
Clinical and Evolutionary Features of SARS-CoV-2 Infection (COVID-19) in Children, a Romanian Perspective

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Material and Method
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Harwood, R.; Yan, H.; Da Camara, N.T.; Smith, C.; Ward, J.; Tudur-Smith, C.; Linney, M.; Clark, M.; Whittaker, E.; Saatci, D.; et al. Which children and young people are at higher risk of severe disease and death after hospitalisation with SARS-CoV-2 infection in children and young people: A systematic review and individual patient meta-analysis. EClinicalMedicine 2022, 44, 101287. [Google Scholar] [CrossRef] [PubMed]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; Mancini, A.; et al. COVID-19 Infection in Children and Infants: Current Status on Therapies and Vaccines. Children 2022, 9, 249. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 14 June 2022).
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics against Coronavirus (COVID-19). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Huang, C.L.; Wang, Y.M.; Li, X.W.; Ren, L.L.; Zhao, J.P.; Hu, Y.; Zhang, L.; Fan, G.H.; Xu, J.Y.; Gu, X.Y.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Anca Pantea Stoian, Mihaela Pricop-Jeckstadt, Adrian Pana, Bogdan-Vasile Ileanu, Ruxandra Schitea, and All-Death by SARS-CoV-2: A Romanian COVID-19 Multi-Centre Comorbidity Study–Scientific Report. Available online: www.nature.com/scientificreports (accessed on 29 June 2022).
- Hoanga, A.; Choratha, K.; Moreirab, A.; Evansa, M.; Burmeister, F.; Burmeistera, F.; Naqvia, R.; Petershacka, M.; Moreira, A. COVID-19 in 7780 Pediatric Patients: A Systematic Review. EClinicalMedicine 2020, 24, 100433. Available online: https://www.journals.elsevier.com/eclinicalmedicine (accessed on 29 June 2022). [CrossRef]
