
Surgical Outcome of Children with a Malignant Liver Tumour in The Netherlands: A Retrospective Consecutive Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Diagnosis and Treatment
2.3. Postoperative Complications
- Haemorrhage: defined as perioperative blood loss requiring reoperation or blood transfusion;
- Infection: any infection clinically related to the surgical procedure;
- Biliary complications: biliary tract stricture or bile leak;
- Vascular complications other than haemorrhage: compromised hepatic blood flow after surgery;
- Other complications: any other postoperative complication due to surgery requiring prolonged hospital stay or reintervention not included in any of the previous categories.
2.4. Follow-Up
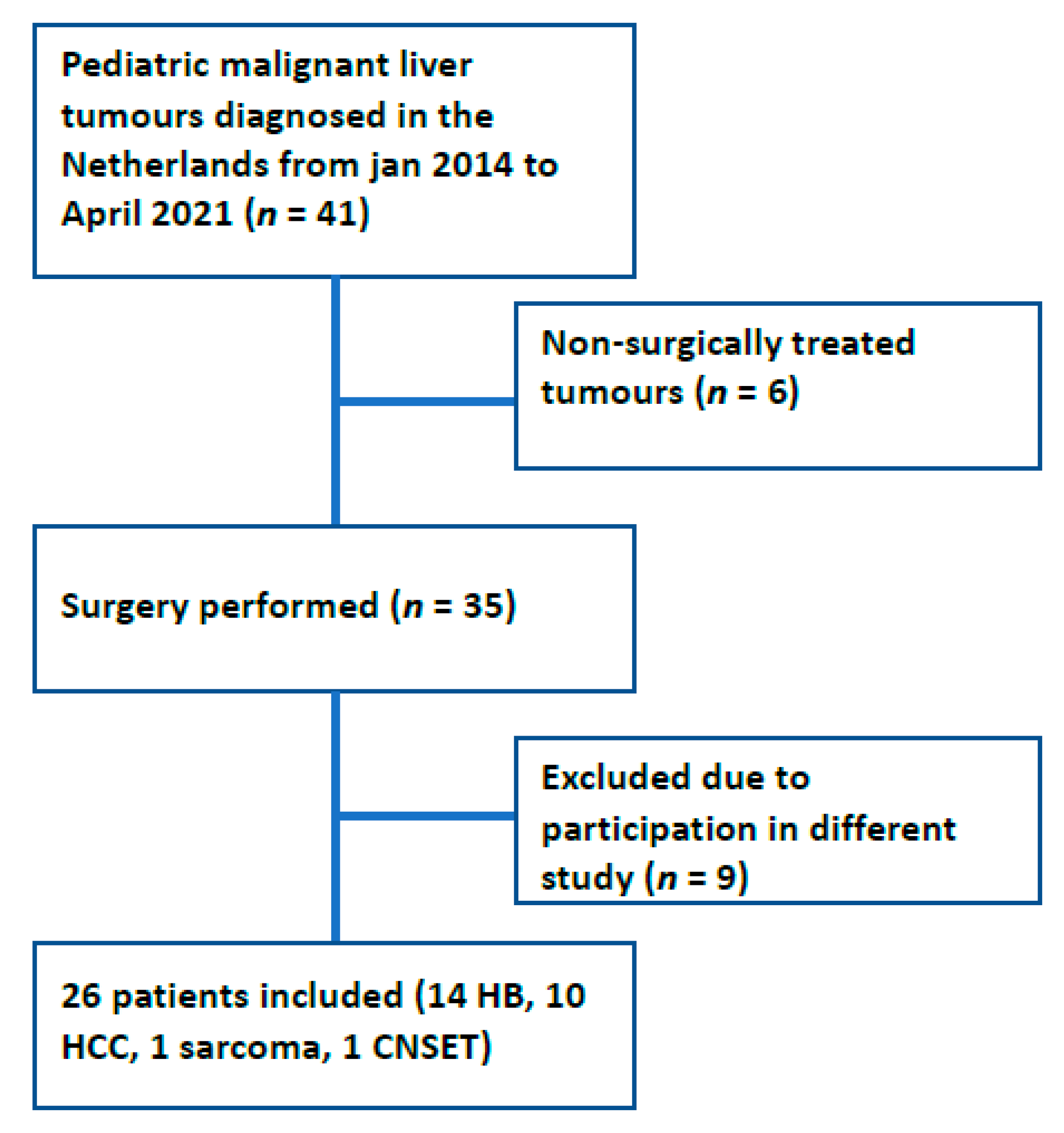
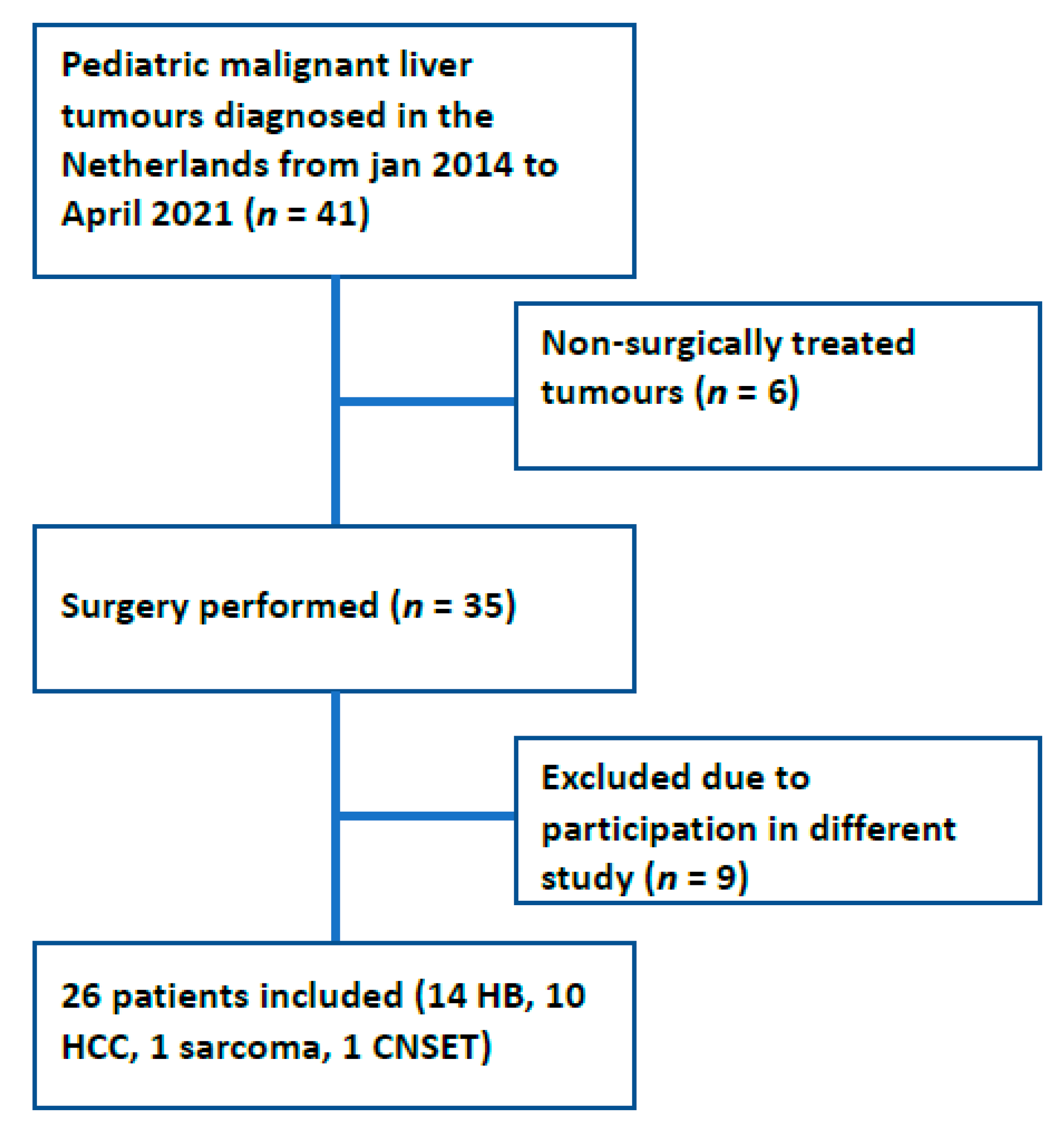
3. Results
3.1. Clinical Features
3.2. Treatment
3.3. Radicality
3.4. Complications
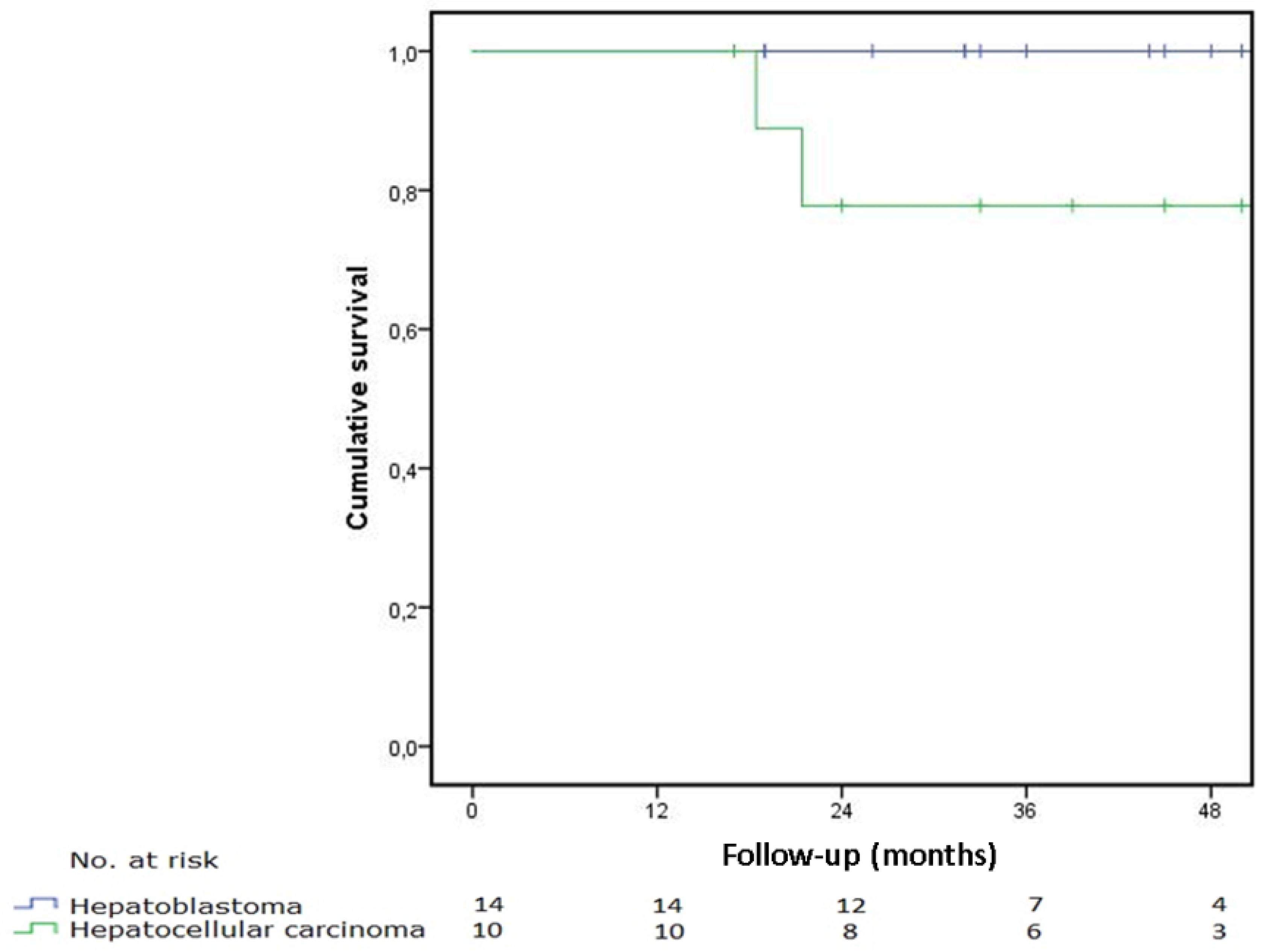
3.5. Survival of Operated Patients
3.6. Comparison to the Historical Group
4. Discussion
4.1. Complications
4.2. Mortality
4.3. Historical Controls
4.4. Patients, Inclusion and Exclusion
4.5. Incidence
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NKR Cijfers—IKNL. Available online: https://iknl.nl/nkr-cijfers (accessed on 1 October 2021).
