
Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice




Abstract
1. Introduction
2. Materials and Methods
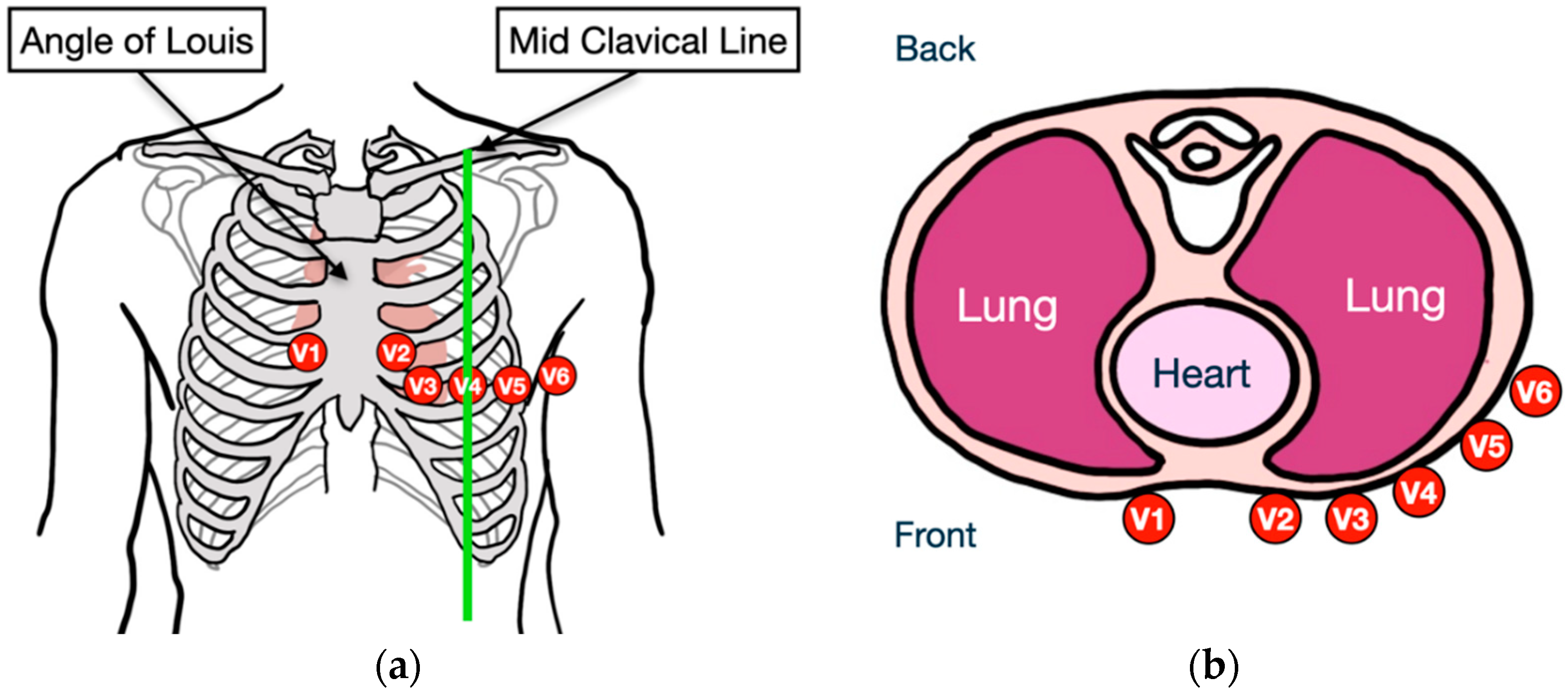
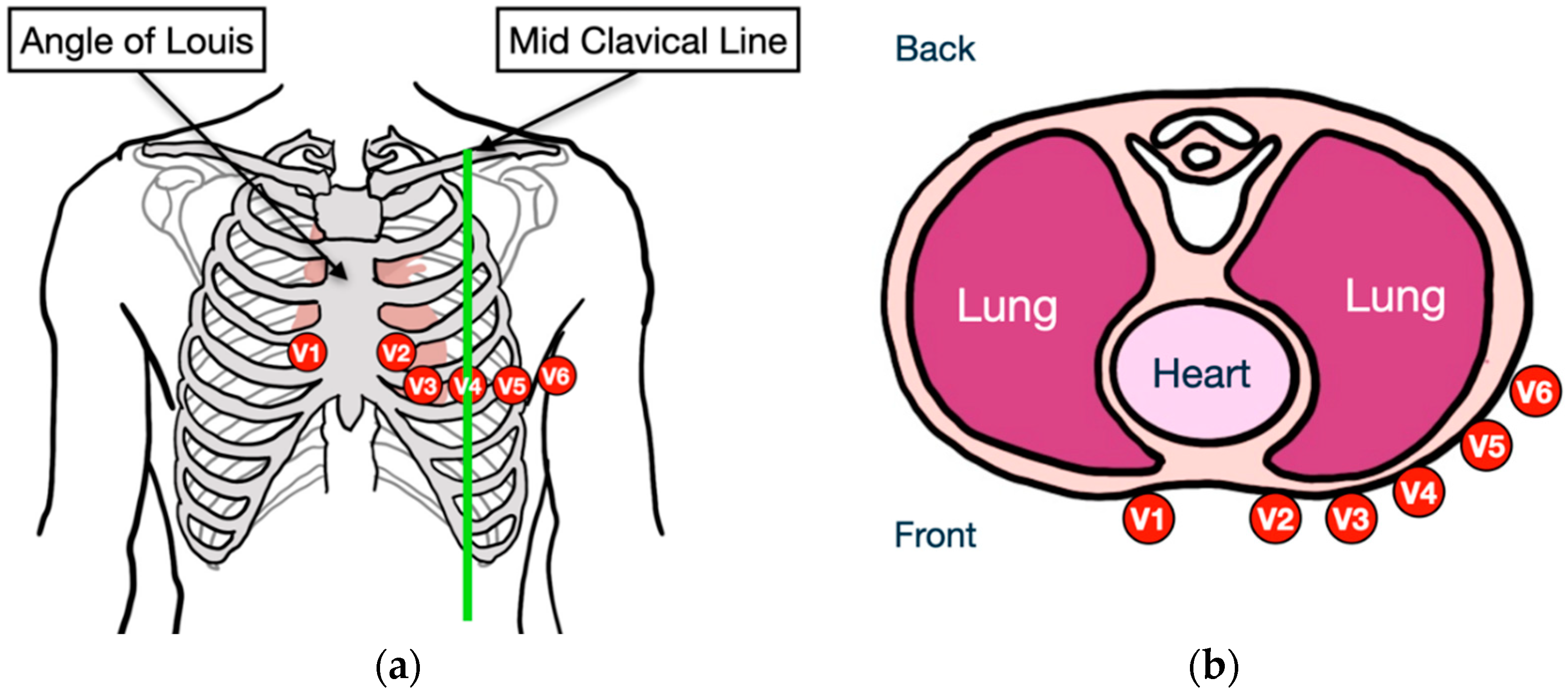
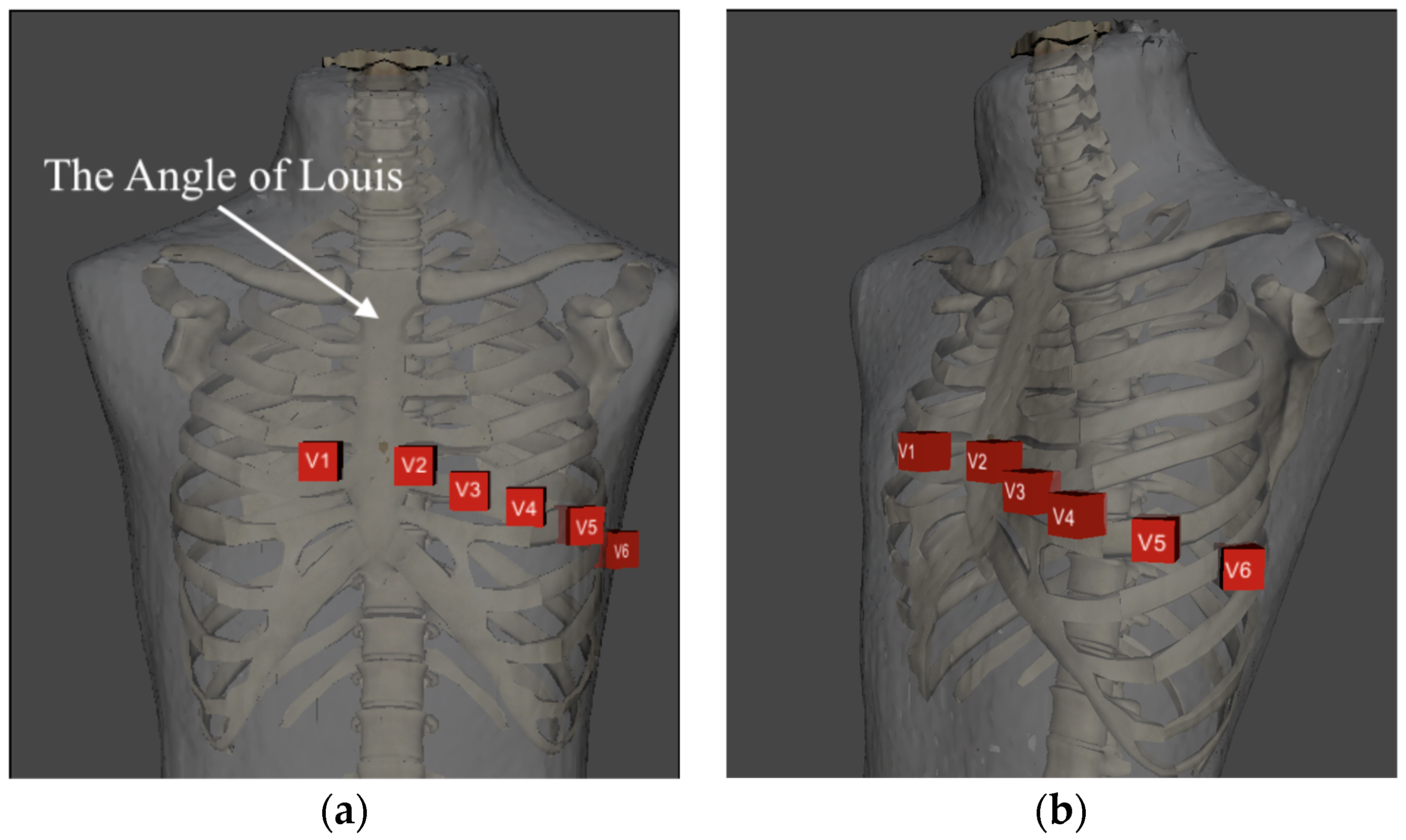
2.1. Chest Lead ECG Positioning
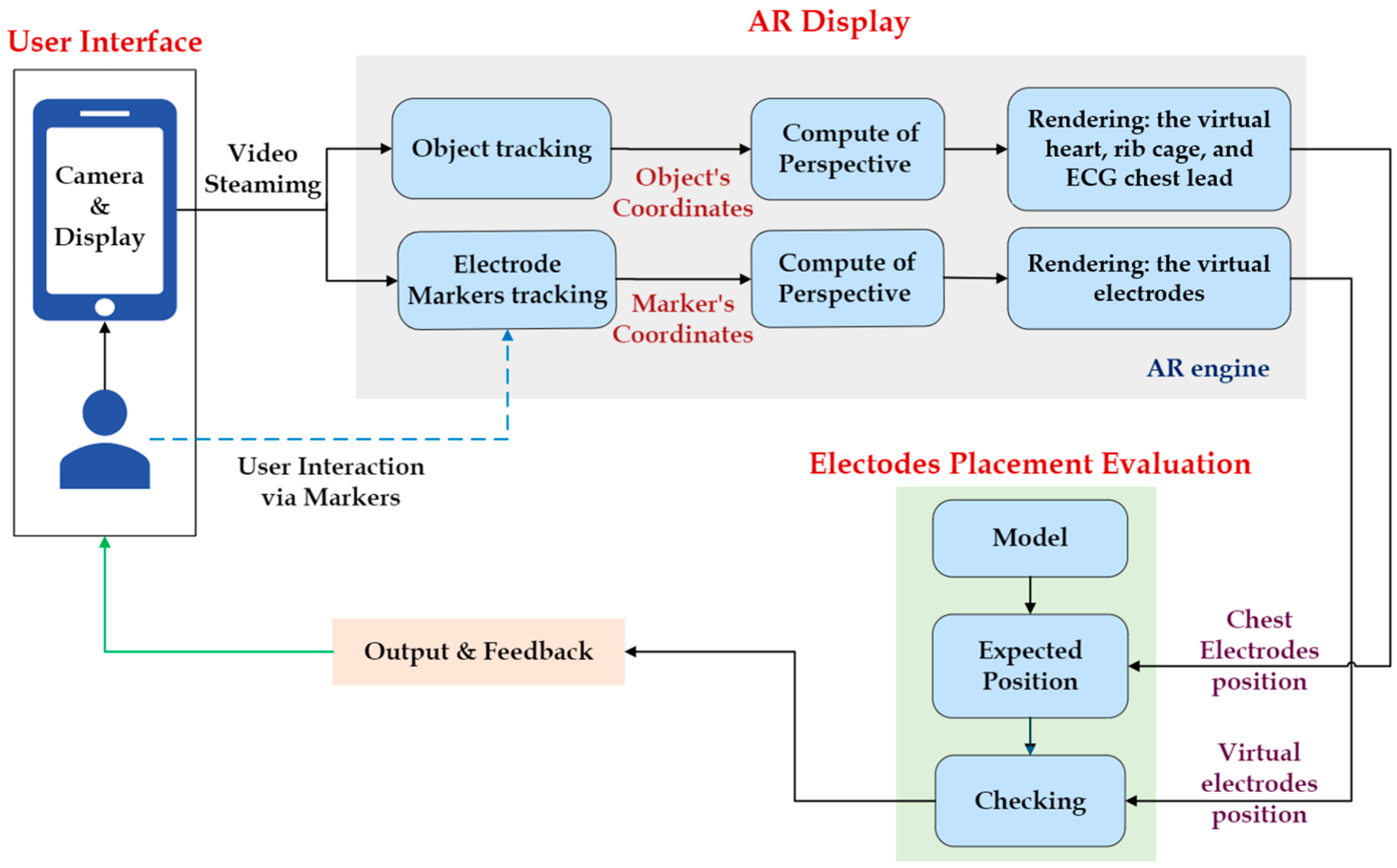
2.2. Overview Architecture of Proposed System
