
Factors Influencing the Progression and Direction of Scoliosis in Children with Neurological Disorders

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
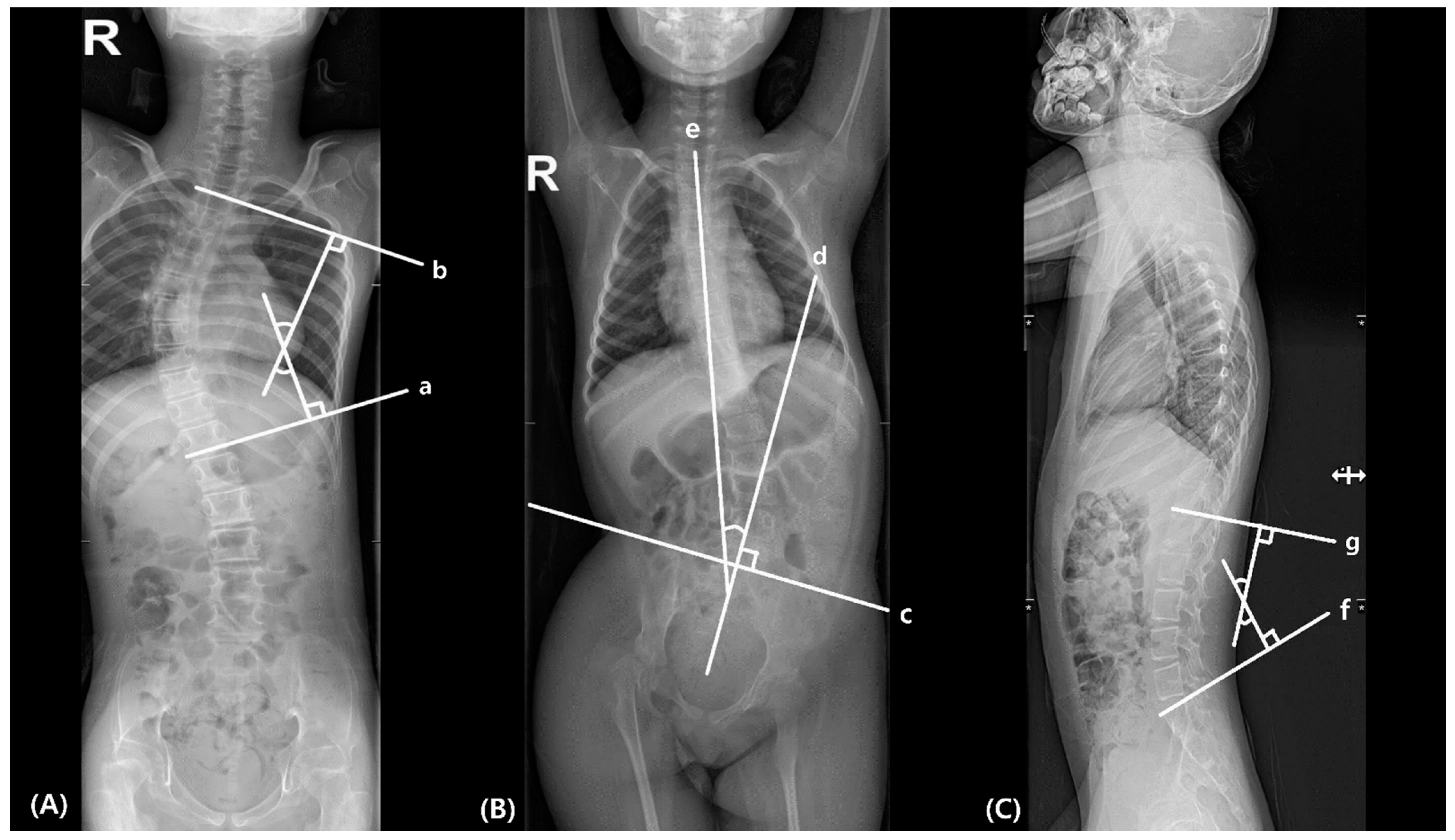
2.2. Measurement Parameters
2.2.1. Scoliosis
2.2.2. Pelvic Obliquity (PO)
2.2.3. Lumbar Lordosis
2.2.4. Vertebral Rotation
2.3. Statistical Methods
3. Results
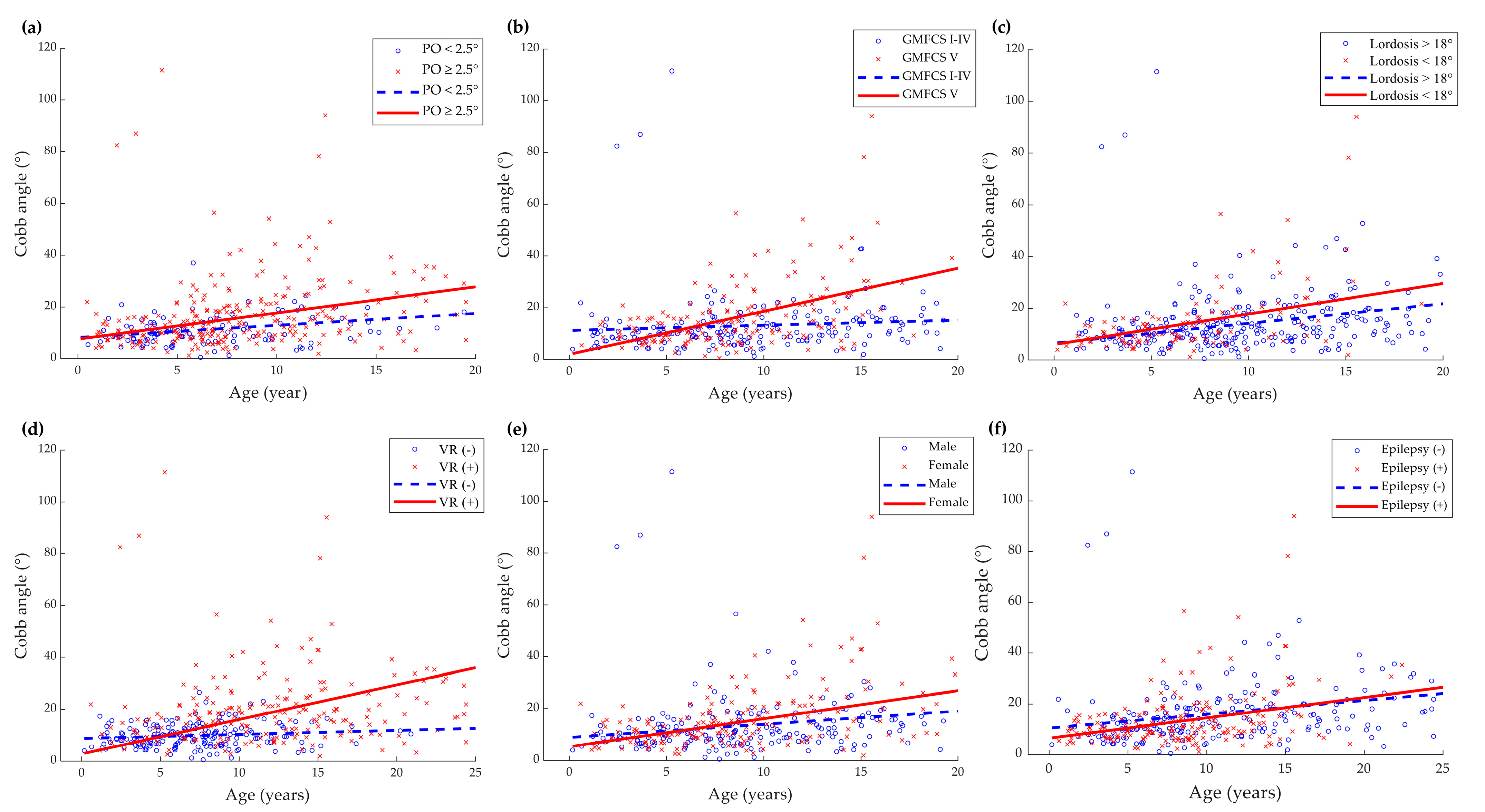
3.1. Factors Affecting the Progression of Scoliosis
3.2. Factors Affecting the Apex Side of Scoliosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roberts, S.B.; Tsirikos, A.I. Factors influencing the evaluation and management of neuromuscular scoliosis: A review of the literature. J. Back Musculoskelet. Rehabil. 2016, 29, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kajiura, I.; Suzuki, T.; Kawabata, H. Natural history of scoliosis in cerebral palsy and risk factors for progression of scoliosis. J. Orthop. Sci. 2018, 23, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Loeters, M.J.; Maathuis, C.G.; Hadders-Algra, M. Risk factors for emergence and progression of scoliosis in children with severe cerebral palsy: A systematic review. Dev. Med. Child. Neurol. 2010, 52, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Shelton, J.E.; Ketchum, J.M.; Cifu, D.X.; Palmer, D.; Sparkman, A.; Jermer-Gu, M.K.; Mendigorin, M. Natural history of scoliosis in nonambulatory spastic tetraplegic cerebral palsy. PM&R 2011, 3, 27–32. [Google Scholar]
- Hagglund, G. Association between pelvic obliquity and scoliosis, hip displacement and asymmetric hip abduction in children with cerebral palsy: A cross-sectional registry study. BMC Musculoskelet. Disord. 2020, 21, 464. [Google Scholar] [CrossRef] [PubMed]
- Porter, D.; Michael, S.; Kirkwood, C. Patterns of postural deformity in non-ambulant people with cerebral palsy: What is the relationship between the direction of scoliosis, direction of pelvic obliquity, direction of windswept hip deformity and side of hip dislocation? Clin. Rehabil. 2007, 21, 1087–1096. [Google Scholar] [CrossRef]
