

Diagnostic Clues in Pediatric Nutcracker Syndrome: From Two Clinical Cases to Current Literature Analysis

 ,
,  and
and 
Abstract
1. Introduction
2. Case Reports
2.1. Case 1
2.2. Case 2
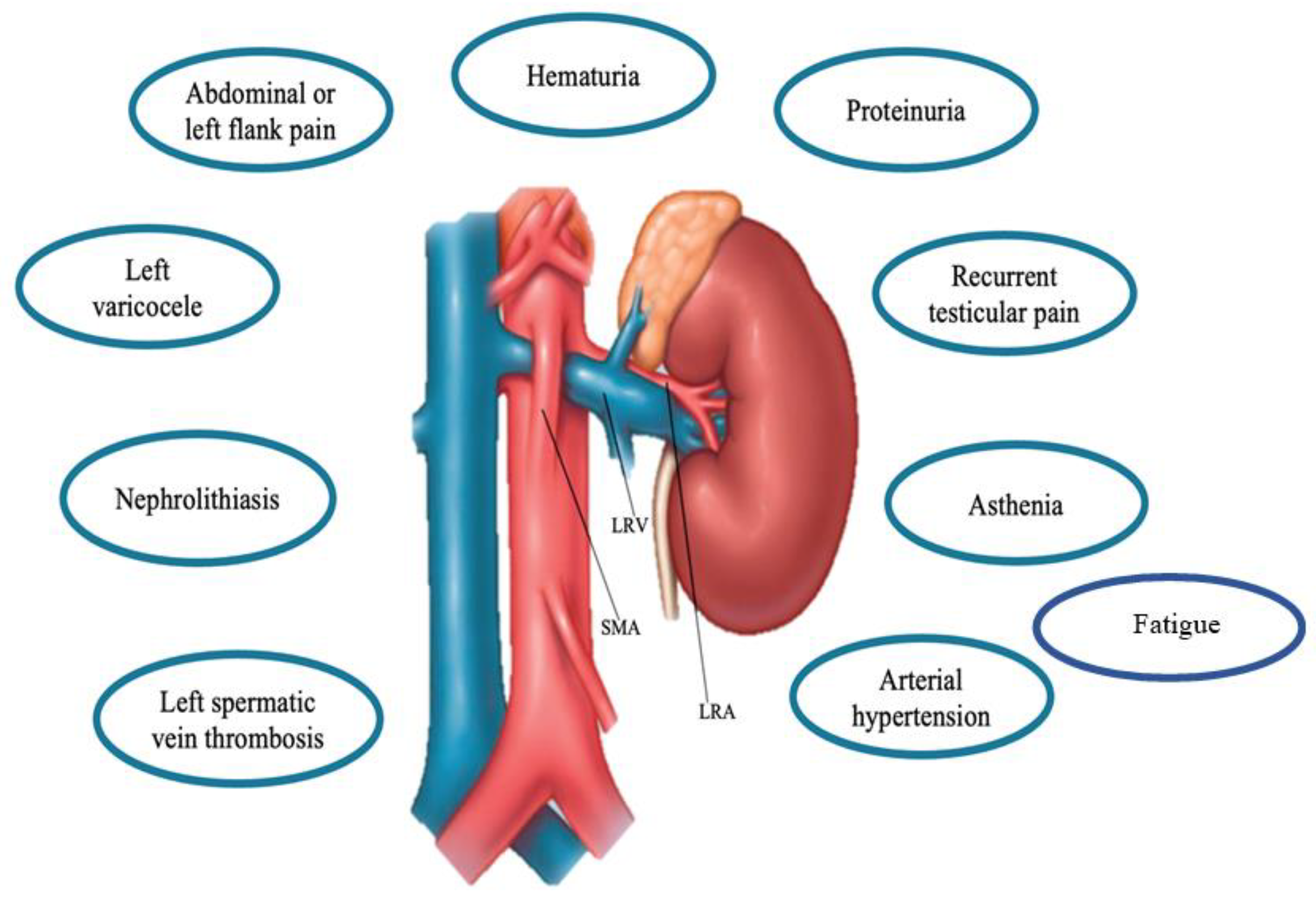
3. Clinical Features of NCS
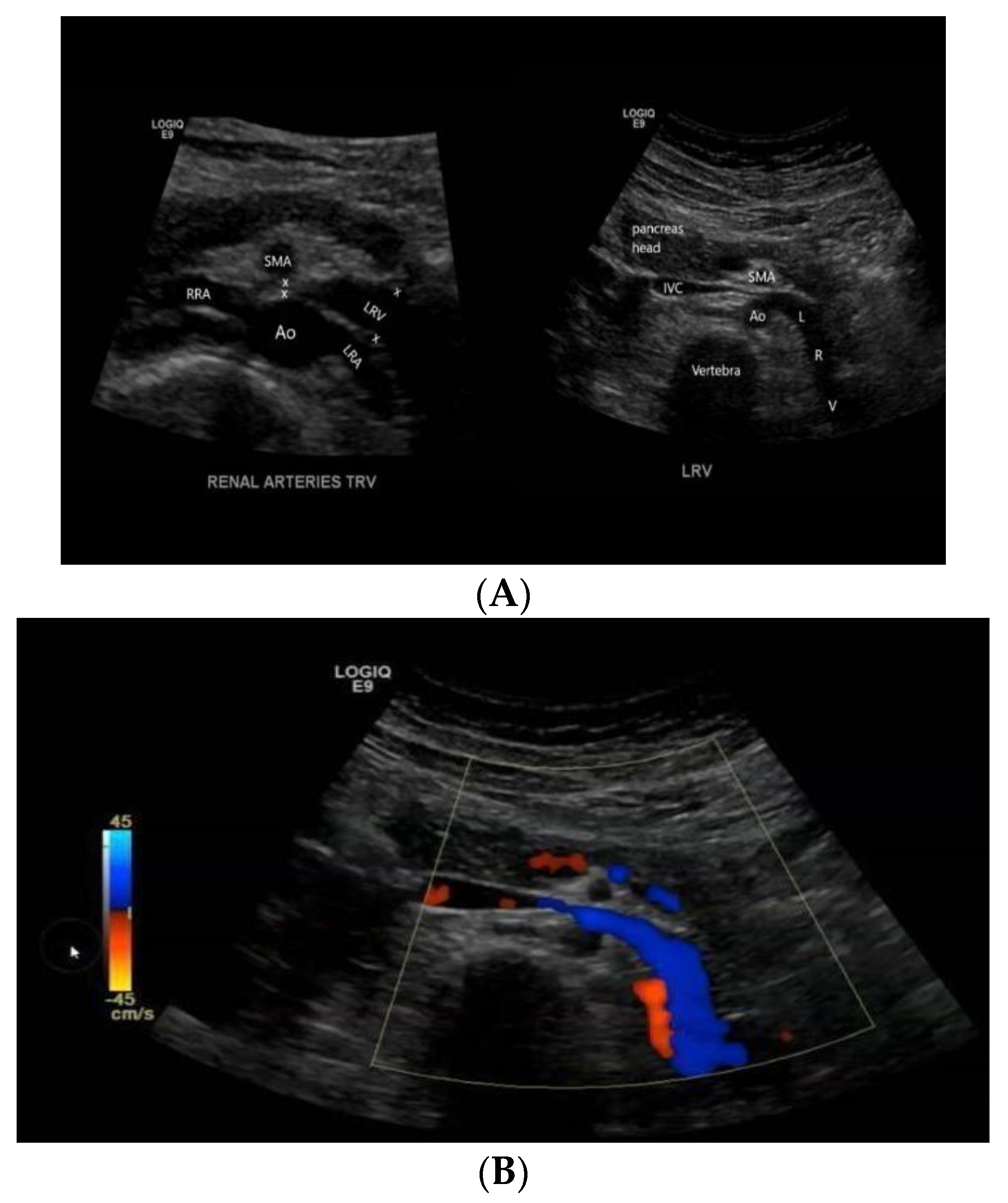
4. Diagnosis of NCS
5. Treatment of NCS
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Granata, A.; Distefano, G.; Sturiale, A.; Figuera, M.; Foti, P.V.; Palmucci, S.; Basile, A. From Nutcracker Phenomenon to Nutcracker Syndrome: A Pictorial Review. Diagnostics 2021, 11, 101. [Google Scholar] [CrossRef]
- Meyer, J.; Rother, U.; Stehr, M.; Meyer, A. Nutcracker syndrome in children: Appearance, diagnostics, and treatment-A systematic review. J. Pediatr. Surg. 2022, 57, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Yoon, T.; Kim, S.H.; Kang, E.; Kim, S. Nutcracker Phenomenon and Syndrome May Be More Prevalent Than Previously Thought. Korean J. Radiol. 2022, 23, 1112–1114. [Google Scholar] [CrossRef]
- Kurklinsky, A.K.; Rooke, T.W. Nutcracker phenomenon and nutcracker syndrome. Mayo Clin. Proc. 2010, 85, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Litra, F.; Barr, L.L. A Rare Cause of Abdominal and Flank Pain in Children: Nutcracker Syndrome. Cureus 2021, 16, e16422. [Google Scholar] [CrossRef] [PubMed]
- Vianello, F.A.; Mazzoni, M.B.; Peeters, G.G.; Fossali, E.F.; Camozzi, P.; Bianchetti, M.G.; Milani, G.P. Micro- and macroscopic hematuria caused by renal vein entrapment: Systematic review of the literature. Pediatr. Nephrol. 2016, 31, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Bin Dahman, H.A.; Aljabry, A.O. A case report of a young girl with recurrent hematuria: A missed diagnosis-renal nutcracker syndrome. BMC Nephrol. 2019, 20, 349. [Google Scholar] [CrossRef]
- Miró, I.; Serrano, A.; Pérez-Ardavín, J.; March, J.A.; Polo, A.; Conca, M.Á.; Sangüesa, C.; Veiga, D.; Carazo, E.; Domínguez, C. Eighteen years of experience with pediatric nutcracker syndrome: The importance of the conservative approach. J. Pediatr. Urol. 2020, 16, 218.e1–218.e6. [Google Scholar] [CrossRef]