- Satdhabudha, A.; Chaiyakulsil, C.; Sritipsukho, P.; Sinlapamongkolkul, P.; Chaumrattanakul, U.; Tangsathapornpong, A.; Bunjoungmanee, P.; Thaweekul, P.; Kwankua, A.; Pharadornuwat, O.; et al. Original Article-Epidemiological and Clinical Characteristics of Pediatric COVID-19 in the Tertiary Care System in Thailand: Comparative Delta and Pre-Delta Era. Mediterr. J. Hematol. Infect. Dis. 2022, 14, e2022044. [Google Scholar] [CrossRef]
- Ho, C.L.T.; Oligbu, P.; Ojubolamo, O.; Pervaiz, M.; Oligbu, G. Clinical Characteristics of Children with COVID-19. AIMS Public Health 2020, 7, 258–273. [Google Scholar] [CrossRef]
- Qiu, H.; Wu, J.; Hong, L.; Luo, Y.; Song, Q.; Chen, D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef]
- Garazzino, S.; Lo Vecchio, A.; Pierantoni, L.; Calò Carducci, F.I.; Marchetti, F.; Meini, A.; Castagnola, E.; Vergine, G.; Donà, D.; Bosis, S.; et al. Epidemiology, Clinical Features and Prognostic Factors of Pediatric SARS-CoV-2 Infection: Results From an Italian Multicenter Study. Front. Pediatr. 2021, 16, 649358. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Girona-Alarcon, M.; on behalf of the KIDS-Corona study group; Bobillo-Perez, S.; Sole-Ribalta, A.; Hernandez, L.; Guitart, C.; Suarez, R.; Balaguer, M.; Cambra, F.-J.; Jordan, I.; et al. The different manifestations of COVID-19 in adults and children: A cohort study in an intensive care unit. BMC Infect. Dis. 2021, 21, 87. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Liguoro, I.; Pilotto, C.; Bonanni, M.; Ferrari, M.E.; Pusiol, A.; Nocerino, A.; Vidal, E.; Cogo, P. SARS-COV-2 infection in children and newborns: A systematic review. Eur. J. Pediatr. 2020, 179, 1029–1046, Erratum in Eur. J. Pediatr. 