- StatLine—Bevolking. Kerncijfers. Available online: https://opendata.cbs.nl/statline (accessed on 1 October 2021).
- Finegold, M.J.; Egler, R.A.; Goss, J.A.; Guillerman, R.P.; Karpen, S.J.; Krishnamurthy, R.; O’Mahony, C.A. Liver tumors: Pediatric population. Liver Transpl. 2008, 14, 1545–1556. [Google Scholar] [CrossRef]
- Chavhan, G.B.; Siddiqui, I.; Ingley, K.M.; Gupta, A.A. Rare malignant liver tumors in children. Pediatr. Radiol. 2019, 49, 1404–1421. [Google Scholar] [CrossRef]
- Czauderna, P.; Lopez-Terrada, D.; Hiyama, E.; Häberle, B.; Malogolowkin, M.H.; Meyers, R.L. Hepatoblastoma state of the art: Pathology, genetics, risk stratification, and chemotherapy. Current Opinion in Pediatrics. Curr. Opin. Pediatr. 2014, 26, 19–28. [Google Scholar] [CrossRef]
- Meyers, R.L. Tumors of the liver in children. Surg. Oncol. 2007, 16, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Murawski, M.; Weeda, V.B.; Maibach, R.; Morland, B.; Roebuck, D.J.; Zimmerman, A.; Casanova, M.; Perilongo, G.; Laithier, V.; Kebudi, R.; et al. Hepatocellular Carcinoma in Children: Does Modified Platinum- and Doxorubicin-Based Chemotherapy Increase Tumor Resectability and Change Outcome? Lessons Learned From the SIOPEL 2 and 3 Studies. J. Clin. Oncol. 