

The Effect of Daily Meditative Practices Based on Mindfulness and Self-Compassion on Emotional Distress under Stressful Conditions: A Randomized Controlled Trial


 and
and 
Abstract
1. Introduction
2. Materials and Methods
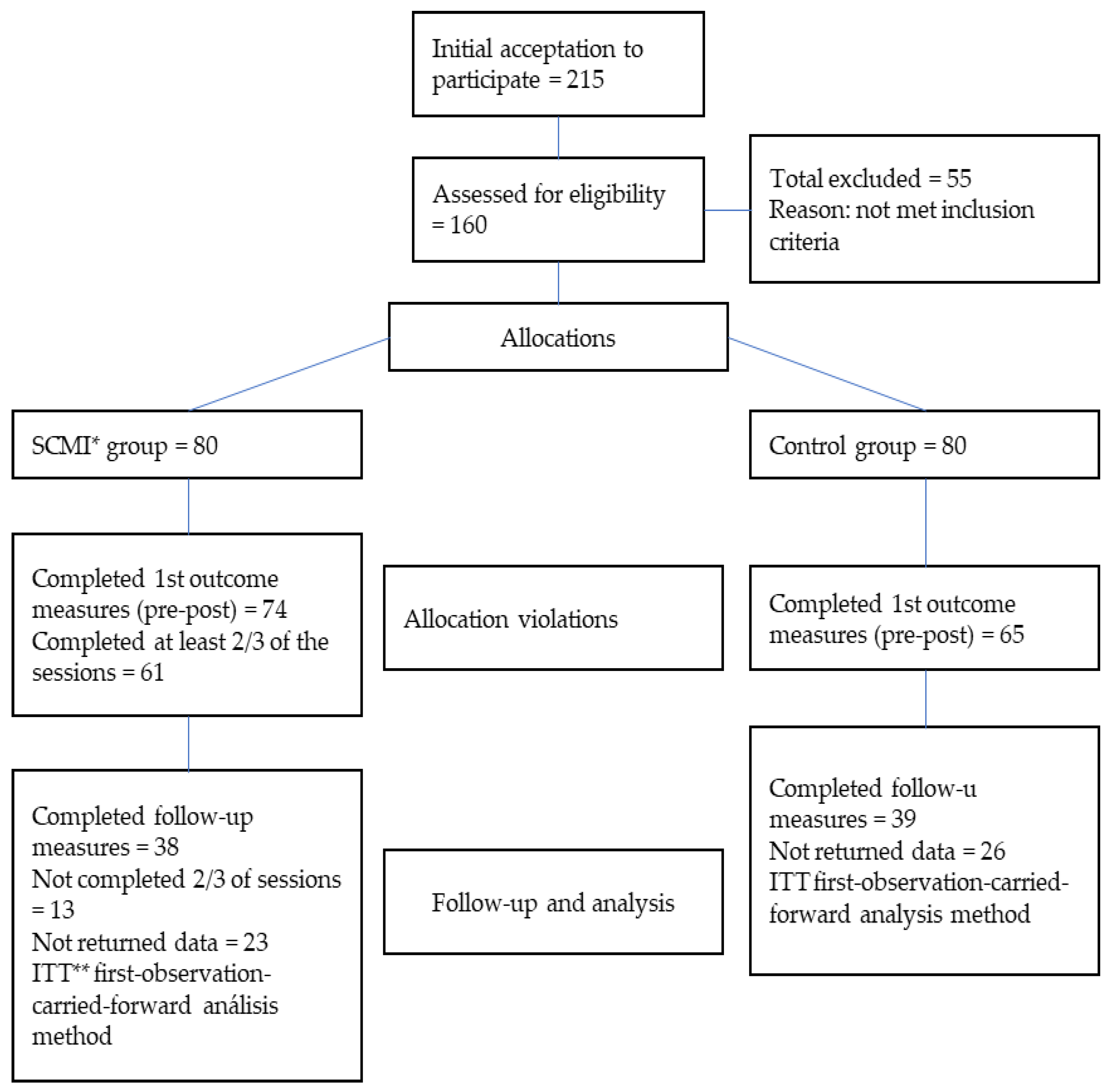
2.1. Participants
- -
- Age 18 years old or over;
- -
- Acceptable internet connectivity;
- -
- Not receiving (psychological or psychiatric) treatment for a mental disorder;
- -
- Not having a serious physical problem;
- -
- Not practicing mindfulness or SC at the time of the study;
- -
- No regular or professional practice of meditation.
