
Effects of Physical Activity, Exercise and Sport on Executive Function in Young People with Attention Deficit Hyperactivity Disorder: A Systematic Review




Abstract
:1. Introduction
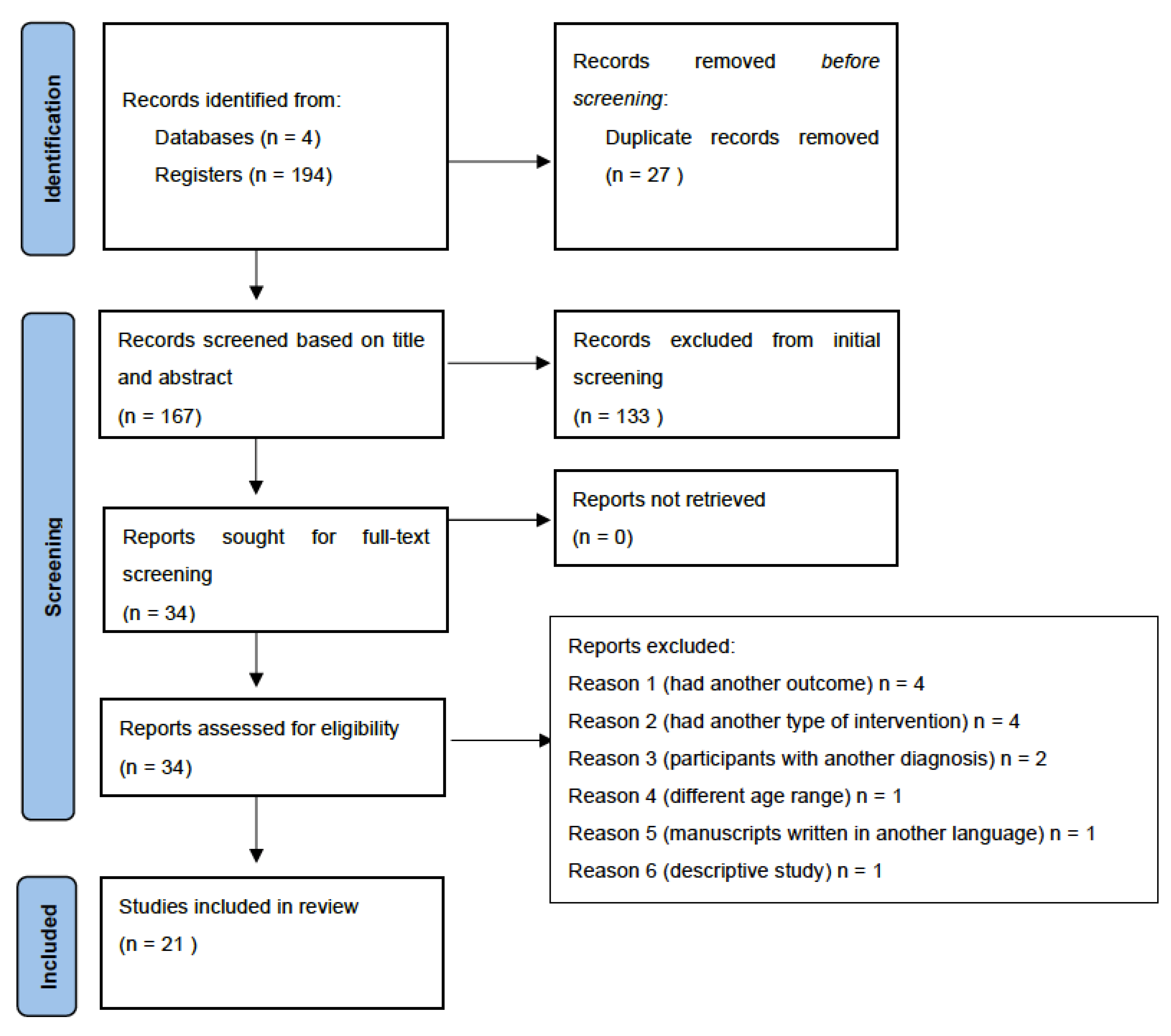
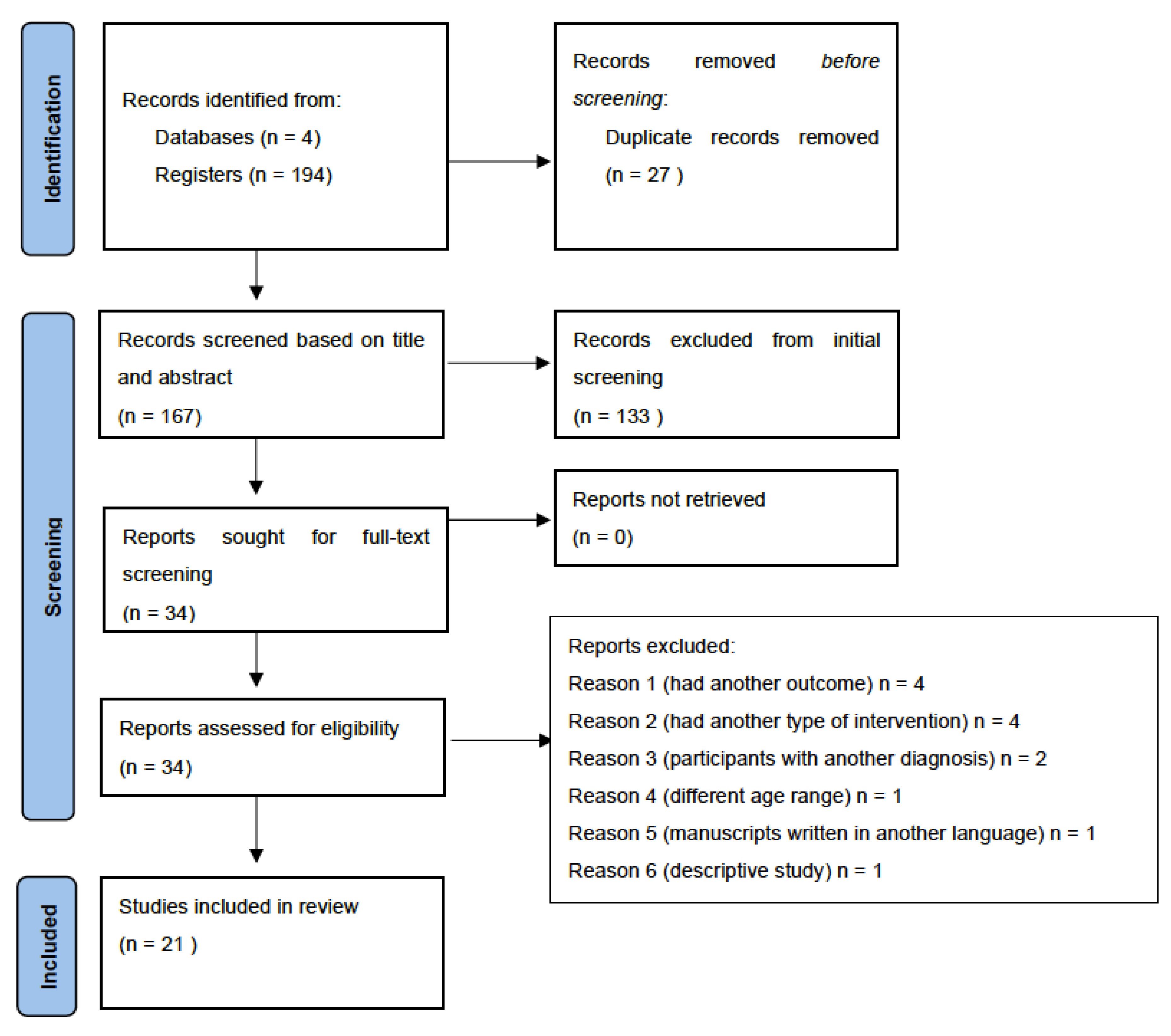
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Assessing the Quality of the Selected Articles
3. Results
3.1. Overall Results
3.2. Physical Activity and Executive Functions
3.3. Exercise and Executive Functions
3.4. Sport and Executive Functions
4. Discussion
4.1. Limitations
4.2. Future Implications
5. Conclusions
6. Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jönsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C.; et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [Green Version]
- Du Rietz, E.; Kuja-Halkola, R.; Brikell, I.; Jangmo, A.; Sariaslan, A.; Lichtenstein, P.; Kuntsi, J.; Larsson, H. Predictive validity of parent- and self-rated ADHD symptoms in adolescence on adverse socioeconomic and health outcomes. Eur. Child Adolesc. Psychiatry 2017, 26, 857–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibley, M.H.; Swanson, J.M.; Le Arnold Hechtman, L.T.; Owens, E.B.; Stehli, A.; Pelham, W.E. Defining ADHD symptom persistence in adulthood: Optimizing sensitivity and specificity. J. Child Psychol. 2017, 58, 655–662. [Google Scholar] [CrossRef]
