
Perceived Psychological Impact on Children and Parents of Experiencing COVID-19 Infection in One or More Family Members

 ,
,  , ,
, ,  , ,
, , Highlights
- The study explores the psychological impact on parents and children who have experienced COVID-19 within their families.
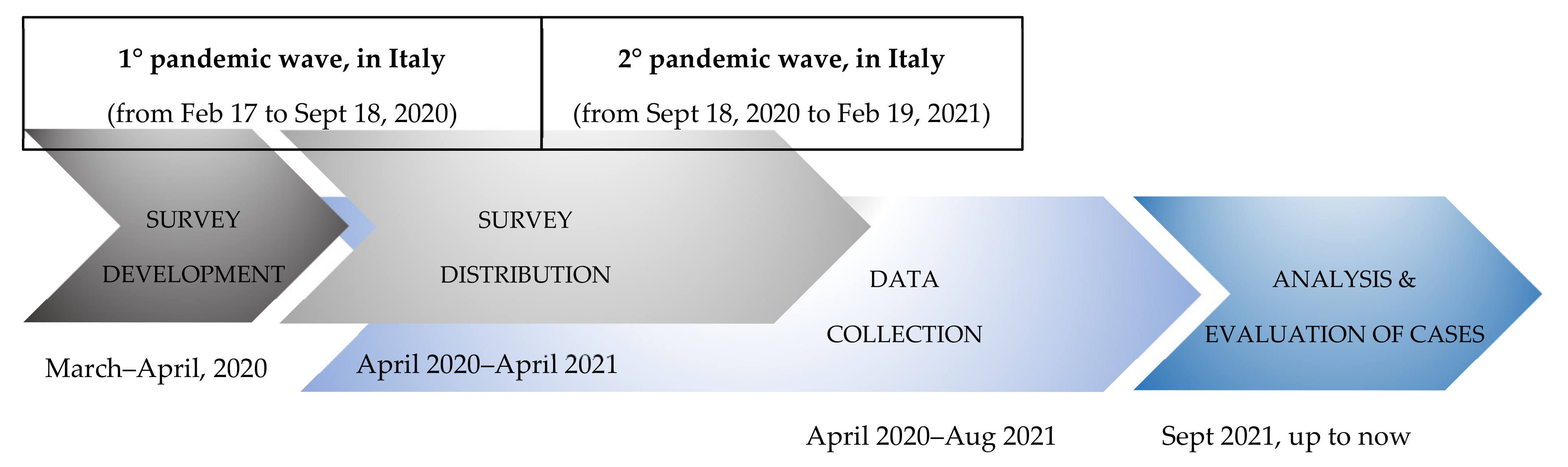
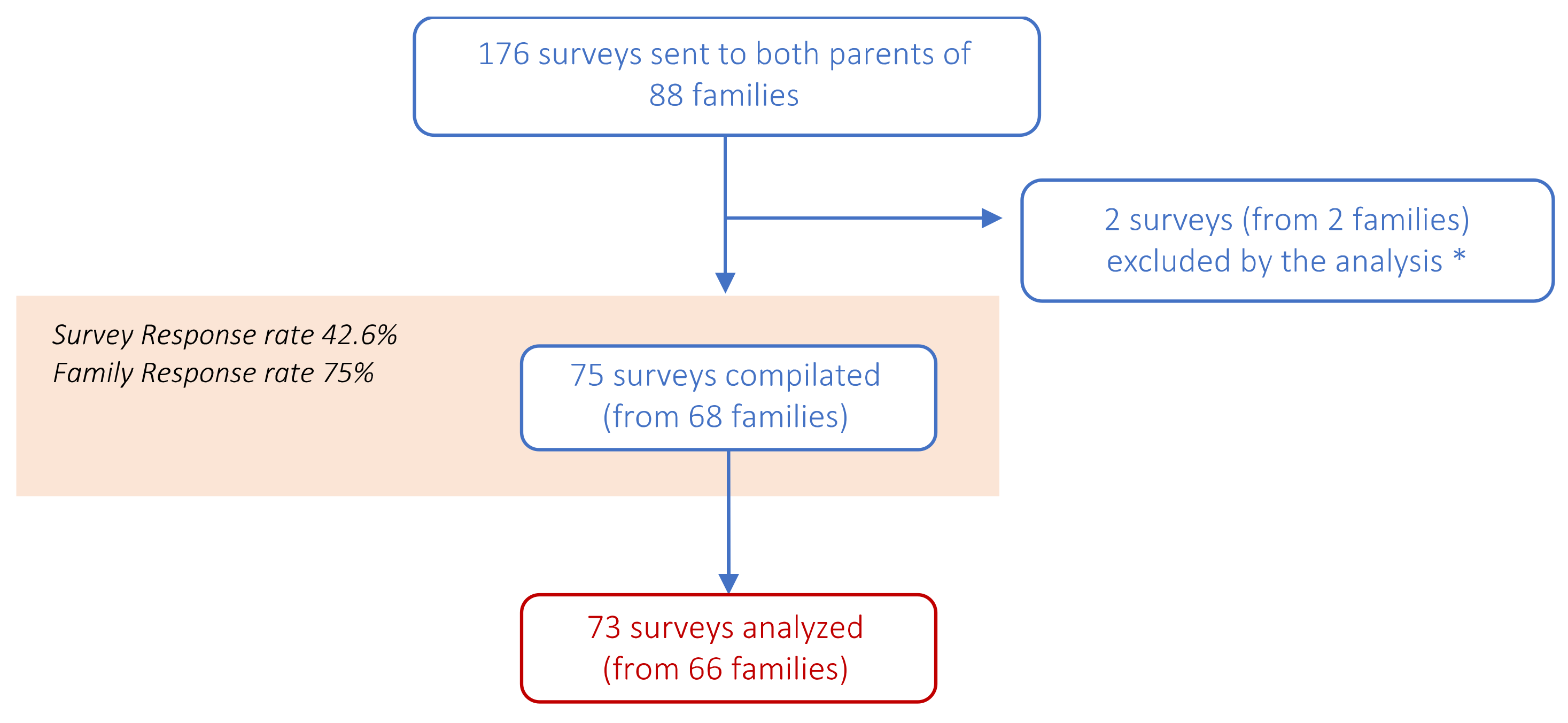
- A cross-sectional, web-based survey was obtained from 68 families who attended a COVID-19 Follow-up Clinic in Italy.
- A majority of the parents reported positive relationships with family members before, during, and after COVID-19.
- Children and adolescents had difficulty adapting to isolation, with changes in functions such as circadian rhythm, relationships with parents, and emotional control reported.
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Instruments
2.2.1. Family Relationships Evaluation
2.2.2. Child Emotional and Behavioral Problems and Adaptation to Home Isolation
2.3. Clinical Data Collection and Definitions
2.4. Statistical Analysis
3. Results
3.1. Results from the “Questionnaire A—Family”
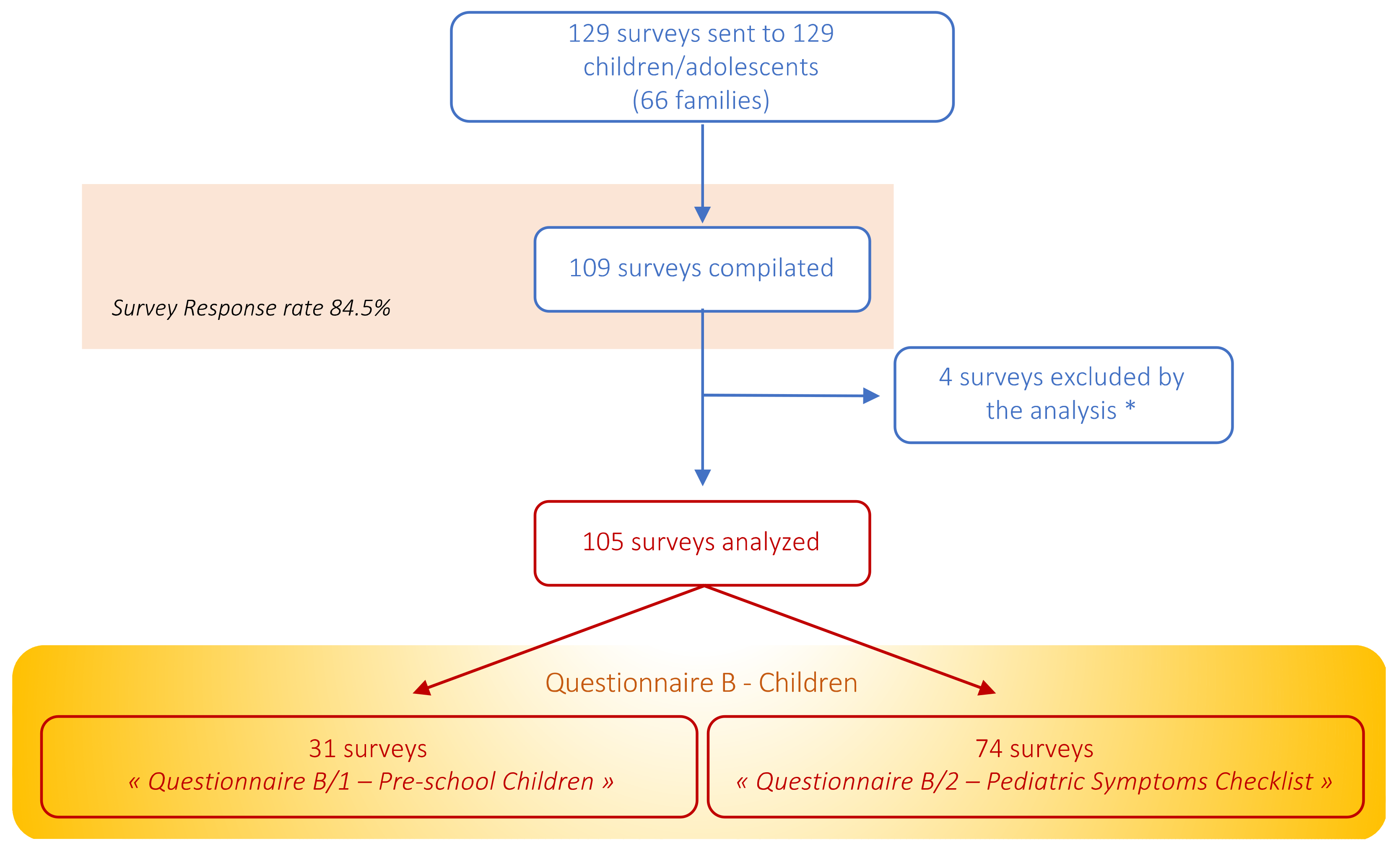
3.2. Results from the “Questionnaire B—Children”
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.K.T.; de Medeiros Carvalho, P.M.; Lima, I.D.A.A.S.; de Oliveira Nunes, J.V.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.; Neto, M.L. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef] [PubMed]
- Petrocchi, S.; Levante, A.; Bianco, F.; Castelli, I.; Lecciso, F. Maternal distress/coping and children’s adaptive behaviors during the covid-19 lockdown: Mediation through children’s emotional experience. Front. Public Health 2020, 8, 587833. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S. Stress: Appraisal and Coping. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Greenberg, J.; Solomon, S.; Pyszczynski, T. Terror management theory of self-esteem and cultural worldviews: Empirical assessments and conceptual refinements. In Advances in Experimental Social Psychology; Zanna, M.P., Ed.; Academic Press: New York, NY, USA, 1997; Volume 29, pp. 61–139. [Google Scholar]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Biondi, S.; Casale, S.; Burrai, J.; Mazza, C.; Cavaggioni, G.; Ferracuti, S.; Giannini, A.M.; Roma, P. Personality and Lockdown: A Study on Italian Undergraduates During