Abstract
Introduction: In low- and middle-income countries including Nepal, respiratory tract infection (RTI) is considered as one of the most prominent public health problems in children. Multiple carriage of respiratory pathogens is common in children, especially in preschoolers as they are easily transmitted through close contact and poor hygienic condition. Thus, this research is based on the study of prevalence, co-existence, associated factors and antibiogram of nasal isolates among healthy preschoolers. Methods: The study was conducted in four randomly selected kindergarten schools (two government run and two private run) of Bhaktapur Municipality. Out of a total 140 students, 136 eligible participants of age group 2–5 years old were involved in the study. Nasal swab was collected for the isolation of five target isolates (Staphylococcus aureus, Streptococcus pneumoniae, Moraxella catarrhalis, Haemophilus influenzae and Haemophilus parainfluenzae) and their antibiotic resistance determination. Results: Of 136 participants involved, 128 (94.5%) were positive for carriage of at least one of the target bacteria. The most common isolate was M. catarrhalis 62.5% (80/128) followed by S. aureus 43.0% (55/128). There was a significant difference in bacterial carriage with respect to type of school (p value < 0.05, OR = 0.50, CI = 0.20–0.90). Regarding bacterial co-existence, the most common co-existence was of S. aureus and M. catarrhalis & S. pneumoniae and M. catarrhalis 48.8%. Multiple logistic regression analysis showed that S. aureus was negatively associated with S. pneumoniae, M. catarrhalis and H. influenzae and S. pneumoniae was positively associated with M. catarrhalis and H. influenzae. Multidrug resistance was seen in 63 isolates (29.4%). Conclusions: Nepalese kindergarten children are at a high risk of respiratory tract infection by multidrug resistant bacteria.
Introduction
Acute respiratory infections (ARIs) in children prominently lead to infectious disease, higher hospitalization, and morbidity rate worldwide [1]. Respiratory tract infections can be broadly divided into upper respiratory tract infections (URTIs) and lower respiratory tract infections (LRTIs). Here, URTIs include mainly tonsillitis, pharyngitis, rhinitis, laryngitis, sinusitis and otitis media [2] whereas LRTIs include bronchitis, bronchiolitis and pneumonia [3]. According to Global Burden of Disease (GBD) 2019, the prevalence rate of URTIs has outnumbered 17.2 (95% confidence interval (CI) 15.4 to 19.3) billion, accounting for almost half, 42.8% (40.0% to 45.8%), of the cases from all causes of disease with children under five years old suffering from the highest incidence [4]. For the same age group, LRTIs caused 808,920 deaths (95% CI 747,286–873,591) in 2017 [5]. This increasing prevalence of respiratory infections among children younger than 5 years has largely affected the public health and increased the economic burden, particularly in low income [6] and developing countries [7].
The human nasopharyngeal microbiota acts as a reservoir for a multitude of bacteria, some of which can become pathogenic (Streptococcus pneumoniae, Moraxella catarrhalis, Haemophilus influenzae and Staphylococcus aureus) and cause acute otitis media, pneumonia, bacteremia and meningitis [8]. Carriage or asymptomatic colonization by these bacteria initiates local and systemic infection [9] causing increased morbidity and mortality rates among children in the worst scenario [10]. M. catarrhalis, along with S. pneumoniae and H. influenzae, comprised the top three bacterial pathogens responsible for community-acquired respiratory infections [11]. A study in Nepal showed Moraxella spp. (45.5%) and S. pneumoniae (16.6%) as the two most common bacterial pathogens isolated, followed by S. aureus (14.7%), H. influenzae (3.4%) and Haemophilus parainfluenzae (2.4%) [12]. Likewise, S. pneumoniae and H. influenzae are the commonest cause of pneumonia, meningitis, and other serious infections in children [13]. Pneumococcal infections can progress to invasive pneumococcal disease (IPD) and respiratory tract infections [14]. Globally, this kills nearly half a million children under 5 years old every year, most of those deaths occurring in developing countries [15].
Colonization and transmission of nasal pathogens can be affected by various factors, such as age, the existence of prior respiratory infection, history of antimicrobial use, and hygienic practices. Multiple carriage of respiratory pathogens is common in children, especially in kindergartens as they get easily transmitted through close contact and poor hygienic condition [12,16]. They usually carry drug-resistant pathogens, particularly in this prevailing stage of antimicrobial overuse or misuse in children. Most cases of colonization remain asymptomatic, but the bacteria can become invasive in susceptible hosts [16]. On 18th January 2015, the National Immunization Programme (NIP) in Nepal introduced a new vaccine, pneumococcal conjugate vaccine (PCV) against 10 serotypes of S. pneumoniae in regular basis in infants following three doses at 6 weeks, 10 weeks and 9 months. Simultaneously, with the aid from the Global Alliance for Vaccines and Immunization, Hib vaccine was first introduced in Nepal in 2009 [17].