- Panagiotidi, M.; Overton, P.; Stafford, T. The relationship between ADHD traits and sensory sensitivity in the general population. Compr. Psychiatry 2017, 80, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Krieger, V.; Amador-Campos, J.A. Assessment of executive function in ADHD adolescents: Contribution of performance tests and rating scales. Child Neuropsychol. 2018, 24, 1063–1087. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A. Activities and programs that improve children’s executive functions. Curr. Dir. Psychol. Sci. 2012, 21, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Hart, H.; Radua, J.; Nakao, T.; Mataix-Cols, D.; Rubia, K. Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: Exploring task-specific, stimulant medication, and age effects. JAMA Psychiatry 2013, 70, 185–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaughn, A.J.; Epstein, J.N.; Rausch, J.; Altaye, M.; Langberg, J.; Newcorn, J.; Hinshaw, S.P.; Hechtman, L.; Arnold, L.E.; Swanson, J.M.; et al. Relation between outcomes on a continuous performance test and ADHD symptoms over time. J. Abnorm. Child Psychol. 2011, 39, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Van-Meerbeke, A.; Zamora, I.; Guzmán, B.; López, C.; Talero-Gutierrez, C. Evaluación de la función ejecutiva en una población escolar con síntomas de déficit de atención e hiperactividad. Evaluation of executive function in a school population with symptoms of attention deficit and hyperactivity. Neurología 2013, 28, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.; Wilson, F.T.; Emslie, H. Detecting executive deficits in children with ADHD or acquired brain injury using the Behavioural Assessment of Dysexecutive Sndrome (BADS). Ir. J. Psychol. 2013, 34, 13–23. [Google Scholar] [CrossRef]
- Ferreiro-Vilasante, M.; Buceta-Cancela, M.J.; Rial-Boubeta, A. Comparación de la flexibilidad cognitiva en el TDAH y la dislexia. Infanc. Aprendiz. 2013, 36, 105–117. [Google Scholar] [CrossRef]
- Ramos-Loyo, J.; Taracena, A.M.; Sánchez-Loyo, L.M.; Matute, E.; González-Garrido, A.A. Relación entre el funcionamiento ejecutivo en pruebas neuropsicológicas y en el contexto social en niños con TDAH. Rev. Neuropsicol. Neuropsiquiatría Neurocienc. 2011, 11, 1–16. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=3640848 (accessed on 30 December 2021).
