
Second and Third Generational Advances in Therapies of the Immune-Mediated Kidney Diseases in Children and Adolescents



Abstract
1. Introduction
2. Therapeutic Drug Monitoring (TDM) and Immunomonitoring in Kidney Diseases
3. Nephrotic Syndrome—An Alternative Management beyond the Classic Protocols
4. Cyclosporine A as a Podocyte Cytoskeleton Stabilizer
5. Is Targeting of a CD80 Molecule-Clinically Relevant?
6. The Role of Angiopoietin-like-4 (Angptl4) in Minimal Change Nephrotic Syndrome and a Hypothetic Target-Treatment
7. Complement System Blocking Agents in Glomerular Diseases (with Defect of Complement)
8. Biologic Drugs in Pediatric Systemic Vasculitis
9. Biologic Drugs in Systemic Lupus Erythematosus with Renal Involvement
10. Summary
- Upregulation of the innate and/or adaptive immune system leads to the development of a variety of immune-mediated kidney diseases in children.
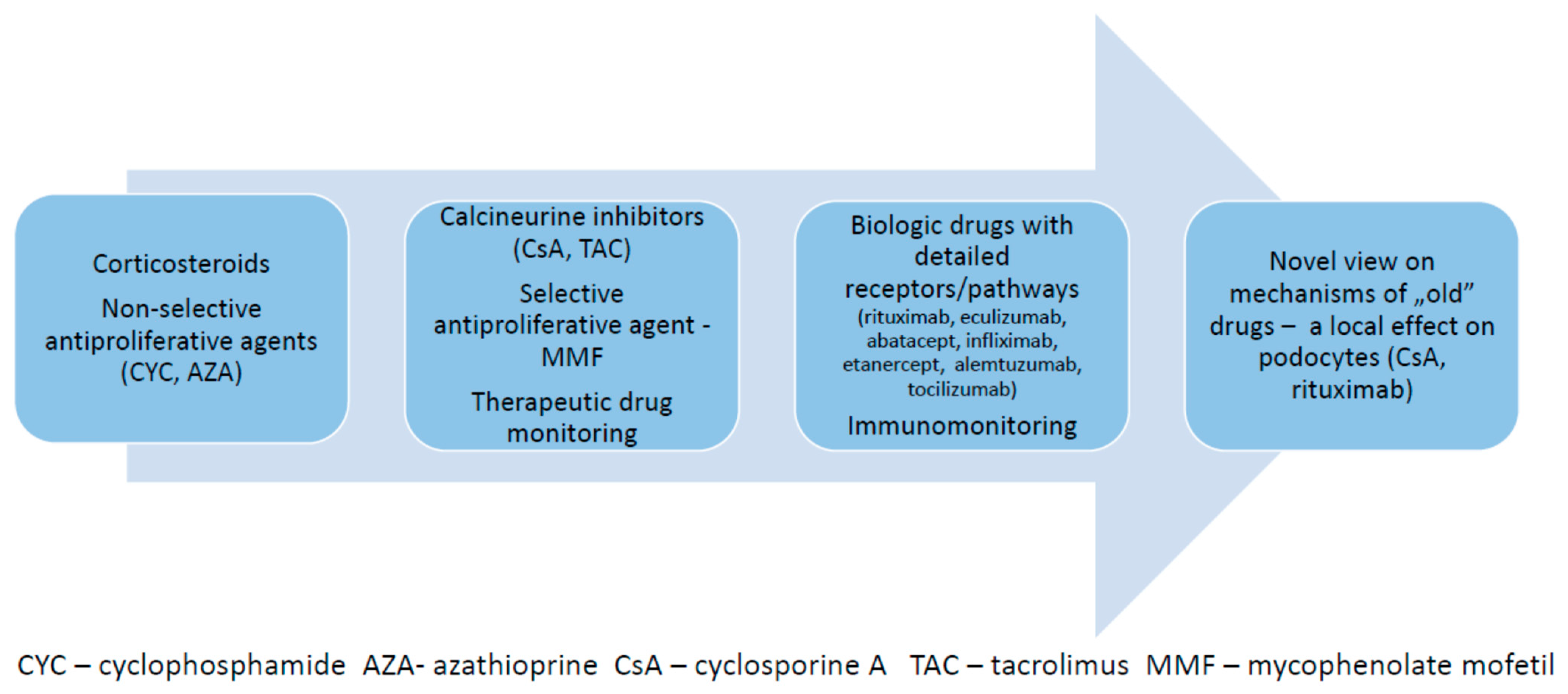
- There is an ongoing progress in pharmacotherapy of immune kidney diseases, based on scientific knowledge, which defines detailed, variable underlying disease-related mechanisms.