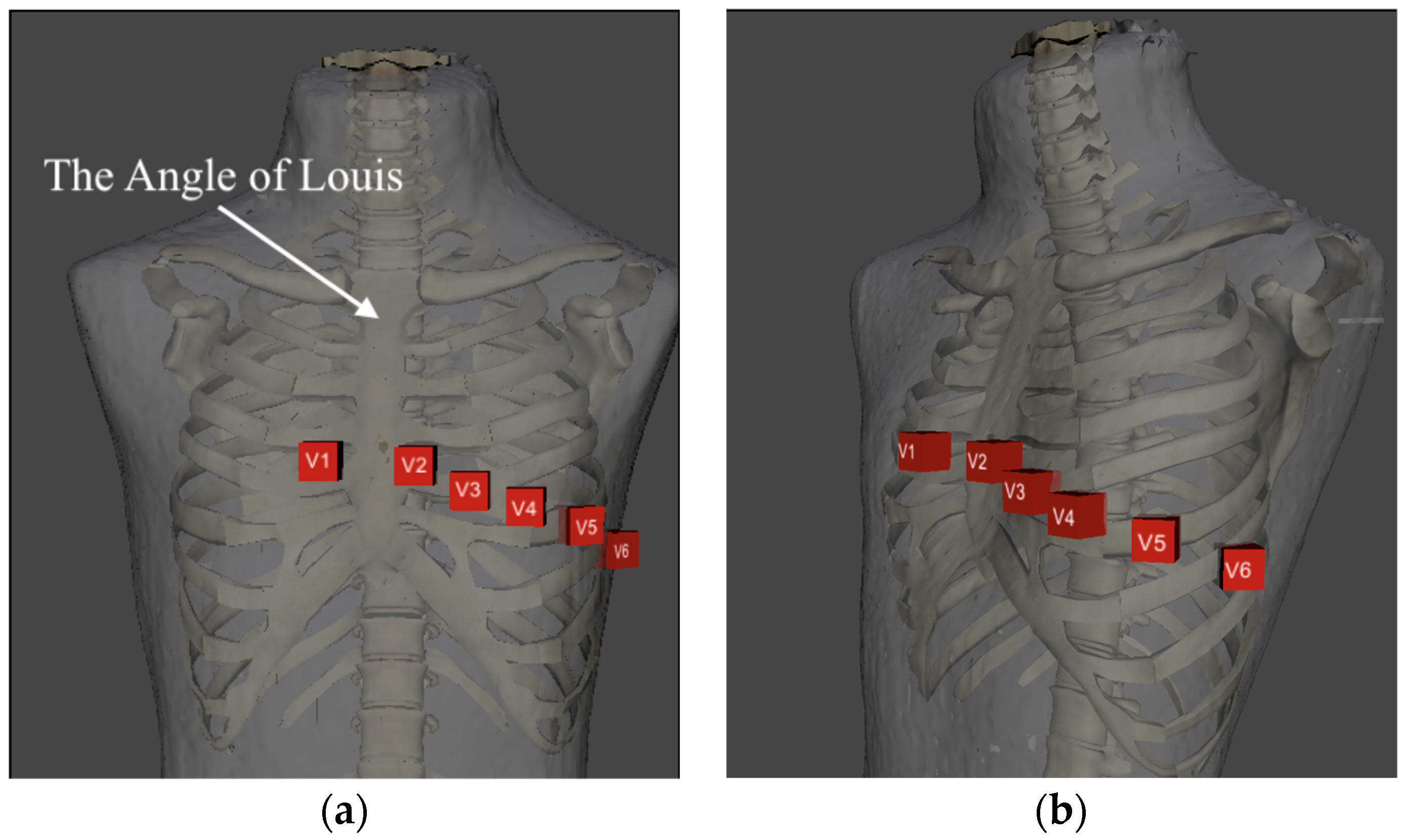
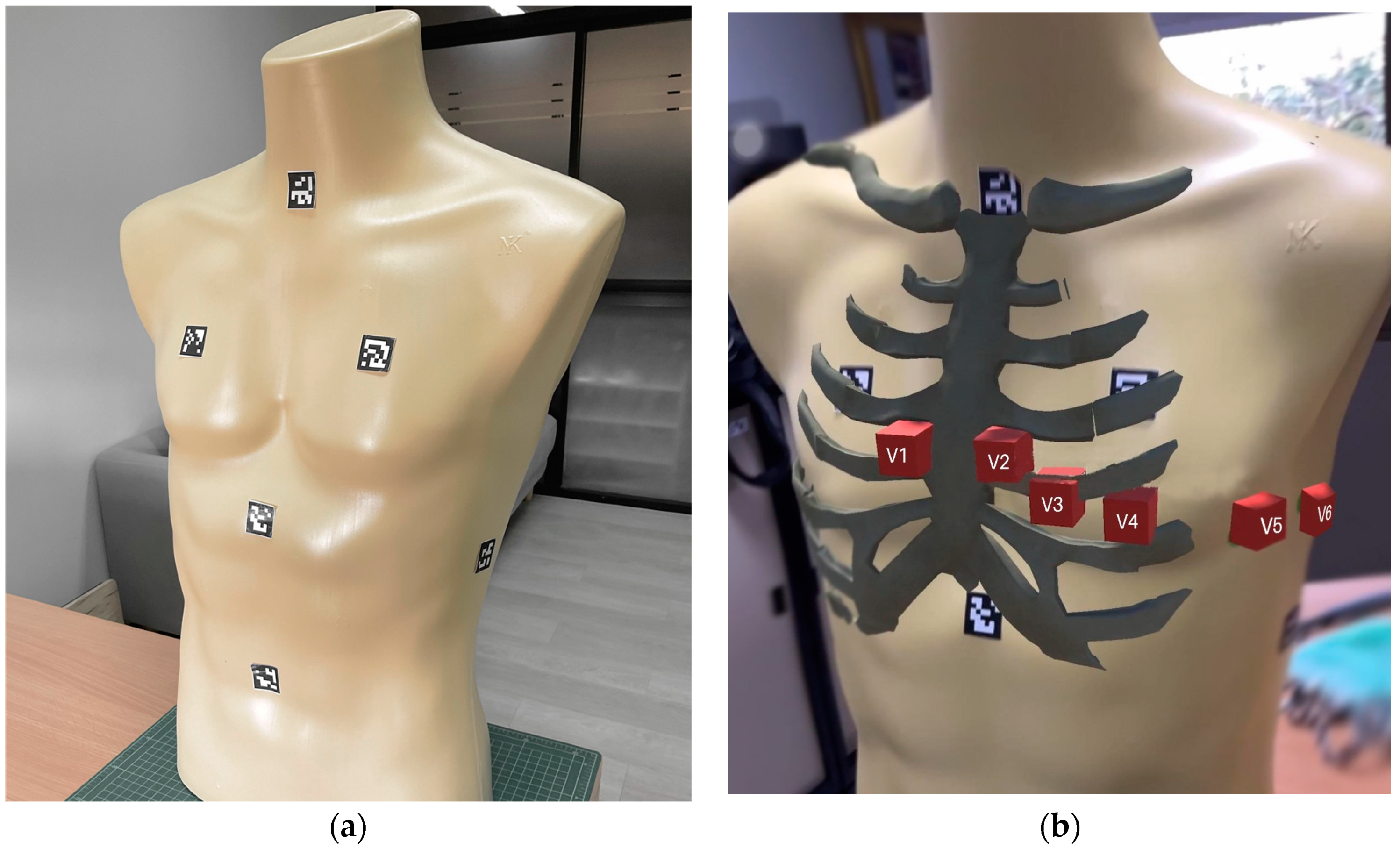
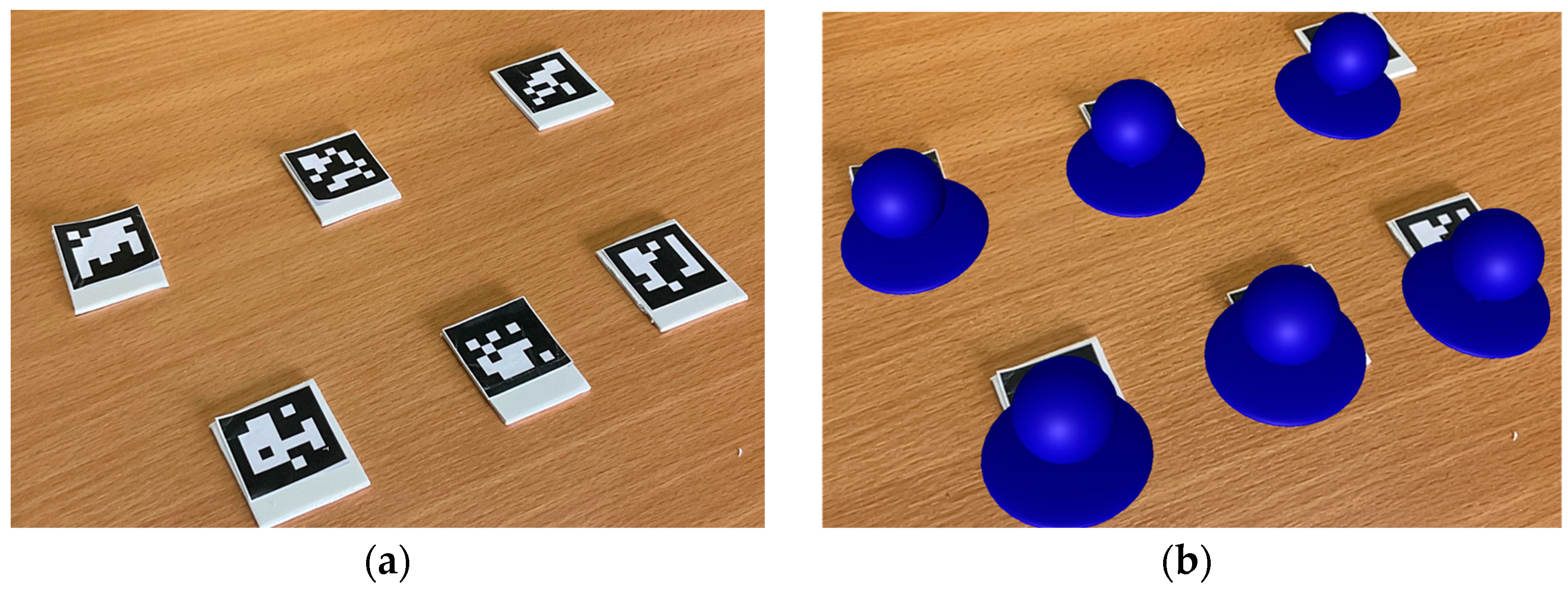
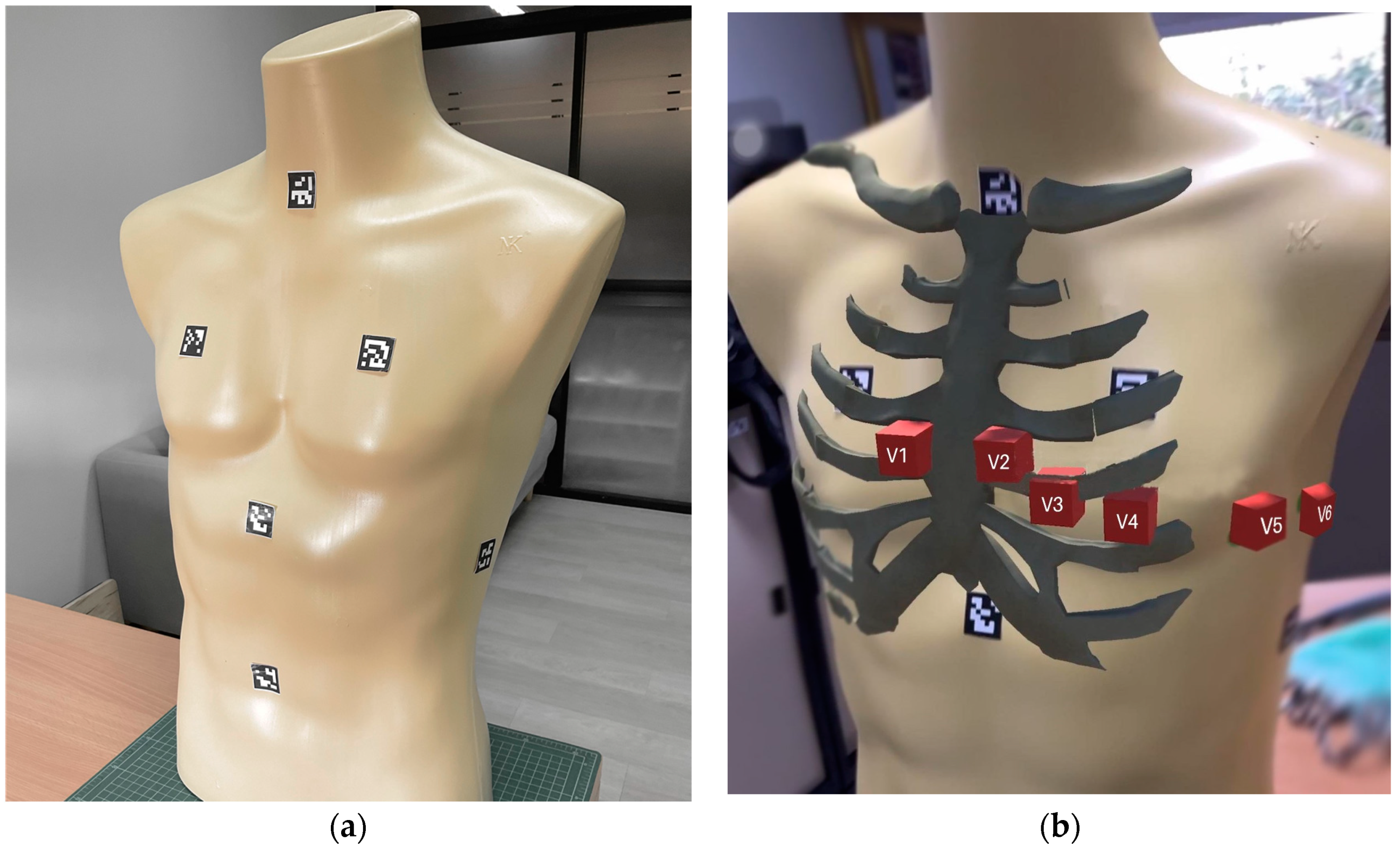
2.2.1. AR Tracking
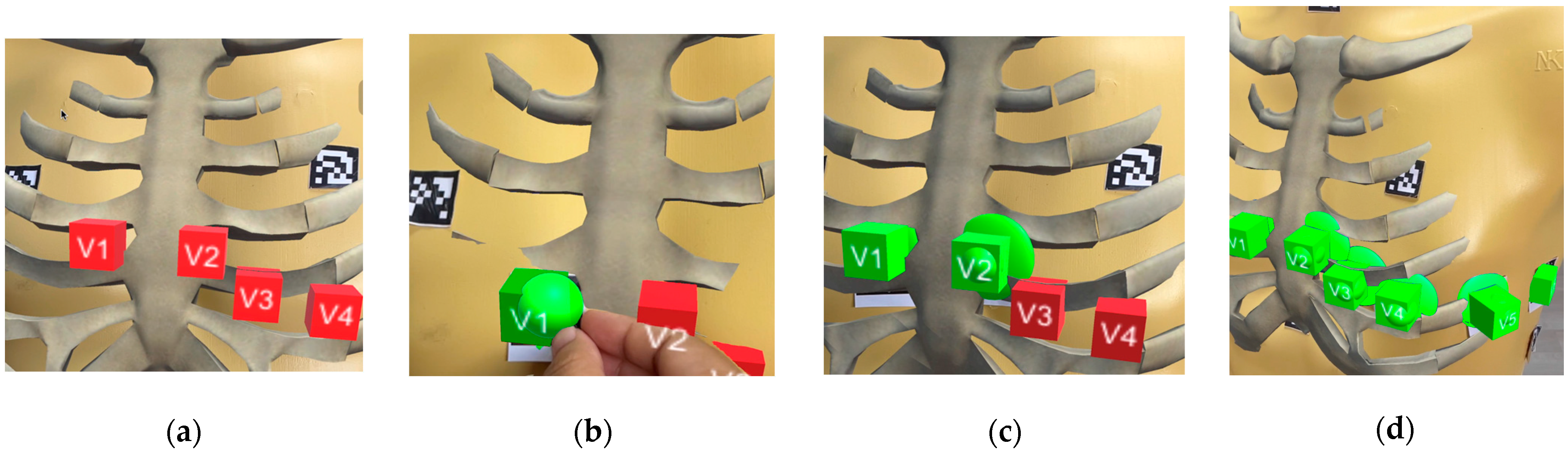
2.2.2. Integrated AR Display and Expert Confirmation
2.2.3. Electrode Placement Evaluation
3. Experiments
3.1. Experimental Objectives