- Semrud-Clikeman, M.; Walkowiak, J.; Wilkinson, A.; Butcher, B. Executive functioning in children with Asperger syndrome, ADHD-combined type, ADHD-predominately inattentive type, and controls. J. Autism Dev. Disord. 2010, 40, 1017–1027. [Google Scholar] [CrossRef]
- Ng, Q.X.; Ho, C.Y.X.; Chan, H.W.; Yong, B.Z.J.; Yeo, W.S. Managing childhood and adolescent attention-deficit/hyperactivity disorder (ADHD) with exercise: A systematic review. Complement. Ther. Med. 2017, 34, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, L.; Beck, M.M.; Bilenberg, N.; Wienecke, J.; Astrup, A.; Lundbye-Jensen, J. Effects of Exercise on Cognitive Performance in Children and Adolescents with ADHD: Potential Mechanisms and Evidence-based Recommendations. J. Clin. Med. 2019, 8, 841. [Google Scholar] [CrossRef] [Green Version]
- Den Heijer, A.E.; Groen, Y.; Tucha, L.; Fuermaier, A.B.; Koerts, J.; Lange, K.W.; Thome, J.; Tucha, O. Sweat it out? The effects of physical exercise on cognition and behavior in children and adults with ADHD: A systematic literature review. J. Neural Transm. 2017, 124, 3–26. [Google Scholar] [CrossRef] [Green Version]
- Xue, J.; Zhang, Y.; Huang, Y. A meta-analytic investigation of the impact of mindfulness-based interventions on ADHD symptoms. Medicine 2019, 98, e15957. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.K.C.; Zhang, D.; Bögels, S.M.; Chan, C.S.; Lai, K.Y.C.; Lo, H.H.M.; Yip, B.H.K.; Lau, E.N.S.; Gao, T.T.; Wong, S.Y.S. Effects of a mindfulness-based intervention (MYmind) for children with ADHD and their parents: Protocol for a randomised controlled trial. BMJ Open 2018, 8, e022514. [Google Scholar] [CrossRef] [Green Version]
- Santonastaso, O.; Zaccari, V.; Crescentini, C.; Fabbro, F.; Capurso, V.; Vicari, S.; Menghini, D. Clinical Application of Mindfulness-Oriented Meditation: A Preliminary Study in Children with ADHD. Int. J. Environ. Res. Public Health 2020, 17, 6916. [Google Scholar] [CrossRef]
- Siebelink, N.M.; Kaijadoe, S.P.T.; van Horssen, F.M.; Holtland, J.N.P.; Bögels, S.M.; Buitelaar, J.K.; Speckens, A.E.M.; Greven, C.U. Mindfulness for Children with ADHD and Mindful Parenting (MindChamp): A Qualitative Study on Feasibility and Effects. J. Atten. Disord. 2021, 25, 1931–1942. [Google Scholar] [CrossRef] [PubMed]
- Palma, T.; Sepulveda, D.C.; Lorca, R.T.; Poblete-Aro, C.; Cadagan, C.; Castillo-Paredes, A. Cambios en los síntomas de inatención, hiperactividad e impulsividad en niños y adolescentes con TDAH mediante los Deportes. Una revisión (Changes in the symptoms of inattention, hyperactivity and impulsivity in children and adolescents with ADHD through. Retos 2021, 41, 701–707. [Google Scholar] [CrossRef]
- Castillo-Paredes, A.; Montalva, F.; Nanjarí, R. Actividad Física, Ejercicio Físico y Calidad de Vida en niños y adolescentes con Trastorno por déficit de atención y/o hiperactividad. Rev. Habanera Cienc. Méd. 2021, 20, e3714. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1729-519X2021000500017&lng=es&tlng=es (accessed on 30 December 2021).
- Veldhuijzen, J.J.; Rouse, P.C.; Hale, E.D. Perceived barriers, facilitators and benefits for regular physical activity and exercise in patients with rheumatoid arthritis: A review of the literature. Sports Med. 2015, 45, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Gapin, J.; Etnier, J.L. The relationship between physical activity and executive function performance in children with attention-deficit hyperactivity disorder. J. Sport Exerc. Psychol. 2010, 32, 753–763. [Google Scholar] [CrossRef] [Green Version]
- Pan, C.-Y.; Chu, C.-H.; Tsai, C.-L.; Lo, S.-Y.; Cheng, Y.-W.; Liu, Y.-J. A racket-sport intervention improves behavioral and cognitive performance in children with attention-deficit/hyperactivity disorder. Res. Dev. Disabil. 2016, 57, 1–10. [Google Scholar] [CrossRef]
- McMorris, T.; Hale, B.J. Differential effects of differing intensities of acute exercise on speed and accuracy of cognition: A meta-analytical investigation. Brain Cogn. 2012, 80, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Cerrillo-Urbina, A.J.; Garcia-Hermoso, A.; Sanchez-Lopez, M.; Pardo-Guijarro, M.J.; Santos, J.L.; Martinez-Vizcaino, V. The effects of physical exercise in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis of randomized control trials. Child Care Health Dev. 2015, 41, 779–788. [Google Scholar] [CrossRef] [Green Version]
- Grassmann, V.; Alves, M.V.; Santos-Galduroz, R.F.; Galduroz, J.C. Possible cognitive benefits of acute physical exercise in children with ADHD. J. Atten. Disord. 2017, 21, 367–371. [Google Scholar] [CrossRef]
- Berger, N.A.; Müller, A.; Brähler, E.; Philipsen, A.; de Zwaan, M. Association of symptoms of attention-deficit/hyperactivity disorder with symptoms of excessive exercising in an adult general population sample. BMC Psychiatry 2014, 14, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wigal, S.B.; Emmerson, N.; Gehricke, J.G.; Galassetti, P. Exercise: Applications to childhood ADHD. J. Atten. Disord. 2013, 17, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Cascaes, S.F.; Valdivia, A.B.A.; da Rosa, I.R. Escalas y listas de evaluación de la calidad de estudios científicos. Rev. Cuba. Inf. Cienc. Salud 2013, 24, 295–312. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S2307-21132013000300007 (accessed on 30 December 2021).