2016, 34, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.; Verma, S.K. Pediatric hepatocellular carcinoma. World J. Gastroenterol. 2018, 24, 3980–3999. [Google Scholar] [CrossRef]
- Pappo, A.; Maibach, R.; Shafford, E.; Brugieres, L.; Brock, P.; Morland, B.; de Camargo, B.; Zsiros, J.; Roebuck, D.; Zimmermann, A.; et al. Cisplatin versus cisplatin plus doxorubicin for standard-risk hepatoblastoma. N. Engl. J. Med. 2009, 361, 1661–1670. [Google Scholar]
- Zsíros, J.; Maibach, R.; Shafford, E.; Brugieres, L.; Brock, P.; Czauderna, P.; Roebuck, D.; Childs, M.; Zimmermann, A.; Laithier, V.; et al. Successful Treatment of Childhood High-Risk Hepatoblastoma With Dose-Intensive Multiagent Chemotherapy and Surgery: Final Results of the SIOPEL-3HR Study. J. Clin. Oncol. 2010, 28, 2584–2590. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, S.; Karnak, I.; Tanyel, F.C.; Şenocak, M.E.; Kutluk, T.; Büyükpamukçu, M.; Büyükpamukçu, N. Hepatic lobectomies in children: Experience of a center in the light of changing management of malignant liver tumors. Pediatr. Surg. Int. 2006, 22, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Meyers, R.L.; Tiao, G.; de Ville De Goyet, J.; Superina, R.; Aronson, D.C. Hepatoblastoma state of the art: Pre-treatment extent of disease, surgical resection guidelines and the role of liver transplantation. Curr. Opin. Pediatr. 