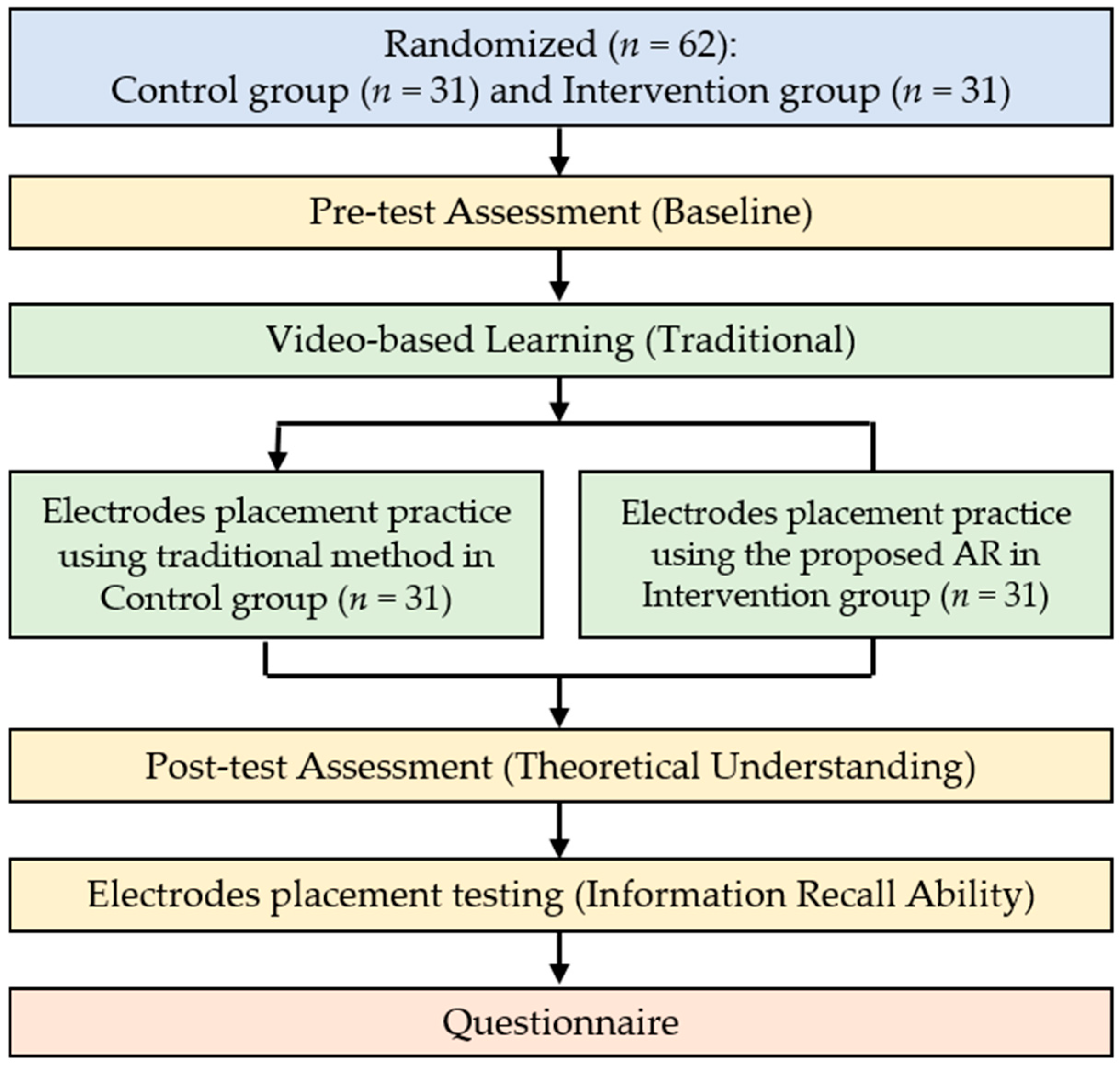
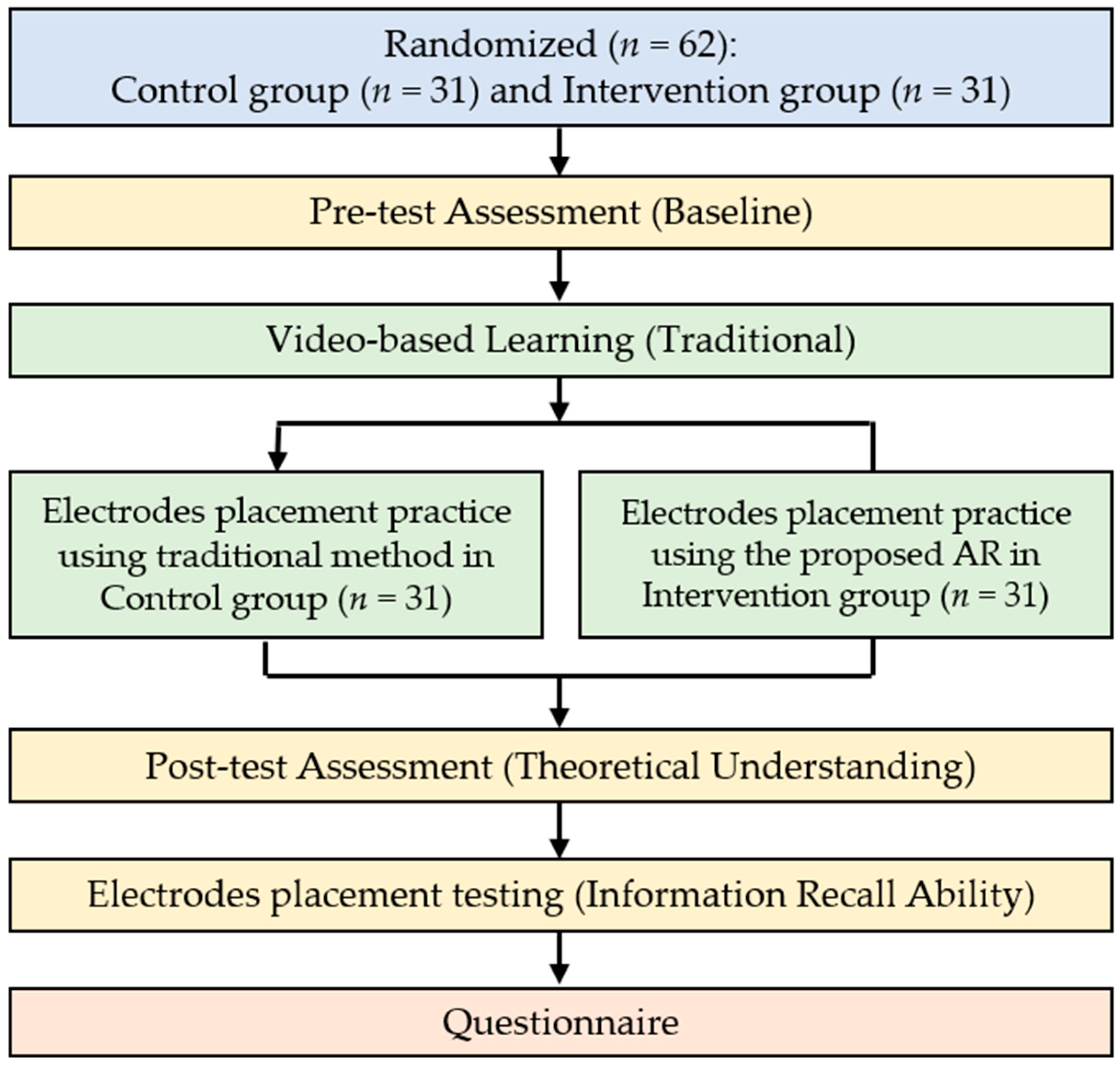
- Verifying impact: This objective involved assessing the impact of the AR application on students’ learning efficiency, covering background theoretical knowledge and ECG electrode placement skills. The study was initiated with a pre-test, a crucial component of our learning assessment, to