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Herbert, R.; Moseley, A.; Sherrington, C.; Maher, C. Physiotherapy Evidence Database. Physiotherapy 2000, 86, 55. [Google Scholar] [CrossRef]
- Benzing, V.; Schmidt, M. The effect of exergaming on executive functions in children with ADHD: A randomized clinical trial. Scand. J. Med. Sci. Sports 2019, 29, 1243–1253. [Google Scholar] [CrossRef]
- Ziereis, S.; Jansen, P. Effects of physical activity on executive function and motor performance in children with ADHD. Res. Dev. Disabil. 2015, 38, 181–191. [Google Scholar] [CrossRef]
- Piepmeier, A.T.; Shih, C.H.; Whedon, M.; Williams, L.M.; Davis, M.E.; Henning, D.A.; Etnier, J.L. The effect of acute exercise on cognitive performance in children with and without ADHD. J. Sport Health Sci. 2015, 4, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Miklós, M.; Komáromy, D.; Futó, J.; Balázs, J. Acute Physical Activity, Executive Function, and Attention Performance in Children with Attention-Deficit Hyperactivity Disorder and Typically Developing Children: An Experimental Study. Int. J. Environ. Res. Public Health 2020, 17, 4071. [Google Scholar] [CrossRef]
- Gawrilow, C.; Stadler, G.; Langguth, N.; Naumann, A.; Boeck, A. Physical activity, affect, and cognition in children with symptoms of ADHD. J. Atten. Disord. 2016, 20, 151–162. [Google Scholar] [CrossRef]
- Benzing, V.; Chang, Y.K.; Schmidt, M. Acute physical activity enhances executive functions in children with ADHD. Sci. Rep. 2018, 8, 12382. [Google Scholar] [CrossRef] [Green Version]
- Ludyga, S.; Brand, S.; Gerber, M.; Weber, P.; Brotzmann, M.; Habibifar, F.; Pühse, U. An event-related potential investigation of the acute effects of aerobic and coordinative exercise on inhibitory control in children with ADHD. Dev. Cogn. Neurosci. 2017, 28, 21–28. [Google Scholar] [CrossRef]
- Memarmoghaddam, M.; Torbati, H.T.; Sohrabi, M.; Mashhadi, A.; Kashi, A. Effects of a selected exercise programon executive function of children with attention deficit hyperactivity disorder. J. Med. Life 2016, 9, 373–379. Available online: https://pubmed.ncbi.nlm.nih.gov/27928441/ (accessed on 30 December 2021).