the COVID-19 Pandemic. Front. Psychiatry 2021, 28, 622366. [Google Scholar] [CrossRef]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among italian people during the covid-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Peñuelas, J.; Sardans, J. The global nitrogen-phosphorus imbalance. Science 2022, 375, 266–267. [Google Scholar] [CrossRef]
- Maas, J.; van Dillen, S.M.E.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Aljunaidy, M.M.; Adi, M.N. The psychological impact of COVID-19 quarantine on children, and the role of parental support and physical environment design. Discov. Psychol. 2021, 1, 2. [Google Scholar] [CrossRef]
- Orgilés, M.; Morales, A.; Delvecchio, E.; Mazzeschi, C.; Espada, J.P. Immediate Psychological Effects of the COVID-19 Quarantine in Youth From Italy and Spain. Front. Psychol. 2020, 11, 2986. [Google Scholar] [CrossRef] [PubMed]
- Cluver, L.; Lachman, J.M.; Sherr, L.; Wessels, I.; Krug, E.; Rakotomalala, S.; Blight, S.; Hillis, S.; Bachman, G.; Green, O.; et al. Parenting in a time of COVID-19. Lancet 2020, 395, e64. [Google Scholar] [CrossRef]
- Johnson, M.S.; Skjerdingstad, N.; Ebrahimi, O.v.; Hoffart, A.; Johnson, S.U. Mechanisms of parental distress during and after the first COVID-19 lockdown phase: A two-wave longitudinal study. PLoS ONE 2021, 16, e0253087. [Google Scholar] [CrossRef]
- Wang, C.; Zhou, L.; Chen, J. The differences of clinical characteristics and outcomes between imported and local patients of COVID-19 in Hunan: A two-center retrospective study. Respir. Res. 2020, 21, 313. [Google Scholar] [CrossRef]
- Narzisi, A. Handle the autism spectrum condition during coronavirus (COVID-19) stay at home period: Ten tips for helping parents and caregivers of young children. Brain Sci. 2020, 10, 207. [Google Scholar] [CrossRef] [PubMed]
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, V.; Nixon, M.; Ma, D.W.L.; Haines, J. The impact of covid-19 on health behavior, stress, financial and food security among middle to high income canadian families with young children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef]
- Koenig, J.; Kohls, E.; Moessner, M.; Lustig, S.; Bauer, S.; Becker, K.; Thomasius, R.; Eschenbeck, H.; Diestelkamp, S.; Gillé, V.; et al. The impact of COVID-19 related lockdown measures on self-reported psychopathology and health-related quality of life in German adolescents. Eur. Child Adolesc. Psychiatry 2021, 10, 1–10. [Google Scholar] [CrossRef]