evaluate the participants’ baseline theoretical comprehension in the control and intervention groups. Subsequently, a post-test, another facet of our learning assessment, measured the increase in theoretical understanding after exposure to the AR application.
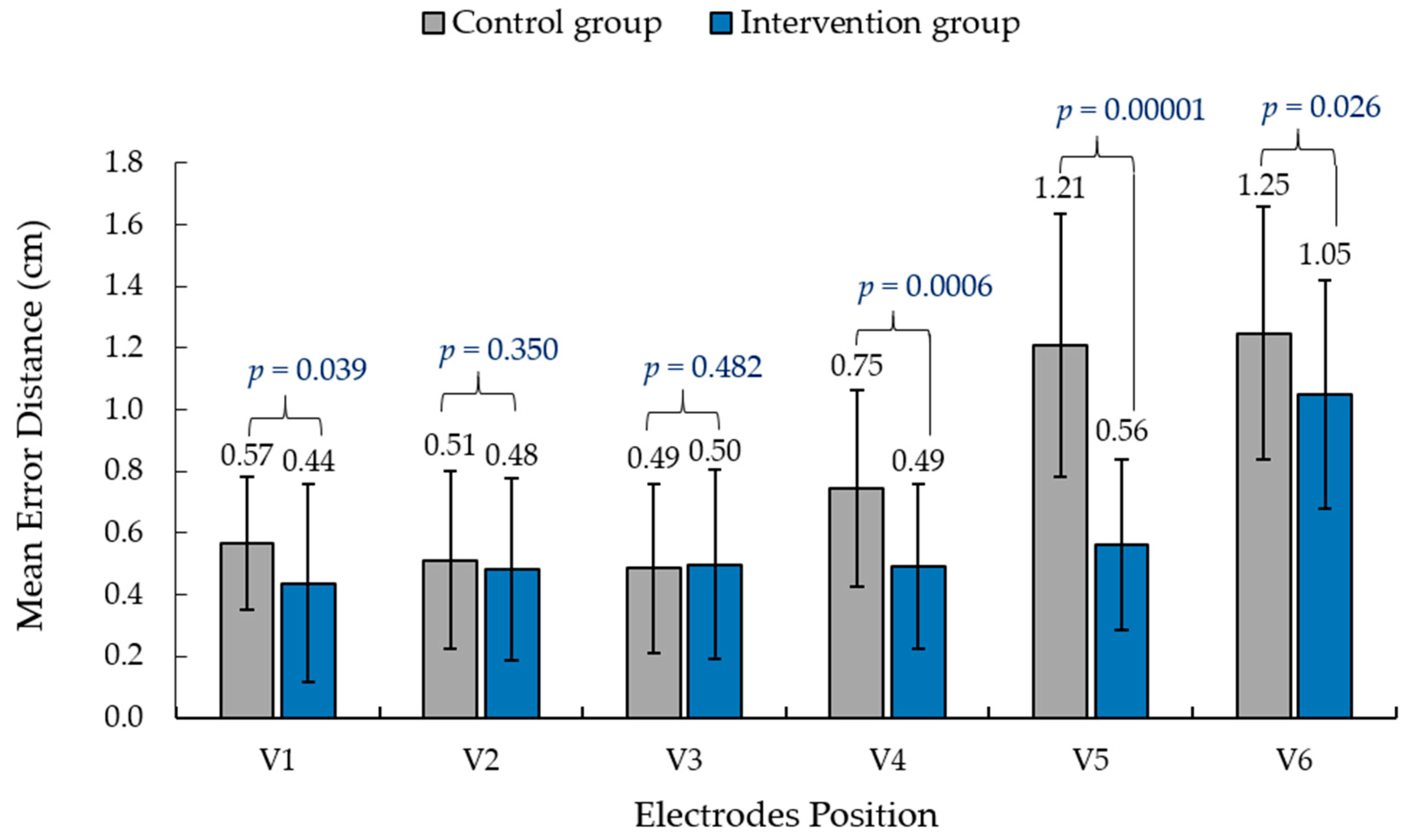
- Proving optimization: This study sought to demonstrate the application’s capacity to optimize the practice of positioning ECG electrodes on the chest. This entailed evaluating the operational efficiency of ECG electrode placement by assessing the accuracy of electrode positioning. To achieve this and further contribute to our optimization assessment, we conducted tests to measure participants’ information recall ability.