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content validity of the expanded and revised Gross Motor Function Classification System. Dev. Med. Child. Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef]
- Cobb, J. Outline for the study of scoliosis. Instr. Course Lect. AAOS 1948, 5, 261–275. [Google Scholar]
- King, H.A.; Moe, J.H.; Bradford, D.S.; Winter, R.B. The selection of fusion levels in thoracic idiopathic scoliosis. J. Bone Jt. Surg. Am. 1983, 65, 1302–1313. [Google Scholar] [CrossRef]
- Maloney, W.J.; Rinsky, L.A.; Gamble, J.G. Simultaneous correction of pelvic obliquity, frontal plane, and sagittal plane deformities in neuromuscular scoliosis using a unit rod with segmental sublaminar wires: A preliminary report. J. Pediatr. Orthop. 1990, 10, 742–749. [Google Scholar] [CrossRef]
- Ames, C.P.; Smith, J.S.; Scheer, J.K.; Bess, S.; Bederman, S.S.; Deviren, V.; Lafage, V.; Schwab, F.; Shaffrey, C.I. Impact of spinopelvic alignment on decision making in deformity surgery in adults: A review. J. Neurosurg. Spine 2012, 16, 547–564. [Google Scholar] [CrossRef] [PubMed]
- Nash, C.; Moe, J.H. A study of vertebral rotation. J. Bone Jt. Surg Am. 1969, 51, 223–229. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Shefi, S.; Soudack, M.; Konen, E.; Been, E. Development of the lumbar lordotic curvature in children from age 2 to 20 years. Spine (Phila Pa 1976) 2013, 38, E602–E608. [Google Scholar] [CrossRef]
- Reamy, B.V.; Slakey, J. Adolescent idiopathic scoliosis: Review and current concepts. Am. Fam. Physician 2001, 64, 111–116. [Google Scholar]
- Saito, N.; Ebara, S.; Ohotsuka, K.; Kumeta, H.; Takaoka, K. Natural history of scoliosis in spastic cerebral palsy. Lancet 1998, 351, 1687–1692. [Google Scholar] [CrossRef]
- Allam, A.M.; Schwabe, A.L. Neuromuscular scoliosis. PM&R 2013, 5, 957–963. [Google Scholar]