2021, 180, 2343. [Google Scholar] [CrossRef] [PubMed]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Santacroce, L.; Marinelli, G.; Mancini, A.; Vimercati, L.; Maggiore, M.E.; D’Oria, M.T.; Hazballa, D.; et al. COVID-19 Infection in Children, Infants and Pregnant Subjects: An Overview of Recent Insights and Therapies. Microorganisms 2021, 9, 1964. [Google Scholar] [CrossRef] [PubMed]
- Gu, H.; Xie, Z.; Li, T.; Zhang, S.; Lai, C.; Zhu, P.; Wang, K.; Han, L.; Duan, Y.; Zhao, Z.; et al. Angiotensin-Converting Enzyme 2 Inhibits Lung Injury Induced by Respiratory Syncytial Virus. Sci. Rep. 2016, 6, 19840. [Google Scholar] [CrossRef]
- Mehta, N.S.; Mytton, O.T.; Mullins, E.W.S.; Fowler, T.A.; Falconer, C.L.; Murphy, O.B.; Langenberg, C.; Jayatunga, W.J.P.; Eddy, D.H.; Nguyen-Van-Tam, J.S. SARS-CoV-2 (COVID-19): What Do We Know about Children? A Systematic Review. Clin. Infect. Dis. 2020, 71, 2469–2479. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Carducci, F.I.C.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Pang, J.; Liu, M.; Ling, W.; Jin, T. Friend or foe? ACE2 inhibitors and GLP-1R agonists in COVID-19 treatment. Obes. Med. 2021, 22, 100312. [Google Scholar] [CrossRef]
- Wong, A.C.P.; Li, X.; Lau, S.K.P.; Woo, P.C.Y. Global epidemiology of bat coronaviruses. Viruses 2019, 11, 174. [Google Scholar] [CrossRef] [PubMed]
- Hikmet, F.; Méar, L.; Edvinsson, Å.; Micke, P.; Uhlén, M.; Lindskog, C. The protein expression profile of ACE2 in human tissues. Mol. Syst. Biol. 2020, 16, e9610. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.-Q.; Chen, D.-H.; Tan, W.-P.; Qiu, S.-Y.; Xu, D.; Liang, H.-X.; Chen, M.-X.; Li, X.; Lin, Z.-S.; Liu, W.-K.; et al. Epidemiology and clinical characteristics of human coronaviruses OC43, 229E, NL63, and HKU1: A study of hospitalized children with acute respiratory tract infection in Guangzhou, China. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Sharun, K.; Tiwari, R.; Dadar, M.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W. COVID-19, an emerging coronavirus infection: Advances and prospects in designing and developing vaccines, immunotherapeutics and therapeutics—A mini-review. Hum. Vaccin. Immunother. 2020, 16, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Monchatre-Leroy, E.; Boué, F.; Boucher, J.-M.; Renault, C.; Moutou, F.; Gouilh, M.A.; Umhang, G. Identification of alpha and beta coronavirus in wildlife species in France: Bats, rodents, rabbits, and hedgehogs. Viruses 2017, 9, 364. [Google Scholar] [CrossRef]
- Parri, N.; Magistà, A.M.; Marchetti, F.; Cantoni, B.; Arrighini, A.; Romanengo, M.; Felici, E.; Urbino, A.; Da Dalt, L.; Verdoni, L.; et al. Characteristic of COVID-19 infection in pediatric patients: Early findings from two Italian Pediatric Research Networks. Eur. J. Pediatr. 2020, 179, 1315–1323. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef]
- Musolino, A.M.; Ferro, V.; Supino, M.C.; Boccuzzi, E.; Scateni, S.; Sinibaldi, S.; Cursi, L.; Schingo, P.M.S.; Reale, A.; Campana, A.; et al. One Year of Lung Ultrasound in Children with SARS-CoV-2 Admitted to a Tertiary Referral Children’s Hospital: A Retrospective Study during 2020–2021. Children 2022, 9, 761. [Google Scholar] [CrossRef]
- Streinu-Cercel, A.; Apostolescu, C.; Săndulescu, O.; Oţelea, D.; Streinu-Cercel, A.; Vlaicu, O.; Paraschiv, S.; Benea, O.E.; Bacruban, R.; Niţescu, M.; et al. SARS-CoV-2 in Romania-analysis of the first confirmed case and evolution of the pandemic in Romania in the first three months. Germs 2020, 10, 132–134. [Google Scholar] [CrossRef]
- Streinu-Cercel, A. SARS-CoV-2 in Romania–situation update and containment strategies. Germs 2020, 10, 8. [Google Scholar] [CrossRef]