- Rodman, A.M.; Rosen, M.L.; Kasparek, S.W.; Mayes, M.; Lengua, L.; McLaughlin, K.A.; Meltzoff, A.N. Social behavior and youth psychopathology during the COVID-19 pandemic: A longitudinal study. PsyArXiv Prepr. 2021. [Google Scholar] [CrossRef]
- Hill, D.L.; Christakis, D.A.; Feudtner, C. Illness in the Family and Shared Stress, Work, and Struggle. JAMA Pediatr. 2022, 176, 549–550. [Google Scholar] [CrossRef]
- Humphrey, L.M.; Hill, D.L.; Carroll, K.W.; Rourke, M.; Kang, T.I.; Feudtner, C. Psychological well-being and family environment of siblings of children with life threatening illness. J. Palliat. Med. 2015, 18, 981–984. [Google Scholar] [CrossRef] [PubMed]
- Jellinek, M.S.; Murphy, J.M.; Little, M.M.; Maria, E.; Pagano, M.; Diane, M.; Kelleher, K.J. Use of the Pediatric Symptom Checklist to Screen for Psychosocial Problems in Pediatric Primary Care: A National Feasibility Study. Arch. Pediatr. Adolesc. Med. 1999, 153, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Di Chiara, C.; Cantarutti, A.; Costenaro, P.; Donà, D.; Bonfante, F.; Cosma, C.; Ferrarese, M.; Cozzani, S.; Petrara, M.R.; Carmona, F.; et al. Long-term Immune Response to SARS-CoV-2 Infection among Children and Adults after Mild Infection. JAMA Netw. Open 2022, 5, e2221616. [Google Scholar] [CrossRef] [PubMed]
- Terrone, G.; Parente, I.; Romano, A.; Auricchio, R.; Greco, L.; Del Giudice, E. The Pediatric Symptom Checklist as screening tool for neurological and psycho-social problems in a paediatric cohort of patients with coeliac disease. Acta Paediatr. 2013, 102, e325–e328. [Google Scholar] [CrossRef]
- Oliva, S.; Russo, G.; Gili, R.; Russo, L.; Di Mauro, A.; Spagnoli, A.; Alunni Fegatelli, D.; Romani, M.; Costa, A.; Veraldi, S.; et al. Risks and Protective Factors Associated with Mental Health Symptoms during COVID-19 Home Confinement in Italian Children and Adolescents: The #Understandingkids Study. Front. Pediatr. 2021, 9, 664702. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19: Interim Guid 27 May 2020; WHO/2019-nCoV/clinical/2020.5; World Health Organization: Geneva, Switzerland, 2020; pp. 1–62. [Google Scholar]