In a nutshell, in low- and middle-income countries including Nepal, respiratory tract infection is considered as one of the prominent public health problems as there are advancing cases of severe mortality and morbidity in children [18]. Most of the studies focus on detection and prevalence of one or two nasal carriages. Little is known about bacterial pathogens and co-existence of nasal carriage bacteria in Nepalese children. Thus, this study investigated the nasal carriage of five common bacterial pathogens (S. pneumoniae, H. influenzae, H. parainfluenzae, M. catarrhalis and S. aureus) in healthy school going children in Bhaktapur Municipality.
Methods
Study design and site
This descriptive cross-sectional study was conducted in four randomly selected kindergarten schools (two government and two private) of Bhaktapur Municipality from May 2018 to November 2018. This Municipality lies in Province no. 3, about 13 km east from the capital city Kathmandu with the total area of 6.88 km2. It has warm temperate climate ranging from -3 °C to 35 °C and is 1401 m above the sea level (latitude: 27.673, longitude: 85.4279, North 27 40′ 23″ and East 85 25′ 40″).
Bhaktapur Municipality lies in the smallest district of Nepal, Bhaktapur district owing its main economic base to agriculture and tourism while other people engage in local handicraft production and business, pottery work and public services. According to the National Census 2011, Bhaktapur has a population of 3,04,651, out of which 0–14 years age-group bears 24.8%. The annual population growth rate is 2.9%; the average life expectancy is 70.9 years and the literacy rate is 81.7%. It has a human development indicator of 0.625 while human poverty indicator, gender development indicator and human empowerment indicators are 27.9, 0.587 and 0.685, respectively [19].
Study population
A total of 136 eligible participants from the age group 2–5 years old were involved in the study. An informed written consent along with pre-set questionnaires comprising demographic information, respiratory health status, immune status, antibiotic consumption up to a week prior to sampling and overall health condition were provided to the guardian two days before the sample collection. On the day of sampling, both the informed written consent and the questionnaires answered by the guardian himself/herself were collected.
Inclusion and exclusion criteria
- Inclusion criteria
- Primarily, children aged 2–5 years old fulfilling health-related criteria mentioned in the questionnaire and most importantly with signed consent.
- Exclusion criteria
- Participants with acute respiratory infections (presence of two or more signs or symptoms such as fever, runny nose or nasal congestion, cough, or sore throat) [20], with any sort of respiratory tract infection or nasal abscesses, with immune-compromised state, those unwilling to participate and those without consent, were excluded.
Sample collection and processing
Nasal swab collection was performed as per CDC guideline [21]. A specimen was collected from both nostrils using the same swab. All samples were labelled properly, transported and processed in the laboratory of Janamaitri Institution of Health Sciences, Balaju, Kathmandu within half an hour of collection. The specimen was inoculated in the respective selective media for the isolation and identification of the target organism and incubated at 37 °C for 48 hrs. Selective media for S. pneumoniae was Columbia blood agar (CBA) (HiMedia, India) with gentamicin (10 mcg), for S. aureus mannitol salt agar (MSA) (HiMedia, India), for M. catarrhalis blood agar (BA) base (HiMedia, India) and deoxyribonuclease (DNase) agar (HiMedia, India) and for H. influenzae and H. parainfluenzae chocolate agar (CA) (HiMedia, India) with bacitracin (10 units) in candle jar.
Bacterial isolation and characterization
The colonies on the plates were examined for their identification via colony morphology, Gram staining followed by microscopic examination and a series of biochemical tests as per the Clinical and Laboratory Standards Institute (CLSI) guideline [22]. Identification of S. aureus was performed through colony morphology in mannitol salt agar, presence of β-hemolysis, catalase and coagulase tests. Identification of S. pneumoniae was done studying its colony morphology in Columbia blood agar with gentamicin, optochin susceptibility test, presence of α-hemolysis and catalase test. Similarly, H. influenzae and H. parainfluenzae were identified viewing colony morphology in chocolate agar with bacitracin (10 units), utilization of X (hemin), V (NAD) and X + V factors and catalase test. Further, M. catarrhalis was identified through colony morphology in blood agar, DNase and oxidase test.
Antimicrobial susceptibility test
The antimicrobial susceptibility test of four bacterial isolates was performed as per CLSI guideline [22] via Kirby Bauer disk diffusion method in Muller Hinton agar (HiMedia, India). The antibiotic sensitivity of isolates was examined using amoxicillin (10 μg), amoxicillin/clavulanic acid (amoxyclav) (30 μg), ceftriaxone (30 μg), chloramphenicol (30 μg), ciprofloxacin (5 μg), co-trimoxazole (1.25 μg), erythromycin (15 μg), gentamicin (10 μg), levofloxacin (5 μg) (HiMedia, India). S. aureus was further examined for methicillin resistance (MRSA) using cefoxitin (30 μg).
Statistical analysis
Statistical Package for the Social Sciences (IBM Corp., USA) version 21 was employed for encoding and analyzing the data. Chi-square test was used for comparison of presence of organism with its categorical variables. For the evaluation of association between demographic characteristics and bacterial co-existence, the multiple logistic regression model was used with significant level p < 0.05.