- Castagnoli, R.; Votto, M.; Licari, A.; Brambilla, I.; Bruno, R.; Perlini, S.; Rovida, F.; Baldanti, F.; Marseglia, G.L. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents. JAMA Pediatr. 2020, 174, 882. [Google Scholar] [CrossRef] [PubMed]
- Swann, O.V.; Holden, K.A.; Turtle, L.; Pollock, L.; Fairfield, C.J.; Drake, T.M.; Seth, S.; Egan, C.; Hardwick, H.E.; Halpin, S.; et al. Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: Prospective multicenter observational cohort study. BMJ 2020, 370, m3249. [Google Scholar] [CrossRef] [PubMed]
- Albuali, W.H.; AlGhamdi, A.A.; Aldossary, S.J.; AlHarbi, S.A.; Majed, S.I.A.; Alenizi, A.; Al-Qahtani, M.H.; Lardhi, A.A.; Al-Turki, S.A.; AlSanea, A.S.; et al. Clinical profile, risk factors and outcomes of pediatric COVID-19: A retrospective cohort multicentre study in Saudi Arabia. BMJ Open 2022, 12, e053722. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Yu, J.; Wang, H.; Zhang, X.; Zhang, S.; Li, Q.; Zhang, Z. Clinical characteristics of COVID-19 in children compared with adults in Shandong Province, China. Infection 2020, 48, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Songa, W.; Lib, J.; Zoua, N.; Guana, W.; Pana, J.; Xua, W. Clinical features of pediatric patients with coronavirus disease (COVID-19). J. Clin. Virol. 2020, 127, 104377. Available online: www.elsevier.com/locate/jcv (accessed on 29 June 2022). [CrossRef] [PubMed]
- Wang, Z.; Zhou, Q.; Wang, C.; Shi, Q.; Lu, S.; Ma, Y.; Luo, X.; Xun, Y.; Li, W.; Baskota, M.; et al. Clinical characteristics of children with COVID-19: A rapid review and meta-analysis. Ann. Transl. Med. 2020, 8, 620. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 infection in children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef]