- Lee, S.Y.; Chung, C.Y.; Lee, K.M.; Kwon, S.S.; Cho, K.J.; Park, M.S. Annual changes in radiographic indices of the spine in cerebral palsy patients. Eur. Spine J. 2016, 25, 679–686. [Google Scholar] [CrossRef]
- Garg, S.; Engelman, G.; Yoshihara, H.; McNair, B.; Chang, F. The Relationship of Gross Motor Functional Classification Scale Level and Hip Dysplasia on the Pattern and Progression of Scoliosis in Children with Cerebral Palsy. Spine Deform. 2013, 1, 266–271. [Google Scholar] [CrossRef]
- Hasler, C.; Brunner, R.; Grundshtein, A.; Ovadia, D. Spine deformities in patients with cerebral palsy; the role of the pelvis. J. Child. Orthop. 2020, 14, 9–16. [Google Scholar] [CrossRef]
- Patel, J.; Shapiro, F. Simultaneous progression patterns of scoliosis, pelvic obliquity, and hip subluxation/dislocation in non-ambulatory neuromuscular patients: An approach to deformity documentation. J. Child. Orthop. 2015, 9, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.P.; Pai Kanhangad, M.; Gullia, A. Curve severity and apical vertebral rotation and their association with curve flexibility in adolescent idiopathic scoliosis. Musculoskelet. Surg. 2021, 105, 303–308. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Bertoncelli, D.; Elbaum, L.; Latalski, M.; Altamura, P.; Musoff, C.; Rampal, V.; Solla, F. Validation of a Clinical Prediction Model for the Development of Neuromuscular Scoliosis: A Multinational Study. Pediatr. Neurol. 2018, 79, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, K.; Wagner, P.; Rodby-Bousquet, E. Development of a risk score for scoliosis in children with cerebral palsy. Acta Orthop. 2020, 91, 203–208. [Google Scholar] [CrossRef]
- Nguyen, D.V.; Senturk, D.; Carroll, R.J. Covariate-Adjusted Linear Mixed Effects Model with an Application to Longitudinal Data. J. Nonparametr Stat. 2008, 20, 459–481. [Google Scholar] [CrossRef]