- Basaran, E.G.; Yilmaz, A.Ç.; Güngör, Ö.; Tayfur, A.Ç.; Büyükkaragöz, B. Clinical Profile and Renal Ultrasound Characteristics of Children with Nutcracker Syndrome in Turkey. Indian Pediatr. 2022, 59, 28–30. [Google Scholar] [CrossRef]
- Reddy, D.K.; Shekar, P. A Nutcracker Syndrome-A Rare but Important Cause of Varicocele in Adolescent Boys. Urology 2020, 141, 143–146. [Google Scholar] [CrossRef]
- Nutcracker Waldrop, R.D.; Henning, P. Nutcracker Syndrome Masquerading as Renal Colic in an Adolescent Athlete: A Case Report. Clin. Pract. Cases Emerg. Med. 2021, 5, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.F.; Zhou, C.Z.; Fu, Y.Q.; Lv, W.F. Nutcracker syndrome accompanied by hypertension: A case report and literature review. J. Int. Med. Res. 2021, 49, 300060520985733. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, M.B.; Kottanatu, L.; Simonetti, G.D.; Ragazzi, M.; Bianchetti, M.G.; Fossali, E.F.; Milani, G.P. Renal vein obstruction and orthostatic proteinuria: A review. Nephrol. Dial. Transplant. 2011, 26, 562–565. [Google Scholar] [CrossRef] [PubMed]
- Alaygut, D.; Bayram, M.; Soylu, A.; Cakmakcı, H.; Türkmen, M.; Kavukcu, S. Clinical course of children with nutcracker syndrome. Urology 2013, 82, 686–690. [Google Scholar] [CrossRef]
- Gulleroglu, K.; Gulleroglu, B.; Baskin, E. Nutcracker syndrome. World J. Nephrol. 2014, 3, 277–281. [Google Scholar] [CrossRef]
- Wang, R.; Wang, M.; Xia, Z.; Gao, C.; Kuang, Q.; Fang, X.; Yu, M.; Peng, Y.; Li, X.; Wei, Y.; et al. Value of magnetic resonance imaging indices of left renal vein entrapment in the diagnosis of nutcracker syndrome in children. Transl. Pediatr. 2021, 10, 1285–1293. [Google Scholar] [CrossRef]
- Avar-Aydin, P.O.; Ozcakar, Z.B.; Cakar, N.; Fitoz, S.; Karakas, H.D.; Yalcinkaya, F. Nutcracker syndrome: A potentially underdiagnosed cause of proteinuria in children with familial Mediterranean fever. Pediatr. Nephrol. 2022, 37, 1615–1621. [Google Scholar] [CrossRef]
- Wang, C.; Wang, F.; Zhao, B.; Xu, L.; Liu, B.; Guo, Q.; Yang, X.; Wang, R. Coexisting nutcracker phenomenon and superior mesenteric artery syndrome in a patient with IgA nephropathy: A case report. Medicine 2021, 100, e26611. [Google Scholar] [CrossRef]
- Ma, Z.; Liu, X.; Ning, Y.; Shao, J.; Liu, W.; He, X. Nutcracker phenomenon incombination with glomerular nephritis in isolated hematuria patients. Int. Urol. Nephrol. 2013, 45, 809–816. [Google Scholar] [CrossRef]