- The adaptive immune system is a target of steroids, antiproliferative drugs, calcineurin inhibitors and several receptor-specific biologic agents.
- The innate immune system is a target of specific monoclonal antibodies.
- Surveillance of the current therapies is based on therapeutic drug monitoring and/or immunomonitoring.
- Apart from the effect on the immune system, specific drugs (calcineurin inhibitors, rituximab, abatacept) also exert a local effect on the microstructure of the podocyte cytoskeleton, which may be clinically relevant in selected cases.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell. Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, N.; Nakanishi, K.; Sako, M.; Oba, M.S.; Mori, R.; Ota, E.; Ishikura, K.; Hataya, H.; Honda, M.; Ito, S.; et al. A multicenter randomized trial indicates initial prednisolone treatment for childhood nephrotic syndrome for two months is not inferior to six-month treatment. Kidney Int. 2015, 87, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Lombel, R.M.; Gipson, D.S.; Hodson, E.M. Treatment of steroid-sensitive nephrotic syndrome: New guidelines from KDIGO. Pediatric Nephrol. 2012, 28, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Haun, M.W.; Estel, S.; Rucker, G.; Friederich, H.C.; Villalobos, M.; Thomas, M.; Hartmann, M. Early palliative care for adults with advanced cancer. Cochrane Database Syst. Rev. 2017, 6, CD011129. [Google Scholar] [CrossRef]
- Yoshikawa, N.; Honda, M.; Iijima, K.; Awazu, M.; Hattori, S.; Nakanishi, K.; Ito, H. Steroid Treatment for Severe Childhood IgA Nephropathy: A Randomized, Controlled Trial. Clin. J. Am. Soc. Nephrol. 2006, 1, 511–517. [Google Scholar] [CrossRef]
- Moore, M.J. Clinical Pharmacokinetics of Cyclophosphamide. Clin. Pharmacokinet. 1991, 20, 194–208. [Google Scholar] [CrossRef]
- Tejani, A.; Phadke, K.; Nicastri, A.; Adamson, O.; Chen, C.; Trachtman, H.; Tejani, C. Efficacy of Cyclophosphamide in Steroid-Sensitive Childhood Nephrotic Syndrome with Different Morphological Lesions. Nephron Exp. Nephrol. 1985, 41, 170–173. [Google Scholar] [CrossRef]
- Zagury, A.; de Oliveira, A.L.; de Moraes, C.A.P.; Montalvão, J.A.D.A.; Novaes, R.H.L.L.; de Sá, V.M.; Carvalho, D.D.B.M.D.; Matuck, T. Long-term follow-up after cyclophosphamide therapy in steroid-dependent nephrotic syndrome. Pediatric Nephrol. 2011, 26, 915–920. [Google Scholar] [CrossRef]
- Kamei, K.; Nakanishi, K.; Ito, S.; Saito, M.; Sako, M.; Ishikura, K.; Hataya, H.; Honda, M.; Iijima, K.; Yoshikawa, N.; et al. Long-Term Results of a Randomized Controlled Trial in Childhood IgA Nephropathy. Clin. J. Am. Soc. Nephrol. 2011, 6, 1301–1307. [Google Scholar] [CrossRef]
- Mircheva, J.; Legendre, C.; Soria-Royer, C.; Thervet, E.; Beaune, P.; Kreis, H. Monitoring of azathioprine-induced immunosuppression with thiopurine methyltransferase activity in kidney transplant recipients. Transplantation 1995, 60, 639–642. [Google Scholar] [CrossRef]
- Plank, C.; Nephrologie, F.A.F.P.; Kalb, V.; Hinkes, B.; Hildebrandt, F.; Gefeller, O.; Rascher, W. Cyclosporin A is superior to cyclophosphamide in children with steroid-resistant nephrotic syndrome—A randomized controlled multicentre trial by the Arbeitsgemeinschaft für Pädiatrische Nephrologie. Pediatric Nephrol. 2008, 23, 1483–1493. [Google Scholar] [CrossRef] [PubMed]