2.2. Instruments
- -
- Sociodemographic data. sex, academic background, employment status, physical problems in the last two weeks, previous history of mental disorders and previous experience with meditation;
- -
- Depression, anxiety and stress scale-21 [28]. This is the short version of a self-administered scale measuring depression, anxiety and stress, with seven items per subscale. The depression scale assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia and inertia. The anxiety scale assesses autonomic arousal, skeletal muscle effects, situational anxiety and subjective experience of anxious affect. The stress scale is sensitive to levels of chronic non-specific arousal. It assesses difficulty relaxing, nervous arousal, and being easily upset/agitated, irritable/over-reactive and impatient. Scores for depression, anxiety and stress are calculated by summing the scores for the relevant items. The instrument is answered on a four-point Likert scale ranging from 0 (nothing) to 3 (a lot). Original internal consistencies (i.e., Cronbach’s alpha) were high: 0.86 for anxiety, 0.93 for depression, and 0.91 for stress. Our sample had the following coefficients: anxiety (0.83), depression (0.89) and stress (0.84). The Spanish adaptation was used [29].
- -
- Self-compassion scale—Short Form [30]. This is a short 12-item instrument extracted from the original SCS measure [31] that is answered on a five-point Likert scale from 1 (hardly ever) to 5 (almost always). The scale covers the three self-compassion dimensions: self-kindness versus self-judgment, common humanity versus isolation, and mindfulness versus over-identification. This short form has obtained adequate psychometric properties, generally with a Cronbach’s alphas higher than 0.80 [32]. Our participants had a Cronbach’s alpha coefficient of 0.83 for SCS-SF total scores. According to the three dimensions, self-kindness/self-judgment obtained an alpha = 0.68, common humanity/isolation, 0.77, and mindfulness/over-identification, 0.71. We used the Spanish adaptation of the scale [33].
2.3. Design
2.4. Procedure
2.5. Ethics
2.6. Data Analysis
3. Results
4. Discussion
- (i)
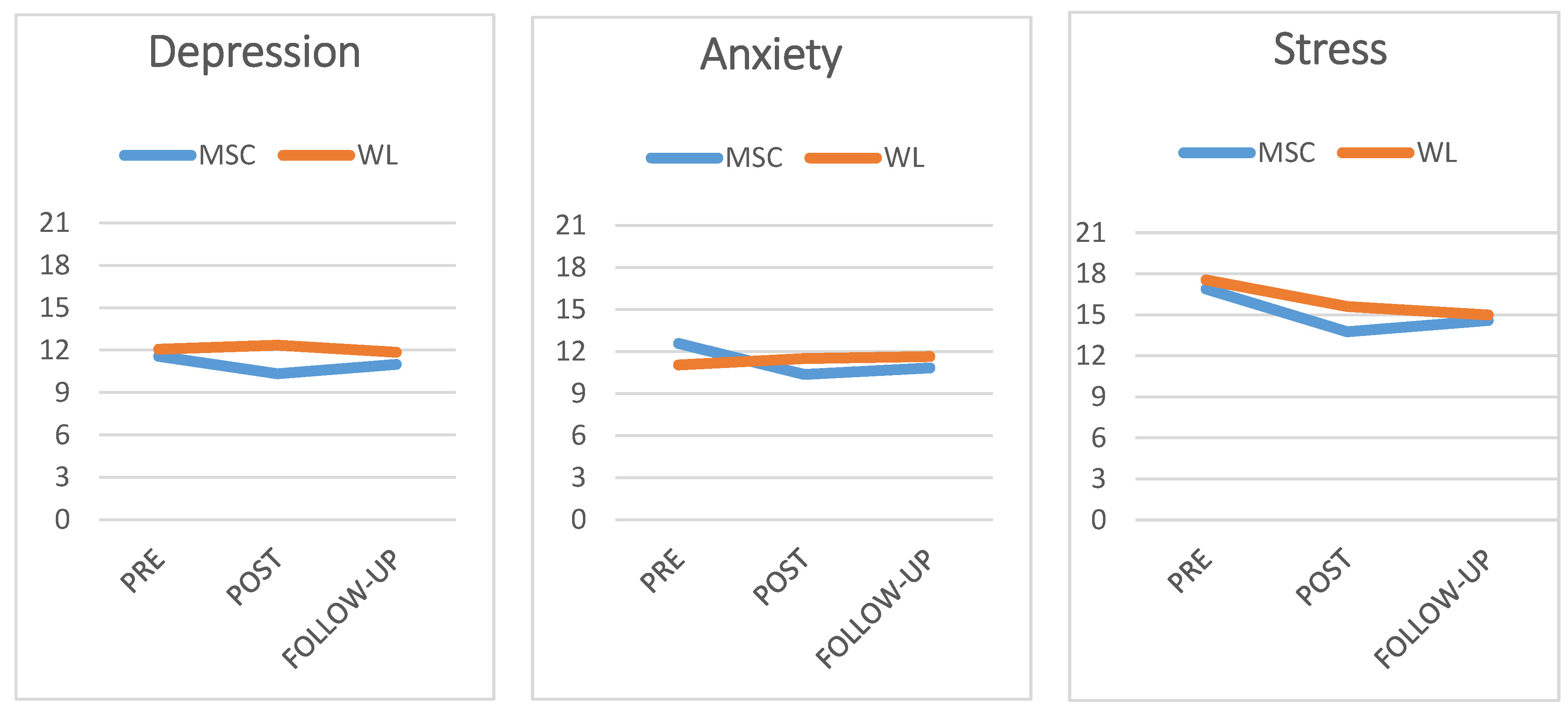
- This intervention was conducted during the hardest time of the coronavirus pandemic. There are data supporting the pervasive effects of those moments on mental health, with different social contexts and personal conditions (e.g., [42,43,44,45]). The pandemic was a greater stressor than any possible psychosocial interventions, to the extent that, once the intervention ended, the harmful effects of the pandemic were observed again. Our data agree with this explanation; while stress levels tended to decrease both in the intervention and control groups—perhaps due to a tendency to adapt to the initial stressful effect of the pandemic—anxiety and depression returned to their initial levels. Previous data support this stronger effect of intense and prolonged stressful events (e.g., [46]). In these cases, a systematic follow-up with complementary reminder intervention sessions might be particularly useful. Although our study included a follow-up, importantly, both a dose–response relationship and an extinction of the effect of meditation after ceasing the practice have been reported [22,23,24];
