
The Joint Observation in Neonatology and Neurodevelopmental Outcome of Preterm Infants at Six Months Corrected Age: Secondary Outcome Data from a Randomised Controlled Trial
 and
on behalf of the JOIN Research Consortium
and
on behalf of the JOIN Research Consortium
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Trial Design, Procedure, Data Collection, and Timing
2.3. Intervention and Follow-Up
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
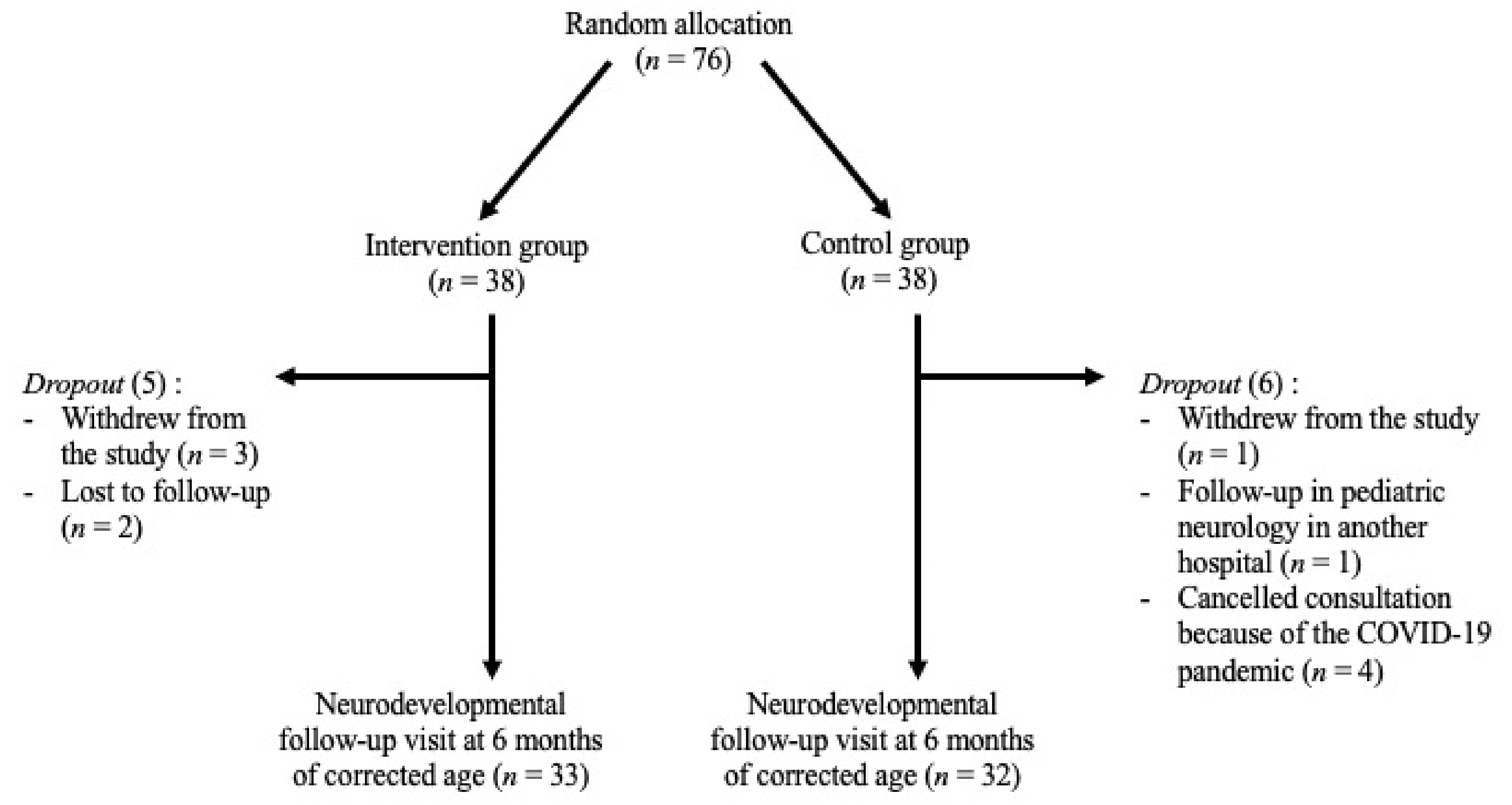
3.1. Population
3.2. Baseline Characteristics
3.3. Six-Month Infant Developmental Outcome
4. Discussion
Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frey, H.A.; Klebanoff, M.A. The epidemiology, etiology, and costs of preterm birth. Semin. Fetal Neonatal Med. 2016, 21, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Perin, J.; Mulick, A.; Yeung, D.; Villavicencio, F.; Lopez, G.; Strong, K.L.; Prieto-Merino, D.; Cousens, S.; Black, R.E.; Liu, L. Global, regional, and national causes of under-5 mortality in 2000–19: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc. Health 2022, 6, 106–115. [Google Scholar] [CrossRef]
- Lasky, R.E.; Williams, A.L. Noise and Light Exposures for Extremely Low Birth Weight Newborns During Their Stay in the Neonatal Intensive Care Unit. Pediatrics 2009, 123, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Hane, A.A.; Myers, M.M.; Hofer, M.A.; Ludwig, R.J.; Halperin, M.S.; Austin, J.; Glickstein, S.B.; Welch, M.G. Family Nurture Intervention Improves the Quality of Maternal Caregiving in the Neonatal Intensive Care Unit: Evidence from a Randomized Controlled Trial. J. Dev. Behav. Pediatr. 2015, 36, 188–196. [Google Scholar] [CrossRef]
- Montirosso, R.; Prete, A.D.; Bellù, R.; Tronick, E. Level of NICU Quality of Developmental Care and Neurobehavioral Performance in Very Preterm Infants. Pediatrics 2012, 129, e1129–e1137. [Google Scholar] [CrossRef]
- Sizun, J.; Guillois, B.; Casper, C.; Thiriez, G.; Kuhn, P. Soins de Développement en Période Néonatale: De la Recherche à la Pratique; Springer: Berlin, Germany, 2014; 330p. [Google Scholar]
- Back, S.A. Brain Injury in the Preterm Infant: New Horizons for Pathogenesis and Prevention. Pediatr. Neurol. 2015, 53, 185–192. [Google Scholar] [CrossRef]
- Back, S.A.; Miller, S.P. Brain injury in premature neonates: A primary cerebral dysmaturation disorder? Ann. Neurol. 2014, 75, 469–486. [Google Scholar] [CrossRef]
- Volpe, J.J. Brain injury in premature infants: A complex amalgam of destructive and developmental disturbances. Lancet Neurol. 2009, 8, 110–124. [Google Scholar] [CrossRef]
- Milgrom, J.; Newnham, C.; Anderson, P.J.; Doyle, L.W.; Gemmill, A.W.; Lee, K.; Hunt, R.W.; Bear, M.; Inder, T. Early sensitivity training for parents of preterm infants: Impact on the developing brain. Pediatr. Res. 2010, 67, 330–335. [Google Scholar] [CrossRef]