Ethical clearance
To conduct this study, approval was taken from the selected schools and written consent was taken from the guardians of the participants. Also, this study was approved by Nepal Health Research Council (NHRC), Reference number 3135, Kathmandu, Nepal.
Results
Demographic study and the prevalence of the target bacterial pathogens among participants
Of the total 136 participants engaged in the study, 81 (59.6%) were male whereas 55 (40.4%) were female. The mean age of the study participants was 3.2 years. The number of students from government schools were 87 (64.0%) and from private schools 49 (36.0%).
Of 136 participants involved, 128 (94.5%) of them were positive for carriage of at least one of the target bacteria and 70 (51.5%) were positive for ≥2 bacterial species’ carriage. The most common isolate was M. catarrhalis 62.5% (80/128), followed by S. aureus 60.9% (78/128), S. pneumoniae 42.9% (55/128) and H. influenzae 0.8% (1/128). Single and multiple bacterial carriages decreased with increasing age except for S. aureus, the carriage of which increased with age as shown in Table 1.

Table 1.
Prevalence of each target bacteria among n = 128 participants positive for carriage of at least one of the target bacteria.
Independent variables and distribution of bacterial carriage
As shown in Table 2, there was a significant relation (p value <0.05, OR = 0.50, CI = 0.20–0.90) between bacterial carriage with respect to type of school i.e., government or private school, where higher single and multiple carriage was seen in children from government schools. Besides that, there was no significant difference between bacterial carriage and independent variables. Here, the overall multiple carriage of target bacteria was lower in the oldest age group (5 years) compared to that in the youngest age group (2 years) (OR = 0.29, CI = 0.01–2.90) and similarly, the higher carrier of bacterial pathogens was seen in independent variables as in female, uneducated parents (both father and mother), in public school and Ward no. 7, the difference, however, was not statistically significant in each of the cases.
Table 2.
Independent variables and bacterial carriage with its odds ratio (OR).
Multiple logistic regression analysis of bacterial co-existence
According to the analysis, bacterial co-existence of both S. pneumoniae & M. catarrhalis and S. aureus & M. catarrhalis was calculated as 48.8% followed by S. aureus & S. pneumoniae 33.3%. Likewise, the triple colonization of S. aureus-S. pneumoniae-M catarrhalis was 11.7% followed by S. pneumoniae-M. catarrhalis-H. influenzae at 0.8%.
Multiple logistic regression analysis showed that S. aureus was negatively associated with S. pneumoniae, M. catarrhalis and H. influenzae. S. pneumoniae was positively associated with M. catarrhalis and H. influenzae but negatively with S. aureus. Likewise, M. catarrhalis was positively associated with S. pneumoniae & H. influenzae and negatively associated with S. aureus. H. influenzae was positively associated with S. pneumoniae & M. catarrhalis and negatively with S. aureus as shown in Table 3.
Table 3.
Multiple logistic regression analysis of bacterial co-existence.
Antimicrobial pattern of target carrier bacteria
Antimicrobial susceptibility testing results showed M. catarrhalis to be highly resistant to amoxicillin and least resistant to chloramphenicol. Likewise, S. aureus was most resistant to amoxicillin and least resistant to levofloxacin. Similarly, S. pneumoniae was most resistant to co-trimoxazole and least resistant to amoxicillin/clavulanate. And finally, H influenzae was resistant to none of the drugs tested. Multidrug resistance (MDR) was seen in 70 (32.7%) of the isolates. The details of the antibiogram of the isolates are depicted in Table 4. The prevalence of MRSA was 20.5%.
Table 4.
Antimicrobial resistance activity of target bacterial isolates.
Multidrug resistance in isolates
Out of the total MDR isolates, most (60.3%) were resistant to 2 classes of drugs and 1 (1.5%) isolate was resistant to all the 7 classes of drugs tested. S. aureus was seen to be the most versatile MDR bacteria as it exhibited drug resistance to the maximum number of classes of drugs. H. influenzae did not exhibit resistance to any drug class. The details of the MDR isolates are shown in Figure 1.
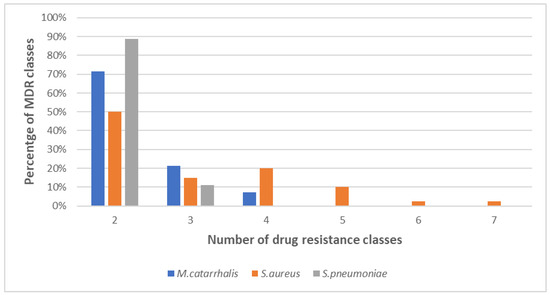
Figure 1.
Number of classes of drug resistance in multidrug-resistant (MDR) isolates.