2014, 26, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Trobaugh-Lotrario, A.D.; Meyers, R.L.; Tiao, G.M.; Feusner, J.H. Pediatric liver transplantation for hepatoblastoma. Transl. Gastroenterol. Hepatol. 2016, 1, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyers, R.L.; Otte, J.B. Liver transplantation for unresectable liver tumors in children. In Pediatric Liver Tumors; Springer: Berlin/Heidelberg, Germany, 2011; pp. 134–145. [Google Scholar]
- Nederlandse Richtlijn Protocol Indicatie en Selectie voor Levertransplantatie bij Volwassenen en Kinderen in Nederland. October 2017; Dutch Transplantation Organisation (Nederlandse Transplantatie Vereniging, Protocol indicatie en selectie levertransplantatie|Nederlandse Transplantatie Stichting). Available online: https://www.transplantatiestichting.nl/richtlijn/protocol-indicatie-en-selectie-levertransplantatie (accessed on 1 October 2021).
- Busweiler, L.A.D.; Wijnen, M.H.W.A.; Wilde, J.C.H.; Sieders, E.; Van Scheltinga, S.E.J.T.; Van Heurn, L.W.E.; Ziros, J.; Bakx, R.; Heij, H.A. Surgical treatment of childhood hepatoblastoma in the Netherlands (1990–2013). Pediatr. Surg. Int. 2017, 33, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. Strengthening the reporting of observational studies in epidemiology (StroBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinberg, A.G.; Finegold, M.J. Primary hepatic tumors of childhood. Hum. Pathol. 1983, 14, 512–537. [Google Scholar] [CrossRef]
- Towbin, A.J.; Meyers, R.L.; Woodley, H.; Miyazaki, O.; Weldon, C.B.; Morland, B.; Hiyama, E.; Czauderna, P.; Roebuck, D.J.; Tiao, G.M. 2017 PRETEXT: Radiologic staging system for primary hepatic malignancies of childhood revised for the Paediatric Hepatic International Tumour Trial (PHITT). Pediatr. Radiol. 2018, 48, 536–554. [Google Scholar] [CrossRef]
- Roebuck, D.J.; Aronson, D.; Clapuyt, P.; Czauderna, P.; de Ville de Goyet, J.; Gauthier, F.; MacKinlay, G.; Maibach, R.; McHugh, K.; Olsen, E.; et al. 2005 PRETEXT: A revised staging system for primary malignant liver tumours of childhood developed by the SIOPEL group. Pediatr. Radiol. 2007, 37, 123–132. [Google Scholar] [CrossRef] [Green Version]
- SIOPEL Guidelines for the Treatment of Hepatoblastoma. Available online: http://www.sehop.org/wp-content/uploads/2015/07/Guidelines-for-treatment-of-hepatoblastoma.pdf (accessed on 1 October 2021).