- Chang, S.H.; Cataldo, J.K. A systematic review of global cultural variations in knowledge, attitudes and health responses to tuberculosis stigma. Int. J. Tuberc. Lung Dis. 2014, 18, 168–173. [Google Scholar] [CrossRef]
- Lin, E.C.L.; Peng, Y.C.; Hung Tsai, J.C. Lessons learned from the anti-SARS quarantine experience in a hospital-based fever screening station in Taiwan. Am. J. Infect. Control 2010, 38, 302–307. [Google Scholar] [CrossRef]
- Yuan, Y.; Zhao, Y.J.; Zhang, Q.E.; Zhang, L.; Cheung, T.; Jackson, T.; Jiang, G.Q.; Xiang, Y.T. COVID-19-related stigma and its sociodemographic correlates: A comparative study. Glob. Health 2021, 17, 54. [Google Scholar] [CrossRef]
- Brown, S.M.; Doom, J.R.; Lechuga-Peña, S.; Watamura, S.E.; Koppels, T. Stress and parenting during the global COVID-19 pandemic. Child Abus. Negl. 2020, 110, 104699. [Google Scholar] [CrossRef]
- Cusinato, M.; Iannattone, S.; Spoto, A.; Poli, M.; Moretti, C.; Gatta, M.; Miscioscia, M. Stress, resilience, and well-being in Italian children and their parents during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8297. [Google Scholar] [CrossRef]
- Shah, S.; Kaul, A.; Shah, R.; Maddipoti, S. Impact of Coronavirus Disease 2019 Pandemic and Lockdown on Mental Health Symptoms in Children. Indian Pediatr. 2021, 58, 75–76. [Google Scholar] [PubMed]
- Tan, Y.; Huang, C.; Geng, Y.; Cheung, S.P.; Zhang, S. Psychological Well-Being in Chinese College Students during the COVID-19 Pandemic: Roles of Resilience and Environmental Stress. Front. Psychol. 2021, 12, 671553. [Google Scholar] [CrossRef] [PubMed]
- Bosch, R.; Pagerols, M.; Prat, R.; Español-Martín, G.; Rivas, C.; Dolz, M.; Haro, J.M.; Ramos-Quiroga, J.A.; Ribasés, M.; Casas, M. Changes in the Mental Health of Children and Adolescents during the COVID-19 Lockdown: Associated Factors and Life Conditions. Int. J. Environ. Res. Public Health 2022, 19, 4120. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Children (n = 129) | Parents | ||
|---|---|---|---|
| Overall (n = 97) | Survey’s Respondents (n = 73) | ||
| Time (days) from baseline to survey completion (mean, DS) * | - | - | 164.71 (56.03) |
| Age at survey completion (mean, DS) | 10 (5.6) | 43 (7.8) | 43.3 (7.2) |
| Gender (female), n (%) | 58 (44.9%) | 63 (64.9%) | 58 (79.5%) |
| Nationality | |||
| Italian | 120 (93%) | 89 (91.7%) | 66 (90.4%) |
| Other | 9 (6.9%) | 8 (8.2%) | 7 (9.6%) |
| Comorbidities§ | 22 (17%) | 10 (10.3%) | 10 (13.7%) |