- Kemper, M.J.; Kuwertz-Broeking, E.; Bulla, M.; Mueller-Wiefel, D.E.; Neuhaus, T.J. Recurrence of severe steroid dependency in cyclosporin A-treated childhood idiopathic nephrotic syndrome. Nephrol. Dial. Transplant. 2004, 19, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, S.; Bagga, A.; Hari, P.; Sharma, S.; Kalaivani, M.; Dinda, A. Efficacy and Safety of Tacrolimus Versus Cyclosporine in Children with Steroid-Resistant Nephrotic Syndrome: A Randomized Controlled Trial. Am. J. Kidney Dis. 2009, 53, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Jahan, A.; Prabha, R.; Chaturvedi, S.; Mathew, B.; Fleming, D.; Agarwal, I. Clinical efficacy and pharmacokinetics of tacrolimus in children with steroid-resistant nephrotic syndrome. Pediatric Nephrol. 2015, 30, 1961–1967. [Google Scholar] [CrossRef]
- Yang, E.M.; Lee, S.T.; Choi, H.J.; Cho, H.Y.; Lee, J.H.; Kang, H.G.; Park, Y.S.; Cheong, H.I.; Ha, I.-S. Tacrolimus for children with refractory nephrotic syndrome: A one-year prospective, multicenter, and open-label study of Tacrobell®, a generic formula. World J. Pediatric 2015, 12, 60–65. [Google Scholar] [CrossRef]
- Dorresteijn, E.M.; Holthe, J.E.K.-V.; Levtchenko, E.N.; Nauta, J.; Hop, W.C.J.; van der Heijden, A.J. Mycophenolate mofetil versus cyclosporine for remission maintenance in nephrotic syndrome. Pediatric Nephrol. 2008, 23, 2013–2020. [Google Scholar] [CrossRef]
- Gellermann, J.; Weber, L.; Pape, L.; Tönshoff, B.; Hoyer, P.; Querfeld, U. Mycophenolate Mofetil versus Cyclosporin A in Children with Frequently Relapsing Nephrotic Syndrome. J. Am. Soc. Nephrol. 2013, 24, 1689–1697. [Google Scholar] [CrossRef]
- Kemper, M.J.; Valentin, L.; Van Husen, M. Difficult-to-treat idiopathic nephrotic syndrome: Established drugs, open questions and future options. Pediatric Nephrol. 2017, 33, 1641–1649. [Google Scholar] [CrossRef]
- Purohit, S.; Piani, F.; Ordoñez, F.A.; de Lucas-Collantes, C.; Bauer, C.; Cara-Fuentes, G. Molecular Mechanisms of Proteinuria in Minimal Change Disease. Front. Med. 2021, 8, 761600. [Google Scholar] [CrossRef]
- Iijima, K.; Sako, M.; Kamei, K.; Nozu, K. Rituximab in steroid-sensitive nephrotic syndrome: Lessons from clinical trials. Pediatric Nephrol. 2017, 33, 1449–1455. [Google Scholar] [CrossRef]
- Sinha, R.; Agrawal, N.; Xue, Y.; Chanchlani, R.; Pradhan, S.; Raina, R.; Marks, S.D. Use of rituximab in paediatric nephrology. Arch. Dis. Child. 2021, 106, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Salvadori, M.; Tsalouchos, A. How immunosuppressive drugs may directly target podocytes in glomerular diseases. Pediatric Nephrol. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Fornoni, A.; Sageshima, J.; Wei, C.; Merscher-Gomez, S.; Aguillon-Prada, R.; Jauregui, A.N.; Li, J.; Mattiazzi, A.; Ciancio, G.; Chen, L.; et al. Rituximab Targets Podocytes in Recurrent Focal Segmental Glomerulosclerosis. Sci. Transl. Med. 2011, 3, 85ra46. [Google Scholar] [CrossRef]
- Weiner, G.J. Rituximab: Mechanism of Action. Semin. Hematol. 2010, 47, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Colucci, M.; Carsetti, R.; Serafinelli, J.; Rocca, S.; Massella, L.; Gargiulo, A.; Russo, A.L.; Capponi, C.; Cotugno, N.; Porzio, O.; et al. Prolonged Impairment of Immunological Memory After Anti-CD20 Treatment in Pediatric Idiopathic Nephrotic Syndrome. Front. Immunol. 2019, 10, 1653. [Google Scholar] [CrossRef] [PubMed]
