Abstract
Introduction: Studies on the prevalence of and risk factors for tuberculosis (TB) among newly diagnosed human immunodeficiency virus (HIV)-infected children in sub-Saharan Africa are scarce and in Nigeria there is paucity of reported data. We determined the prevalence of and risk factors for pulmonary TB (PTB) in newly diagnosed (treatment-naïve) HIV-1 infected children at the pediatric HIV clinic of the Jos University Teaching Hospital (JUTH) in Nigeria. Methods: We performed a retrospective analysis of 876 children, aged 2 months – 13 years, diagnosed with HIV-1 infection between July 2005 and December 2012, of which 286 were diagnosed with PTB at presentation after TB screening. The study site was the AIDS Prevention Initiative in Nigeria (APIN)-supported Pediatric HIV clinic at JUTH, Jos. A multivariate forward logistic regression modelling was used to identify risk factors for PTB-HIV co-infection. Results: The prevalence of PTB-HIV co-infection was 32% (286/876). Severe immunosuppression (SI) and World Health Organization (WHO) HIV clinical stage 3/4 were identified as independent risk factors for PTB-HIV co-infection in HIV infected children. The odds of PTB-HIV co-infection was increased two-fold in HIV-infected children with WHO clinical stage 3/4 compared to those with stage 1/2 (adjusted odds ratio (AOR) 1.76 [1.31-2.37], p<0.001) and 1.5-fold in children with SI compared to those without SI (AOR 1.52 [1.12-2.06], p=0.007). Conclusions: In our setting, the burden of PTB was high among newly diagnosed HIV-infected children, and late WHO HIV clinical stage and severe immunosuppression were associated with PTB-HIV co-infection. Therefore there is a clear need to improve strategies for early diagnosis of both HIV and PTB to optimize clinical outcomes.
Introduction
Of the estimated 34 million people living with human immunodeficiency virus (HIV) infection worldwide, at least one-third of them are also deemed to be co-infected with Mycobacterium tuberculosis (M. tuberculosis) [1]. These dual epidemics of HIV and tuberculosis (TB) are particularly worse in Africa, where HIV infection has been the most important factor contributing to the increasing incidence of TB over the last decade [1]. The incidence of TB among newly diagnosed HIV-infected children varies from 0.61 per 100 child-years (and a prevalence of 3%) in low burden countries like the United States [2] to 53.3 per 100 patient-years in high burden countries like South Africa [3].
Data on the incidence or prevalence of and risk factors for TB among children newly diagnosed with HIV in sub-Saharan Africa are scarce [3,4,5,6]. In Nigeria, the prevalence of pulmonary TB (PTB) in HIV-infected children and the predisposing risk factors are poorly described. Therefore, such a description would be useful in highlighting the burden of PTB-HIV co-infection in children, and in developing prevention strategies to protect HIV infected children from co-infection with M. tuberculosis.
In this study, we determined the prevalence of and risk factors for PTB in newly diagnosed HIV-1 infected children, prior to commencing anti-retroviral treatment (ART), at the pediatric HIV clinic of the Jos University Teaching Hospital (JUTH) in Jos, Nigeria.
Methods
Study design
This was a retrospective analysis of data on 876 children diagnosed with HIV-1 infection between July 2005 and December 2012, some of whom were also found to have PTB at presentation.
Study subjects
These were children, aged 2 months – 13 years diagnosed with HIV-1, of which some were diagnosed with PTB at initial presentation after TB screening, prior to commencing anti-retroviral therapy (ART).
Study setting
The site of this study was the AIDS Prevention Initiative in Nigeria (APIN)-supported Pediatric HIV clinic at JUTH, Jos. This clinic provides comprehensive HIV care services for the city of Jos, which is located in the Jos North Local Government Area (LGA) of Plateau State. The clinic serves as a referral center for both health facilities in the other LGAs of the state and some neighboring states in the country. Plateau State has a population of about 3,206,531 with the state capital having a population of approximately 900,000 [7].