- (ii)
- Participants belonged to a non-clinical community sample. Initially, they were worried about the potential emotional impact of the pandemic, but this did not imply they had an emotional disorder. All the mean scores of participants in the pre-intervention phase indicated a mild level of depression, anxiety or stress, far from the scores obtained by Spanish mental health patients in the DASS-21 scale [47]. The re-analysis of data efficacy [10,23] has shown a better result with clinical samples compared to non-clinical ones (e.g., [48,49]), including online interventions (e.g., [50]). This could imply that SC intervention programs are effective but are especially so in participants with more serious psychological conditions, which could also imply greater adherence and maintenance of gains. As experts have pointed out, seeking mental health help can be understood as a first act of compassion [2,51];
- (iii)
- The third reason is a methodological issue. The discrepancy can be attributable to several methodological differences between our program and, e.g., MBSR or MSC (program duration, session duration, type of practice, etc.). In a strict sense, those comparisons cannot be carried out, except as a tendency analysis.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neff, K. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude Toward Oneself. Self. Identity 2003, 2, 85–101. [Google Scholar] [CrossRef]
- Neff, K.D. Self-Compassion: Theory, Method, Research, and Intervention. Annu. Rev. Psychol. 2022, 74, 193–218. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D.; Germer, C.K. A Pilot Study and Randomized Controlled Trial of the Mindful Self-Compassion Program. J. Clin. Psychol. 2013, 69, 28–44. [Google Scholar] [CrossRef]
- Muris, P.; Petrocchi, N. Protection or Vulnerability? A Meta-Analysis of the Relations Between the Positive and Negative Components of Self-Compassion and Psychopathology. Clin. Psychol. Psychother. 2017, 24, 373–383. [Google Scholar] [CrossRef]
- Cleare, S.; Gumley, A.; O’Connor, R.C. Self-Compassion, Self-Forgiveness, Suicidal Ideation, and Self-Harm: A Systematic Review. Clin. Psychol. Psychother. 2019, 26, 511–530. [Google Scholar] [CrossRef] [PubMed]
- Inwood, E.; Ferrari, M. Mechanisms of Change in the Relationship between Self-Compassion, Emotion Regulation, and Mental Health: A Systematic Review. Appl. Psychol. Health Well Being 2018, 10, 215–235. [Google Scholar] [CrossRef] [PubMed]
- MacBeth, A.; Gumley, A. Exploring Compassion: A Meta-Analysis of the Association between Self-Compassion and Psychopathology. Clin. Psychol. Rev. 2012, 32, 545–552. [Google Scholar] [CrossRef]
- Gutiérrez-Hernández, M.E.; Rodríguez, L.F.F.; Megolla, A.D.; Oyanadel, C.; Castro, W.P. Analysis of the Predictive Role of Self-Compassion on Emotional Distress during COVID-19 Lockdown. Soc. Sci. 2022, 11, 151. [Google Scholar] [CrossRef]