- Grenda, R.; Jarmużek, W.; Rubik, J.; Piątosa, B.; Prokurat, S. Rituximab is not a “magic drug” in post-transplant recurrence of nephrotic syndrome. Eur. J. Pediatric 2016, 175, 1133–1137. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hansrivijit, P.; Puthenpura, M.M.; Ghahramani, N. Efficacy of abatacept treatment for focal segmental glomerulosclerosis and minimal change disease: A systematic review of case reports, case series, and observational studies. Clin. Nephrol. 2020, 94, 117–126. [Google Scholar] [CrossRef]
- Bomback, A.S.; Appel, G.B.; Gipson, D.S.; Hladunewich, M.A.; Lafayette, R.; Nester, C.M.; Parikh, S.V.; Smith, R.J.; Trachtman, H.; Heeger, P.S.; et al. Improving Clinical Trials for Anticomplement Therapies in Complement-Mediated Glomerulopathies: Report of a Scientific Workshop Sponsored by the National Kidney Foundation. Am. J. Kidney Dis. 2021, 71, 570–581. [Google Scholar] [CrossRef]
- Muff-Luett, M.; Sanderson, K.R.; Engen, R.M.; Zahr, R.S.; Wenderfer, S.E.; Tran, C.L.; Sharma, S.; Cai, Y.; Ingraham, S.; Winnicki, E.; et al. Eculizumab exposure in children and young adults: Indications, practice patterns, and outcomes—a Pediatric Nephrology Research Consortium study. Pediatric Nephrol. 2021, 36, 2349–2360. [Google Scholar] [CrossRef]
- Oosterveld, M.J.; Garrelfs, M.R.; Hoppe, B.; Florquin, S.; Roelofs, J.J.; Heuvel, L.V.D.; Amann, K.; Davin, J.-C.; Bouts, A.H.; Schriemer, P.J.; et al. Eculizumab in Pediatric Dense Deposit Disease. Clin. J. Am. Soc. Nephrol. 2015, 10, 1773–1782. [Google Scholar] [CrossRef]
- Holle, J.; Berenberg-Goßler, L.; Wu, K.; Beringer, O.; Kropp, F.; Müller, D.; Thumfart, J. Outcome of membranoproliferative glomerulonephritis and C3-glomerulopathy in children and adolescents. Pediatric Nephrol. 2018, 33, 2289–2298. [Google Scholar] [CrossRef] [PubMed]
- Le Quintrec, M.; Lapeyraque, A.-L.; Lionet, A.; Sellier-Leclerc, A.-L.; Delmas, Y.; Baudouin, V.; Daugas, E.; Decramer, S.; Tricot, L.; Cailliez, M.; et al. Patterns of Clinical Response to Eculizumab in Patients with C3 Glomerulopathy. Am. J. Kidney Dis. 2018, 72, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Brogan, P.; Yeung, R.S.M.; Cleary, G.; Rangaraj, S.; Kasapcopur, O.; Hersh, A.O.; Li, S.; Paripovic, D.; Schikler, K.; Zeft, A.; et al. Phase IIa Global Study Evaluating Rituximab for the Treatment of Pediatric Patients with Granulomatosis with Polyangiitis or Microscopic Polyangiitis. Arthritis Rheumatol. 2021, 74, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Null, N. Etanercept plus Standard Therapy for Wegener’s Granulomatosis. N. Engl. J. Med. 2005, 352, 351–361. [Google Scholar] [CrossRef]
- Langford, C.A.; Monach, P.A.; Specks, U.; Seo, P.; Cuthbertson, D.; McAlear, C.A.; Ytterberg, S.R.; Hoffman, G.S.; Krischer, J.P.; Merkel, P.A.; et al. An open-label trial of abatacept (CTLA4-IG) in non-severe relapsing granulomatosis with polyangiitis (Wegener’s). Ann. Rheum. Dis. 2014, 73, 1376–1379. [Google Scholar] [CrossRef]
- Gopaluni, S.; Smith, R.; Goymer, D.; Cahill, H.; Broadhurst, E.; Wallin, E.; McClure, M.; Chaudhry, A.; Jayne, D. Alemtuzumab for refractory primary systemic vasculitis—A randomised controlled dose ranging clinical trial of efficacy and safety (ALEVIATE). Arthritis Res. Ther. 2022, 24, 81. [Google Scholar] [CrossRef]