- Silva, A.P.; Prado, S.O.; Scardovelli, T.A.; Boschi, S.R.; Campos, L.C.; Frère, A.F. Measurement of the effect of physical exercise on the concentration of individuals with ADHD. PLoS ONE 2015, 10, e0122119. [Google Scholar] [CrossRef]
- Chou, C.C.; Huang, C.J. Effects of an 8-week yoga program on sustained attention and discrimination function in children with attention deficit hyperactivity disorder. PeerJ 2017, 5, e2883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.K.; Hung, C.L.; Huang, C.J.; Hatfield, B.D.; Hung, T.M. Effects of an aquatic exercise program on inhibitory control in children with ADHD: A preliminary study. Arch. Clin. Neuropsychol. 2014, 29, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.K.; Song, J.; Park, J.H. Effects of combination exercises on electroencephalography and frontal lobe executive function measures in children with ADHD: A pilot study. Biomed Res. 2017, 455–460. Available online: https://www.alliedacademies.org/articles/effects-of-combination-exercises-on-electroencephalography-and-frontal-lobe-executive-function-measures-in-children-with-adhd-a-pi.pdf (accessed on 30 December 2021).
- Chang, Y.K.; Liu, S.; Yu, H.H.; Lee, Y.H. Effect of acute exercise on executive function in children with attention deficit hyperactivity disorder. Arch. Clin. Neuropsychol. 2012, 27, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Pontifex, M.B.; Saliba, B.J.; Raine, L.B.; Picchietti, D.L.; Hillman, C.H. Exercise improves behavioral, neurocognitive, and scholastic performance in children with attention-deficit/hyperactivity disorder. J. Pediatr. 2013, 162, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, C.L.; Huang, C.J.; Tsai, Y.J.; Chang, Y.K.; Hung, T.M. Neuroelectric and behavioral effects of acute exercise on task switching in children with attention-deficit/hyperactivity disorder. Front. Psychol. 2016, 7, 1589. [Google Scholar] [CrossRef] [Green Version]
- Durgut, E.; Orengul, A.C.; Algún, Z.C. Comparison of the effects of treadmill and vibration training in children with attention deficit hyperactivity disorder: A randomized controlled trial. NeuroRehabilitation 2020, 47, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Ludyga, S.; Gerber, M.; Mücke, M.; Brand, S.; Weber, P.; Brotzmann, M. The acute effects of aerobic exercise on cognitive flexibility and task-related heart rate variability in children with ADHD and healthy controls. J. Atten. Disord. 2020, 24, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.S.; Ho, C.S. Reaction performance improvement in children with ADHD through adapted physical Activity—A pilot study. Ger. J. Sports Med./Dtsch. Z. 2021, 72, 21–27. [Google Scholar] [CrossRef]
- Kadri, A.; Slimani, M.; Bragazzi, N.L.; Tod, D.; Azaiez, F. Effect of taekwondo practice on cognitive function in adolescents with attention deficit hyperactivity disorder. Int. J. Env. Res. Public Health 2019, 16, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, C.Y.; Tsai, C.L.; Chu, C.H.; Sung, M.C.; Huang, C.Y.; Ma, W.Y. Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: A pilot study. J. Atten. Disord. 2019, 23, 384–397. [Google Scholar] [CrossRef]
- Crova, C.; Struzzolino, I.; Marchetti, R.; Masci, I.; Vannozzi, G.; Forte, R.; Pesce, C. Cognitively challenging physical activity benefits executive function in overweight children. J. Sports Sci. 2014, 32, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yu, Q.; Li, Z.; Cunha, P.M.; Zhang, Y.; Kong, Z.; Lin, W.; Chen, S.; Cai, Y. Effects of Acute and Chronic Exercises on Executive Function in Children and Adolescents: A Systemic Review and Meta-Analysis. Front Psychol. 2020, 11, 3482. [Google Scholar] [CrossRef]
- Ishihara, T.; Sugasawa, S.; Matsuda, Y.; Mizuno, M. Relationship between sports experience and executive function in 6–12-year-old children: Independence from physical fitness and moderation by gender. Dev Sci. 2018, 21, e12555. [Google Scholar] [CrossRef]

{kind=link}
| Authors | Criteria | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total | |