Discussion
This study revealed that the target pathogens were seen in 94.5% of the participants. The highest carriage rate was of M. catarrhalis (62.5%), followed by S. aureus (60.9%), S. pneumoniae (42.9%) and H. influenzae (0.8%). The pattern of the global carriage rate of these bacteria, as reported by previous studies was found to be: M. catarrhalis (16–67%) [11,23,24,25,26,27,28], S. pneumoniae (10–69%) [11,23,25,27,28,29,30], S. aureus (10–50%) [11,23,25,27,28,31], H. parainfluenzae & H. influenzae (10–83%) [11,23,24,25,27,28]. The reason behind these large ranges in the prevalence of these bacteria is vague and poorly understood. Some previously published research, however, suggests that these discrepancies can be attributed to various factors like the time of study, geographical site, socio-economic conditions, number of siblings, hygiene status, vaccination against respiratory pathogens [11,31,32,33].
Of the target bacteria involved in our study, M. catarrhalis was found to be the most prevalent, with a carriage rate of 62.5%. A similar study done in another city of Nepal, Pokhara reported the carriage rate to be 45.5% [12]. This finding is lower than that revealed in China (76.6%) [16] and higher than that from Indonesia (42.7%) [11], while very low carriage was reported in Turkey (3.1%) [34]. M. catarrhalis is responsible for 10–20% of otitis media cases in children [35]. The difference in carriage rate is less understood, and some of the underlined factors have been explained earlier in the previous paragraph [4]. In an underdeveloped country like Nepal, very little published data is available regarding M. catarrhalis colonization in Nepalese children which makes it even more difficult in ascertaining the overall prevalence of this emerging pathogen in Nepalese children.
Likewise, S. aureus was the second most predominant bacterium found in our study. The carriage rate of this bacterium in this study was 60.9%, which is higher than that found in other countries like China (21.8%), India (35.0%) Brazil (48.0%) and Turkey (7.9%). [16,34,36,37] and the high prevalence found in our study in comparison to other countries might be attributed to factors like the temperate climatic conditions of the place of study, poor hygiene status, below par socio-economic conditions, poor nutritional status, etc. Colonization is seen to increase with increase in age, which can be explained owing to the fact that attending kindergarten schools or being in pre-school are factors associated with high S. aureus colonization [36]. Children are more commonly reported to be persistent carriers than adults, with the maximum rate of carriage in their first year of life followed by transition from persistent to intermittent or non-carriers during adolescence [38].
The prevalence rate of S. pneumoniae in this study was as high as 42.9%. This high prevalence can be attributed to the fact that this study was performed in 2018 and pneumococcal immunization had been started in the NIP only 3 years before, in January. Approximately 95% of children below the age of 3 years had full dosage of PCV10 while none of the children above 3 years were immunized against S. pneumoniae. Our finding is similar to the prevalence found in Ethiopia (43.8%) [39]. In contrast, lower prevalence was found in other countries like the Czech Republic (38.1%), and Romania (25.5%) and even lower prevalence was found in Turkey (14.0%) [25,40,41]. The reason for the low carriage rate in these countries may be due to the use of PCV13 vaccine that covers more serotypes than PCV7 and PCV10 vaccines [42]. PCV10 is the anti-pneumococcal vaccine that is being used in Nepal since January 2015 [17]. The existing high prevalence of S. pneumoniae might also indicate the need for introduction of PCV13. A study in Nepal regarding the reduction of pneumococcal carriage after the introduction of PCV10 indicated significant reduction of vaccine serotypes that cause the majority of invasive pneumococcal disease [43]. The high prevalence found in our study was due to the fact that our study detected all serotypes and also the subpopulation of children that were not immunized. Similar studies done in various countries of Asia have demonstrated that the carriage rate of S. pneumoniae ranged from 21.1% in China to 49.5% in Indonesia [11,16]. This disparity might be due to risk factors related to socio-economic status, exposure and presence of URTI symptoms, vaccine type, nutritional status and antibiotic prescription policies in children.
H. influenzae is an important cause of invasive bacterial disease in children worldwide [44]. The prevalence rate of this microorganism in our study was as low as 0.8%. Before the introduction of Hib vaccine in 2009, the prevalence of this bacterium was as high as 5% among children and since the introduction of the pentavalent diphtheria-tetanus-pertussis/Hib/hepatitis B (DTP-Hib-HepB) vaccine, the prevalence has reduced to being almost non-existent [45], while the global carriage rate ranges from 10% to 83% [23,24,25,27]. This low prevalence, hence, can be attributed to factors like vaccination coverage, colonization and antagonism by other common colonizers, environmental conditions etc. A similar low prevalence of 2.3% was reported in China [16]. Hib disease exists as an important infection in Asia, however, there has been uncertainty about the rates of disease caused by Hib in this part of the world, with some studies to have claimed it being as low as 0% to 1% after the introduction of routine infant immunization [46]. Nasal carriage of H. parainfluenzae was not detected in this study but other studies done in Nepal showed its prevalence to be 3.7% in children from the age group 5–9 years [12]. This low prevalence might be due to the factors similar to low prevalence of H. influenzae, as discussed earlier.