- Mackintosh, K.; Power, K.; Schwannauer, M.; Chan, S.W.Y. The Relationships Between Self-Compassion, Attachment and Interpersonal Problems in Clinical Patients with Mixed Anxiety and Depression and Emotional Distress. Mindfulness 2018, 9, 961–971. [Google Scholar] [CrossRef]
- Winders, S.J.; Murphy, O.; Looney, K.; O’Reilly, G. Self-Compassion, Trauma, and Posttraumatic Stress Disorder: A Systematic Review. Clin. Psychol. Psychother. 2020, 27, 300–329. [Google Scholar] [CrossRef] [PubMed]
- Marsh, I.C.; Chan, S.W.Y.; Macbeth, A. Self-Compassion and Psychological Distress in Adolescents—A Meta-Analysis. Mindfulness 2018, 9, 1011–1027. [Google Scholar] [CrossRef] [PubMed]
- Chio, F.H.N.; Mak, W.W.S.; Yu, B.C.L. Meta-Analytic Review on the Differential Effects of Self-Compassion Components on Well-Being and Psychological Distress: The Moderating Role of Dialecticism on Self-Compassion. Clin. Psychol. Rev. 2021, 85, 101986. [Google Scholar] [CrossRef] [PubMed]
- Eichholz, A.; Schwartz, C.; Meule, A.; Heese, J.; Neumüller, J.; Voderholzer, U. Self-Compassion and Emotion Regulation Difficulties in Obsessive–Compulsive Disorder. Clin. Psychol. Psychother. 2020, 27, 630–639. [Google Scholar] [CrossRef]
- Meyer, L.P.; Leppma, M. The Role of Mindfulness, Self-Compassion, and Emotion Regulation in Eating Disorder Symptoms Among College Students. J. Coll. Couns. 2019, 22, 211–224. [Google Scholar] [CrossRef]
- Gutiérrez-Hernández, M.E.; Fanjul, L.F.; Díaz-Megolla, A.; Reyes-Hurtado, P.; Herrera-Rodríguez, J.F.; Enjuto-Castellanos, M.D.P.; Peñate, W. Covid-19 Lockdown and Mental Health in a Sample Population in Spain: The Role of Self-Compassion. Int. J. Env. Res. Public Health 2021, 18, 2103. [Google Scholar] [CrossRef] [PubMed]
- Diedrich, A.; Grant, M.; Hofmann, S.G.; Hiller, W.; Berking, M. Self-Compassion as an Emotion Regulation Strategy in Major Depressive Disorder. Behav. Res. Ther. 2014, 58, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Germer, C.K.; Neff, K.D. Self-Compassion in Clinical Practice. J Clin Psychol 2013, 69, 856–867. [Google Scholar] [CrossRef]
- Gilbert, P. The Origins and Nature of Compassion Focused Therapy. Br. J. Clin. Psychol./Br. Psychol. Soc. 2014, 53, 6–41. [Google Scholar] [CrossRef]
- Fumero, A.; Peñate, W.; Oyanadel, C.; Porter, B. The Effectiveness of Mindfulness-Based Interventions on Anxiety Disorders. A Systematic Meta-Review. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 704–719. [Google Scholar] [CrossRef]
- Porter, B.; Oyanadel, C.; Sáez-Delgado, F.; Andaur, A.; Peñate, W. Systematic Review of Mindfulness-Based Interventions in Child-Adolescent Population: A Developmental Perspective. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1220–1243. [Google Scholar] [CrossRef]
- Finlay-Jones, A.; Kane, R.; Rees, C. Self-Compassion Online: A Pilot Study of an Internet-Based Self-Compassion Cultivation Program for Psychology Trainees. J. Clin. Psychol. 2017, 73, 797–816. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.N.; Tellegen, C.L.; Steindl, S.R. A Meta-Analysis of Compassion-Based Interventions: Current State of Knowledge and Future Directions. Behav. Ther. 2017, 48, 778–792. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Che, X.; Lei, Y.; Li, H. Investigating the Influence of Self-Compassion-Focused Interventions on Posttraumatic Stress: A Systematic Review and Meta-Analysis. Mindfulness 2021, 12, 2865–2876. [Google Scholar] [CrossRef] [PubMed]