- Ruck-Gibis, J.; Plotkin, H.; Hanley, J.; Wood-Dauphinee, S. Reliability of the gross motor function measure for children with osteogenesis imperfecta. Pediatr. Phys. Ther. 2001, 13, 10–17. [Google Scholar] [CrossRef]
- Wright, M.J.; Halton, J.M.; Martin, R.F.; Barr, R.D. Long-term gross motor performance following treatment for acute lymphoblastic leukemia. Med. Pediatr. Oncol. Off. J. SIOP—Int. Soc. Pediatr. Oncol. (Soc. Int. D’oncologie Pédiatrique 1998, 31, 86–90. [Google Scholar] [CrossRef]
- Miller, A.; Temple, T.; Miller, F. Impact of orthoses on the rate of scoliosis progression in children with cerebral palsy. J. Pediatr. Orthop. 1996, 16, 332–335. [Google Scholar] [CrossRef]
- Shakil, H.; Iqbal, Z.A.; Al-Ghadir, A.H. Scoliosis: Review of types of curves, etiological theories and conservative treatment. J. Back Musculoskelet. Rehabil. 2014, 27, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Shilt, J.S.; Lai, L.P.; Cabrera, M.N.; Frino, J.; Smith, B.P. The impact of intrathecal baclofen on the natural history of scoliosis in cerebral palsy. J. Pediatr. Orthop. 2008, 28, 684–687. [Google Scholar] [CrossRef] [PubMed]
- Jones-Quaidoo, S.M.; Yang, S.; Arlet, V. Surgical management of spinal deformities in cerebral palsy. A review. J. Neurosurg. Spine 2010, 13, 672–685. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Value, N (Range or %) |
|---|---|
| Subjects | 116 |
| Female | 55 (47.4) |
| Age at the first radiograph (years) 1 | 3.1 (1.7–5.9) |
| Age at the last radiograph (years) 1 | 18.05 (11.34–21.91) |
| Interval between each radiograph (years) 1 | 1.11 (0.75–1.91) |
| Period between initial and last radiographs (years) 1 | 5.0 (2.6–8.4) |
| Handedness, right/left/unknown | 38/34/44 (32.8/29.3/38.0) |
| Functional asymmetry of upper limbs, yes/no/unknown | 56/47/13 (48.3/40.5/11.2) |
| Presence of epilepsy | 51 (44.0) |
| GMFCS 2 level | |
| I | 7 (6.4) |
| II | 14 (12.7) |
| III | 6 (5.5) |
| IV | 37 (33.6) |
| V | 46 (41.8) |
| Measurements | ICC 1 | 95% CI 2 |