- Symington, A.; Pinelli, J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst. Rev. 2006, 2, CD001814. [Google Scholar]
- Schneider, J.; Borghini, A.; Harari, M.M.; Faure, N.; Tenthorey, C.; Le Berre, A.; Tolsa, J.F.; Horsch, A. Joint observation in NICU (JOIN): Study protocol of a clinical randomised controlled trial examining an early intervention during preterm care. BMJ Open 2019, 9(3), e026484. [Google Scholar] [CrossRef]
- Consort—Welcome to the CONSORT Website. Available online: http://www.consort-statement.org/ (accessed on 14 April 2022).
- Largo, R.H.; Pfister, D.; Molinari, L.; Kundu, S.; Lipp, A.; Duc, G. Significance of prenatal, perinatal and postnatal factors in the development of AGA preterm infants at five to seven years. Dev. Med. Child Neurol. 1989, 31, 440–456. [Google Scholar] [CrossRef]
- Brazelton, T.B.; Nugent, J.K. Neonatal Behavioral Assessment Scale; No. 137; Cambridge University Press: Cambridge, UK, 1995. [Google Scholar]
- Als, H. A Synactive Model of Neonatal Behavioral Organization: Framework for the Assessment of Neurobehavioral Development in the Premature Infant and for Support of Infants and Parents in the Neonatal Intensive Care Environment. Phys. Occup. Ther. Pediatr. 1986, 6, 3–53. [Google Scholar]
- Bullinger, A.; Goubet, N. Le bébé prématuré, acteur de son développement. Enfance 1999, 52, 27–32. [Google Scholar] [CrossRef]
- Kennedy, H.; Ball, K.; Barlow, J. How does video interaction guidance contribute to infant and parental mental health and well-being? Clin. Child Psychol. Psychiatry 2017, 22, 500–517. [Google Scholar] [CrossRef]
- Bayley, N.; Scales Infant. Bayley Scales of Infant and Toddler Development, 3rd ed.; Technical manual; Harcourt: San Antonio, TX, USA, 2006. [Google Scholar]
- Johnson, S.; Moore, T.; Marlow, N. Using the Bayley-III to assess neurodevelopmental delay: Which cut-off should be used? Pediatr. Res. 2014, 75, 670–674. [Google Scholar] [CrossRef]
- Çelik, P.; Ayranci Sucakli, I.; Yakut, H.I. Which Bayley-III cut-off values should be used in different developmental levels? Turk. J. Med. Sci. 2020, 50, 764–770. [Google Scholar] [CrossRef]
- Griffiths, R. The Abilities of Young Children: A Comprehensive System of Mental Measurement for the First Eight Years of Life, Revised ed.; Test Agency Ltd.: Oxford, UK, 1984; 181p. [Google Scholar]
- Givrad, S.; Hartzell, G.; Scala, M. Promoting infant mental health in the neonatal intensive care unit (NICU): A review of nurturing factors and interventions for NICU infant-parent relationships. Early Hum. Dev. 2021, 154, 105281. [Google Scholar] [CrossRef]
- Welch, M.G.; Firestein, M.R.; Austin, J.; Hane, A.A.; Stark, R.I.; Hofer, M.A.; Garland, M.; Glickstein, S.B.; Brunelli, S.A.; Ludwig, R.J.; et al. Family Nurture Intervention in the Neonatal Intensive Care Unit improves social-relatedness, attention, and neurodevelopment of preterm infants at 18 months in a randomized controlled trial. J. Child Psychol. Psychiatry 2015, 56, 1202–1211. [Google Scholar] [CrossRef]