- Jin, M.; Hu, P.; Ding, R.; Chen, P.; Qiu, Q.; Wu, J.; Liu, S.; Xie, Y.; Chen, X. Effectiveness of supine/standing urinalysis for differential diagnosis of left renal vein entrapment syndrome combined with or without glomerulopathy. Nephrology 2014, 19, 332–338. [Google Scholar] [CrossRef]
- Rao, J.; Yang, J.; Liu, Z.; Wang, L.; Liu, L.; Yin, Z.; Yang, L. Right retrocaval ureter and left nutcracker syndrome: A case report. Urology 2008, 71, 1226.e9. [Google Scholar] [CrossRef] [PubMed]
- Kolber, M.K.; Cui, Z.; Chen, C.K.; Habibollahi, P.; Kalva, S.P. Nutcracker syndrome: Diagnosis and therapy. Cardiovasc. Diagn. Ther. 2021, 11, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Gulleroglu, N.B.; Gulleroglu, K.; Uslu, N.; Baskin, E. Left renal vein entrapment in postural proteinuria: The diagnostic utility of the aortomesenteric angle. Eur. J. Pediatr. 2022, 181, 3339–3343. [Google Scholar] [CrossRef] [PubMed]
- Arthurs, O.J.; Mehta, U.; Set, P.A. Nutcracker and SMA syndromes: What is the normal SMA angle in children? Eur. J. Radiol. 2012, 81, e854–e861. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Sampath, R.; Khan, M.S. Current trends in the diagnosis and management of renal nutcracker syndrome: A review. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Cho, S.W.; Kim, H.D.; Chung, J.W.; Park, J.H.; Han, M.C. Nutcracker syndrome: Diagnosis with Doppler US. Radiology 1996, 198, 93–97. [Google Scholar] [CrossRef]
- Kim, S.H.; Doppler, U.S. CT Diagnosis of Nutcracker Syndrome. Korean J. Radiol. 2019, 20, 1627–1637. [Google Scholar] [CrossRef]
- Atasoy, D.; Cansu, A.; Bekirçavuşoğlu, A.F.; Özdoğan, E.B.; Ahmetoğlu, A. The utility of magnetic resonance angiography in children with nutcracker syndrome. Turk. J. Med. Sci. 2021, 51, 2396–2402. [Google Scholar] [CrossRef]
- Ananthan, K.; Onida, S.; Davies, A.H. Nutcracker Syndrome: An Update on Current Diagnostic Criteria and Management Guidelines. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 886–894. [Google Scholar] [CrossRef]
- Merrett, N.D.; Wilson, R.B.; Cosman, P.; Biankin, A.V. Superior mesenteric artery syndrome: Diagnosis and treatment strategies. J. Gastrointest. Surg. 2009, 13, 287–292. [Google Scholar] [CrossRef]