- Quist Møller, S.A.; Sami, S.; Shapiro, S.L. Health Benefits of (Mindful) Self-Compassion Meditation and the Potential Complementarity to Mindfulness-Based Interventions: A Review of Randomized-Controlled Trials. OBM Integr. Complement. Med. 2018, 4, 002. [Google Scholar] [CrossRef]
- Beshai, S.; Bueno, C.; Yu, M.; Feeney, J.R.; Pitariu, A. Examining the Effectiveness of an Online Program to Cultivate Mindfulness and Self-Compassion Skills (Mind-OP): Randomized Controlled Trial on Amazon’s Mechanical Turk. Behav. Res. Ther. 2020, 134, 103724. [Google Scholar] [CrossRef]
- Finlay-Jones, A.; Boyes, M.; Perry, Y.; Sirois, F.; Lee, R.; Rees, C. Online Self-Compassion Training to Improve the Wellbeing of Youth with Chronic Medical Conditions: Protocol for a Randomised Control Trial. BMC Public Health 2020, 20, 106. [Google Scholar] [CrossRef]
- Johansson, M.; Marcusson-Clavertz, D.; Gunnarsson, C.; Olsson, I.; Kaldo, V.; Bratt, A. Feasibility and Preliminary Evaluation of Internet-Based Compassion and Cognitive–Behavioral Stress-Management Courses for Health Care Professionals: A Randomized Controlled Pilot Trial. Internet Interv. 2022, 30, 100574. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Sydney Psychology Foundation: Sydney, Australia, 1995; ISBN 7334-1423-0. [Google Scholar]
- Daza, P.; Novy, D.M.; Stanley, M.A.; Averill, P. The Depression Anxiety Stress Scale-21: Spanish Translation and Validation with a Hispanic Sample. J. Psychopathol. Behav. Assess 2002, 24, 195–205. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and Factorial Validation of a Short Form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Neff, K.D. The Development and Validation of a Scale to Measure Self-Compassion. Self. Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- Babenko, O.; Guo, Q. Measuring Self-Compassion in Medical Students: Factorial Validation of the Self-Compassion Scale–Short Form (SCS-SF). Acad. Psychiatry 2019, 43, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Campayo, J.; Navarro-Gil, M.; Andrés, E.; Montero-Marin, J.; López-Artal, L.; Demarzo, M.M.P. Validation of the Spanish Versions of the Long (26 Items) and Short (12 Items) Forms of the Self-Compassion Scale (SCS). Health Qual. Life Outcomes 2014, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Peyton, S. Your Resonant Self: Guided Meditations and Exercises to Engage Your Brain’s Capacity for Healing; W. W. Norton & Company: New York, NY, USA, 2017. [Google Scholar]
- Gilbert, P. Compassion Focused Therapy: Distinctive Features; Routledge: London, UK, 2010. [Google Scholar]
- Germer, C.K.; Neff, K. Teaching the Mindful Self-Compassion Program: A Guide for Professionals; Guilford Press: New York, NY, USA, 2019; 452p. [Google Scholar]