Source of data
Patient data were obtained from an electronic medical records system (EMRS), data having been entered into the EMRS from paper-based records that were completed at the point of care. The data obtained were baseline data at the time of patient enrollment into care and included the following variables: demographic (age, sex), clinical (height, weight, World Health Organization (WHO) HIV clinical stage, oral thrush, diagnosis of PTB) and laboratory (hemoglobin (Hb) level, viral load and absolute CD4+ cell count).
Study procedure
Children diagnosed with HIV (at our HIV clinic or referred from other health facilities), were screened for PTB.
All children had laboratory tests performed as part of routine clinical care. For HIV serodiagnosis, children aged 18 months and above had two different rapid HIV tests – Uni-Gold (Trinity Biotech Plc Bray Co., Wicklow, Ireland) and Determine (Determine Alere Medical Co. Ltd., Matsuhidai, Japan) HIV-1/2 tests. For those under 18 months of age, Roche Cobas Amplicor HIV-1 DNA PCR test, version 1.5 (Roche Molecular Systems, Branchburg, NJ, USA) was used for diagnosing HIV infection. The CD4+ lymphocyte count was measured using flow cytometry (Partec GmbH, Munster, Germany) and HIV-1 RNA viral load was measured using Roche Cobas Amplicor HIV-1 Monitor, version 1.5 (Roche Diagnostics GmbH, Mannheim, Germany).
The diagnosis of HIV was based on the Nigerian National Guidelines for Pediatric HIV and AIDS Treatment and Care [8]. The diagnosis of PTB at the time of presentation was based on Nigeria National Guidelines [9] which include clinical, chest radiograph features, sputum or gastric aspirate smear microscopy and history of TB contact for children with HIV.
Operational definitions
In our study, a child with a combination of clinical features and chest radiograph suggestive of PTB with or without sputum or gastric aspirate smear positive microscopy was classified as having PTB [9] and a child with both PTB and HIV at the time of HIV diagnosis was considered a case of PTB-HIV co-infection [9]. The clinical features of PTB include: chronic cough ≥ 2 weeks, progressive weight loss or failure to thrive, fever, poor appetite, night sweats, reduced playfulness or fatigue, wasting, pallor, and chest signs. Smear positive microscopy refers to Ziehl-Neelsen staining for presence of acid-fast bacilli (AFB) on light microscopy. Thus, a PTB case was either a clinically diagnosed PTB case (not smear positive) or bacteriologically confirmed PTB case (smear positive).
A WHO weight-for-age Z score (WAZ) of < -3 was considered as severe malnutrition [10]; the Z-scores adjusted for age and sex were determined from subjects’ weight and height using the WHO AnthroPlus software (WHO, Geneva, Switzerland) [11]. Severe immunosuppression (SI) was determined from the absolute CD4+ cell count using the CDC definition for SI in children < 13 years [12] as follows: counts of <750/cmm for children <1 year, 500/cmm for those one to five years and <200/cmm for those >5 years. Anemia as defined by the WHO referred to Hb < 8 g/dL [13].
Statistical analysis
PTB-HIV co-infection was the outcome variable and all other variables were independent variables. Z-scores were categorized into a binary variable using the WHO Z score cut-off of <-3 for severe malnutrition. The variable hemoglobin was also categorized into a binary variable using the WHO cut-off of Hb <8 g/dL for anemia.
The association between each independent variable and PTB-HIV co-infection was initially examined using the Chi squared or Fisher’s exact test for categorical variables while the Wilcoxon-Mann-Whitney test was used for variables that were not normally distributed. Univariate and multivariate logistic regression models were fitted to determine the risk factors for PTB-HIV co-infection. For the multivariate model, a forward step-wise modeling strategy was used where variables with p<0.05 remained in the model and those with p>0.10 exited the model, at each step of the modeling process. Sex and age were included a priori in the multivariate model due to the association of these variables with a wide range of health parameters [14,15]. Results were expressed as odds ratios (ORs) with their 95% confidence intervals (CIs). All analyses were performed using Stata software version 10.0 (Stata Corporation, College Station, Texas, USA) and all tests were two-sided, with a p-value of <0.05 considered statistically significant.
Ethical approval
The parents/guardians of the children gave written informed consent for use of the data for this research which was approved by the Ethics committee of the Jos University Teaching Hospital, AIDS Prevention Initiative in Nigeria (APIN) Ltd, Abuja and Harvard T.H. Chan School of Public Health, Boston, USA.