- Milgrom, J.; Newnham, C.; Martin, P.R.; Anderson, P.J.; Doyle, L.W.; Hunt, R.W.; Achenbach, T.M.; Ferretti, C.; Holt, C.J.; Inder, T.E.; et al. Early communication in preterm infants following intervention in the NICU. Early Hum. Dev. 2013, 89, 755–762. [Google Scholar] [CrossRef]
- Vandenberg, K.A. Individualized developmental care for high risk newborns in the NICU: A practice guideline. Early Hum. Dev. 2007, 83, 433–442. [Google Scholar] [CrossRef]
- Madigan, S.; Oatley, H.; Racine, N.; Fearon, R.M.P.; Schumacher, L.; Akbari, E.; Cooke, J.E.; Tarabulsy, G.M. A Meta-Analysis of Maternal Prenatal Depression and Anxiety on Child Socioemotional Development. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 645–657.e8. [Google Scholar] [CrossRef]
- Nordhov, S.M.; Rønning, J.A.; Dahl, L.B.; Ulvund, S.E.; Tunby, J.; Kaaresen, P.I. Early intervention improves cognitive outcomes for preterm infants: Randomized controlled trial. Pediatrics 2010, 126, e1088–e1094. [Google Scholar] [CrossRef]
- Newnham, C.A.; Milgrom, J.; Skouteris, H. Effectiveness of a modified Mother-Infant Transaction Program on outcomes for preterm infants from 3 to 24 months of age. Infant Behav. Dev. 2009, 32, 17–26. [Google Scholar] [CrossRef]
- Fukkink, R.G. Video feedback in widescreen: A meta-analysis of family programs. Clin. Psychol. Rev. 2008, 28, 904–916. [Google Scholar] [CrossRef]
- Spittle, A.J.; Anderson, P.J.; Lee, K.J.; Ferretti, C.; Eeles, A.; Orton, J.; Boyd, R.N.; Inder, T.; Doyle, L.W. Preventive care at home for very preterm infants improves infant and caregiver outcomes at 2 years. Pediatrics 2010, 126, e171–e178. [Google Scholar] [CrossRef]
- Muller-Nix, C.; Forcada-Guex, M.; Pierrehumbert, B.; Jaunin, L.; Borghini, A.; Ansermet, F. Prematurity, maternal stress and mother-child interactions. Early Hum. Dev. 2004, 79, 145–158. [Google Scholar] [CrossRef]
- Moore, T.; Johnson, S.; Haider, S.; Hennessy, E.; Marlow, N. Relationship between test scores using the second and third editions of the Bayley Scales in extremely preterm children. J. Pediatr. 2012, 160, 553–558. [Google Scholar] [CrossRef]


{kind=link}
| Intervention Group (N = 33) | Control Group (N = 32) | p-Value | |
|---|---|---|---|
| Pregnancy variables | |||
| Maternal age (M, IQR) | 32 (30–34.5) | 32.5 (30–36.8) | p = 0.381 U = 461.5 |
| Number of pregnancies (M, IQR) | 1 (1–2) | 1 (1–2) | p = 0.810 U = 512 |
| Maternal Largo score (M, IQR) missing n = 1 | 2 (2–3.8) | 2 (1–3) | p = 0.319 U = 441 |
| Paternal Largo score (M, IQR) missing n = 7 | 3 (2–4) | 3 (1.5–3) | p = 0.802 U = 405 |
| Multiple pregnancy (N, %) | 9 (27.3) | 5 (15.6) | 0.367 |
| Assisted reproduction (N, %) | 4 (12.1) | 3 (9.4) | 1 |
| Prenatal steroids (N, %) | 26 (78.8) | 29 (90.6) | 0.303 |
| Neonatal variables | |||
| Female (N, %) | 21 (63.6) | 16 (50) | 0.321 |