- Brewster, R.C.L.; Parsons, C.; Laird-Gion, J.; Hilker, S.; Irwin, M.; Sommerschield, A.; Michaelis, K.A.; Lam, M.; Parsons, A.; Mansbach, J.M. COVID-19-associated croup in children. Pediatrics 2022, 2022, 56492. [Google Scholar] [CrossRef]
- Badal, S.; Bajgain, K.T.; Badal, S.; Thapa, R.; Bajgain, B.B.; Santana, M.J. Prevalence, clinical characteristics, and outcomes of pediatric COVID-19: A systematic review and meta-analysis. J. Clin. Virol. 2021, 135, 104715. [Google Scholar] [CrossRef]
- Zachariah, P.; Johnson, C.L.; Halabi, K.C.; Ahn, D.; Sen, A.I.; Fischer, A.; Banker, S.L.; Giordano, M.; Manice, C.S.; Diamond, R.; et al. Epidemiology, Clinical Features, and Disease Severity in Patients With Coronavirus Disease 2019 (COVID-19) in a Children’s Hospital in New York City, New York. JAMA Pediatr. 2020, 174, e202430. [Google Scholar] [CrossRef]
- Christophers, B.; Gallo Marin, B.; Oliva, R.; Powell, W.T.; Savage, T.J.; Michelow, I.C. Trends in clinical presentation of children with COVID-19: A systematic review of individual participant data. Pediatr. Res. 2022, 91, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Parri, N.; Lenge, M.; Buonsenso, D. Children with COVID-19 in pediatric emergency departments in Italy. N. Engl. J. Med. 2020, 383, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Murata, Y.; Tomari, K.; Matsuoka, T. Children with croup and SARS-CoV-2 infection during the large outbreak of Omicron. Pediatr. Infect. Dis. J. 2022, 41, e249. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 27, 2251–2261. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| group classification BY STAGE | Characteristics |
|---|---|
| Asymptomatic cases | All the following requirements need to be met: chest X-ray (CXR) negative, Absence of symptoms/signs no additional instances meet the criteria, for other groups |