- Merrill, J.T.; Shanahan, W.R.; Scheinberg, M.; Kalunian, K.C.; Wofsy, D.; Martin, R.S. Phase III trial results with blisibimod, a selective inhibitor of B-cell activating factor, in subjects with systemic lupus erythematosus (SLE): Results from a randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2018, 77, 883–889. [Google Scholar] [CrossRef]
- Brunner, H.I.; Abud-Mendoza, C.; Mori, M.; Pilkington, C.A.; Syed, R.; Takei, S.; Viola, D.O.; Furie, R.A.; Navarra, S.; Zhang, F.; et al. Efficacy and safety of belimumab in paediatric and adult patients with systemic lupus erythematosus: An across-study comparison. RMD Open 2021, 7, e001747. [Google Scholar] [CrossRef]
- Wallace, D.J.; Isenberg, D.A.; Morand, E.F.; Vazquez–Mateo, C.; Kao, A.H.; Aydemir, A.; Pudota, K.; Ona, V.; Aranow, C.; Merrill, J.T. Safety and clinical activity of atacicept in the long-term extension of the phase 2b ADDRESS II study in systemic lupus erythematosus. Rheumatology 2021, 60, 5379–5389. [Google Scholar] [CrossRef]
- Huang, L.; Wang, J.; Yang, J.; Zhang, H.; Hu, Y.; Miao, J.; Mao, J.; Fang, L. Impact of Sampling Time Variability on Tacrolimus Dosage Regimen in Pediatric Primary Nephrotic Syndrome: Single-Center, Prospective, Observational Study. Front. Pharmacol. 2022, 12, 726667. [Google Scholar] [CrossRef]
- Bergan, S.; Brunet, M.; Hesselink, D.A.; Johnson-Davis, K.L.; Kunicki, P.K.; Lemaitre, F.; Marquet, P.; Molinaro, M.; Noceti, O.; Pattanaik, S.; et al. Personalized Therapy for Mycophenolate: Consensus Report by the International Association of Therapeutic Drug Monitoring and Clinical Toxicology. Ther. Drug Monit. 2021, 43, 150–200. [Google Scholar] [CrossRef] [PubMed]
- Zijp, T.R.; Izzah, Z.; Åberg, C.; Gan, C.T.; Bakker, S.J.L.; Touw, D.J.; van Boven, J.F.M. Clinical Value of Emerging Bioanalytical Methods for Drug Measurements: A Scoping Review of Their Applicability for Medication Adherence and Therapeutic Drug Monitoring. Drugs 2021, 81, 1983–2002. [Google Scholar] [CrossRef] [PubMed]
- Teisseyre, M.; Cremoni, M.; Boyer-Suavet, S.; Crepin, T.; Benzaken, S.; Zorzi, K.; Esnault, V.; Brglez, V.; Seitz-Polski, B. Rituximab Immunomonitoring Predicts Remission in Membranous Nephropathy. Front. Immunol. 2021, 12, 738788. [Google Scholar] [CrossRef] [PubMed]
- Davin, J.-C. The glomerular permeability factors in idiopathic nephrotic syndrome. Pediatric Nephrol. 2015, 31, 207–215. [Google Scholar] [CrossRef]
- Bhatia, D.; Sinha, A.; Hari, P.; Sopory, S.; Saini, S.; Puraswani, M.; Saini, H.; Mitra, D.K.; Bagga, A. Rituximab modulates T- and B-lymphocyte subsets and urinary CD80 excretion in patients with steroid-dependent nephrotic syndrome. Pediatric Res. 2018, 84, 520–526. [Google Scholar] [CrossRef]
- Kemper, M.J.; Lehnhardt, A.; Zawischa, A.; Oh, J. Is rituximab effective in childhood nephrotic syndrome? Yes and no. Pediatric Nephrol. 2013, 29, 1305–1311. [Google Scholar] [CrossRef]
- Faul, C.; Donnelly, M.; Merscher-Gomez, S.; Chang, Y.H.; Franz, S.; Delfgaauw, J.; Chang, J.-M.; Choi, H.Y.; Campbell, K.N.; Kim, K.; et al. The actin cytoskeleton of kidney podocytes is a direct target of the antiproteinuric effect of cyclosporine A. Nat. Med. 2008, 14, 931–938. [Google Scholar] [CrossRef]
- Zhang, B.; Shi, W. Is the Antiproteinuric Effect of Cyclosporine A Independent of Its Immunosuppressive Function in T Cells? Int. J. Nephrol. 2012, 2012, 809456. [Google Scholar] [CrossRef]
