
Rhabdomyolysis in Pediatric Patients with SARS-CoV-2 Infection



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACE-2 | Angiotensin-converting enzyme 2 |
| BACM | Benign acute childhood myositis |
| COVID-19 | Coronavirus disease 2019 |
| CK | Creatine kinase |
| RT-PCR | reverse transcription-polymerase chain reaction assay |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
References
- Buckholz, A.P.; Kaplan, A.; Rosenblatt, R.E.; Wan, D. Clinical Characteristics, Diagnosis, and Outcomes of 6 Patients with COVID-19 Infection and Rhabdomyolysis. Mayo Clin. Proc. 2020, 95, 2557–2559. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Tong, Q. Rhabdomyolysis as Potential Late Complication Associated with COVID-19. Emerg. Infect. Dis. 2020, 26, 1618–1620. [Google Scholar] [CrossRef]
- Khosla, S.G.; Nylen, E.S.; Khosla, R. Rhabdomyolysis in Patients Hospitalized With COVID-19 Infection: Five Case Series. J. Investig. Med. High Impact. Case Rep. 2020, 8, 2324709620984603. [Google Scholar] [CrossRef] [PubMed]
- Meegada, S.; Muppidi, V.; Wilkinson, D.C., 3rd; Siddamreddy, S.; Katta, S.K. Coronavirus Disease 2019-Induced Rhabdomyolysis. Cureus 2020, 12, e10123. [Google Scholar] [CrossRef] [PubMed]
- Rivas-García, S.; Bernal, J.; Bachiller-Corral, J. Rhabdomyolysis as the main manifestation of coronavirus disease 2019. Rheumatology 2020, 59, 2174–2176. [Google Scholar] [CrossRef] [PubMed]
- Solís, J.G.; Esquivel Pineda, A.; Alberti Minutti, P.; Albarrán Sánchez, A. Case Report: Rhabdomyolysis in a Patient with COVID-19: A Proposed Diagnostic-Therapeutic Algorithm. Am. J. Trop. Med. Hyg. 2020, 103, 1158–1161. [Google Scholar] [CrossRef]
- Mokhtari, A.K.; Maurer, L.R.; Christensen, M.A.; Moheb, M.E.; Naar, L.; Alser, O.; Gaitanidis, A.; Langeveld, K.; Kapoen, C.; Breen, K.; et al. Rhabdomyolysis in Severe COVID-19: Male Sex, High Body Mass Index, and Prone Positioning Confer High Risk. J. Surg. Res. 2021, 266, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Mughal, M.S.; Kaur, I.P.; Alhashemi, R.; Rehman, R.; Du, D. Acute viral myositis complicated by rhabdomyolysis: A sole manifestation of COVID-19 infection. J. Community Hosp. Intern. Med. Perspect 2021, 11, 289–291. [Google Scholar] [CrossRef]
- Haroun, M.W.; Dieiev, V.; Kang, J.; Barbi, M.; Marashi Nia, S.F.; Gabr, M.; Eman, G.; Kajita, G.; Swedish, K. Rhabdomyolysis in COVID-19 Patients: A Retrospective Observational Study. Cureus 2021, 13, e12552. [Google Scholar] [CrossRef] [PubMed]