| Benzing et al., 2019 | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Ziereis & Jansen, 2015 | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Piepmeier et al., 2015 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Miklós et al., 2020 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Gawrilow et al., 2016 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Benzing et al., 2018 | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Ludyga et al., 2017 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Memarmoghaddam et al., 2016 | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Silva et al., 2015 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Chang et al., 2014 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Chou & Huang, 2017 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Lee et al., 2017 | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Chang et al., 2012 | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Pontifex et al., 2013 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Hung et al., 2016 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Durgut et al., 2020 | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Ludyga et al., 2020 | Y | Y | N | Y | N | Y | Y | Y | Y | Y | Y | 8 |
| Chan & Ho, 2021 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Pan et al., 2016 | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Kadri et al., 2019 | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Pan et al., 2015 | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Subjects | Objective | Intervention Type | |
|---|---|---|---|
| Benzing et al., 2019 | 51 subjects (82.4% boys and 17.6% girls aged 8 to 12 years). | Investigate the effects of cognitively and physically demanding exergaming on executive function | Physical activity |
| Exercise = 28 (10.46 ± 1.30) | |||
| Control = 23 (10.39 ± 1.44) | |||
| Ziereis & Jansen, 2015 | 43 subjects (32 boys and 11 girls aged 7 to 12 years). | Determine whether physical activity improves cognitive performance in children with ADHD | Physical activity |
| Experimental Group 1 = 13 (9.2 ± 1.3) | |||
| Experimental Group 2 = 14 (9.6 ± 1.6) | |||
| Control Group = 16 (9.5 ±1.4) | |||
| Piepmeier et al., 2015 | 32 adolescents (female gender 12 and male gender 20, 10.75 ± 2.27 years) | Examine the effect of acute exercise on cognitive performance by children with and without ADHD | Physical activity |
| ADHD group = 14 (10.14 ± 1.96 years) | |||
| Non-ADHD group = 18 (11.22 ± 2.43 years) | |||
| Miklós et al., 2020 | 150 children aged 6–12 years. | Examine the effects of an intense exercise on attention and executive function | Physical activity |
| Non-medicated group = 50 (25 exercise and 25 control). | |||
| Medicated group = 50 (25 exercise and 25 control). | |||
| Control group = 50 (25 exercise and 25 control). | |||
| Gawrilow et al., 2016 | 47 boys | Investigate the effects of a single bout of physical activity on cognitive functioning in children with ADHD | Physical activity |
| (8.3 to 13.6 years) | |||
| (M = 10.47; SD = 1.49) | |||
| Benzing et al., 2018 | 46 children ADHD Exergaming = 24 Control = 22 | Investigate the effects of an acute bout of physical activity on multiple aspects of executive functions in children with ADHD | Physical activity |
| 8–12 years (82.6% boys) | |||
| Ludyga et al., 2017 | 36 subjects (11 to 16 years) | Investigate the acute effects of aerobic exercise and coordinative exercise on inhibitory control in children with ADHD | Exercise |
| ADHD = 18 (7 girls and 11 boys) | |||
| Control = 18 (8 girls and 10 boys) | |||
| Memarmoghaddam et al., 2016 | 36 male students (7 to 11 years) | Examine the effectiveness of a Selected exercise program on the executive function of children with ADHD | Exercise |
| PA group = 19 (8.31 ± 1.29) | |||
| Control Group = 17 (8.29 ± 1.31) | |||
| Silva et al., 2015 | 56 volunteers aged 10–16 years. | Quantify the effect of physical activity on the attention of children with ADHD | Exercise |
| CG = 28 subjects without ADHD. | |||
| SG = 28 subjects with ADHD and no medication (30 remained). | |||
| Chou & Huang, 2017 | 49 participants (38 boys and 11 girls, 10.50 ± 1.05 years). | Investigated whether a yoga exercise intervention influenced the sustained attention and discrimination function in children with ADHD | Exercise |
| Exercise group = 24 (19 boys and 5 girls, 10.71 ± 1.00 years). | |||
| Control group = 25 (19 boys and 6 girls, 10.30 ± 1.07 years) | |||