Results
Out of 876 HIV-1 infected children, 286 were diagnosed with PTB within the study period (2005-2012) giving an overall PTB-HIV co-infection prevalence of 32.6%. There was a significant decline in the prevalence of co-infection over the years, with the prevalence being 46.5% (86/185) in 2006 and 6.1% (4/66) in 2012, p<0.001. A test for trend showed declining number of cases of co-infection over time from 2005 to 2012, p<0.001 (Figure 1).
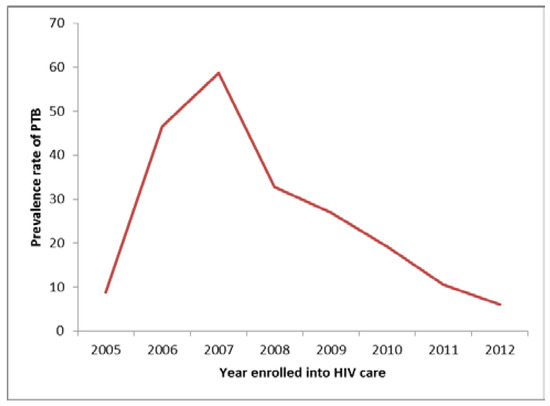
Figure 1.
Trend in the prevalence of PTB-HIV co-infection among children over a period of 8 years (2005-2012).
In the entire cohort of 876 children, the majority were males (52.5%), ≤ 5 years of age (67.7%), and were enrolled during the first four years (2005-2008) of starting the pediatric HIV care programme (59.3%). Most of them were in WHO clinical stage 1/2 (56.3%) and only a few had common clinical manifestations such as oral thrush (3%), severe malnutrition (26.3%), anemia (6.2%) or severe immunodeficiency (35.7%). Their median and interquartile range (IQR) CD4+ cell count was 535 (298-890) cells/cmm, viral load 44026 (6037-200377) copies/mL and log viral load 10.7 (8.7-12.2) copies/mL (Table 1).

Among patients with PTB-HIV co-infection, there were significantly more children in WHO clinical stage 3/4 compared to stage 1/2 (53.6% versus 46.5%, p<0.001) and with severe immunosuppression compared to those without severe immunosuppression (57.7% versus 42.3%, p=0.005). The median (IQR) CD4+ cell count was significantly lower in children with PTB co-infection than in those with HIV infection alone (484 cells/cmm (308-755) versus 558/cmm (293-953), p=0.020) (Table 1). The number and proportion of children with PTB-HIV co-infection presenting with advanced HIV infection (WHO clinical stage 3/4) declined significantly over the years (2005-2012), p=0.019.
In the unadjusted logistic regression analyses, WHO clinical stage 3/4 and presence of severe immunosuppression were significantly associated with PTB-HIV co-infection with ORs being 1.8 and 1.52 respectively. The odds of co-infection decreased by 0.01% for every unit increase in absolute CD4+ cell count, p=0.002 (Table 2).

Multivariate logistic regression analyses showed that the risk of having PTB-HIV co-infection was two-fold higher in children with WHO clinical stage 3/4 compared to those with stage 1/2, p<0.001 and 1.5-fold higher in those with severe immunosuppression compared to those without severe immunosuppression, p=0.007.
Discussion
The overall prevalence of PTB-HIV co-infection was 32.6% in our cohort of children and the risk factors for co-infection were WHO clinical stage 3/4 and severe immunosuppression.