In general, the carriage of bacterial pathogens decreased with age in case of M. catarrhalis and S. pneumoniae [16], and this study also documented the same. The reason behind this might be the poor innate immunity and close peer contact among the lower age group children, owing to facts like higher occupancy of class rooms and more indoor activities conducted for children of the lower age groups, included in our study. In contrast, the carriage of S. aureus increased with age, as seen in this study, and also in those done in China and Indonesia [11,16]. Considering other variables, although there was no significant difference in the education level of parents in this study, other studies showed a positive relationship with multiple bacterial carriage in children, suggestive of finer hygiene knowledge from educated families [16]. Poor hygienic conditions could also associate a higher risk of bacterial carriage in the kindergarten children in this study.
Meanwhile, there was a significant difference in the bacterial carriage and multiple bacterial carriage between public and private schools, showing the highest prevalence of multiple carriage among public schools, supported by other studies conducted in Nepal and India [12,36]. where the prevalence rate was high in government schools, which may be due to high occupancy (mean occupancy 15.5 students in private schools vs 26.0 students per class in public schools) of the class, nutritional status and hygiene status.
Here, in this study, positive association was seen among S. pneumoniae and M. catarrhalis whilst S. aureus was negatively associated with S. pneumoniae and M. catarrhalis. Because only one isolate of H. influenzae was detected in our study, we could not estimate its positive/negative association with other isolates. A similar finding was reported in a study conducted in Indonesia, where positive associations were observed for S. pneumoniae with M. catarrhalis and H. influenzae with M. catarrhalis while M. catarrhalis and S. aureus were negatively associated [11]. Likewise, a study in South Africa also depicted a synergic relationship between S. pneumoniae and H. influenzae colonization and a negative association between S. pneumoniae and S. aureus, or H. influenzae and S. aureus colonization. The underlying biological mechanisms, however, are not well understood [47], with suggestions that interference between S. pneumoniae and S. aureus may result from hydrogen peroxide production by S. pneumoniae [48].
Conjugate pneumococcal vaccines reduce carriage of vaccine serotypes and can lead to replacement by non-vaccine serotypes resulting to alteration of carriage of other pathogens [49]. Likewise, competition between S. pneumoniae and S. aureus could suggest that pneumococcal vaccination is likely to increase S. aureus carriage. On the other hand, pneumococcal vaccination might reduce carriage of pathogens that benefit from pneumococcal colonization via synergistic interactions, and studies suggests that pneumococcal vaccination might minimize influenza-associated pneumonia [47].
The selection of antibiotics for susceptibility testing of the isolates was based on their common use in various sectors like medicine, veterinary and poultry by means of which they circulate in the society. When all isolates were considered, levofloxacin appeared to be the most efficient drug while erythromycin was the least efficient drug. The high susceptibility to levofloxacin complies to the fact that the use of this drug is not encouraged in children as it causes cartilage toxicity and that the bacterial flora in children has restricted exposure to it [50]. Meanwhile, erythromycin, a broad-spectrum antibiotic, is being over used commonly in various sectors like medicine, veterinary, poultry, etc., and as a result its resistance is evidently widespread [51]. In an under developed country like Nepal, the majority of hospitals still ignore a proper laboratory evidence-based drug prescription in treating bacterial diseases. Hence broad-spectrum antibiotics are generally used on empirical basis to treat most of the bacterial infections. In this regard the findings of our study suggest that such antibiotics comparatively are less effective against the isolates.
Multidrug resistance of the isolates is quite common in this study. Of the overall isolates, 29.4% were MDR. A maximum multidrug resistance of 63.5% was seen in S. aureus. Out of the total MDR strains, most of the isolates were resistant to two classes of drugs (60.3%) while 1 isolate of S. aureus was resistant to all the 7 classes of drugs tested, which was similar to findings in Nigeria where one S. aureus isolate with mecA gene exhibited extended drug resistance [52]. Children studying in public schools were shown to harbor a significantly higher number of isolates when compared to their counterparts studying in private schools, which can be explained owing to the fact that higher occupancy, better socio-economic conditions, better nutritional and hygiene status, as described earlier, are available to children going to private school.
Because this research was conducted within a limited financial resource, serotyping and other molecular studies to elucidate the mechanism of drug resistance could not be done. However, this is one of the very few kinds of studies done in an underdeveloped country like Nepal where antibacterial therapy is still practiced on empirical basis in the majority of cases. The findings of this study could be pivotal in guiding the stakeholders to take the necessary measures required to prevent the further damages than can possibly be caused by potential pathogens and MDR isolates in the especially vulnerable age group like children.