3.2. Learning Assessment
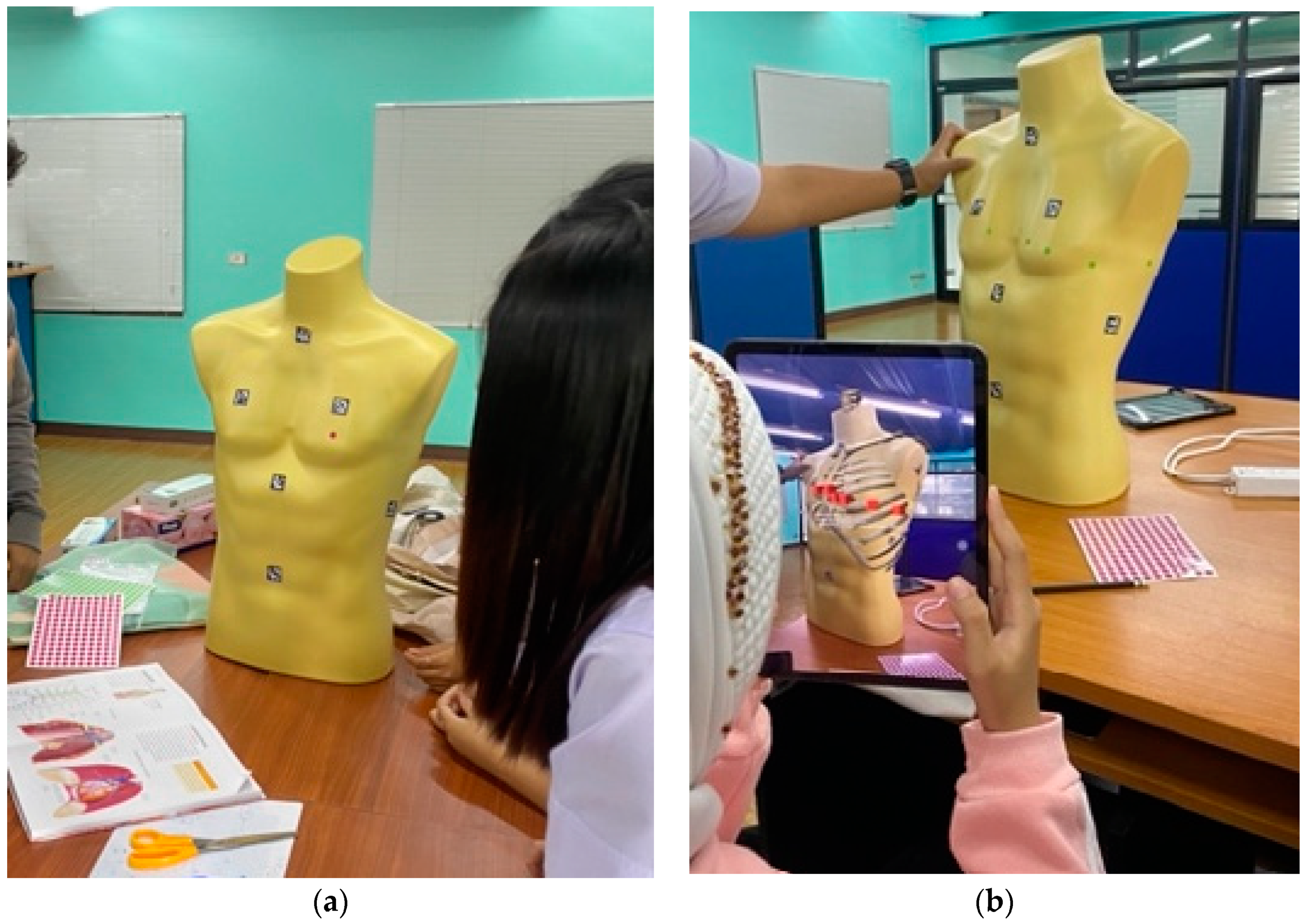
3.3. Learning Materials and Practice Session
3.4. Testing of Information Recall Ability
3.5. Satisfaction
4. Results
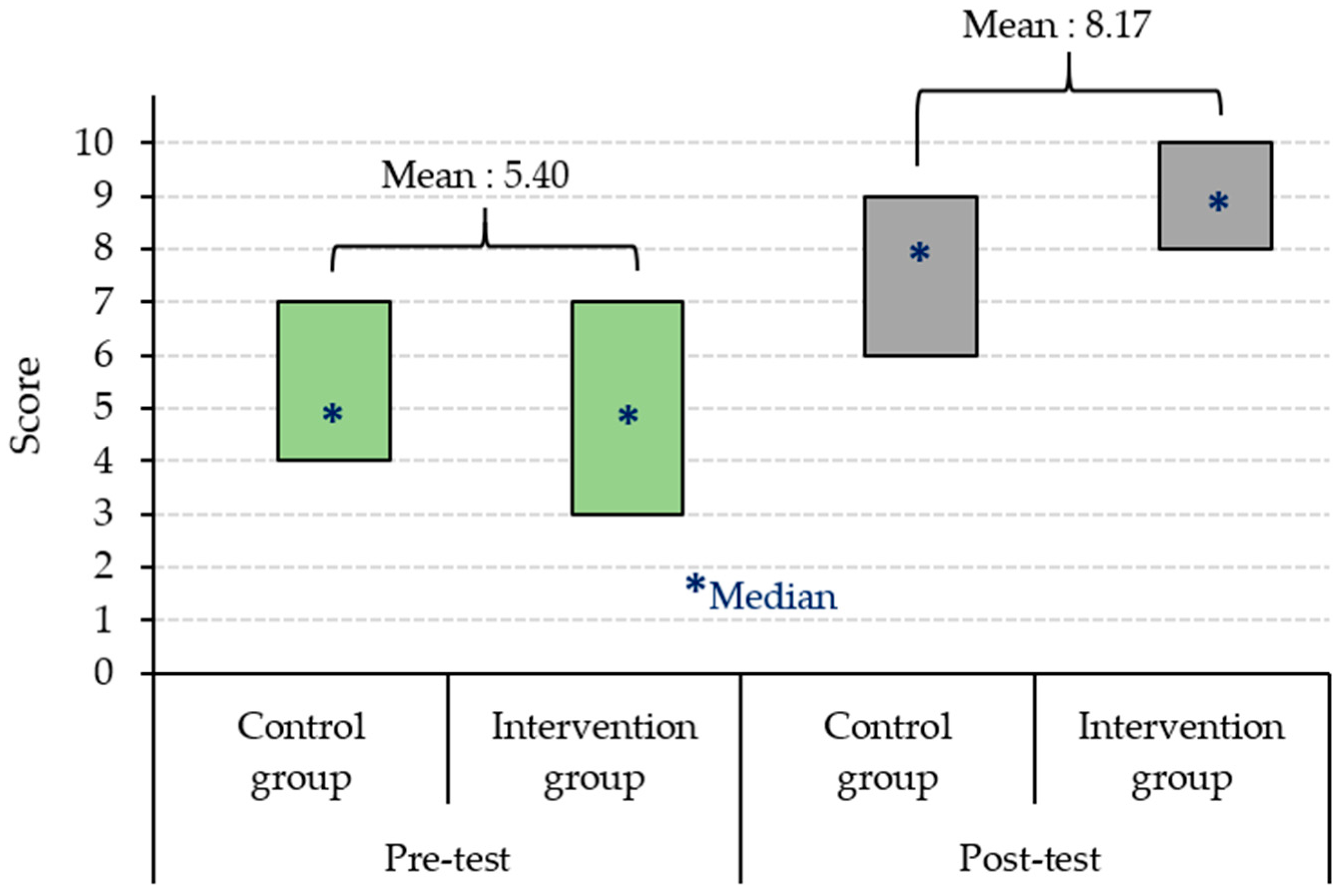
4.1. Theoretical Understanding
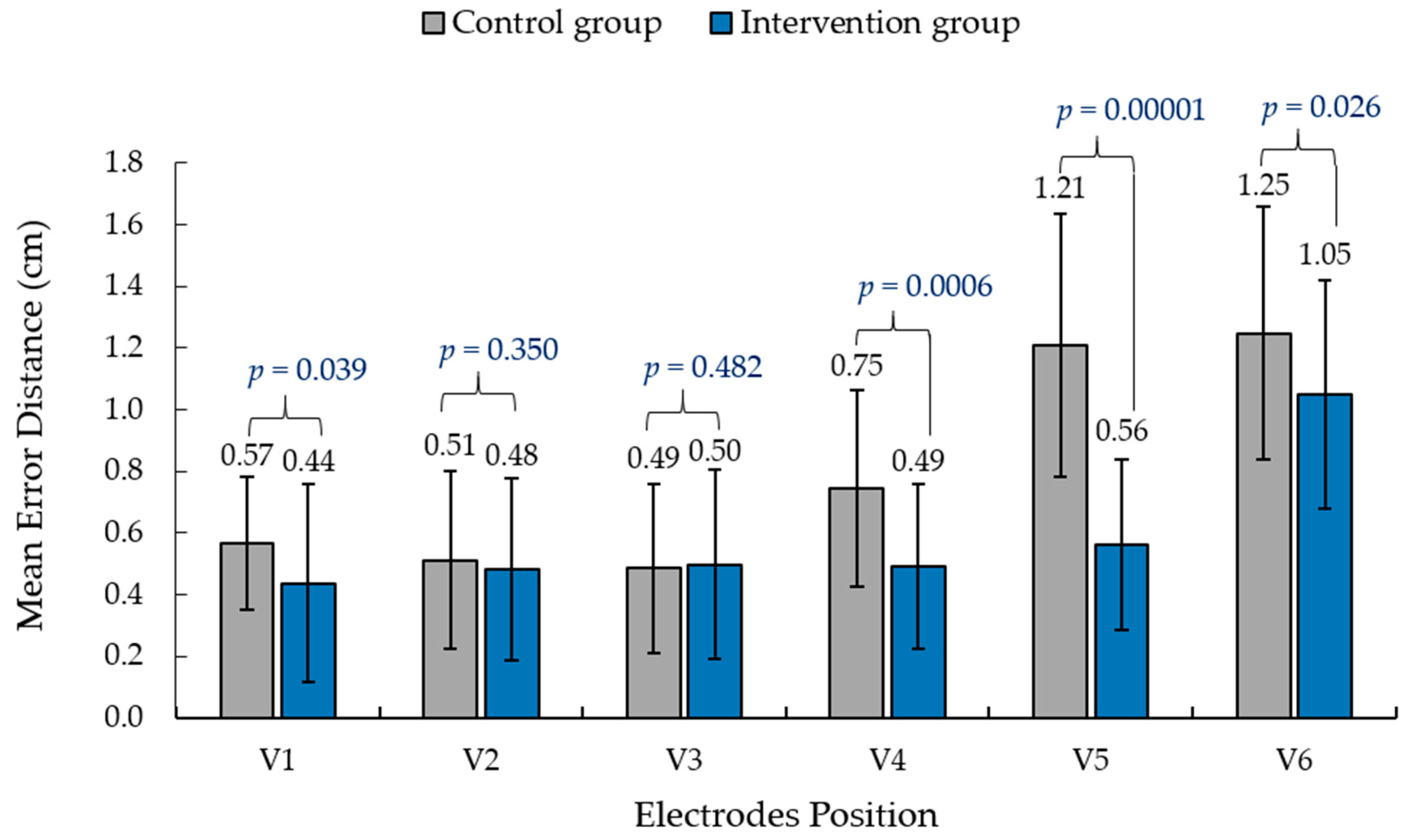
4.2. Information Recall Ability
4.3. Satisfaction with Learning Methods
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- 1.