- Gefen, A.M.; Palumbo, N.; Nathan, S.K.; Singer, P.S.; Castellanos-Reyes, L.J.; Sethna, C.B. Pediatric COVID-19-associated rhabdomyolysis: A case report. Pediatr. Nephrol. 2020, 35, 1517–1520. [Google Scholar] [CrossRef]
- Tram, N.; Chiodini, B.; Montesinos, I.; Vicinanza, A.; Beretta-Piccoli, X.; Gubbelmans, N.; Demey, M.; Genis, N.; Tilmanne, A.; Smeesters, P.R.; et al. Rhabdomyolysis and Acute Kidney Injury as Leading COVID-19 Presentation in an Adolescent. Pediatr Infect. Dis. J. 2020, 39, e314–e315. [Google Scholar] [CrossRef] [PubMed]
- Gilpin, S.; Byers, M.; Byrd, A.; Cull, J.; Peterson, D.; Thomas, B.; Jacobson, P. Rhabdomyolysis as the Initial Presentation of SARS-CoV-2 in an Adolescent. Pediatrics 2021, 147, e2020019273. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, P.K.; Sigoli, E.; Bragança, L.J.G.; Cornachione, A.S. The Musculoskeletal Involvement After Mild to Moderate COVID-19 Infection. Front. Physiol. 2022, 13, 813924. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.Y.; Wu, P.-S.; Cheng, C.-F.; Yiang, G.-T.; Yu, C.-H. Characteristics, contacts, and relative risk of SARS-CoV-2 infection among children during school closures. J. Microbiol. Immunol. Infect. 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- Shao, W.; Zhang, W.; Fang, X.; Yu, D.; Wang, X. Challenges of SARS-CoV-2 Omicron Variant and appropriate countermeasures. J. Microbiol. Immunol. Infect. 2022, 55, 387–394. [Google Scholar] [CrossRef]
- Suh, J.; Mukerji, S.S.; Collens, S.I.; Padera, R.F., Jr.; Pinkus, G.S.; Amato, A.A.; Solomon, I.H. Skeletal Muscle and Peripheral Nerve Histopathology in COVID-19. Neurology 2021, 97, e849–e858. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.-C.; Cheng, H.-Y.; Chang, H.-H.; Liu, C.-C.; Yang, C.-C.; Jian, S.-W.; Liu, D.-P.; Cohen, T.; Lin, H.-H. Comparison of Estimated Effectiveness of Case-Based and Population-Based Interventions on COVID-19 Containment in Taiwan. JAMA Intern. Med. 2021, 181, 913–921. [Google Scholar] [CrossRef]
- Steinbrook, R. Lessons From the Success of COVID-19 Control in Taiwan. JAMA Intern. Med. 2021, 181, 922. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.T.; Tsai, J.J.; Chang, K.; Chen, C.H.; Lin, P.C.; Tsai, C.Y.; Tsai, Y.Y.; Hsu, M.C.; Chuang, W.L.; Chang, J.M.; et al. Identification and Analysis of SARS-CoV-2 Alpha Variants in the Largest Taiwan COVID-19 Outbreak in 2021. Front. Med. 2022, 9, 869818. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.-C.; Chang, W.-W.; Lee, W.-S. Analysis of an outbreak of COVID-19(alpha-variant) with rapid progression to mortality in Taipei, Taiwan. J. Infect. 2022, 84, e33–e34. [Google Scholar] [CrossRef] [PubMed]