| Chang et al., 2014 | 27 participants aged 5 to 10 years (23 boys and 4 girls, 8.44 ± 8.29) | Examine whether an aquatic exercise intervention influences restraint inhibition in children with ADHD | Exercise |
| Exercise group = 14 (10 boys and 4 girls, 8.19 ± 7.65 years). | |||
| Control group = 13 (13 children, 8.78 ± 8.33 years). | |||
| Lee et al., 2017 | 12 children | Investigate the effects of exercise on neuropsychological variables of executive function with electroencephalography in children with ADHD | Exercise |
| CEG = 6 (8.83 ± 0.98 years) | |||
| NEG = 6 (8.83 ± 0.98 years) | |||
| Chang et al., 2012 | 40 Children | Determine the effect of acute aerobic exercise on executive function in children with ADHD | Exercise |
| (3 girls y 37 boys, 8–13 years) | |||
| Pontifex et al., 2013 | ADHD Group = 20 (6 females), age 8–10 | Examine the effects of a single bout of aerobic exercise on the inhibitory control deficits in children with ADHD | Exercise |
| Healthy Group = 20 children (6 females), age 9.8 ± 0.1 | |||
| Hung et al., 2016 | 34 children with ADHD (1 female) | Examined the effects of an acute aerobic exercise session on task switching in children with ADHD | Exercise |
| aged 10.16 ± 1.74 | |||
| Durgut et al., 2020 | 30 children ADHD | Compare the effects of Treadmill Training and Whole-body Vibration Training on attention and quality of life in children with ADHD. | Exercise |
| age between 7–11 years | |||
| Ludyga et al., 2020 | Children ADHD = 18 | Investigate cognitive flexibility and task-related heart rate variability following moderately intense aerobic exercise and after watching a video in both children with ADHD and healthy controls | Exercise |
| Healthy peers = 18 | |||
| age between 11–16 years | |||
| Chan et al., 2021 | 37 children ADHD | Investigate the efficacy of an adapted physical activity program on reaction performance in children with ADHD | Exercise |
| aged 8–11 years | |||
| Pan et al., 2016 | 32 children (6 to 12 years). | Examine the effects of a racket-sport intervention on executive functions, motor skills, and social behaviors | Sports |
| Group, I = 16 children (8.93 ± 1.49) | |||
| Group II = 16 children (8.87 ± 1.56) | |||
| Kadri et al., 2019 | 40 young people (36 males and 4 females). | Investigate the effects of a one-and-a-half-year-long Taekwondo (TKD) intervention on cognitive function in adolescents with ADHD | Sports |
| TKD group = 20 (14.5 ± 3.5 years, 18 males and two females). | |||
| Control group = 20 (14.2 ± 3.0 years, 18 males and two females). | |||
| Pan et al., 2019 | ADHD training = 15 | Examined the effects a 12-week Table Tennis exercise on motor skills and executive functions in children with ADHD | Sports |
| ADHD non-training = 15 | |||
| TD children without ADHD non-training = 30 | |||
| All groups age 7–12 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montalva-Valenzuela, F.; Andrades-Ramírez, O.; Castillo-Paredes, A. Effects of Physical Activity, Exercise and Sport on Executive Function in Young People with Attention Deficit Hyperactivity Disorder: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 61-76. https://doi.org/10.3390/ejihpe12010006
Montalva-Valenzuela F, Andrades-Ramírez O, Castillo-Paredes A. Effects of Physical Activity, Exercise and Sport on Executive Function in Young People with Attention Deficit Hyperactivity Disorder: A Systematic Review. European Journal of Investigation in Health, Psychology and Education. 2022; 12(1):61-76. https://doi.org/10.3390/ejihpe12010006
Chicago/Turabian StyleMontalva-Valenzuela, Felipe, Oscar Andrades-Ramírez, and Antonio Castillo-Paredes. 2022. "Effects of Physical Activity, Exercise and Sport on Executive Function in Young People with Attention Deficit Hyperactivity Disorder: A Systematic Review" European Journal of Investigation in Health, Psychology and Education 12, no. 1: 61-76. https://doi.org/10.3390/ejihpe12010006
APA StyleMontalva-Valenzuela, F., Andrades-Ramírez, O., & Castillo-Paredes, A. (2022). Effects of Physical Activity, Exercise and Sport on Executive Function in Young People with Attention Deficit Hyperactivity Disorder: A Systematic Review. European Journal of Investigation in Health, Psychology and Education, 12(1), 61-76. https://doi.org/10.3390/ejihpe12010006