Conclusions
Kindergarten children, especially in a developing country like Nepal, are under an immense threat of respiratory tract infection as they harbor a plethora of potential bacterial pathogens. Moraxella catarrhalis was the most prevalent isolate. Single and multiple carriage decreased with age for other bacteria except for S. aureus. The carriage of S. pneumoniae is still high despite the introduction of PCV. Children studying in public schools harbored significantly higher single and multiple carriage. A positive association was seen among S. pneumoniae, and M. catarrhalis whilst S. aureus was negatively associated with these isolates. Broad-spectrum antibiotics are comparatively less effective against the isolates. A high prevalence of multidrug resistant pathogens as nasal microbiota has been detected. Hence, an immediate measure needs to be taken by the respective authority in order to prevent the further loss and hence ensure the children’s right to health, as promised by the Nation’s constitution.
Author Contributions
GP conceptualized and coordinated the study. GP and NA carried out the study design. GP, NA and BS were involved with the data collection. NA and BA carried out data entry and analysis. NA and SW prepared the initial manuscript draft. GP, NA, BS, SW and VS revised the manuscript and prepared the final draft. All authors read and approved the final version of the manuscript.
Funding
Financial support and the laboratory facility for this study was provided by Janamaitri Foundation Institute of Health Sciences, Kathmandu, Nepal. The funder had no role in other parts of the study like study design or data collection, analysis, interpretation, manuscript writing and submission for publication.
Acknowledgments
The authors acknowledge the support of all school principals, teaching and non-teaching staff, parents/guardians and participating children from all the study sites.
Conflicts of interest
All authors—none to declare.
References
- Assane, D.; Makhtar, C.; Abdoulaye, D.; et al. Viral and bacterial etiologies of acute respiratory infections among children under 5 years in Senegal. Microbiol Insights 2018, 11, 1178636118758651. [Google Scholar] [CrossRef]
- Thomas, M.; Bomar, P.A. Upper respiratory tract infection. In StatPearls; StatPearls Publishing: Treasure Islan, FL, 2021. [Google Scholar]
- Dasaraju, P.V.; Liu, C. Infections of the respiratory system. In Medical Microbiology, 4th ed.; Baron, S., Ed.; University of Texas Medical Branch at Galveston Galveston: TX, 1996. [Google Scholar]
- Jin, X.; Ren, J.; Li, R.; et al. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. EClinicalMedicine 2021, 37, 100986. [Google Scholar] [CrossRef]
- GBD 2017 Lower Respiratory Infections Collaborators. Quantifying risks and interventions that have affected the burden of lower respiratory infections among children younger than 5 years: An analysis for the Global Burden of Disease Study 2017. Lancet Infect Dis. 2020, 20, 60–79. [Google Scholar] [CrossRef]
- Tazinya, A.A.; Halle-Ekane, G.E.; Mbuagbaw, L.T.; Abanda, M.; Atashili, J.; Obama, M.T. Risk factors for acute respiratory infections in children under five years attending the Bamenda Regional Hospital in Cameroon. BMC Pulm Med. 2018, 18, 7. [Google Scholar] [CrossRef]
- Taylor, S.; Lopez, P.; Weckx, L.; et al. Respiratory viruses and influenza-like illness: Epidemiology and outcomes in children aged 6 months to 10 years in a multi-country population sample. J Infect. 2017, 74, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.F.; Parameswaran, G.I. Moraxella catarrhalis, a human respiratory tract pathogen. Clin Infect Dis. 2009, 49, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Siegel, S.J.; Weiser, J.N. Mechanisms of bacterial colonization of the respiratory tract. Annu Rev Microbiol. 2015, 69, 425–444. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.E.; Cleary, D.W.; Clarke, S.C. Secondary bacterial infections associated with influenza pandemics. Front Microbiol. 2017, 8, 1041. [Google Scholar] [CrossRef]
- Dunne, E.M.; Murad, C.; Sudigdoadi, S.; et al. Carriage of Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, and Staphylococcus aureus in Indonesian children: A cross-sectional study. PLoS ONE 2018, 14, e0195098. [Google Scholar] [CrossRef]
- Thapa, S.; Gokhale, S.; Sharma, A.L.; et al. Burden of bacterial upper respiratory tract pathogens in school children of Nepal. BMJ Open Respir Res. 2017, 4, e000203. [Google Scholar] [CrossRef]
- Wahl, B.; O’Brien, K.L.; Greenbaum, A.; et al. Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: Global, regional, and national estimates for 2000-15. Lancet Glob Health 2018, 6, e744–e757. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Factsheet About Pneumococcal Disease. Available online: https://www.ecdc.europa.eu/en/pneumococcal-disease/facts (accessed on 22 January 2022).
- Centers for Disease Control and Prevention. 2020. Global pneumococcal disease and vaccine. 2020. Available online: https://www.cdc.gov/ncird/ (accessed on 15 June 2021).
- Pan, H.; Cui, B.; Huang, Y.; Yang, J.; Ba-Thein, W. Nasal carriage of common bacterial pathogens among healthy kindergarten children in Chaoshan region, southern China: A cross-sectional study. BMC Pediatr. 2016, 16, 161. [Google Scholar] [CrossRef]
- Government of Nepal. Ministry of Health and Population. National Immunization Programme. Available online: https://mohp.gov.np/eng/program/child-health-services/nip (accessed on 15 June 2021).