- How many chest leads are there in total?
- A)
- 4
- B)
- 6
- C)
- 8
- D)
- 10
- 2.
- Which chest lead is placed in the fourth intercostal space to the right of the sternum?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V4
- 3.
- Which lead placement provides a view of the electrical activity in the left ventricle?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 4.
- In which intercostal space is the V4 lead placed?
- A)
- Fourth intercostal space
- B)
- Fifth intercostal space
- C)
- Sixth intercostal space
- D)
- Seventh intercostal space
- 5.
- Which lead placement provides a view of the electrical activity in the right ventricle?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 6.
- Which lead placement is used to diagnose hypertrophy of the left ventricle?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V4
- 7.
- Which lead placement provides the inferior view of the heart?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 8.
- Which lead placement provides the lateral view of the heart?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 9.
- In which lead placement should the electrode be placed closest to the heart?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V4
- 10.
- Which lead placement provides a view of the electrical activity in the mid-axillary line?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V6
References
- Sirakaya, M.; Alsancak Sirakaya, D. Trends in educational augmented reality studies: A systematic review. Malays. Online J. Educ. Technol. 2018, 6, 60–74. [Google Scholar] [CrossRef]
- Pelet, J.E. (Ed.) Mobile Platforms, Design, and Apps for Social Commerce; IGI Global: Hershey, PA, USA, 2017. [Google Scholar]
- Eckert, M.; Volmerg, J.S.; Friedrich, C.M. Augmented reality in medicine: Systematic and bibliographic review. JMIR Mhealth Uhealth 2019, 7, e10967. [Google Scholar] [CrossRef] [PubMed]
- Bin, S.; Masood, S.; Jung, Y. Virtual and augmented reality in medicine. In Biomedical Information Technology; Elsevier: Amsterdam, The Netherlands, 2020; pp. 673–686. [Google Scholar] [CrossRef]
- Ferrari, V.; Klinker, G.; Cutolo, F. Augmented reality in healthcare. J. Healthc. Eng. 2019, 2019, 9321535. [Google Scholar] [CrossRef]
- Gerup, J.; Soerensen, C.B.; Dieckmann, P. Augmented reality and mixed reality for healthcare education beyond surgery: An integrative review. Int. J. Med. Educ. 2020, 11, 1–18. [Google Scholar] [CrossRef]
- Bui, D.T.; Barnett, T.; Hoang, H.T.; Chinthammit, W. Tele-mentoring using augmented reality technology in healthcare: A systematic review. Australas. J. Educ. Technol. 2021, 37, 68–88. [Google Scholar] [CrossRef]
- Aung, Y.M.; Al-Jumaily, A. AR based upper limb rehabilitation system. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 213–218. [Google Scholar] [CrossRef]
- Hondori, H.M.; Khademi, M.; McKenzie, A.; Dodakian, L.; Lopes, C.V.; Cramer, S.C. Abstract T MP43: Utility of augmented reality in relation to virtual reality in stroke rehabilitation. Stroke 2018, 45, 1. [Google Scholar] [CrossRef]
- Martín-Gutiérrez, J.; Saorín, J.L.; Contero, M.; Alcañiz, M.; Pérez-López, D.C.; Ortega, M. Design and validation of an augmented book for spatial abilities development in engineering students. Comput. Graph. 2010, 34, 77–91. [Google Scholar] [CrossRef]
- Akçayir, M.; Akçayir, G. Advantages and challenges associated with AR for education: A systematic review of the literature. Educ. Res. Rev. 2016, 20, 1–11. [Google Scholar] [CrossRef]
- Martín-Gutiérrez, J.; Fabiani, P.; Benesova, W.; Meneses, M.D.; Mora, C.E. Augmented reality to promote collaborative and autonomous learning in higher education. Comput. Hum. Behav. 2015, 51, 752–761. [Google Scholar] [CrossRef]
- Kamińska, D.; Zwoliński, G.; Laska-Leśniewicz, A.; Raposo, R.; Vairinhos, M.; Pereira, E.; Urem, F.; Ljubić Hinić, M.; Haamer, R.E.; Anbarjafari, G. Augmented Reality: Current and New Trends in Education. Electronics 2023, 12, 3531. [Google Scholar] [CrossRef]
- Di Serio, Á.; Ibáñez, M.B.; Kloos, C.D. Impact of an augmented reality system on students’ motivation for a visual art course. Comput. Educ. 2013, 68, 586–596. [Google Scholar] [CrossRef]
- Wu, H.K.; Lee, S.W.Y.; Chang, H.Y.; Liang, J.C. Current status, opportunities and challenges of augmented reality in education. Comput. Educ. 2013, 62, 41–49. [Google Scholar] [CrossRef]
- Kao, G.Y.M.; Ruan, C.A. Designing and evaluating a high interactive augmented reality system for programming learning. Comput. Hum. Behav. 2022, 132, 107245. [Google Scholar]
- Geng, X.; Yamada, M. An augmented reality learning system for Japanese compound verbs: Study of learning performance and cognitive load. Smart Learn. Environ. 2020, 7, 27. [Google Scholar] [CrossRef]
- Bujak, K.R.; Radu, I.; Catrambone, R.; MacIntyre, B.; Zheng, R.; Golubski, G. A psychological perspective on augmented reality in the mathematics classroom. Comput. Educ. 2013, 68, 536–544. [Google Scholar] [CrossRef]
- Lee, K. Augmented reality in education and training. TechTrends 2012, 56, 13–21. [Google Scholar] [CrossRef]
- Tang, Y.M.; Chau, K.Y.; Kwok, A.P.K.; Zhu, T.; Ma, X. A systematic review of immersive technology applications for medical practice and education-trends, application areas, recipients, teaching contents, evaluation methods, and performance. Educ. Res. Rev. 2022, 35, 100429. [Google Scholar] [CrossRef]
- Dhar, P.; Rocks, T.; Samarasinghe, R.M.; Stephenson, G.; Smith, C. Augmented reality in medical education: Students’ experiences and learning outcomes. Med. Educ. Online 2021, 26, 1953953. [Google Scholar] [CrossRef]
- Parsons, D.; MacCallum, K. Current perspectives on augmented reality in medical education: Applications, affordances and limitations. Adv. Med. Educ. Pract. 2021, 12, 77–91. [Google Scholar] [CrossRef]
- Kassutto, S.M.; Baston, C.; Clancy, C. Virtual, augmented, and alternate reality in medical education: Socially distanced but fully immersed. ATS Sch. 2021, 2, 651–664. [Google Scholar] [CrossRef]
- Xu, X.; Mangina, E.; Campbell, A.G. HMD-based virtual and augmented reality in medical education: A systematic review. Front. Virtual Real. 2021, 2, 692103. [Google Scholar] [CrossRef]
- Kugelmann, D.; Stratmann, L.; Nühlen, N.; Bork, F.; Hoffmann, S.; Samarbarksh, G.; Waschke, J. An augmented reality magic mirror as additive teaching device for gross anatomy. Ann. Anat. Anz. 2018, 215, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Gsaxner, C.; Pepe, A.; Wallner, J.; Schmalstieg, D.; Egger, J. Markerless image-to-face registration for untethered augmented reality in head and neck surgery. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Cham, Switzerland, 2019; pp. 236–244. [Google Scholar]