- Kim, K.W.; Cho, J.Y.; Kim, S.H.; Yoon, J.H.; Kim, D.S.; Chung, J.W.; Park, J.H. Diagnostic value of computed tomographic findings of nutcracker syndrome: Correlation with renal venography and renocaval pressure gradients. Eur. J. Radiol. 2011, 80, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Cheon, J.E.; Kim, W.S.; Kim, I.O.; Kim, S.H.; Yeon, K.M.; Ha, I.S.; Cheong, H.I.; Choi, Y. Nutcracker syndrome in children with gross haematuria: Doppler sonographic evaluation of the left renal vein. Pediatr. Radiol. 2006, 36, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Nalcacioglu, H.; Ceyhan Bilgici, M.; Tekcan, D.; Genc, G.; Bostanci, Y.; Yakupoglu, Y.K.; Sarikaya, S.; Ozkaya, O. Nutcracker Syndrome in Children: Role of Doppler Ultrasonographic Indices in Detecting the Pattern of Symptoms. J. Clin. Med. 2018, 7, 214. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.I.; Park, J.M.; Lee, J.S.; Kim, M.J. Doppler ultrasonographic indices in diagnosing nutcracker syndrome in children. Pediatr. Nephrol. 2007, 22, 409–413. [Google Scholar] [CrossRef]
- Takahashi, Y.; Sano, A.; Matsuo, M. An ultrasonographic classification for diverse clinical symptoms of pediatric nutcracker phenomenon. Clin. Nephrol. 2005, 64, 47–54. [Google Scholar] [CrossRef]
- Chait, J.; Sen, I.; Kalra, M. Nutcracker Syndrome: How to Diagnose It and When/How Should It Be Treated in the Pelvic Venous Disease Population. Tech. Vasc. Interv. Radiol. 2021, 24, 100734. [Google Scholar] [CrossRef]
- Nishimura, Y.; Fushiki, M.; Yoshida, M.; Nakamura, K.; Imai, M.; Ono, T.; Morikawa, S.; Hatayama, T.; Komatz, Y. Left renal vein hypertension in patients with left renal bleeding of unknown origin. Radiology 1986, 160, 663–667. [Google Scholar] [CrossRef]
- Beinart, C.; Sniderman, K.W.; Tamura, S.; Vaughan, E.D., Jr.; Sos, T.A. Left renal vein to inferior vena cava pressure relationship in humans. J. Urol. 1982, 127, 1070–1071. [Google Scholar] [CrossRef]
- He, Y.; Wu, Z.; Chen, S.; Tian, L.; Li, D.; Li, M.; Jin, W.; Zhang, H. Nutcracker syndrome–how well do we know it? Urology 2014, 83, 12–17. [Google Scholar] [CrossRef]