The prevalence of PTB-HIV co-infection for our study was high; this could be expected since Nigeria is both a high burden TB and a high HIV prevalence country [16]. Our high PTB-HIV co-infection prevalence figure of 32.6% suggests a high rate of co-infection, comparable to the high burden in South Africa, where an incidence figure of TB-HIV co-infection of 53.3 per 100 patient years was reported in children [3]. The rates of PTB-HIV co-infection among children in Nigeria and South Africa contrasts with the lower prevalence rate of 3% for a low burden country like the United States [2]. Our PTB diagnosis was based in most cases (about 70%) on clinical and chest radiograph features without bacteriological confirmation, which may have overestimated the number of PTB cases. But this alone cannot explain our observed overall high prevalence, since a Ugandan study reported a lower prevalence compared to our study, 9.5%, although the majority of diagnoses (80%) were based on clinical features and chest radiograph, like in our study [5]. Nevertheless, our observed annual prevalence of co-infection was decreasing, with the rate in 2012 of 6.1% comparable to that of the Ugandan study (9.5%) reported in 2011 [5]. The diagnosis of PTB in children remains challenging, partly due to the inability of children ≤ 8 years to generate a productive sputum specimen [17] and because of their paucibacillary nature [18]. The majority (70%) of our study subjects were children ≤ 5 years of age. Thus, in typical HIV care and treatment settings in Africa, our methods of PTB diagnosis would be considered more representative since routine sputum or gastric aspirate smear microscopy is uncommon. The PTB-HIV co-infection prevalence rate of 32.6% that we obtained was far higher than the prevalence rate of 9.6% we earlier reported in adults in the same APIN HIV clinic study site [19] in which diagnosis was based on a positive smear microscopy. Again, this difference could be attributed to differences in diagnostic criteria, with a possible over-diagnosis of PTB in children compared to adults.
We observed a declining prevalence rate of PTB-HIV co-infection from 46.5% in 2006 to 6.1% in 2012. This decline appears to closely mirror the declining prevalence rate of HIV vertical transmission from 4.4% in 2005 [20] to 3.2% in 2015 [21] in Nigeria. Also, the decline may be due to the global increase in HIV awareness and increasingly early diagnosis of HIV in children. We recently reported a very low rate of 0.7% mother-to-child HIV transmission [22] in this same study site as our present study, which would seem to suggest a decline in the number of pediatric HIV cases, thus paralleling a decline in PTB-HIV co-infection cases.
Our results showed that children with WHO HIV clinical stage 3/4 were at greater risk for PTB-HIV co-infection than those with HIV stage 1/2. WHO clinical stage 3/4 indicates advanced and severe HIV disease which predisposes to opportunistic infections, the most common in children being tuberculosis. A study in children from Côte d’Ivoire similarly showed that HIV stage 3/4 was a risk factor for co-infection [4]. In our study, severe immunosuppression was an important risk factor for PTB-HIV co-infection. This finding is consistent with those of other studies in African children [4,5,23]. Severe immunosuppression in TB-HIV co-infection has largely been attributed to CD4+ T-cell depletion [24,25]. Severe immunosuppression in children with HIV mono-infection or HIV-TB co-infection has been associated with poor clinical outcomes and increased mortality with or without ART [26,27,28,29,30]. Also, co-infection with HIV and TB increases the risk of death with or without ART [5,28,29].
A limitation of this study was our inability to routinely provide bacteriological confirmation of PTB in most cases, resulting in a possible overestimation of the number of PTB cases and hence a higher prevalence of PTB-HIV co-infection. However, it is well-recognized that bacteriological confirmation is often difficult in pediatric populations.
Conclusions
In our setting, the burden of PTB was high among newly diagnosed HIV-infected children, and late WHO HIV clinical stage and severe immunosuppression were associated with PTB-HIV co-infection. Therefore there is a clear need to improve strategies for early diagnosis of both HIV and PTB to optimize clinical outcomes.
Author Contributions
AOE contributed to study design, statistical analysis and drafting of the manuscript. AOE, SO, EUE, OOA, NYS, IOA, ASS, POU, PIO, JAI, PJK contributed to data acquisition and interpretation, as well as critical revision for intellectual content. All authors reviewed and approved the final version of the manuscript.
Funding
This publication was facilitated, in part, by: the US Department of Health and Human Services, Health Resources and Services Administration (U51HA02522- 01-01) and the Centers for Disease Control and Prevention (PS 001058) which supported HIV/AIDS treatment and care services at APIN, JUTH, Jos; and the Medical Education Partnership Initiative in Nigeria (MEPIN) project funded by the National Institute of Health, the Health Resources and Services Administration (HRSA) and the Office of the U.S. Global AIDS Coordinator under award R24TW008878. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding organizations.