- Brach, T. Radical Acceptance: Embracing Your Life with the Heart of a Buddha; Random House: New York, NY, USA, 2004; pp. 1–333. [Google Scholar]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Goodreads: London, UK, 2005; pp. 1–304. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Dell Publishing: London, UK, 1990. [Google Scholar]
- Crits-Christoph, P.; Gibbons, M.B.C.; Mukherjee, D. Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change; John Wiley & Sons: New York, NY, USA, 2013; ISBN 1118038207. [Google Scholar]
- Ferrari, M.; Hunt, C.; Harrysunker, A.; Abbott, M.J.; Beath, A.P.; Einstein, D.A. Self-Compassion Interventions and Psychosocial Outcomes: A Meta-Analysis of RCTs. Mindfulness 2019, 10, 1455–1473. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Mazzi, M.; Wu, A.W.; Rimondini, M. What We Have Learned from Two Decades of Epidemics and Pandemics: A Systematic Review and Meta-Analysis of the Psychological Burden of Frontline Healthcare Workers. Psychother. Psychosom. 2021, 90, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Wang, S.; Cai, M.; Sun, R.; Liu, X. Self-Compassion and Life-Satisfaction among Chinese Self-Quarantined Residents during COVID-19 Pandemic: A Moderated Mediation Model of Positive Coping and Gender. Pers. Individ Dif. 2021, 170, 110457. [Google Scholar] [CrossRef]
- Joseph, C.A.; O’Shea, B.Q.; Eastman, M.R.; Finlay, J.M.; Kobayashi, L.C. Physical Isolation and Mental Health among Older US Adults during the COVID-19 Pandemic: Longitudinal Findings from the COVID-19 Coping Study. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 1273–1282. [Google Scholar] [CrossRef]
- Carmassi, C.; Dell’Osso, L.; Bertelloni, C.A.; Pedrinelli, V.; Dell’Oste, V.; Cordone, A.; Ruggeri, M.; Schimmenti, S.; Bonetto, C.; Tosato, S. Three-Month Follow-up Study of Mental Health Outcomes After a National COVID-19 Lockdown: Comparing Patients With Mood or Anxiety Disorders Living in an Area With a Higher Versus Lower Infection Incidence. J. Clin. Psychiatry 2022, 83, 39558. [Google Scholar] [CrossRef]
- Carlsson, J.M.; Mortensen, E.L.; Kastrup, M. A Follow-up Study of Mental Health and Health-Related Quality of Life in Tortured Refugees in Multidisciplinary Treatment. J. Nerv. Ment. Dis. 2005, 193, 651–657. [Google Scholar] [CrossRef]
- Bados, A.; Solanas, A.; Andrés, R. Psychometric properties of the Spanish version of Depression, Anxiety and Stress Scales (DASS). Psicothema 2005, 17, 679–683. [Google Scholar]
- Hwang, W.C.; Chan, C.P. Compassionate Meditation to Heal From Race-Related Stress: A Pilot Study With Asian Americans. Am. J. Orthopsychiatry 2019, 89, 482–492. [Google Scholar] [CrossRef]
- Wong, C.C.Y.; Mak, W.W.S. Writing Can Heal: Effects of Self-Compassion Writing among Hong Kong Chinese College Students. Asian Am. J. Psychol. 2016, 7, 74–82. [Google Scholar] [CrossRef]
- Mitchell, A.E.; Whittingham, K.; Steindl, S.; Kirby, J. Feasibility and Acceptability of a Brief Online Self-Compassion Intervention for Mothers of Infants. Arch. Womens Ment. Health 2018, 21, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P. Introducing Compassion-Focused Therapy. Adv. Psychiatr. Treat. 2009, 15, 199–208. [Google Scholar] [CrossRef]