| Positive SARS-CoV-2 Nasal-Pharyngeal Swab (n, %) | 77 (59.7%) | 64 (65.9%) | 52 (71.2%) |
| Confirmed COVID-19 (n, %) | 92 (71.3%) | 72 (74.2%) | 55 (75.3%) |
| COVID-19 clinical presentation (among confirmed cases): | |||
| asymptomatic | 20 (21.7%) | 5 (6.9%) | 4 (7.3%) |
| mild COVID-19 | 71 (77.2%) | 61 (84.7%) | 49 (89.1%) |
| moderate/severe COVID-19 | 0 | 4 (4.1%) | 1 (1.8%) |
| critical COVID-19 | 1 (MIS-C) | 1 (1%) | 1 (1.8%) |
| Pandemic wave | |||
| 1st wave | 72 (55.8%) | 67 (69%) | 44 (60.3%) |
| 2nd wave | 57 (44.2%) | 30 (30.9%) | 29 (39.7%) |
| Total (n = 73) | 1st Wave (n = 44) | 2nd Wave (n = 29) | p-Value * | |
|---|---|---|---|---|
| Time from baseline to survey compilation, days (mean, DS) | 164.7 (56) | 165,3 (64.8) | 163,7 (40.2) | 0.1724 |
| Diagnosis of COVID-19 was shared with people other than close contacts (yes/total answer) | 69/72 (95.8%) | 42/43 (97.7%) | 27/29 (93.1%) | 0.561 |
| Fear of a people’s behavioural change, after the communication of COVID-19 (yes/total answer) | 39/73 (53.4%) | 22/44 (50%) | 17/29 (58.6%) | 0.485 |
| Objective finding of people’s behavioural change, after the communication of COVID-19 (yes/total answer) | 22/72 (30.5%) | 11/43 (25.6%) | 11/29 (37.9%) | 0.304 |
| Type of observed behavioral change (negative) | 8/22 (36.4%) | 8/11 (72.7%) | 0/11 (0%) | 0.001 |
| Before COVID-19 | ||||
| Quality of the relationship with the partner (≥3) | 65/67 (97%) | 38/39 (97.4%) | 27/28 (96.4%) | 1.000 |
| Quality of the relationship with son/daughters (≥3) | 73/73 (100%) | 44/44 (100%) | 29/29 (100%) | - |
| Quality of the relationship within siblings (≥3) | 42/42 (100%) | 17/17 (100%) | 25/25 (100%) | - |
| During COVID-19 | ||||
| Quality of the relationship with the partner (≥3) | 59/66 (89.4%) | 36/38 (94.7%) | 23/28 (82.1%) | 0.125 |
| Quality of the relationship with son/daughters (≥3) | 68/71 (95.8%) | 42/42 (100%) | 26/29 (89.6%) | 0.064 |
| Quality of the relationship within siblings (≥3) | 34/39 (87.2%) | 13/14 (92.9%) | 21/25 (84%) | 0.636 |
| At survey compilation | ||||
| Quality of the relationship with the partner (≥3) | 65/68 (95.6%) | 38/40 (95%) | 27/28 (96.4%) | 1.000 |
| Quality of the relationship with son/daughters (≥3) | 72/73 (98.6%) | 43/44 (97.7%) | 29/29 (100%) | 1.000 |