Acknowledgments
We thank APIN, JUTH for permission to use the patients’ data.
Conflicts of Interest
All authors – none to declare.
References
- USAID. The Twin Epidemics: HIV and TB Co-Infection; United States Agency for International Development: Washington, DC, USA, 2014. Available online: https://www.usaid.gov/news-information/fact-sheets/twin-epidemics-hiv-and-tb-co-infection (accessed on 8 September 2015).
- Thomas, P.; Bornschlegel, K.; Singh, T.P.; et al. Tuberculosis in human immunodeficiency virus-infected and human immunodeficiency virus-exposed children in New York City. The New York City Pediatric Spectrum of HIV Disease Consortium. Pediatr Infect Dis J 2000, 19, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Walters, E.; Cotton, M.F.; Rabie, H.; Schaaf, H.S.; Walters, L.O.; Marais, B.J. Clinical presentation and outcome of tuberculosis in human immunodeficiency virus infected children on anti-retroviral therapy. BMC Pediatr 2008, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Auld, A.F.; Tuho, M.Z.; Ekra, K.A.; et al. Tuberculosis in human immunodeficiency virus-infected children starting antiretroviral therapy in Côte d’Ivoire. Int J Tuberc Lung Dis 2014, 18, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Bakeera-Kitaka, S.; Conesa-Botella, A.; Dhabangi, A.; et al. Tuberculosis in human immunodeficiency virus infected Ugandan children starting on antiretroviral therapy. Int J Tuberc Lung Dis 2011, 15, 1082–1086. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Okechukwu, A.A.; Okechukwu, O.I. Clinical correlate of tuberculosis in HIV co-infected children at the University of Abuja Teaching Hospital, Gwagwalada, Nigeria. Niger J Clin Pract 2011, 14, 206–211. [Google Scholar] [CrossRef] [PubMed]
- National Population Commission. Population Distribution by Sex, State, LGA & Senatorial District. 2006 Population and Housing Census: Priority Table Volume III. National Population Commission, of Abuja, Nigeria. Available online: http://catalog.ihsn.org/index.php/catalog/3340/download/48521 (accessed on 26 August 2015).
- Federal Ministry of Health. National Guidelines for Paediatric HIV and AIDS Treatment and Care; Federal Ministry of Health: Abuja, Nigeria, 2010; Available online: http://preventcrypto.org/wp-content/uploads/2015/10/NigeriaPaediatricARTguidelines20101369045239.pdf (accessed on 28 February 2016).
- Federal Ministry of Health. National Tuberculosis and Leprosy Control Programme—Workers’ Manual, 5th ed.; Federal Ministry of Health: Abuja, Nigeria; Department of Public Health, 2010; Available online: http://www.who.int/hiv/pub/guidelines/nigeria_tb.pdf (accessed on 26 August 2014).
- World Health Organization (WHO). Global Database on Child Growth and Malnutrition; World Health Organization: Geneva, Switzerland; Available online: http://www.who.int/nutgrowthdb/about/introduction/en/index5.html (accessed on 20 April 2014).
- World Health Organization (WHO). Application Tools: WHO AnthroPlus Software; World Health Organization: Geneva, Switzerland; Available online: http://www.who.int/growthref/tools/en/ (accessed on 21 April 2014).
- Centers for Disease Control and Prevention (CDC). 1994 Revised classification system for human immunodeficiency virus infection in children less than 13 years of age; Official authorized addenda: Human immunodeficiency virus infection codes and official guidelines for coding and reporting ICD-9-CM. MMWR Morb Mortal Wkly Rep 1994, 43, 1–19. [Google Scholar]
- World Health Organization (WHO). Iron Deficiency Anaemia: Assessment, Prevention and Control; World Health Organization: Geneva, Switzerland, 2001; Available online: http://www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/WHO_NHD_01.3/en/ (accessed on 26 August 2014)A Guide for Program Managers.