| Mild cases | Any of the following: symptoms of upper respiratory tract infection or absence of pneumonic focus on CXR. not fitting into another group |
| Moderate cases | All the following: Cough, signs of severe respiratory distress, and Oxygen < 92% Presence of pneumonia at CXR Absence of criteria for critical group classification Signs of severe respiratory distress/need for any respiratory support |
| Critical cases | Any of the following: Hospitalisation in ICU/patient intubated/multiorgan failure shock, encephalopathy, renal, cardiac or coagulation dysfunction. |
| Characteristics | First Group | Second Group | p-Value |
|---|---|---|---|
| n (%) | n (%) | ||
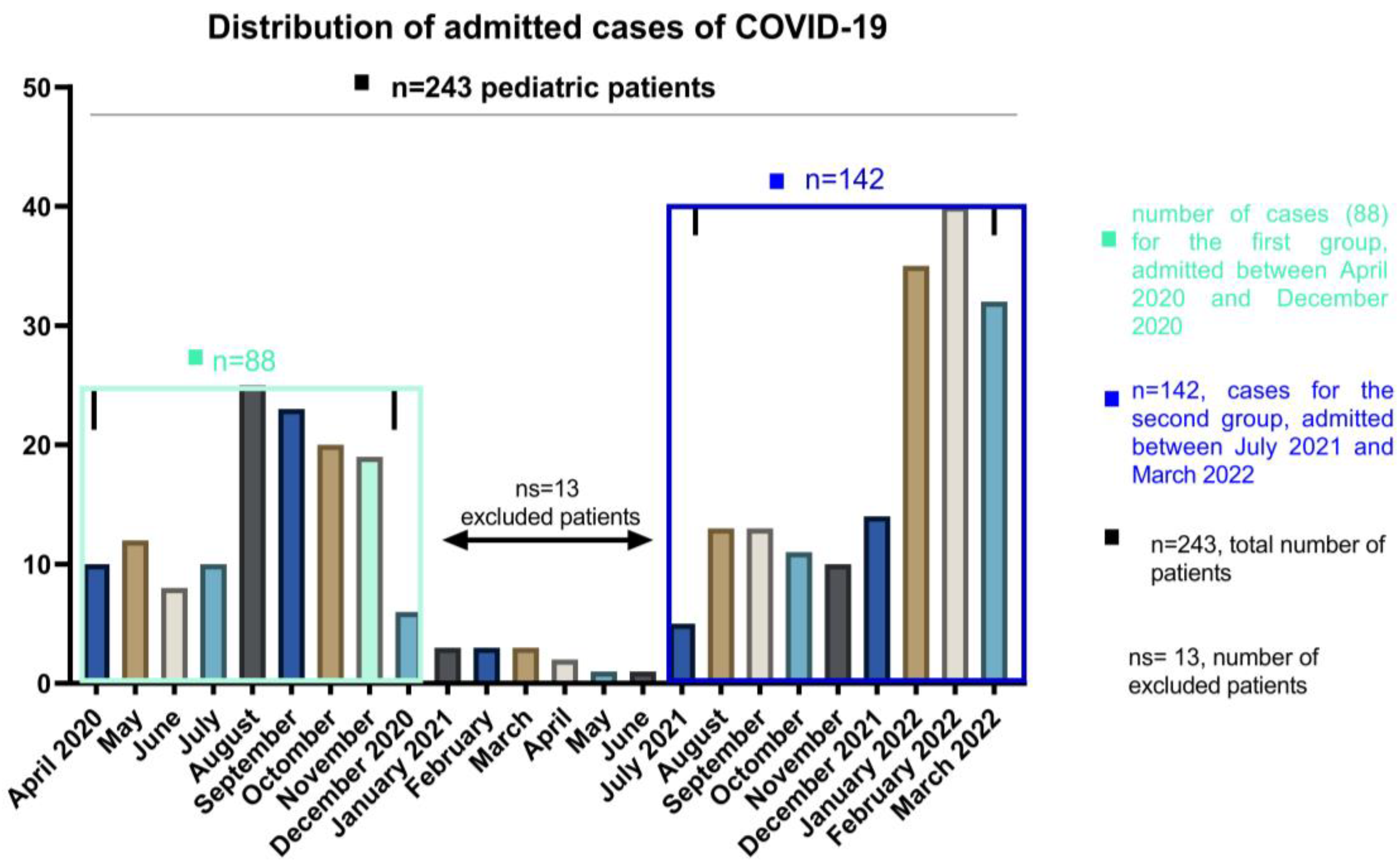
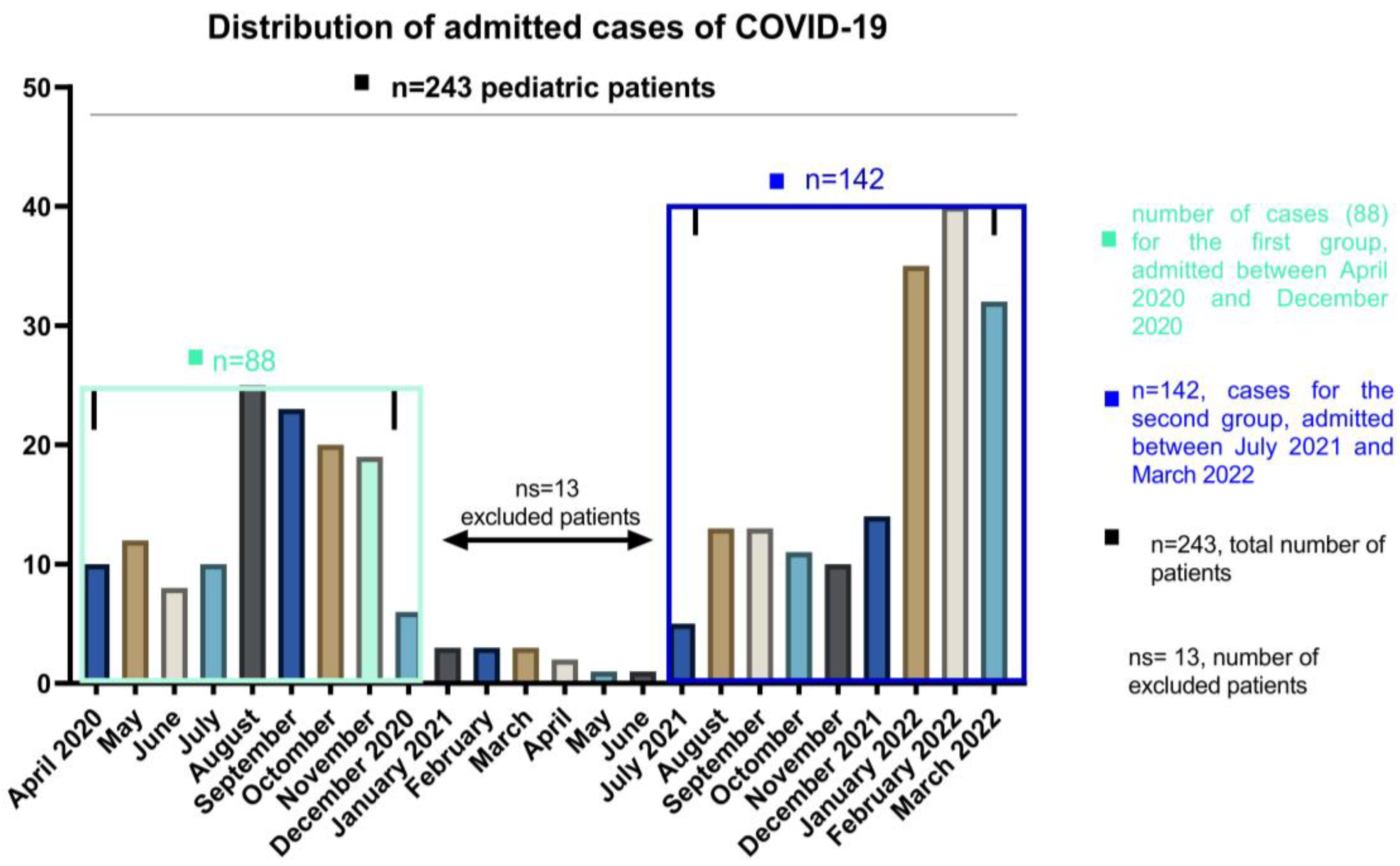
| Pediatric patients | 88 (38.26) | 142 (61.74) | |
| Male gender (%) | 49 (55) | 76 (53.5) | 0.05 |
| Age-years | n (%) | n (%) | |
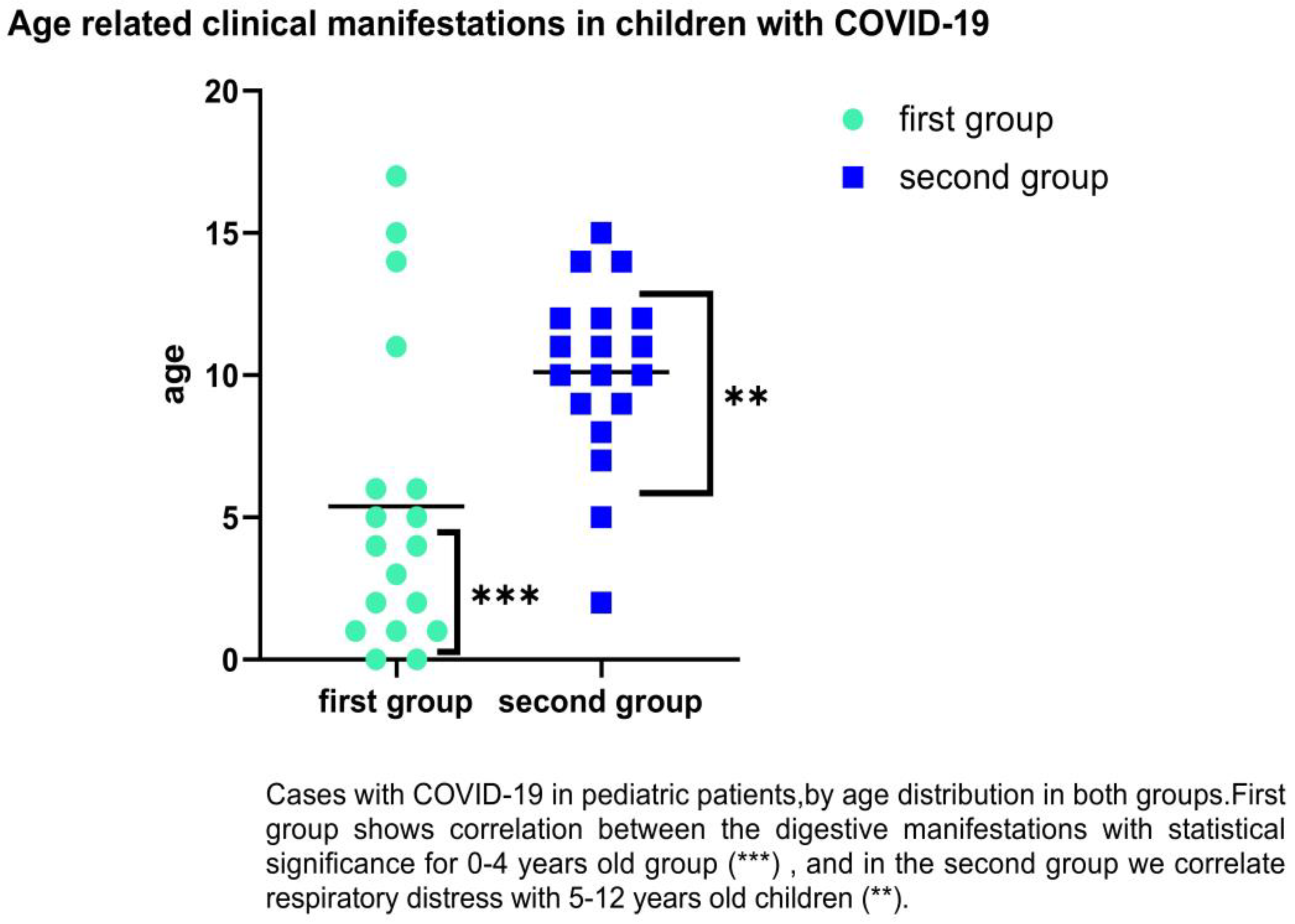
| 0–4 | 34 (38.64) | 38(26.76) | 0.001 |
| 5–12 | 34 (38.64) | 74 (52.11) | 0.02 |
| 13–18 | 20 (22.72) | 30 (21.13) | 0.65 |
| Distress | n (%) | n (%) | |
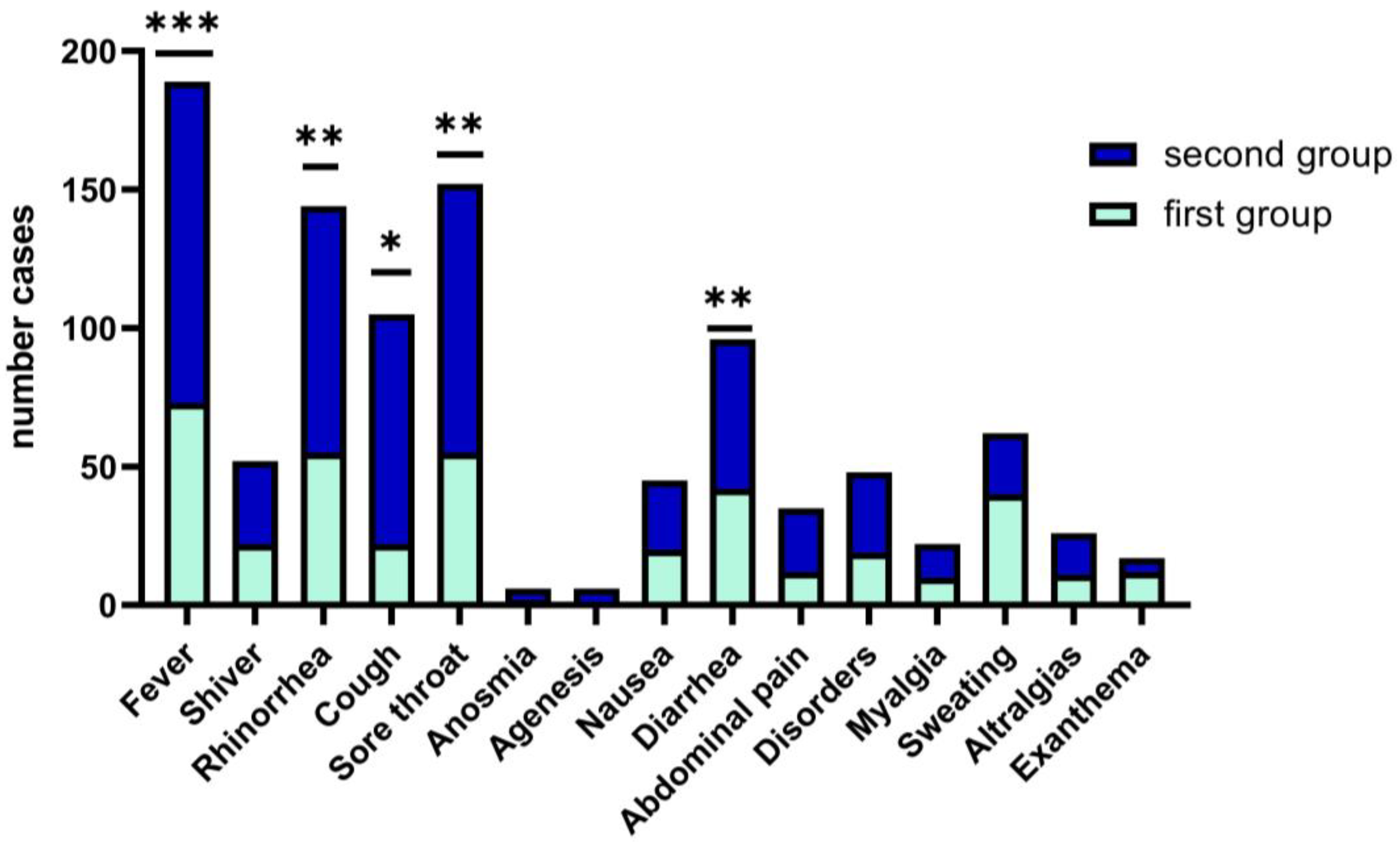
| Fever Age range | 73 (83) | 116 (81.9) | 0.001 |
| 0–1 | 23 (31.5) | 10 (8.62) | 0.001 |
| 0–4 | 20 (27.4) | 13 (11.2) | |
| 5–12 | 18 (24.7) | 68 (58.6) | 0.001 |
| 13–18 | 12 (16.4) | 25 (21.6) | |
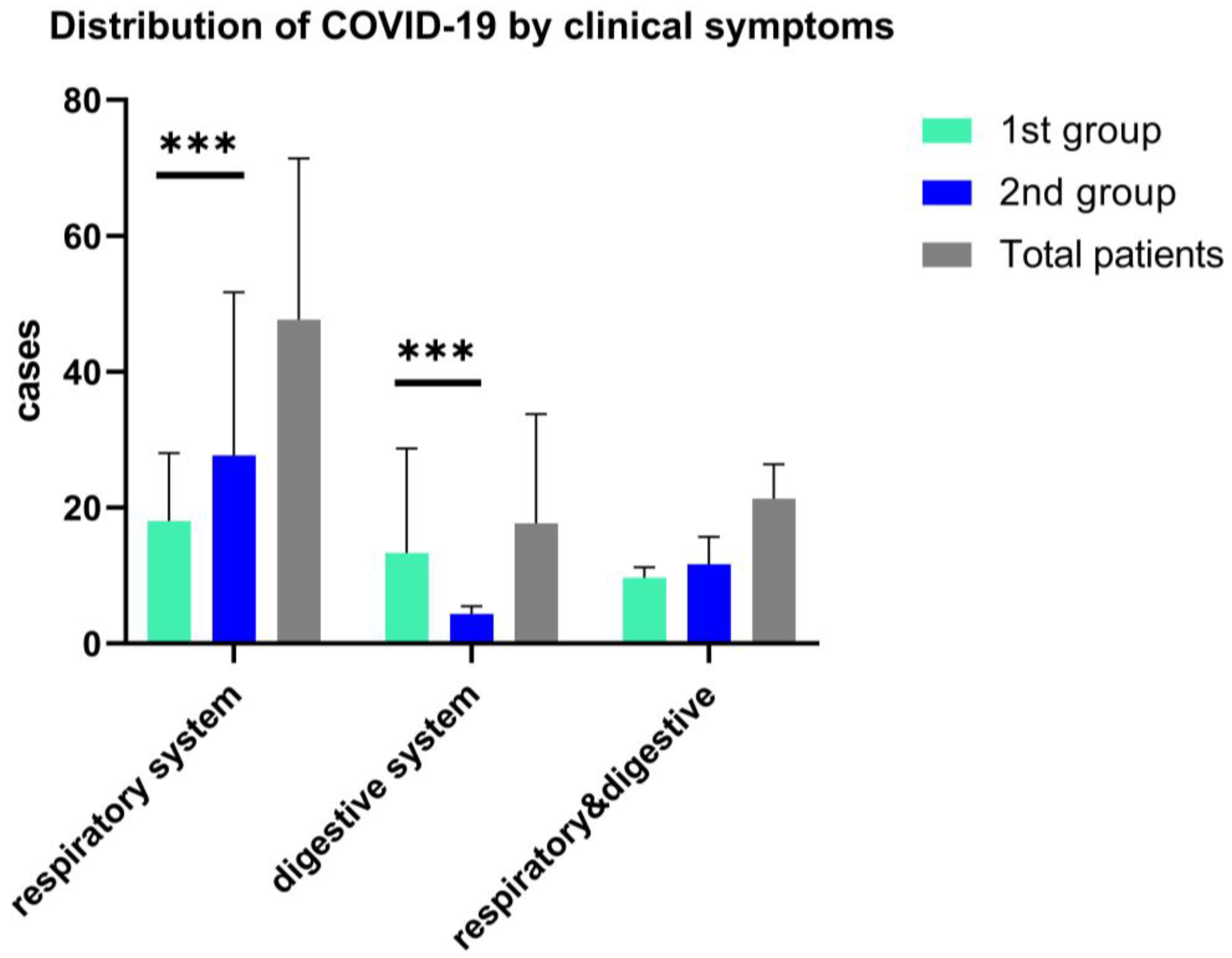
| Shortness of breath/respiratory distress | 55 (62) | 89 (62.68) | 0.02 |
| 0–4 | 18 (32.7) | 17 (19.1) | |
| 5–12 | 12 (35.29) | 62 (83.78) | 0.04 |
| 13–18 | 25 (45.45) | 10 (11.24) | |
| Sore throat Age range | 55 (62%) | 97 (68%) | 0.05 |
| 0–4 | 10 (18.18) | 12 (12.37) | |
| 5–12 | 13(23.64) | 43 (44.3) | 0.05 |
| 13–18 | 32(58.2) | 42 (43.4) | 0.05 |
| Diarrhoea Age range | 42 (47.73) | 54 (38) | 0.0001 |