- Büscher, A.K.; Beck, B.B.; Melk, A.; Hoefele, J.; Kranz, B.; Bamborschke, D.; Baig, S.; Lange-Sperandio, B.; Jungraithmayr, T.; Weber, L.T.; et al. Rapid Response to Cyclosporin A and Favorable Renal Outcome in Nongenetic Versus Genetic Steroid– Resistant Nephrotic Syndrome. Clin. J. Am. Soc. Nephrol. 2015, 11, 245–253. [Google Scholar] [CrossRef]
- Malakasioti, G.; Iancu, D.; Tullus, K. Calcineurin inhibitors in nephrotic syndrome secondary to podocyte gene mutations: A systematic review. Pediatric Nephrol. 2021, 36, 1353–1364. [Google Scholar] [CrossRef]
- Shimada, M.; Araya, C.; Rivard, C.; Ishimoto, T.; Johnson, R.J.; Garin, E.H. Minimal change disease: A “two-hit” podocyte immune disorder? Pediatric Nephrol. 2011, 26, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Ishimoto, T.; Shimada, M.; Araya, C.E.; Huskey, J.; Garin, E.H.; Johnson, R.J. Minimal Change Disease: A CD80 podocytopathy? Semin. Nephrol. 2011, 31, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, F.K.; Orhan, D.; Inözü, M.; Duzova, A.; Gulhan, B.; Ozaltin, F.; Topaloglu, R. CD 80 expression and infiltrating regulatory T cells in idiopathic nephrotic syndrome of childhood. Pediatric Int. 2019, 61, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Cara-Fuentes, G.; Wasserfall, C.H.; Wang, H.; Johnson, R.J.; Garin, E.H. Minimal change disease: A dysregulation of the podocyte CD80– CTLA-4 axis? Pediatric Nephrol. 2014, 29, 2333–2340. [Google Scholar] [CrossRef][Green Version]
- Garin, E.H.; Mu, W.; Arthur, J.M.; Rivard, C.J.; Araya, C.E.; Shimada, M.; Johnson, R.J. Urinary CD80 is elevated in minimal change disease but not in focal segmental glomerulosclerosis. Kidney Int. 2010, 78, 296–302. [Google Scholar] [CrossRef]
- Ling, C.; Liu, X.; Shen, Y.; Chen, Z.; Fan, J.; Jiang, Y.; Meng, Q. Urinary CD80 levels as a diagnostic biomarker of minimal change disease. Pediatric Nephrol. 2014, 30, 309–316. [Google Scholar] [CrossRef]
- Yu, C.-C.; Fornoni, A.; Weins, A.; Hakroush, S.; Maiguel, D.; Sageshima, J.; Chen, L.; Ciancio, G.; Faridi, M.H.; Behr, D.; et al. Abatacept in B7-1– Positive Proteinuric Kidney Disease. N. Engl. J. Med. 2013, 369, 2416–2423. [Google Scholar] [CrossRef]
- Jayaraman, V.K.; Thomas, M. Abatacept experience in steroid and rituximab-resistant focal segmental glomeruloscle-rosis. BMJ Case Rep. 2016, 2016, bcr2016214396. [Google Scholar] [CrossRef]
- Teh, Y.M.; Lim, S.K.; Jusoh, N.; Osman, K.; Mualif, S.A. CD80 Insights as Therapeutic Target in the Current and Future Treatment Options of Frequent-Relapse Minimal Change Disease. BioMed Res. Int. 2021, 2021, 6671552. [Google Scholar] [CrossRef]
- Clement, L.C.; Avila-Casado, C.; Macé, C.; Soria-Castro, E.; Bakker, W.W.; Kersten, S.; Chugh, S.S. Podocyte-secreted angiopoietin-like-4 mediates proteinuria in glucocorticoid-sensitive nephrotic syndrome. Nat. Med. 2010, 17, 117–122. [Google Scholar] [CrossRef]
- Cara-Fuentes, G.; Segarra, A.; Silva-Sanchez, C.; Wang, H.; Lanaspa, M.A.; Johnson, R.J.; Garin, E.H. Angiopoietin-like-4 and minimal change disease. PLoS ONE 2017, 12, e0176198. [Google Scholar] [CrossRef] [PubMed]
- Macé, C.; Chugh, S.S. Nephrotic Syndrome: Components, Connections, and Angiopoietin-Like 4–Related Therapeutics. J. Am. Soc. Nephrol. 2014, 25, 2393–2398. [Google Scholar] [CrossRef] [PubMed]
- Thurman, J.M.; Nester, C.M. All Things Complement. Clin. J. Am. Soc. Nephrol. 2016, 11, 1856–1866. [Google Scholar] [CrossRef] [PubMed]
