Am. J. Pathol. 2019, 189, 1145–1158. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinicopathologic Findings | Interstitial GA (n:17) | Necrobiotic GA (n:15) | Sarcoidal GA (n:3) | Mixed GA (n:4) | Overall (n:39) | |
|---|---|---|---|---|---|---|
| Mean AGE | 74 (y) | 70 (y) | 70 (y) | 73 (y) | 72 (y) | |
| Location | Upper extremities | 7 (18%) | 7 (18%) | 1 (3%) | 2 (%) | 17 (%) |
| Lower extremities | 4 (10%) | 3 (8%) | 2 (5%) | 0 (0%) | 9 (23%) | |
| Trunk | 6 (15%) | 5 (13%) | 0 (0%) | 1 (3%) | 12 (31%) | |
| Perivascular Inflammation | Mild | 10 (26%) | 4 (10%) | 0 (0%) | 1 (3%) | 15 (38%) |
| Moderate | 4 (10%) | 9 (23%) | 3 (8%) | 3 (8%) | 19 (49%) | |
| Severe | 3 (8%) | 2 (5%) | 0 (0%) | 0 (0%) | 5 (13%) | |
| Multinucleated Giant Cells | 4 (10%) | 10 (26%) | 2 (5%) | 2 (5%) | 18 (46%) | |
| Type of Malignancy | Interstitial GA (n:17) | Necrobiotic GA (n:15) | Sarcoidal GA (n:3) | Mixed GA (n:5) | All (n:39) | |
|---|---|---|---|---|---|---|
| Hematologic Malignancies | CLL | 2 | 5 | 0 | 1 | 8(20%) |
| AML | 2 | 1 | 0 | 0 | 3 (8%) | |
| MDS/MPN | 2 | 1 | 0 | 0 | 3 (8%) | |
| CMML | 1 | 0 | 0 | 0 | 1 (3%) | |
| MF | 0 | 0 | 1 | 2 | 3 (8%) | |
| B cell lymphoma | 0 | 0 | 1 | 0 | 1 (3%) | |
| Overall | 7 | 7 | 2 | 3 | ||
| Solid Organ Malignancies | Breast carcinoma | 4 | 0 | 1 | 0 | 5 (13%) |
| Prostate carcinoma | 3 | 3 | 0 | 1 | 7 (18%) | |
| Ovarian carcinoma | 0 | 1 | 0 | 0 | 1 (3%) | |
| RCC | 0 | 1 | 0 | 1 | 2 (5%) | |
| Urothelial | 1 | 0 | 0 | 0 | 1 (3%) | |
| Melanoma | 2 | 3 | 0 | 0 | 5 (13%) | |
| Lung carcinoma | 1 | 0 | 0 | 0 | 1 (3%) | |
| Endometrial carcinoma | 1 | 0 | 0 | 0 | 1 (3%) | |
| Overall | 12 | 8 | 1 | 2 | ||
| Clinicopathologic Findings | Interstitial GA (n:14) | Necrobiotic GA (n:18) | Sarcoidal GA (n:1) | Mixed GA (n:3) | Overall (n: 36) | |
|---|---|---|---|---|---|---|
| Mean AGE | 63 (yo) | |||||
| Location | Upper extremities | 3 (%) | 7 (%) | 0 (0%) | 2 (%) | 12 (%) |
| Lower extremities | 9 (%) | 4 (%) | 1 (%) | 0 (0%) | 14 (%) | |
| Trunk | 2 (%) | 7 (%) | 0 (0%) | 1 (%) | 10 (%) | |
| Perivascular Inflammation | Mild | 3 (%) | 7 (%) | 1 0%) | 0 (%) | 11 (%) |
| Moderate | 6 (%) | 9 (%) | 0 (0%) | 0 (%) | 15 (%) | |
| Severe | 5 (%) | 2 (%) | 0 (0%) | 3 (%) | 10 (%) | |
| Multinucleated Giant Cells | 8 (22%) | 14 (39%) | 1(3%) | 3 (8%) | 26 (77%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagci, B.; Karakas, C.; Kaur, H.; Smoller, B.R. Histopathologic Aspects of Malignancy-Associated Granuloma Annulare: A Single Institution Experience. Dermatopathology 2023, 10, 95-103. https://doi.org/10.3390/dermatopathology10010015
Bagci B, Karakas C, Kaur H, Smoller BR. Histopathologic Aspects of Malignancy-Associated Granuloma Annulare: A Single Institution Experience. Dermatopathology. 2023; 10(1):95-103. https://doi.org/10.3390/dermatopathology10010015
Chicago/Turabian StyleBagci, Buket, Cansu Karakas, Harsimran Kaur, and Bruce R. Smoller. 2023. "Histopathologic Aspects of Malignancy-Associated Granuloma Annulare: A Single Institution Experience" Dermatopathology 10, no. 1: 95-103. https://doi.org/10.3390/dermatopathology10010015
APA StyleBagci, B., Karakas, C., Kaur, H., & Smoller, B. R. (2023). Histopathologic Aspects of Malignancy-Associated Granuloma Annulare: A Single Institution Experience. Dermatopathology, 10(1), 95-103. https://doi.org/10.3390/dermatopathology10010015