- Shin, J.I.; Park, J.M.; Lee, S.M.; Shin, Y.H.; Kim, J.H.; Lee, J.S.; Kim, M.J. Factors affecting spontaneous resolution of hematuria in childhood nutcracker syndrome. Pediatr. Nephrol. 2005, 20, 609–613. [Google Scholar] [CrossRef]
- Tanaka, H.; Waga, S. Spontaneous remission of persistent severe hematuria in an adolescent with nutcracker syndrome: Seven years’ observation. Clin. Exp. Nephrol. 2004, 8, 68–70. [Google Scholar] [CrossRef] [PubMed]
- Ha, T.S.; Lee, E.J. ACE inhibition can improve orthostatic proteinuria associated with nutcracker syndrome. Pediatr. Nephrol. 2006, 21, 1765–1768. [Google Scholar] [CrossRef]
- Shin, J.I.; Lee, J.S. ACE inhibition in nutcracker syndrome with orthostatic proteinuria: How about a hemodynamic effect? Pediatr. Nephrol. 2007, 22, 758. [Google Scholar] [CrossRef] [PubMed]
- De Macedo, G.L.; Dos Santos, M.A.; Sarris, A.B.; Gomes, R.Z. Diagnosis and treatment of the Nutcracker syndrome: A review of the last 10 years. J. Vasc. Bras. 2018, 17, 220–228. [Google Scholar] [PubMed]
- Wang, L.; Yi, L.; Yang, L.; Liu, Z.; Rao, J.; Liu, L.; Yang, J. Diagnosis and surgical treatment of nutcracker syndrome: A single-center experience. Urology 2009, 73, 871–876. [Google Scholar] [CrossRef]
- Ullery, B.W.; Itoga, N.K.; Mell, M.W. Transposition of the left renal vein for the treatment of nutcracker syndrome in children: A short-term experience. Ann. Vasc. Surg. 2014, 28, 1938.e5. [Google Scholar] [CrossRef]
- Chen, W.; Chu, J.; Yang, J.Y.; Li, H.P.; Zhuang, W.Q.; Huang, Y.H.; Guo, W.B. Endovascular stent placement for the treatment of nutcracker phenomenon in three pediatric patients. J. Vasc. Interv. Radiol. 2005, 16, 1529–1533. [Google Scholar] [CrossRef]
- Cronan, J.C.; Hawkins, C.M.; Kennedy, S.S.; Marshall, K.W.; Rostad, B.S.; Gill, A.E. Endovascular management of nutcracker syndrome in an adolescent patient population. Pediatr. Radiol. 2021, 51, 1487–1496. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Feature Description | References | Normal Values/Notes | Reference Values Compatible with NCS | Instrumental Technique |
|---|---|---|---|---|