- Wittekind, C.; Compton, C.; Quirke, P.; Nagtegaal, I.; Merkel, S.; Hermanek, P.; Sobin, L.H. A Uniform Residual Tumor (R) Classification Integration of the R Classification and the Circumferential Margin Status. Cancer 2009, 115, 3483–3488. [Google Scholar] [CrossRef]
- Katayama, H.; Kurokawa, Y.; Nakamura, K.; Ito, H.; Kanemitsu, Y.; Masuda, N.; Tsubosa, Y.; Satoh, T.; Yokomizo, A.; Fukuda, H.; et al. Extended Clavien-Dindo classification of surgical complications: Japan Clinical Oncology Group postoperative complications criteria. Surg. Today 2016, 46, 668–685. [Google Scholar] [CrossRef] [Green Version]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The clavien-dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Paediatric Hepatic International Tumour Trial PHITT. 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03017326 (accessed on 1 October 2021).
- Tannuri, A.C.A.; Tannuri, U.; Gibelli, N.E.M.; Romão, R.L.P. Surgical treatment of hepatic tumors in children: Lessons learned from liver transplantation. J. Pediatr. Surg. 2009, 44, 2083–2087. [Google Scholar] [CrossRef] [PubMed]
- Zwintscher, N.P.; Azarow, K.S.; Horton, J.D. Morbidity and mortality associated with liver resections for primary malignancies in children. Pediatr. Surg. Int. 2014, 30, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, Y.; Zhu, H.; Qiu, L.; Guo, C. Prediction of perioperative outcome after hepatic resection for pediatric patients. BMC Gastroenterol. 2019, 19, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czauderna, P.; Haeberle, B.; Hiyama, E.; Rangaswami, A.; Krailo, M.; Maibach, R.; Rinaldi, E.; Feng, Y.; Aronson, D.; Malogolowkin, M.; et al. The Children’s Hepatic tumors International Collaboration (CHIC): Novel global rare tumor database yields new prognostic factors in hepatoblastoma and becomes a research model. Eur. J. Cancer 2016, 52, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Category | Number | (%) |
|---|---|---|
| Sex | ||
| Male | 14 | 54 |
| Female | 12 | 46 |
| Age (months) | ||
| Median | 49 | |
| Interquartile range | 17.5–153 | |
| AFP (ug/L) | ||
| Mean | 180,367 | |
| Median | 2300 | |
| Interquartile range | 15.1–275,000 | |
| PRETEXT | ||
| I | 2 | 8 |
| II | 8 | 31 |
| III | 8 | 31 |
| IV | 3 | 11 |
| Not applicable | 5 | 19 |
| Hepatoblastoma | 14 | 54 |
| Mixed epithelial/mesenchymal | 11 | 79 |
| Epithelial | 3 | 21 |
| Hepatocellular carcinoma | 10 | 38 |
| Sarcoma | 1 | 4 |
| Calcifying Nested Stromal Epithelial Tumour | 1 | 4 |
| All Liver Tumours | HB | HCC | ||||
|---|---|---|---|---|---|---|
| Type of Surgery | Number | (%) | Number | (%) | Number | (%) |
| Partial liver resection | 19 | 73 | 12 | 86 | 6 | 60 |
| Segmentectomy/local excision | 5 | 19 | 1 | 7 | 3 | 30 |
| Hemihepatectomy left | 3 | 12 | 2 | 14 | 1 | 10 |
| Hemihepatectomy right | 4 | 15 | 3 | 21 | 1 | 10 |
| Extended hemihepatectomy left | 3 | 12 | 3 | 21 | 0 | 0 |
| Extended hemihepatectomy right | 4 | 15 | 3 | 21 | 1 | 10 |