| Quality of the relationship within siblings (≥3) | 40/41 (97.6%) | 15/16 (93.7%) | 25/25 (100%) | 0.390 |
| Responder was working before COVID-19 (yes) | 56/72 (77.8%) | 36/44 (81.8%) | 20/28 (71.4%) | 0.386 |
| Impact of COVID-19 on work (yes) | 20/66 (30.3%) | 13/39 (33.3%) | 7/27 (25.9%) | 0.593 |
| Negative impact | 8/9 § |
| TOT (n = 31) | COVID-19 CASE (n = 20) | COVID-19 Negative (n = 11) | p-Value * | |
|---|---|---|---|---|
| Age at survey compilation, mean (DS) | 3.01 (1.71) | 2.85 (1.86) | 3.33 (1.43) | 0.232 |
| Gender (female) | 14/31 (45.2%) | 9/20 (45%) | 5/11 (45.5%) | 1.000 |
| Comorbidities (yes) | 5/31 (16.1%) | 4/20 (20%) | 1/11 (9%) | 0.631 |
| Scarce ability to adapt to isolation (≥3) | 11/31 (35.5%) | 7/20 (35%) | 4/11 (36.4%) | 1.000 |
| Functional change occurred during isolation (yes) | 23/31 (74.2%) | 13/20 (65%) | 10/11 (90.9%) | 0.203 |
| Change in circadian rhythm (yes) | 7/28 (25%) | 4/18 (22.2%) | 3/10 (30%) | 0.674 |
| Change in nutrition (yes) | 3/25 (12%) | 3/15 (20%) | 0/10 (0%) | 0.250 |
| Change in sphincteric control (yes) | 2/22 (9.1%) | 2/12 (16.7%) | 0/10 (0%) | 0.481 |
| Speech alteration (yes) | 3/26 (11.5%) | 3/16 (18.7%) | 0/10 (0%) | 0.262 |
| Play alteration (yes) | 5/27 (18.5%) | 4/17 (23.5%) | 1/10 (10%) | 0.621 |
| Change in body care (yes) | 4/23 (17.4%) | 0/12 (0%) | 4/11 (36.4%) | 0.037 |
| Change in emotional expression and control (yes) | 9/25 (36%) | 4/14 (28.6%) | 5/11 (45.5%) | 0.434 |
| Change in relationship with parents (yes) | 12/28 (42.8%) | 6/17 (21.4%) | 6/11 (21.4%) | 0.441 |
| Change in relationship with siblings (yes) | 7/25 (28%) | 4/14 (28.6%) | 3/11 (27.3%) | 1.000 |
| TOT (n = 74) | COVID-19 CASES (n = 62) | COVID-19 Negative (n = 12) | p-Value * | |
|---|---|---|---|---|
| Age at survey compilation, mean (DS) | 10.9 (2.7) | 10.3 (2.7) | 10.9 (2.7) | 0.775 |
| Gender (female) | 29 (39.2%) | 23 (37%) | 6 (50%) | 0.521 |
| Comorbidities (yes) | 17 (22.9%) | 14 (22.6%) | 3 (25%) | 1.000 |
| Scarce ability to adapt to isolation (≥3) | 27/73 (36.9%) | 23/61 (37.7%) | 4/12 (33.3%) | 1.000 |
| Functional change occurred during isolation, any (yes) | 74 (100%) | 62 (100%) | 12 (100%) | - |
| Pediatric Symptom Checklist (PSC) scores of≥28 | 6/74 (8.1%) | 5/62 (8%) | 1/12 (8.3%) | 1.000 |
| Attention Problems subscale (≥7) | 12/72 (16.7%) | 11/60 (18.3%) | 1/12 (8.3%) | 0.676 |