| AMA Angle between the abdominal aorta and the SMA | [1,22,29,30,31] | The normal AMA is between 38° and 65°. A smaller AMA than this range of value, causes an entrapment of LRV with a significant increase in the pressure gradient between LRV and IVC | <35° | Doppler US, CT or MRI |
| Beck angle Angle between the aorta and SMA in the point of entrapment of LRV (at the aorto-mesenteric angle) | [1,4] | The beck sign represents the stenosis of the LRV at the aorto-mesenteric angle. | <32° | Doppler US, CT or MRI |
| LRV diameter ratio Comparison between the antero-posterior diameters of the LRV at the renal hilar and stenotic Aorto-mesenteric portion. | [1,4] | A LRV diameter ratio higher than the cut-off value is a specific sign for NCS and has a positive predictive value of 100% | >4.9 | Doppler US, CT or MRI |
| PVR Peak velocity ratio across the entrapped LRV (between the renal hilum and aortomesenteric area | [1,26,27,32] | The best PV ratio cutoff values for the differentiation of the NCS was 4.7 in children. | >4.7 | Doppler US |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cioffi, S.; Di Domenico, F.; Russo, G.; De Nigris, A.; Guarino, S.; Miraglia del Giudice, E.; Marzuillo, P.; Di Sessa, A. Diagnostic Clues in Pediatric Nutcracker Syndrome: From Two Clinical Cases to Current Literature Analysis. Children 2022, 9, 1988. https://doi.org/10.3390/children9121988
Cioffi S, Di Domenico F, Russo G, De Nigris A, Guarino S, Miraglia del Giudice E, Marzuillo P, Di Sessa A. Diagnostic Clues in Pediatric Nutcracker Syndrome: From Two Clinical Cases to Current Literature Analysis. Children. 2022; 9(12):1988. https://doi.org/10.3390/children9121988
Chicago/Turabian StyleCioffi, Speranza, Federica Di Domenico, Giuseppina Russo, Angelica De Nigris, Stefano Guarino, Emanuele Miraglia del Giudice, Pierluigi Marzuillo, and Anna Di Sessa. 2022. "Diagnostic Clues in Pediatric Nutcracker Syndrome: From Two Clinical Cases to Current Literature Analysis" Children 9, no. 12: 1988. https://doi.org/10.3390/children9121988
APA StyleCioffi, S., Di Domenico, F., Russo, G., De Nigris, A., Guarino, S., Miraglia del Giudice, E., Marzuillo, P., & Di Sessa, A. (2022). Diagnostic Clues in Pediatric Nutcracker Syndrome: From Two Clinical Cases to Current Literature Analysis. Children, 9(12), 1988. https://doi.org/10.3390/children9121988