| Total hepatectomy with orthotopic liver transplantation | 7 | 27 | 2 | 14 | 4 | 40 |
| Category | Partial Liver Resection n = 19 | OLT n = 7 |
|---|---|---|
| Haemorrhage | 1 (1 b) | 2 (2 a) |
| Clavien–Dindo 3b | 0 | 2 |
| Clavien–Dindo 4b | 1 | 0 |
| Infection | 3 | 1 (1 a) |
| Clavien–Dindo 3a | 1 | 0 |
| Clavien–Dindo 3b | 0 | 1 |
| Clavien–Dindo 4a | 2 | 0 |
| Biliary | 0 | 0 |
| Vascular | 0 | 0 |
| Other | 2 | 9 (3 a) |
| Clavien–Dindo 3a | 0 | 1 |
| Clavien–Dindo 3b | 1 | 6 |
| Clavien–Dindo 4a | 1 | 1 |
| Clavien–Dindo 4b | 0 | 1 |
| All Liver Tumours n = 26 (%) | HB n = 14 (%) | HB Historical Group n = 94 (%) | p Value | |
|---|---|---|---|---|
| Complication percentage | 9 (35) | 4 (29) | 42/73 (54) | 0.0774 |
| Haemorrhage | 3 (12) | 1 (7) | 33/73 (45) | 0.0071 * |
| Biliary | 0 (0) | 0 (0) | 9/73 (13) | 0.344 |
| Vascular | 0 (0) | 0 (0) | 2/73 (3) | 1.0 |
| Infection | 4 (15) | 3 (21) | 6/73 (8) | 0.1548 |
| Other | 7 (27) | 3 (21) | NA | |
| Recurrent disease | 2 HCC, 1 CNSET AWD (12%) | 0 (0) | Total 16/94, liver 3/94, pulmonary 12/94, both 1 (17) | 0.1199 |
| OLT | 7 (27) | 14 (2) | 18/94 (19) | 1 |
| Survival 30 d. | 100 (nr at risk 26) | 100 (nr at risk 14) | 100 | |
| Survival 90 d. | 100 (nr at risk 26) | 100 (nr at risk 14) | NA | |
| Survival 1 jr. | 100 (nr at risk 25) | 100 (nr at risk 14) | NA | |
| Survival 5 jr. | 92 (nr at risk 4) | 100 (nr at risk 2) | 82 (77/94) | 0.1199 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klunder, M.B.; Bruggink, J.L.M.; Huynh, L.D.H.; Bodewes, F.A.J.A.; van der Steeg, A.F.W.; Kraal, K.C.J.M.; van de Ven, C.P.; van Grotel, M.; Zsiros, J.; Wijnen, M.H.W.A.; et al. Surgical Outcome of Children with a Malignant Liver Tumour in The Netherlands: A Retrospective Consecutive Cohort Study. Children 2022, 9, 525. https://doi.org/10.3390/children9040525
Klunder MB, Bruggink JLM, Huynh LDH, Bodewes FAJA, van der Steeg AFW, Kraal KCJM, van de Ven CP, van Grotel M, Zsiros J, Wijnen MHWA, et al. Surgical Outcome of Children with a Malignant Liver Tumour in The Netherlands: A Retrospective Consecutive Cohort Study. Children. 2022; 9(4):525. https://doi.org/10.3390/children9040525
Chicago/Turabian StyleKlunder, Merel B., Janneke L. M. Bruggink, Leon D. H. Huynh, Frank A. J. A. Bodewes, Alida F. W. van der Steeg, Kathelijne C. J. M. Kraal, C. P. (Kees) van de Ven, Martine van Grotel, József Zsiros, Marc H. W. A. Wijnen, and et al. 2022. "Surgical Outcome of Children with a Malignant Liver Tumour in The Netherlands: A Retrospective Consecutive Cohort Study" Children 9, no. 4: 525. https://doi.org/10.3390/children9040525
APA StyleKlunder, M. B., Bruggink, J. L. M., Huynh, L. D. H., Bodewes, F. A. J. A., van der Steeg, A. F. W., Kraal, K. C. J. M., van de Ven, C. P., van Grotel, M., Zsiros, J., Wijnen, M. H. W. A., Molenaar, I. Q., Porte, R. J., de Meijer, V. E., & de Kleine, R. H. (2022). Surgical Outcome of Children with a Malignant Liver Tumour in The Netherlands: A Retrospective Consecutive Cohort Study. Children, 9(4), 525. https://doi.org/10.3390/children9040525