- Barkham, M.; Stiles, W.B.; Connell, J.; Mellor-Clark, J. Psychological Treatment Outcomes in Routine NHS Services: What Do We Mean by Treatment Effectiveness? Psychol. Psychother. Theory Res. Pract. 2012, 85, 1–16. [Google Scholar] [CrossRef]
- Nicholson, R.A.; Berman, J.S. Is Follow-up Necessary in Evaluating Psychotherapy? Psychol. Bull. 1983, 93, 261–278. [Google Scholar] [CrossRef]
- Chambless, D.L.; Hollon, S.D. Defining Empirically Supported Therapies. J. Consult. Clin. Psychol. 1998, 66, 7–18. [Google Scholar] [CrossRef]
- Tolin, D.F.; Mckay, D.; Forman, E.M.; Klonsky, E.D.; Thombs, B.D. Empirically Supported Treatment: Recommendations for a New Model. Clin. Psychol. Sci. Pract. 2015, 22, 317–338. [Google Scholar] [CrossRef]
- Garrison, L.P.; Neumann, P.J.; Erickson, P.; Marshall, D.; Mullins, C.D. Using Real-World Data for Coverage and Payment Decisions: The ISPOR Real-World Data Task Force Report. Value Health 2007, 10, 326–335. [Google Scholar] [CrossRef]
- Klonoff, D.C. The Expanding Role of Real-World Evidence Trials in Health Care Decision Making. J. Diabetes Sci. Technol. 2020, 14, 174–179. [Google Scholar] [CrossRef]
- Schurman, B. Framework for FDA’s Real-World Evidence Program. Appl. Clin. Trials 2019, 28, 15–17. [Google Scholar]
- Akobeng, A.K. Principles of Evidence Based Medicine. Arch. Dis. Child 2005, 90, 837–840. [Google Scholar] [CrossRef] [PubMed]
- Szatmari, P.; Susser, E. Being Precise About Precision Mental Health. JAMA Psychiatry 2022, 79, 1149–1150. [Google Scholar] [CrossRef] [PubMed]
- Muris, P.; Otgaar, H. The Process of Science: A Critical Evaluation of More than 15 Years of Research on Self-Compassion with the Self-Compassion Scale. Mindfulness 2020, 11, 1469–1482. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mindfulness | Self-Compassion | Mindfulness/Self-Compassion |
|---|---|---|
| 1. Brief theoretical concepts on posture and meditation. Conscious breathing. 3. Seated meditations: sitting with the breath, and sitting with the breath and the body. 5. Meditation: body scan. 7. Practice: feet soles for rooting. 9. Walking meditation. 15. Meditation: the lake. 19. Meditation: the mountain. 25. Exercise: the raisins. 27. Practice: surfing the waves. 30. Meditation: Resting from worries | 4. Meditation: a cell. 6. Meditation: loving kindness to a loved one. 8. Meditation: creating a safe place. 10. Meditation: loving kindness to ourselves. 12. Meditation: the compassionate friend. 14. Meditation: giving and receiving compassion. 16. Meditation: imagining a compassionate self. 18. Finding difficult emotions. 21. Meditation: empathy with the inner critic. 23. Meditation: the Tonglen—awakening the heart of compassion. 26. Meditation: cultivating a forgiving heart. 28. Meditation: compassion for oneself and for others. | 2. Reassuring touch and self-compassion. 11. Meditation: discovering the resonant self-witness. 13. Meditation: embrace life with a smile. 17. Meditation: the radical acceptance of pain. 20. Meditation: receiving fear. 22. Informal practice: compassion with equanimity. 24. Meditation: the prenatal self. 29. Meditation: “who am I?” |