| Gestational age, weeks (M, IQR) | 30.1 (28.7–31.4) | 30.2 (29.6–31.4) | p = 0.412 U = 465.5 |
| Birth weight, grams (M, IQR) | 1240 (990–1456.5) | 1237.5 (1006–1523.8) | p = 0.896 U = 518 |
| Small for gestational age (N, %) | 5 (15.2) | 7 (21.9) | 0.562 |
| Head circumference at birth, centimeters (M, IQR) | 26.5 (25–28.3) | 27 (25.6–28.5) | p = 0.429 U = 468 |
| Inborn (N, %) | 31 (93.9) | 29 (90.6) | 0.672 |
| Arterial cord pH (M, IQR) missing n = 18 | 7.3 (7.2–7.3) | 7.3 (7.2–7.3) | p = 0.676 U = 253.5 |
| Apgar 5 min (M, IQR) | 9 (8–10) | 9 (8–9) | p = 0.325 U = 456 |
| CRIB score (M, IQR) | 6 (3.5–7) | 5 (3–6.8) | p = 0.500 U = 477 |
| Mechanical ventilation, hours (M, IQR) | 0 (0–13) | 0 (0–9.5) | p = 0.510 U = 484.5 |
| Noninvasive ventilation, hours (M, IQR) missing n = 1 | 658.5 (229.5–919.8) | 304.5 (65.3–789.8) | p = 0.093 U = 387 |
| Moderate and severe BPD – bronchopulmonary dysplasia (N, %) | 2 (6.1) | 3 (9.4) | p = 0.443 |
| Postnatal steroids (N, %) | 2 (6.1) | 2 (6.3) | 1 |
| Persistent ductus arteriosus (PDA) (N. %) | 33 (100) | 32 (100) | 0.303 |
| - medical treatment | 3 (9.1) | 6 (18.8) | |
| - surgical ligature | 0 (100) | 0 (100) | |
| Other surgery (N, %) | 1 (3) | 3 (9.4) | 0.355 |
| Early onset sepsis (EOS) (N, %) | 1 (3) | 2 (6.3) | 0.613 |
| Late onset sepsis (LOS) (N, %) | 7 (21.2) | 6 (18.8) | 1 |
| Necrotizing enterocolitis (NEC) (N, %) | 1 (3) | 0 (0) | 1 |
| Intraventricular hemorrhage (IVH) (N, %) | 0.514 | ||
| - grade 1 | 4 (12.1) | 7 (21.9) | |
| - grade 2 | 1 (3) | 1 (3.1) | |
| - grade 3 | 0 (0) | 1 (3.1) | |
| - grade 4 | 0 (0) | 0 (0) | |
| Periventricular leukomalacia (PVL) (N, %) | 33 (100) | 32 (100) | 0.513 |
| - grade 1 | 1 (3) | 2 (6.3) | |
| - grade 2 | 1 (3) | 0 (0) | |
| - grade 3 | 0 (0) | 0 (0) | |
| - grade 4 | 0 (0) | 0 (0) | |
| Retinopathy of prematurity (ROP) (N, %) | 1 (3) | 0 (0) | 1 |
| Abnormal hearing test (N, %) | 1 (3) | 1 (3.1) | 1 |
| Length of stay in level III hospital, days (M, IQR) | 49 (36 – 62) | 37 (21 – 56) | p = 0.198 U = 430 |
| Issue (N, %) | 33 (100) | 32 (100) | 0.136 |
| death | 0 (0) | 0 (0) | |
| transfer to another unit/hospital | 15 (45.5) | 21 (65.6) | |
| discharge home | 18 (54.5) | 11 (34.4) | |
| Intervention group (N = 33) | Control group (N = 32) | p-value | |
|---|---|---|---|
| Six-month CA assessment variables | |||
| Chronological age, months (M, IQR) | 9 (8–9) | 8 (8–9) | p = 0.346 U = 461.5 |
| Corrected age, months (M, IQR) | 6 (6–7) | 6 (6–7) | p = 0.447 U = 476.5 |
| Hospitalization after NICU discharge (N, %) | 7 (21.2) | 8 (25) | 0.775 |
| Relevant medical condition (N, %) | 7 (21.2) | 7 (21.9) | 1 |
| Physiotherapy (N, %) | 15 (45.5) | 10 (31.3) | 0.310 |
| Daycare attendance (N, %) missing n = 2 | 4 (12.1) | 3 (10) | 0.646 |
| Maternal return to work (N, %) missing n = 3 | 23 (69.7) | 18 (62.1) | 0.596 |
| Siblings (N, %) missing n = 1 | 13 (40.6) | 13 (40.6) | 1 |