| Internalizing Problems subscale (≥5) | 4/74 (5.4%) | 4/62 (6.5%) | 0/12 | 1.000 |
| Externalizing Problems subscale (≥7) | 4/72 (5.6%) | 4/60 (6.7%) | 0/12 | 1.000 |
| Complains of aches/pains (≥1) | 23/70 (32.9%) | 21/59 (35.6%) | 2/11 (18.2%) | 0.318 |
| Spends more time alone (≥1) | 28/71 (39.4%) | 24/60 (40%) | 4/11 (36.4%) | 1.000 |
| Tires easily, has little energy (≥1) | 37/72 (51.4%) | 33/60 (55%) | 4/12 (33.3%) | 0.214 |
| Fidgety, unable to sit still (≥1) | 34/72 (47.2%) | 30/60 (50%) | 4/12 (33.3%) | 0.354 |
| Has trouble with a teacher (≥1) | 17/72 (23.6%) | 15/60 (25%) | 2/12 (16.7%) | 0.719 |
| Less interested in school (≥1) | 43/72 (59.7%) | 36/60 (60%) | 7/12 (58.3%) | 1.000 |
| Acts as if driven by a motor (≥1) | 24/72 (33.3%) | 21/60 (35%) | 3/12 (25%) | 0.739 |
| Daydreams too much (≥1) | 31/72 (43.1%) | 25/60 (41.7%) | 6/12 (50%) | 0.751 |
| Distracted easily (≥1) | 48/72 (66.7%) | 40/60 (66.7%) | 8/12 (66.7%) | 1.000 |
| Is afraid of new situations (≥1) | 37/72 (51.4%) | 31/60 (51.7%) | 6/12 (50%) | 1.000 |
| Feels sad, unhappy (≥1) | 26/72 (36.1%) | 20/60 (33.3%) | 6/12 (50%) | 0.330 |
| Is irritable, angry (≥1) | 39/72 (54.2%) | 33/60 (55%) | 6/12 (50%) | 0.762 |
| Feels hopeless (≥1) | 7/72 (9.7%) | 6/60 (10%) | 1/12 (8.3%) | 1.000 |
| Has trouble concentrating (≥1) | 38/72 (52.8%) | 32/60 (53.3%) | 6/12 (50%) | 1.000 |
| Less interest in friends (≥1) | 18/72 (25%) | 15/60 (25%) | 3/12 (25%) | 1.000 |
| Fights with others (≥1) | 31/72 (43%) | 29/60 (48.3%) | 2/12 (16.7%) | 0.057 |
| Absent from online school (≥1) | 16/72 (22.2%) | 14/60 (23.3%) | 2/12 (16.7%) | 1.000 |
| School grades dropping (≥1) | 25/72 (34.7%) | 22/60 (36.7%) | 3/12 (25%) | 0.524 |
| Is down on him or herself (≥1) | 16/72 (22.2%) | 13/60 (21.7%) | 3/12 (25%) | 0.722 |
| Visits doctor with doctor finding nothing wrong (≥1) | 5/72 (6.9%) | 3/60 (4.2%) | 2/12 (2.8%) | 0.191 |
| Has trouble sleeping (≥1) | 21/71 (29.6%) | 17/59 (28.8%) | 4/12 (33.3%) | 0.740 |
| Worries a lot (≥1) | 36/74 (48.6%) | 30/62 (48.4%) | 6/12 (50%) | 1.000 |
| Wants to be with you more than before (≥1) | 38/70 (54.3%) | 32/59 (54.3%) | 6/11 (54.5%) | 1.000 |
| Feels he or she is bad (≥1) | 8/70 (11.4) | 7/59 (11.9%) | 1/11 (9.1%) | 1.000 |
| Takes unnecessary risks (≥1) | 5/69 (7.3%) | 5/58 (8.6%) | 0/11 | 0.585 |