- Bhatta, D.R.; Gokhale, S.; Sharma, A.L.; et al. Carrier state of Haemophilus influenzae type b (Hib), Streptococcus pneumoniae, Streptococcus pyogenes, Neisseria meningitidis and Corynebacterium diphtheriae among school children in Pokhara, Nepal. Asian Pacific J Trop Dis. 2014, 4, 45–49. [Google Scholar] [CrossRef]
- District Coordination Committee Office Bhaktapur, Nepal. Bhaktapur at a Glance. Available online: https://dccbhaktapur.gov.np/en/brief-introduction/ (accessed on 15 June 2020).
- Centers for Disease Control and Prevention. National Center for Immunization and Respiratory Diseases (NCIRD). 2017. Available online: https://www.cdc.gov/flu/about/glossary.htm (accessed on 20 June 2021).
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. 2000. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_01_02/specimen_collection_year_3.pdf (accessed on 20 June 2021).
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; Document M100-S10; CLSI: Wayne, PA, 2018. [Google Scholar]
- Liu, L.; Xie, W.; Chunmei, J. Survey of respiratory tract microbial population in children. Chin. J Microecol. 2007, 19, 22–26. [Google Scholar]
- Naaber, P.; Tamm, E.; Pütsepp, A.; Kõljalg, S.; Maimets, M. Nasopharyngeal carriage and antibacterial susceptibility of Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis in Estonian children. Clin Microbiol Infect. 2000, 6, 675–677. [Google Scholar] [CrossRef]
- Zemlicková, H.; Urbásková, P.; Adámková, V.; Motlová, J.; Lebedová, V.; Procházka, B. Characteristics of Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis and Staphylococcus aureus isolated from the nasopharynx of healthy children attending day-care centres in the Czech Republic. Epidemiol Infect. 2006, 134, 1179–1187. [Google Scholar] [CrossRef]
- Quiñones, D.; Llanes, R.; Toraño, G.; Pérez, M. Nasopharyngeal colonization by Moraxella catarrhalis and study of antimicrobial susceptibility in healthy children from Cuban day-care centers. Arch Med Res. 2005, 36, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Jourdain, S.; Smeesters, P.R.; Denis, O.; et al. Differences in nasopharyngeal bacterial carriage in preschool children from different socio-economic origins. Clin Microbiol Infect. 2011, 17, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Kovács, E.; Sahin-Tóth, J.; Tóthpál, A.; van der Linden, M.; Tirczka, T.; Dobay, O. Co-carriage of Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis among three different age categories of children in Hungary. PLoS ONE 2020, 15, e0229021. [Google Scholar] [CrossRef]
- Adegbola, R.A.; DeAntonio, R.; Hill, P.C.; et al. Carriage of Streptococcus pneumoniae and other respiratory bacterial pathogens in low and lower-middle income countries: A systematic review and meta-analysis. PLoS ONE 2014, 9, e103293. [Google Scholar] [CrossRef]
- Bae, S.; Yu, J.Y.; Lee, K.; Lee, S.; Park, B.; Kang, Y. Nasal colonization by four potential respiratory bacteria in healthy children attending kindergarten or elementary school in Seoul, Korea. J Med Microbiol. 2012, 51 Pt 5, 678–685. [Google Scholar] [CrossRef]
- Luo, X.; Liang, J.; Gao, S.; Li, Z.; Dong, Z.R. Surveys on bacteria nasopharyngeal carriage prevalence in 186 children. Chin. J Microecol. 2006, 18, 204–208. [Google Scholar]
- Littorin, N.; Rünow, E.; Ahl, J.; Resman, F.; Riesbeck, K. Decreased prevalence of Moraxella catarrhalis in addition to Streptococcus pneumoniae in children with upper respiratory tract infection after introduction of conjugated pneumococcal vaccine: A retrospective cohort study. Clin Microbiol Infect. 2021, 27, 630.e1–630.e6. [Google Scholar] [CrossRef]
- Cura Yayla, B.C.; Özsürekçi, Y.; Aykaç, K.; et al. Characteristics and management of children with COVID-19 in Turkey. Balk Med J. 2020, 37, 341–347. [Google Scholar] [CrossRef]
- Gönüllü, N.; Yıldız, S.; Aydoğan, O.; et al. Nasopharyngeal carriage of potential pathogenic bacteria in healthy children living in İstanbul. Med Bull Haseki. 2020, 58, 470–476. [Google Scholar] [CrossRef]
- Shaffer, T.L.; Balder, R.; Buskirk, S.W.; Hogan, R.J.; Lafontaine, E.R. Use of the Chinchilla model to evaluate the vaccinogenic potential of the Moraxella catarrhalis filamentous hemagglutinin-like proteins MhaB1 and MhaB2. PLoS ONE 2013, 8, e67881. [Google Scholar] [CrossRef]