| 0–1 | 18 (42.86) | 12 (22.2) | 0.0001 |
| 1–4 | 10 (23.8) | 15 (14.8) | 0.04 |
| 5–12 | 9 (21.43) | 14 (25.93) | |
| 13–18 | 5 (11.9) | 13 (24.1) | |
| Days median, [IQR] | Days median, [IQR] | ||
| Hospitalization Age range | 4 [2–5] | 5 [3–7] | 0.04 |
| 0–4 | 5 [3–5] | 5 [4–7] | 0.01 |
| 5–12 | 4 [3,4] | 5 [3–7] | 0.3 |
| 13–18 | 3 [2–4] | 3 [2–4] | |
| Fully vaccinated, years age | n (%) | n (%) | |
| 5–12 | 9 (10.23) | 14 (9.85) | 0.65 |
| 13–18 | 12 (13.63) | 21 (14.79) | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jugulete, G.; Pacurar, D.; Pavelescu, M.L.; Safta, M.; Gheorghe, E.; Borcoș, B.; Pavelescu, C.; Oros, M.; Merișescu, M. Clinical and Evolutionary Features of SARS-CoV-2 Infection (COVID-19) in Children, a Romanian Perspective. Children 2022, 9, 1282. https://doi.org/10.3390/children9091282
Jugulete G, Pacurar D, Pavelescu ML, Safta M, Gheorghe E, Borcoș B, Pavelescu C, Oros M, Merișescu M. Clinical and Evolutionary Features of SARS-CoV-2 Infection (COVID-19) in Children, a Romanian Perspective. Children. 2022; 9(9):1282. https://doi.org/10.3390/children9091282
Chicago/Turabian StyleJugulete, Gheorghiță, Daniela Pacurar, Mirela Luminița Pavelescu, Mihaela Safta, Elena Gheorghe, Bianca Borcoș, Carmen Pavelescu, Mihaela Oros, and Mădălina Merișescu. 2022. "Clinical and Evolutionary Features of SARS-CoV-2 Infection (COVID-19) in Children, a Romanian Perspective" Children 9, no. 9: 1282. https://doi.org/10.3390/children9091282
APA StyleJugulete, G., Pacurar, D., Pavelescu, M. L., Safta, M., Gheorghe, E., Borcoș, B., Pavelescu, C., Oros, M., & Merișescu, M. (2022). Clinical and Evolutionary Features of SARS-CoV-2 Infection (COVID-19) in Children, a Romanian Perspective. Children, 9(9), 1282. https://doi.org/10.3390/children9091282