- Chao, K.Y.; Hsiao, T.Y.; Cheng, W. Survey Responses of School Closures During the COVID-19 Outbreak in Taiwan. Front. Public. Health 2022, 10, 726924. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Centers for Disease Control. Available online: https://sites.google.com/cdc.gov.tw/2019ncov/taiwan (accessed on 24 August 2022).
- Grifoni, A.; Sette, A. From Alpha to omicron: The response of T cells. Curr. Res. Immunol. 2022, 3, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Korobova, Z.R.; Arsentieva, N.A.; Liubimova, N.E.; Dedkov, V.G.; Gladkikh, A.S.; Sharova, A.A.; Chernykh, E.I.; Kashchenko, V.A.; Ratnikov, V.A.; Gorelov, V.P.; et al. A Comparative Study of the Plasma Chemokine Profile in COVID-19 Patients Infected with Different SARS-CoV-2 Variants. Int. J. Mol. Sci. 2022, 23, 9058. [Google Scholar] [CrossRef]
- Natekar, J.P.; Pathak, H.; Stone, S.; Kumari, P.; Sharma, S.; Auroni, T.T.; Arora, K.; Rothan, H.A.; Kumar, M. Differential Pathogenesis of SARS-CoV-2 Variants of Concern in Human ACE2-Expressing Mice. Viruses 2022, 14, 1139. [Google Scholar] [CrossRef] [PubMed]
- Thorne, L.G.; Bouhaddou, M.; Reuschl, A.K.; Zuliani-Alvarez, L.; Polacco, B.; Pelin, A.; Batra, J.; Whelan, M.V.X.; Hosmillo, M.; Fossati, A.; et al. Evolution of enhanced innate immune evasion by SARS-CoV-2. Nature 2022, 602, 487–495. [Google Scholar] [CrossRef]
- Halfmann, P.J.; Iida, S.; Iwatsuki-Horimoto, K.; Maemura, T.; Kiso, M.; Scheaffer, S.M.; Darling, T.L.; Joshi, A.; Loeber, S.; Singh, G.; et al. SARS-CoV-2 Omicron virus causes attenuated disease in mice and hamsters. Nature 2022, 603, 687–692. [Google Scholar] [CrossRef]
- Shuai, H.; Chan, J.F.; Hu, B.; Chai, Y.; Yuen, T.T.; Yin, F.; Huang, X.; Yoon, C.; Hu, J.C.; Liu, H.; et al. Attenuated replication and pathogenicity of SARS-CoV-2 B.1.1.529 Omicron. Nature 2022, 603, 693–699. [Google Scholar] [CrossRef]
- Kerr, J.; Macartney, K.; Britton, P.N. Influenza-associated myositis: A single-centre, 5-year retrospective study. Eur. J. Pediatrics 2021, 180, 577–584. [Google Scholar] [CrossRef]
- Chiu, N.C.; Chi, H.; Tai, Y.L.; Peng, C.C.; Tseng, C.Y.; Chen, C.C.; Tan, B.F.; Lin, C.Y. Impact of Wearing Masks, Hand Hygiene, and Social Distancing on Influenza, Enterovirus, and All-Cause Pneumonia During the Coronavirus Pandemic: Retrospective National Epidemiological Surveillance Study. J. Med. Internet Res. 2020, 22, e21257. [Google Scholar] [CrossRef]
- Brisca, G.; Mariani, M.; Pirlo, D.; Romanengo, M.; Pistorio, A.; Gaiero, A.; Panicucci, C.; Piccotti, E.; Bruno, C. Management and outcome of benign acute childhood myositis in pediatric emergency department. Ital. J. Pediatr. 2021, 47, 57. [Google Scholar] [CrossRef]