- Pathak, A.; Marothi, Y.; Iyer, R.V.; et al. Nasal carriage and antimicrobial susceptibility of Staphylococcus aureus in healthy preschool children in Ujjain, India. BMC Pediatr. 2010, 10, 100. [Google Scholar] [CrossRef]
- Lamaro-Cardoso, J.; de Lencastre, H.; Kipnis, A.; et al. Molecular epidemiology and risk factors for nasal carriage of Staphylococcus aureus and methicillin-resistant S. aureus in infants attending day care centers in Brazil. J Clin Microbiol. 2009, 47, 3991–3997. [Google Scholar] [CrossRef]
- Brugger, S.D.; Frey, P.; Aebi, S.; Hinds, J.; Mühlemann, K. Multiple colonization with S. pneumoniae before and after introduction of the seven-valent conjugated pneumococcal polysaccharide vaccine. PLoS ONE 2010, 5, e11638. [Google Scholar] [CrossRef]
- Gebre, T.; Tadesse, M.; Aragaw, D.; et al. Nasopharyngeal carriage and antimicrobial susceptibility patterns of Streptococcus pneumoniae among children under five in Southwest Ethiopia. Children (Basel) 2017, 4, 27. [Google Scholar] [CrossRef]
- Luminos, M.; Dorobat, O.; Jugulete, G.; et al. Nasopharyngeal carriage of Streptococcus pneumoniae in Romanian children before the introduction of the pneumococcal conjugated vaccination into the national immunization programme: A national, multi-centre, cross-sectional observational study. Int J Infect Dis. 2014, 29, 169–173. [Google Scholar] [CrossRef][Green Version]
- Arvas, A.; Çokuğraş, H.; Gür, E.; Gönüllü, N.; Taner, Z.; Tokman, H.B. Pneumococcal nasopharyngeal carriage in young healthy children after pneumococcal conjugate vaccine in Turkey. Balk Med J. 2017, 34, 362–366. [Google Scholar] [CrossRef]
- Ordeno, J.M. Anti-pneumonia vaccine PCV13 ‘more superior’ than PCV10. Available online: https://www.gmanetwork.com/news/scitech/science/725651/anti-pneumonia-vaccine-pcv13-more-superior-than-pcv10-expert/story/ (accessed on 20 June 2021).
- Shrestha, B.; Thorson, S.; Gurung, M.; et al. Impact of PCV10 on nasopharyngeal carriage of Streptococcus pneumoniae in community children of Nepal. Pneumo Nepal Proj. 2017, 7, 1000348. [Google Scholar]
- Yang, Y.; Cheng, W.; Pan, X.; et al. Prevalence of Haemophilus influenzae type b infection in Chinese children: A systematic review and meta-analysis. Lancet 2017, 390, S42. [Google Scholar] [CrossRef]
- Shrestha, S.; Stockdale, L.K.; Gautam, M.C.; et al. Impact of vaccination on Haemophilus influenzae type b carriage in healthy children less than 5 years of age in an urban population in Nepal. J Infect Dis. 2021, 224 (Suppl. 3), 267–274. [Google Scholar] [CrossRef]
- Williams, E.J.; Lewis, J.; John, T.; et al. Haemophilus influenzae type b carriage and novel bacterial population structure among children in urban Kathmandu, Nepal. J Clin Microbiol. 2011, 49, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Dunne, E.M.; Smith-Vaughan, H.C.; Robins-Browne, R.M.; Mulholland, E.K.; Satzke, C. Nasopharyngeal microbial interactions in the era of pneumococcal conjugate vaccination. Vaccine 2013, 31, 2333–2342. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Trzcin, K.; Thompson, C.M.; Malley, R.; Lipsitch, M. Interference between Streptococcus pneumoniae and Staphylococcus aureus: In vitro hydrogen peroxide-mediated killing by Streptococcus pneumoniae. J Bacteriol. 2006, 188, 4996–5001. [Google Scholar] [CrossRef]
- Devine, V.T.; Jefferies, J.M.; Clarke, S.C.; Faust, S.N. Nasopharyngeal bacterial carriage in the conjugate vaccine era with a focus on pneumococci. J Immunol Res. 2015, 2015, 394368. [Google Scholar] [CrossRef]
- Bradley, J.S.; Kauffman, R.E.; Balis, D.A.; et al. Assessment of musculoskeletal toxicity 5 years after therapy with levofloxacin. Pediatrics 2014, 134, e146–e153. [Google Scholar] [CrossRef]
- University of Minnesota. Antimicrobial resistance learning site. Antibiotics in veterinary medicine. Available online: https://amrls.umn.edu/antibiotics-veterinary-medicine (accessed on 27 January 2022).
- Onanuga, A.; Adamu, O.J.; Odetoyin, B.; Hamza, J.A. Nasal carriage of multi-drug resistant Panton Valentine leukocidin positive Staphylococcus aureus in healthy individuals of Tudun-Wada, Gombe State, Nigeria. Afr J Infect Dis. 2020, 15, 24–33. [Google Scholar] [CrossRef] [PubMed]





© GERMS 2022.