- Barmaki, R.; Yu, K.; Pearlman, R.; Shingles, R.; Bork, F.; Osgood, G.M.; Navab, N. Enhancement of anatomical education using augmented reality: An empirical study of body painting. Anat. Sci. Educ. 2019, 12, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Ebner, F.; De Gregorio, A.; Schochter, F.; Bekes, I.; Janni, W.; Lato, K. Effect of an augmented reality ultrasound trainer app on the motor skills needed for a kidney ultrasound: Prospective trial. JMIR Serious Games 2019, 7, e12713. [Google Scholar] [CrossRef] [PubMed]
- McCann, K.; Holdgate, A.; Mahammad, R.; Waddington, A. Accuracy of ECG electrode placement by emergency department clinicians. Emerg. Med. Australas. 2007, 19, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Bifulco, P.; Narducci, F.; Vertucci, R.; Ambruosi, P.; Cesarelli, M.; Romano, M. Telemedicine supported by Augmented Reality: An interactive guide for untrained people in performing an ECG test. Biomed. Eng. Online 2014, 13, 153. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Goldberger, Z.D.; Shvilkin, A. Clinical Electrocardiography: A Simplified Approach E-Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2017. [Google Scholar]
- Kato, H.; Billinghurst, M. Marker tracking and hmd calibration for a video-based augmented reality conferencing system. In Proceedings of the 2nd IEEE and ACM International Workshop on Augmented Reality (IWAR’99), San Francisco, CA, USA, 20–21 October 1999; pp. 85–94. [Google Scholar]
- Neumann, U.; You, S. Natural feature tracking for augmented reality. IEEE Trans. Multimed. 1999, 1, 53–64. [Google Scholar] [CrossRef]
- Alexiou, E.; Upenik, E.; Ebrahimi, T. Towards subjective quality assessment of point cloud imaging in augmented reality. In Proceedings of the 2017 IEEE 19th International Workshop on Multimedia Signal Processing (MMSP), Luton, UK, 16–18 October 2017; pp. 1–6. [Google Scholar]
- Dinayusadewi, N.P.; Agustika, G.N.S. Development of augmented reality application as a mathematics learning media in elementary school geometry materials. J. Educ. Technol. 2020, 4, 204–210. [Google Scholar] [CrossRef]
- Wake, N.; Rosenkrantz, A.B.; Huang, R.; Park, K.U.; Wysock, J.S.; Taneja, S.S.; Chandarana, H. Patient-specific 3D printed and augmented reality kidney and prostate cancer models: Impact on patient education. 3D Print. Med. 2019, 5, 4. [Google Scholar] [CrossRef]
- Rahmat, R.F.; Akbar, F.; Syahputra, M.F.; Budiman, M.A.; Hizriadi, A. Interactive augmented reality implementation of hijaiyah alphabet for children education. J. Phys. Conf. Ser. 2018, 978, 012102. [Google Scholar] [CrossRef]
- Muñoz-Saavedra, L.; Miró-Amarante, L.; Domínguez-Morales, M. Augmented and virtual reality evolution and future tendency. Appl. Sci. 2020, 10, 322. [Google Scholar] [CrossRef]
- Albertazzi, D.; Okimoto, M.L.; Ferreira, M.G.G. Developing an usability test to evaluate the use of augmented reality to improve the first interaction with a product. Work 2012, 41 (Suppl. S1), 1160–1163. [Google Scholar] [CrossRef] [PubMed]
- Bakri, F.; Marsal, O.; Muliyati, D. Textbooks equipped with augmented reality technology for physics topic in high-school. J. Penelit. Pengemb. Pendidik. Fis. 2019, 5, 113–122. [Google Scholar] [CrossRef]
- Fidan, M.; Tuncel, M. Integrating Augmented Reality into Problem Based Learning: The Effects on Learning Achievement and Attitude in Physics Education. Comput. Educ. 2019, 142, 103635. [Google Scholar] [CrossRef]
- Boonbrahm, P.; Kaewrat, C.; Boonbrahm, S. Interactive marker-based augmented reality for CPR training. Int. J. Technol. 2019, 10, 291–319. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ECG Chest Lead Position | Average Error Distance ± SD (cm) |
|---|---|
| V1 | 0.31 ± 0.03 |
| V2 | 0.30 ± 0.03 |
| V3 | 0.21 ± 0.03 |
| V4 | 0.23 ± 0.03 |
| V5 | 0.44 ± 0.03 |
| V6 | 0.40 ± 0.04 |
| Mean | 0.31 ± 0.03 |
| No. | Question |
|---|---|
| Q1 | My attention was quickly captured by the materials. |
| Q2 | I could easily complete the ECG placement tasks with guidance. |
| Q3 | I enjoy this method of learning. |
| Q4 | I have learned the ’structural composition and relative locations of ECG placements. |
| Q5 | I am confident that I can place all electrodes in the future. |
| Q6 | The ECG placement tasks were not difficult for me at all. |
| Q7 | I did not bored at the conclusion of the course. |
| Q8 | I have mastered the order of electrode placement for ECG chest leads. |
| Q9 | I am eager to learn more about the ECG placement through this course. |
| Q10 | I was confident in my knowledge of the course material. |
| Participants | Mean Score | SD | Z-Score | p-Value | Result |
|---|---|---|---|---|---|
| Control group | 5.45 | 0.97 | 0.640 | 0.32 | Not significant |
| Intervention group | 5.32 | 1.21 |
| Participants | Mean Score | SD | Z-Score | p-Value | Result |
|---|---|---|---|---|---|
| Control group | 7.61 | 0.76 | −4.476 | 0.00001 | Significant |
| Intervention group | 8.74 | 0.77 |
| Factor | Question No. | Group | Range | Median | Mean ± SD |
|---|---|---|---|---|---|
| Learning Interest | Q1 | Control | 2–4 | 3 | 3.32 ± 0.54 |
| Intervention | 3–5 | 5 | 4.52 ± 0.57 | ||
| Q7 | Control | 1–3 | 2 | 2.32 ± 0.70 | |
| Intervention | 4–5 | 5 | 4.58 ± 0.50 | ||
| Task Difficulty | Q2 | Control | 2–4 | 3 | 2.77 ± 0.67 |
| Intervention | 3–5 | 4 | 3.94 ± 0.57 | ||
| Q6 | Control | 3–5 | 3 | 3.52 ± 0.57 | |
| Intervention | 3–5 | 4 | 3.71 ± 0.59 | ||
| Academic Outcome | Q4 | Control | 2–4 | 3 | 2.97 ± 0.80 |
| Intervention | 3–5 | 4 | 3.68 ± 0.65 | ||
| Q8 | Control | 2–4 | 3 | 3.45 ± 0.57 | |
| Intervention | 3–5 | 4 | 4.10 ± 0.65 | ||
| Confidence | Q5 | Control | 3–4 | 4 | 3.61 ± 0.50 |
| Intervention | 4–5 | 5 | 4.65 ± 0.49 | ||
| Q10 | Control | 2–5 | 3 | 3.65 ± 0.91 | |
| Intervention | 3–5 | 4 | 3.94 ± 0.68 | ||
| Satisfaction | Q3 | Control | 1–4 | 3 | 2.87 ± 0.67 |
| Intervention | 4–5 | 5 | 4.68 ± 0.48 | ||
| Q9 | Control | 3–5 | 3 | 3.65 ± 0.75 | |
| Intervention | 4–5 | 5 | 4.55 ± 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaewrat, C.; Anopas, D.; Aung, S.T.; Punsawad, Y. Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice. Informatics 2024, 11, 5. https://doi.org/10.3390/informatics11010005
Kaewrat C, Anopas D, Aung ST, Punsawad Y. Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice. Informatics. 2024; 11(1):5. https://doi.org/10.3390/informatics11010005
Chicago/Turabian StyleKaewrat, Charlee, Dollaporn Anopas, Si Thu Aung, and Yunyong Punsawad. 2024. "Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice" Informatics 11, no. 1: 5. https://doi.org/10.3390/informatics11010005
APA StyleKaewrat, C., Anopas, D., Aung, S. T., & Punsawad, Y. (2024). Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice. Informatics, 11(1), 5. https://doi.org/10.3390/informatics11010005