| Pre | Post | ||||
|---|---|---|---|---|---|
| Group | M (SD) | M (SD) | F (1124) | n2 | |
| SCS | WL | 33.67 (9.07) | 34.13 (10.23) | 30.30 *** | 0.194 |
| SCMI | 32.48 (9.55) | 40.11 (10.28) | |||
| SK-SJ | WL | 10.90 (3.56) | 10.88 (3.90) | 30.12 *** | 0.191 |
| SCMI | 10.52 (3.57) | 13.29 (3.70) | |||
| CH-I | WL | 11.19 (2.92) | 11.51 (3.40) | 15.62 *** | 0.109 |
| SCMI | 10.65 (3.40) | 13.21 (3.79) | |||
| M-OI | WL | 11.76 (3.75) | 11.91 (3.78) | 22.10 *** | 0.148 |
| SCMI | 11.30 (3.50) | 13.67 (3.32) |
| Variable | Group | Pre Mean (SD) | Post Mean (SD) | Follow-Up Mean (SD) |
|---|---|---|---|---|
| DEPRESSION | SCMI | 11.56 (3.22) | 10.33 (2.71) | 10.95 (2.67) |
| WL | 12.06 (4.51 | 12.35 (5.04) | 11.85 (3.85) | |
| ANXIETY | SCMI | 12.58 (3.48) | 10.37 (2.76) | 10.84 (2.76) |
| WL | 11.51 (4.05) | 11.51 (4.52) | 11.65 (3.06) | |
| STRESS | SCMI | 16.89 (10.79) | 13.76 (3.55) | 14.59 (0.41) |
| WL | 17.55 (12.01) | 15.61 (4.91) | 14.99 (4.21) |
| Post (n = 61) | Follow-Up (n = 38) | |||||
|---|---|---|---|---|---|---|
| Anxiety | Depression | Stress | Anxiety | Depression | Stress | |
| SCS | 0.47 *** | 0.51 *** | 0.59 *** | 0.34 ** | 0.30 * | 0.27 * |
| SK-SJ | 0.40 *** | 0.49 *** | 0.63 *** | 0.34 ** | 0.32 ** | 0.22 |
| CH-I | 0.33 ** | 0.37 ** | 0.33 ** | 0.30 * | 0.29 * | 0.22 |
| M-OI | 0.51 *** | 0.51 *** | 0.61 *** | 0.37 ** | 0.31 ** | 0.25 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Hernández, M.E.; Fanjul Rodríguez, L.F.; Díaz Megolla, A.; Oyanadel, C.; Peñate Castro, W. The Effect of Daily Meditative Practices Based on Mindfulness and Self-Compassion on Emotional Distress under Stressful Conditions: A Randomized Controlled Trial. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 762-775. https://doi.org/10.3390/ejihpe13040058
Gutiérrez-Hernández ME, Fanjul Rodríguez LF, Díaz Megolla A, Oyanadel C, Peñate Castro W. The Effect of Daily Meditative Practices Based on Mindfulness and Self-Compassion on Emotional Distress under Stressful Conditions: A Randomized Controlled Trial. European Journal of Investigation in Health, Psychology and Education. 2023; 13(4):762-775. https://doi.org/10.3390/ejihpe13040058
Chicago/Turabian StyleGutiérrez-Hernández, María Elena, Luisa Fernanda Fanjul Rodríguez, Alicia Díaz Megolla, Cristián Oyanadel, and Wenceslao Peñate Castro. 2023. "The Effect of Daily Meditative Practices Based on Mindfulness and Self-Compassion on Emotional Distress under Stressful Conditions: A Randomized Controlled Trial" European Journal of Investigation in Health, Psychology and Education 13, no. 4: 762-775. https://doi.org/10.3390/ejihpe13040058
APA StyleGutiérrez-Hernández, M. E., Fanjul Rodríguez, L. F., Díaz Megolla, A., Oyanadel, C., & Peñate Castro, W. (2023). The Effect of Daily Meditative Practices Based on Mindfulness and Self-Compassion on Emotional Distress under Stressful Conditions: A Randomized Controlled Trial. European Journal of Investigation in Health, Psychology and Education, 13(4), 762-775. https://doi.org/10.3390/ejihpe13040058