- Holmes, C.B.; Hausler, H.; Nunn, P. A review of sex differences in the epidemiology of tuberculosis. Int J Tuberc Lung Dis 1998, 2, 96–104. [Google Scholar] [PubMed]
- Bellamy, R.; Beyers, N.; McAdam, K.P.; et al. Genetic susceptibility to tuberculosis in Africans: A genome-wide scan. Proc Natl Acad Sci USA 2000, 97, 8005–8009. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Tuberculosis Control 2015; World Health Organization: Geneva, Switzerland, 2015; Available online: www.who.int/tb/publications/global_report (accessed on 8 September 2015).
- Graham, S.M.; Coulter, J.B.; Gilks, C.F. Pulmonary disease in HIV-infected African children. Int J Tuberc Lung Dis 2001, 5, 12–23. [Google Scholar] [PubMed]
- Ruiz Jiménez, M.; Guillén Martín, S.; Prieto Tato, L.M.; et al. Induced sputum versus gastric lavage for the diagnosis of pulmonary tuberculosis in children. BMC Infect Dis 2013, 13, 222. [Google Scholar] [CrossRef] [PubMed]
- Agbaji, O.; Ebonyi, A.O.; Meloni, S.T.; et al. Factors associated with pulmonary tuberculosis-HIV co-infection in treatment-naive adults in Jos, North Central Nigeria. J AIDS Clin Res 2013, 4, 1000222. [Google Scholar]
- United Nations General Assembly Special Session Country Progress Report, Nigeria. 2010. Available online: http://data.unaids.org/pub/Report/2010/nigeria_2010_country_progress_report_en.pdf (accessed on 28 February 2016).
- UNAIDS. HIV and AIDS Estimates; UNAIDS: Geneva, Switzerland, 2014; Available online: http://www.unaids.org/en/regionscountries/countries/nigeria/ (accessed on 21 November 2015).
- Sagay, A.S.; Ebonyi, A.O.; Meloni, S.T.; et al. Mother-to-child transmission outcomes of HIV-exposed infants followed up in Jos, North-Central Nigeria. Curr HIV Res 2015, 13, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Braitstein, P.; Nyandiko, W.; Vreeman, R.; et al. The clinical burden of tuberculosis among human immunodeficiency virus-infected children in Western Kenya and the impact of combination antiretroviral treatment. Pediatr Infect Dis J 2009, 28, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Geldmacher, C.; Zumla, A.; Hoelscher, M. Interaction between HIV and Mycobacterium tuberculosis: HIV-1-induced CD4 T-cell depletion and the development of active tuberculosis. Curr Opin HIV AIDS 2012, 7, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Naing, C.; Mak, J.W.; Maung, M.; Wong, S.F.; Kassim, A.I. Meta-analysis: The association between HIV infection and extrapulmonary tuberculosis. Lung 2013, 191, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Ebonyi, A.O.; Oguche, S.; Ejeliogu, E.U.; et al. Risk factors for first-line antiretroviral treatment failure in HIV-1 infected children attending Jos University Teaching Hospital, Jos, North Central Nigeria. Br J Med Med Res 2014, 4, 2983–2994. [Google Scholar] [CrossRef][Green Version]
- Bolton-Moore, C.; Mubiana-Mbewe, M.; Cantrell, R.A.; et al. Clinical outcomes and CD4 cell response in children receiving antiretroviral therapy at primary health care facilities in Zambia. JAMA 2007, 298, 1888–1899. [Google Scholar] [CrossRef] [PubMed]
- Raguenaud, M.E.; Isaakidis, P.; Zachariah, R.; et al. Excellent outcomes among HIV+ children on ART, but unacceptably high pre-ART mortality and losses to follow-up: A cohort study from Cambodia. BMC Pediatr 2009, 9, 54. [Google Scholar] [CrossRef] [PubMed]
- Yotebieng, M.; Van Rie, A.; Moultrie, H.; et al. Effect on mortality and virological response of delaying antiretroviral therapy initiation in children receiving tuberculosis treatment. AIDS 2010, 24, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Buck, W.C.; Olson, D.; Kabue, M.M.; et al. Risk factors for mortality in Malawian children with human immunodeficiency virus and tuberculosis co-infection. Int J Tuber Lung Dis 2013, 17, 1389–1395. [Google Scholar] [CrossRef] [PubMed]

© GERMS 2016.