- Angeletti, A.; Reyes-Bahamonde, J.; Cravedi, P.; Campbell, K.N. Complement in Non-Antibody-Mediated Kidney Diseases. Front. Med. 2017, 4, 99. [Google Scholar] [CrossRef] [PubMed]
- Koopman, J.J.E.; van Essen, M.F.; Rennke, H.G.; de Vries, A.P.J.; van Kooten, C. Deposition of the Membrane Attack Complex in Healthy and Diseased Human Kidneys. Front. Immunol. 2021, 11, 599974. [Google Scholar] [CrossRef]
- Mastrangelo, A.; Serafinelli, J.; Giani, M.; Montini, G. Clinical and Pathophysiological Insights into Immunological Mediated Glomerular Diseases in Childhood. Front. Pediatric 2020, 8, 205. [Google Scholar] [CrossRef]
- Akamine, K.; Punaro, M. Biologics for childhood systemic vasculitis. Pediatric Nephrol. 2018, 34, 2295–2309. [Google Scholar] [CrossRef]
- Mundel, P.; Greka, A. Developing therapeutic ‘arrows’ with the precision of William Tell. Curr. Opin. Nephrol. Hypertens. 2015, 24, 388–392. [Google Scholar] [CrossRef]


{kind=link}
| Drug | Systemic Target/Mechanism | Local (Kidney) Target/Mechanism | Diseases | Generational Line of Therapy |
|---|---|---|---|---|
| Steroids (including ACTH) | Induce downregulation of pro-inflammatory genes by binding to a specific cytoplasmic glucocorticoid receptor (GR); regulate gene expression by binding to glucocorticoid response elements (GRE) on DNA | Attenuation of podocyte apoptosis Blocking of TRPC6 signal pathway Blocking of CD80 upregulation | Nephrotic syndrome All other types of immune-mediated glomerulonephritis | first |
| Cyclophosphamide | Exerts cytotoxic effect by cross-linking of strands of DNA and RNA, and by inhibition of protein synthesis | none | Nephrotic syndrome Lupus nephritis Vasculitis with renal involvement IgAN | second |
| Azathioprine | Acts by the incorporation into replicating DNA; blocks de novo pathway of purine synthesis | none | IgAN AAV | second |
| Mycophenolate mofetil | Mycophenolic acid (MPA), a drug derivative, acts as a selective, noncompetitive inhibitor of inosine monophosphate dehydrogenase IMPDH); inhibits T- and B-lymphocyte proliferation | Decrease of uPAR expression Modification of ATP depletion (by inhibiting IMPDH) in podocytes | Nephrotic syndrome Lupus nephritis Vasculitis with renal involvement IgAN | second |
| Cyclosporine A | Inhibits the phosphatase activity of calcineurin, which regulates nuclear translocation and subsequent activation of NFAT transcription factors; CsA is a specific inhibitor of T cell activation | Stabilization of actin cytoskeleton by preserving a phosphorylation-dependent synaptopodin-14-3-3-ẞ integrin interaction Decrease of TRPC6 and ANGPTL4 upregulation | Nephrotic syndrome | second |
| Tacrolimus | Inhibits T lymphocyte activation and transcription of cytokine genes, including the gene for interleukin-2 | Decrease of TRPC6 and ANGPTL4 upregulation | Nephrotic syndrome | third (off-label) |
| Drug | Systemic Target/Mechanism | Local (Kidney) Target/Mechanism | Diseases | Generational Line of Therapy |
|---|---|---|---|---|
| rituximab | Binds to CD20 on B cells and mediates B-cell lysis and depletion | stabilizes podocytes cytoskeleton by regulation (preservation) of sphingomyelin phosphodiesterase acid-like 3b (SMLPD-3b), a protein participating in the podocyte cytoskeleton activity | Nephrotic syndrome AAV GPA MPA IgA vasculitis Membranous nephropathy | third (off-label) Clinical trials (adults and adolescents) Case reports |