- Hannah, J.R.; Ali, S.S.; Nagra, D.; Adas, M.A.; Buazon, A.D.; Galloway, J.B.; Gordon, P.A. Skeletal muscles and COVID-19: A systematic review of rhabdomyolysis and myositis in SARS-CoV-2 infection. Clin. Exp. Rheumatol. 2022, 40, 329–338. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 6 | 10 | 10 | 6 | 8 | 7 | 6 | 5 |
| Sex | M | F | M | F | M | M | M | M |
| Duration between calf pain and fever (days) | 5 | 5 | 4 | 3 | 5 | 4 | 4 | 4 |
| SARS-CoV-2 RT-PCR CT value | 16 | 17 | 20 | 24 | 13 | 15 | 21 | 17 |
| White blood cell count (/μL) | 3220 | 2320 | 4170 | 2650 | 3940 | 4500 | 5350 | 4710 |
| Hemoglobin (g/dL) | 13.1 | 13.0 | 14.7 | 12.6 | 13.2 | 14.0 | 11.6 | 13.6 |
| Platelet count (×103/μL) | 227 | 201 | 250 | 231 | 121 | 231 | 178 | 277 |
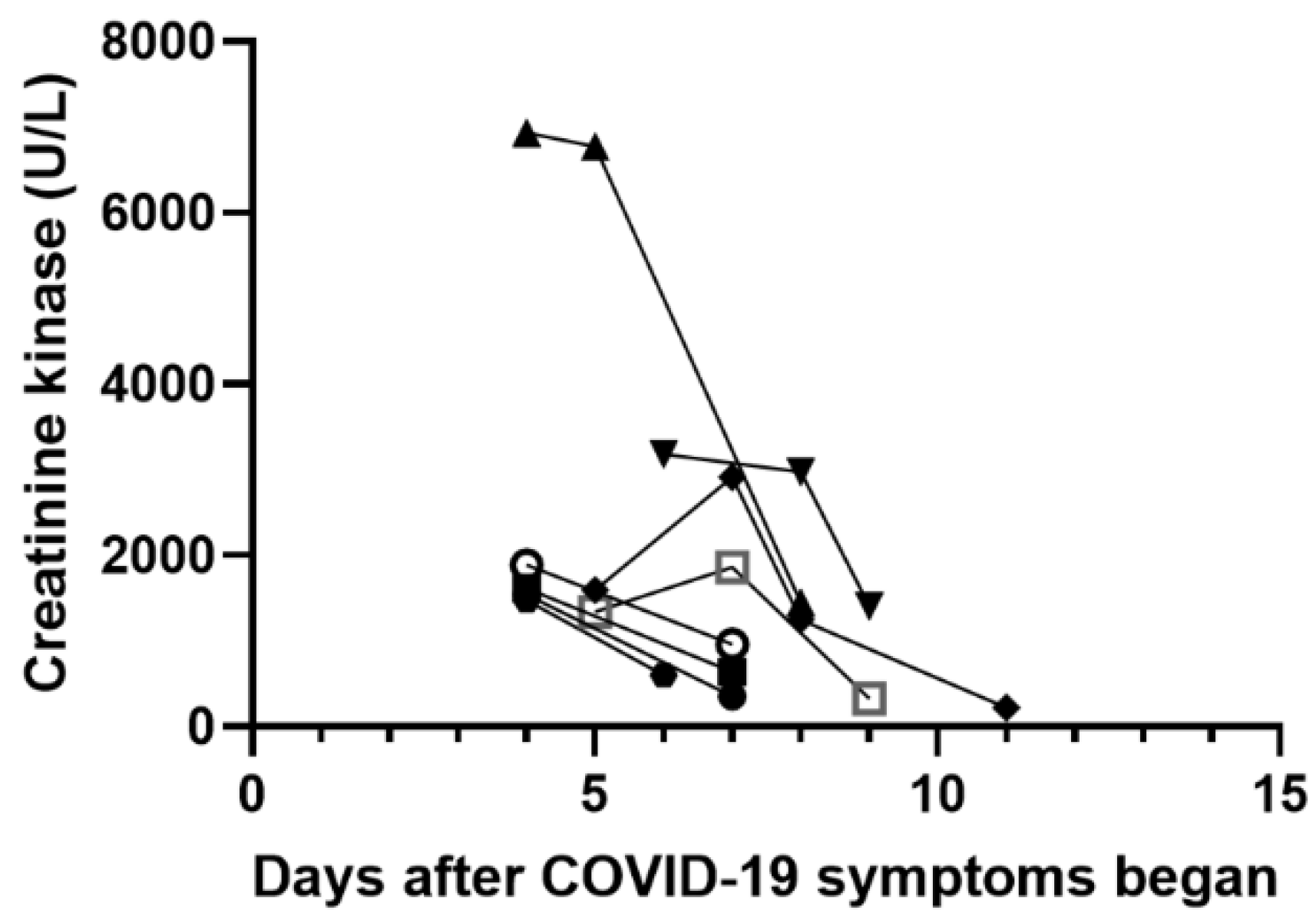
| Creatine kinase (CK, U/L) | 1596 | 3180 | 1543 | 6937 | 1614 | 1892 | 1346 | 1475 |
| Creatine kinase MB fraction (CK-MB, ng/mL) | 19.8 | 66.8 | 47.5 | 91.0 | 20.9 | 30.1 | 18.2 | 19.2 |
| Aspartate aminotransferase (AST, U/L) | ND | 184 | 68 | 170 | 66 | 65 | 119 | 60 |
| Alanine aminotransferase (ALT, U/L) | 15 | 29 | 23 | 34 | 16 | 20 | 25 | 19 |
| Blood urea nitrogen (BUN, mg/dL) | 12 | 9 | 13 | 9 | 11 | 13 | 7 | 11 |
| Serum creatinine (mg/dL) | 0.46 | 0.45 | 0.46 | 0.28 | 0.38 | 0.49 | 0.38 | 0.31 |
| C-reactive protein (CRP, mg/dL) | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 |
| Serum sodium (mmol/L) | 138 | 140 | 138 | 141 | 138 | 140 | 141 | 137 |
| Serum potassium (mmol/L) | 3.9 | 3.7 | 4.0 | 4.2 | 3.9 | 3.9 | 4.0 | 3.7 |
| Urine occult blood | - | ND | - | - | ND | ND | - | - |
| Urine red blood cell count (/HPF) | 0–2 | ND | 0–2 | 0–2 | ND | ND | 0–2 | 0–2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, P.-S.; Wong, S.-B.; Cheng, C.-F.; Yu, C.-H. Rhabdomyolysis in Pediatric Patients with SARS-CoV-2 Infection. Children 2022, 9, 1441. https://doi.org/10.3390/children9101441
Wu P-S, Wong S-B, Cheng C-F, Yu C-H. Rhabdomyolysis in Pediatric Patients with SARS-CoV-2 Infection. Children. 2022; 9(10):1441. https://doi.org/10.3390/children9101441
Chicago/Turabian StyleWu, Ping-Sheng, Shi-Bing Wong, Ching-Feng Cheng, and Chun-Hsien Yu. 2022. "Rhabdomyolysis in Pediatric Patients with SARS-CoV-2 Infection" Children 9, no. 10: 1441. https://doi.org/10.3390/children9101441
APA StyleWu, P.-S., Wong, S.-B., Cheng, C.-F., & Yu, C.-H. (2022). Rhabdomyolysis in Pediatric Patients with SARS-CoV-2 Infection. Children, 9(10), 1441. https://doi.org/10.3390/children9101441