| Gets hurt frequently (≥1) | 5/69 (7.3%) | 5/58 (8.6%) | 0/11 | 0.585 |
| Seems to be having less fun (≥1) | 23/70 (32.9%) | 18/59 (30.5%) | 5/11 (45.5%) | 0.485 |
| Acts younger than children his or her age (≥1) | 16/68 (23.5%) | 15/57 (26.3%) | 1/11(9.1%) | 0.437 |
| Does not listen to rules (≥1) | 28/68 (41.2%) | 24/57 (42.1%) | 4/11 (36.4%) | 1.000 |
| Does not show feelings (≥1) | 16/69 (23.2%) | 14/58 (24.1%) | 2/11 (18.2%) | 1.000 |
| Does not understand other people’s feeling (≥1) | 12/69 (17.4%) | 10/58 (17.4%) | 2/11 (18.2%) | 1.000 |
| Teases others (≥1) | 27/67 (40.3%) | 24/57 (42.1%) | 3/10 (30%) | 0.728 |
| Blames others for his or her troubles (≥1) | 21/67 (31.3%) | 17/57 (29.8%) | 4/10 (40%) | 0.713 |
| Takes things that do not belong to him or her (≥1) | 9/67 (13.4%) | 7/57 (12.3%) | 2/10 (20%) | 0.614 |
| Refuses to share (≥1) | 16/66 (24.4%) | 13/56 (23.2%) | 3/10 (30%) | 0.695 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costenaro, P.; Di Chiara, C.; Boscolo, V.; Barbieri, A.; Tomasello, A.; Cantarutti, A.; Cozzani, S.; Liberati, C.; Oletto, S.; Giaquinto, C.; et al. Perceived Psychological Impact on Children and Parents of Experiencing COVID-19 Infection in One or More Family Members. Children 2022, 9, 1370. https://doi.org/10.3390/children9091370
Costenaro P, Di Chiara C, Boscolo V, Barbieri A, Tomasello A, Cantarutti A, Cozzani S, Liberati C, Oletto S, Giaquinto C, et al. Perceived Psychological Impact on Children and Parents of Experiencing COVID-19 Infection in One or More Family Members. Children. 2022; 9(9):1370. https://doi.org/10.3390/children9091370
Chicago/Turabian StyleCostenaro, Paola, Costanza Di Chiara, Valentina Boscolo, Alessia Barbieri, Alice Tomasello, Anna Cantarutti, Sandra Cozzani, Cecilia Liberati, Serenella Oletto, Carlo Giaquinto, and et al. 2022. "Perceived Psychological Impact on Children and Parents of Experiencing COVID-19 Infection in One or More Family Members" Children 9, no. 9: 1370. https://doi.org/10.3390/children9091370
APA StyleCostenaro, P., Di Chiara, C., Boscolo, V., Barbieri, A., Tomasello, A., Cantarutti, A., Cozzani, S., Liberati, C., Oletto, S., Giaquinto, C., & Donà, D. (2022). Perceived Psychological Impact on Children and Parents of Experiencing COVID-19 Infection in One or More Family Members. Children, 9(9), 1370. https://doi.org/10.3390/children9091370