|---|---|---|
| Scoliosis Cobb angle (°) | 0.955 | 0.945–0.964 |
| Pelvic obliquity (°) | 0.840 | 0.804–0.870 |
| Lumbar lordosis angle (°) | 0.929 | 0.906–0.945 |
| Vertebral rotation (Nash-Moe grade) | 0.807 | 0.755–0.847 |
| Apex of Scoliosis, N (%) | p Value | ||||
|---|---|---|---|---|---|
| Right | Left | Total | |||
| Functional asymmetry of upper limbs | Yes | 13 (33.3) | 26 (66.7) | 39 (100.0) | 0.39 |
| No | 14 (43.8) | 18 (56.3) | 32 (100.0) | ||
| Unknown | 6 (54.5) | 5 (45.5) | 11 (100.0) | ||
| Handedness | Right | 6 (54.5) | 5 (45.5) | 11 (100.0) | 0.12 |
| Left | 13 (41.9) | 18 (58.1) | 31 (100.0) | ||
| Unknown | 4 (21.1) | 15 (78.9) | 19 (100.0) | ||
| Higher side of pelvic obliquity | Right | 13 (28.9) | 32 (71.1) | 45 (100.0) | <0.001 * |
| Left | 11 (84.6) | 2 (15.4) | 13 (100.0) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, Y.-J.; Park, J.-G.; Jo, L.; Hwang, Y.; Yoon, M.-J.; Kim, J.-S.; Lim, S.; Hong, B.-Y. Factors Influencing the Progression and Direction of Scoliosis in Children with Neurological Disorders. Children 2022, 9, 81. https://doi.org/10.3390/children9010081
Yoo Y-J, Park J-G, Jo L, Hwang Y, Yoon M-J, Kim J-S, Lim S, Hong B-Y. Factors Influencing the Progression and Direction of Scoliosis in Children with Neurological Disorders. Children. 2022; 9(1):81. https://doi.org/10.3390/children9010081
Chicago/Turabian StyleYoo, Yeun-Jie, Jung-Geun Park, Leechan Jo, Youngdeok Hwang, Mi-Jeong Yoon, Joon-Sung Kim, Seonghoon Lim, and Bo-Young Hong. 2022. "Factors Influencing the Progression and Direction of Scoliosis in Children with Neurological Disorders" Children 9, no. 1: 81. https://doi.org/10.3390/children9010081
APA StyleYoo, Y.-J., Park, J.-G., Jo, L., Hwang, Y., Yoon, M.-J., Kim, J.-S., Lim, S., & Hong, B.-Y. (2022). Factors Influencing the Progression and Direction of Scoliosis in Children with Neurological Disorders. Children, 9(1), 81. https://doi.org/10.3390/children9010081