| Sleep disorder (N, %) | 0 (0) | 2 (6.3) | 0.238 |
| Acquisition of the sitting position (N, %) | 27 (81.8) | 29 (90.6) | 0.475 |
| Acquisition of moving on 4 points (N. %) | 12 (36.4) | 12 (37.5) | 1 |
| Weight at 6 months, grams (M, IQR) | 7400 (6600–8020) | 7175 (6362.5–8462.5) | p = 1 U = 528 |
| Length at 6 months, centimeters (M, IQR) | 68 (65–69) | 67 (64–69.8) | p = 0.721 U = 501 |
| Head circumference at 6 months, centimeters (M, IQR) | 43.2 (42–44.2) | 44 (42.8–44.5) | p = 0.076 U = 393 |
| Neurological exam variables | |||
| Tone disorder (N, %) | 4 (12.1) | 6 (18.8) | 0.511 |
| Visual impairment (N, %) | 2 (6.1) | 2 (6.3) | 1 |
| - strabismus | 1 (3) | 1 (3.1) | |
| - retinal immaturity | 0 (0) | 1 (3.1) | |
| - retinal detachment and retinopathy of prematurity | 1 (3) | 0 (0) | |
| Hearing impairment: abnormal auditory evoked potentials (N, %) | 1 (3) | 0 (0) | 1 |
| Standardised developmental tests | |||
| Bayley—cognition scale (M, IQR) | 110 (105–115) n = 20 | 115 (106.3–115) n = 16 | p = 0.102 U = 110.5 |
| Bayley—language scale (M, IQR) | 94 (91–100) n = 20 | 97 (91.8–102.3) n = 16 | p = 0.479 U =138 |
| Bayley—motor scale (M, IQR) | 97 (85–106) n = 20 | 100 (91.8–111.5) n = 16 | p = 0.315 U = 128.5 |
| Griffiths—developmental quotient (M, IQR) | 99 (96.3–110.8) n = 12 | 100 (92–103) n = 15 | p = 0.591 U = 79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lovey, O.; Bickle-Graz, M.; Morisod Harari, M.; Horsch, A.; Schneider, J., on behalf of the JOIN Research Consortium. The Joint Observation in Neonatology and Neurodevelopmental Outcome of Preterm Infants at Six Months Corrected Age: Secondary Outcome Data from a Randomised Controlled Trial. Children 2022, 9, 1380. https://doi.org/10.3390/children9091380
Lovey O, Bickle-Graz M, Morisod Harari M, Horsch A, Schneider J on behalf of the JOIN Research Consortium. The Joint Observation in Neonatology and Neurodevelopmental Outcome of Preterm Infants at Six Months Corrected Age: Secondary Outcome Data from a Randomised Controlled Trial. Children. 2022; 9(9):1380. https://doi.org/10.3390/children9091380
Chicago/Turabian StyleLovey, Oriane, Myriam Bickle-Graz, Mathilde Morisod Harari, Antje Horsch, and Juliane Schneider on behalf of the JOIN Research Consortium. 2022. "The Joint Observation in Neonatology and Neurodevelopmental Outcome of Preterm Infants at Six Months Corrected Age: Secondary Outcome Data from a Randomised Controlled Trial" Children 9, no. 9: 1380. https://doi.org/10.3390/children9091380
APA StyleLovey, O., Bickle-Graz, M., Morisod Harari, M., Horsch, A., & Schneider, J., on behalf of the JOIN Research Consortium. (2022). The Joint Observation in Neonatology and Neurodevelopmental Outcome of Preterm Infants at Six Months Corrected Age: Secondary Outcome Data from a Randomised Controlled Trial. Children, 9(9), 1380. https://doi.org/10.3390/children9091380