| eculizumab | Binds to complement protein C5, inhibiting its cleavage to C5a and C5b; this prevents a generation of the terminal complement complex C5b-9 | none | Atypical hemolytic uremic syndrome (aHUS) Lupus nephritis C3 nephropathy MPGN type I DDD | first third (off label) second/third (off-label) |
| abatacept | A fusion molecule including Fc region of IgG1 and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4-Ig) Blocks CTLA-4 present on Tregs | Blocking of B7-1 signalling and restoration of ẞ1 integrin activation | Nephrotic syndrome GPA (Granulomatosis with Polyangiitis) Takayasu arteritis | fourth (off-label) Clinical trials (adults and adolescents) Case reports |
| infliximab etanercept | Anti-TNFα moab Human Fc fusion protein- blocks the TNFα -receptor | none | AAV Takayasu disease PAN | Clinical trials (children) Case reports |
| alemtuzumab | Anti-CD52 depleting moab, lysis of all cells expressing CD52 | none | AAV | Clinical trials (adults) Case reports |
| tocilizumab | Anti-IL6 moab | none | Kawasaki disease | Children (case reports) |
| anakinra | Anti-IL-1 moab | none | Kawasaki disease | Clinical trial (children) |
| blisibimod | Blocks of B-cell activating factor (BAFF) | none | SLE | Clinical trial (adults) |
| belimumab | Anti-BAFF moab | none | SLE | Clinical trials (adults and children) |
| atacicept | A recombinant human fusion protein that binds to BLyS (B lymphocyte stimulator) and APRIL (a proliferation-inducing ligand); inhibits interactions with their specific receptors | none | SLE | Clinical trial (adults) |
| Rule | Clinical Practice |
|---|---|
| There is an association between the dose and drug concentration in the blood/plasma. | The activity of drug-specific metabolic pathways is programmed genetically and also is age-dependent. |
| Pharmacokinetics and pharmacodynamics of the drug depend on function of the specific pathways and organs (routes of drug metabolism and clearance). | There is an association between drug concentration and its clinical efficacy and toxicity. |
| Specific drugs administered simultaneously may interact, and this reaction changes its’ metabolism and pharmacokinetics. | Multidrug management requires more frequent TDM. |
| The pharmacokinetic effect of the biologic drug is expressed as a number of targeted cells. | There is an association between the number of target cells and the clinical course of the disease. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grenda, R.; Obrycki, Ł. Second and Third Generational Advances in Therapies of the Immune-Mediated Kidney Diseases in Children and Adolescents. Children 2022, 9, 536. https://doi.org/10.3390/children9040536
Grenda R, Obrycki Ł. Second and Third Generational Advances in Therapies of the Immune-Mediated Kidney Diseases in Children and Adolescents. Children. 2022; 9(4):536. https://doi.org/10.3390/children9040536
Chicago/Turabian StyleGrenda, Ryszard, and Łukasz Obrycki. 2022. "Second and Third Generational Advances in Therapies of the Immune-Mediated Kidney Diseases in Children and Adolescents" Children 9, no. 4: 536. https://doi.org/10.3390/children9040536
APA StyleGrenda, R., & Obrycki, Ł. (2022). Second and Third Generational Advances in Therapies of the Immune-Mediated Kidney Diseases in Children and Adolescents. Children, 9(4), 536. https://doi.org/10.3390/children9040536