
The Social Networks and Social Support of Siblings of Children with Cancer

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Screening and Recruitment
2.3. Data Collection
2.4. Data Integration and Analysis
3. Results
3.1. Sample Demographics
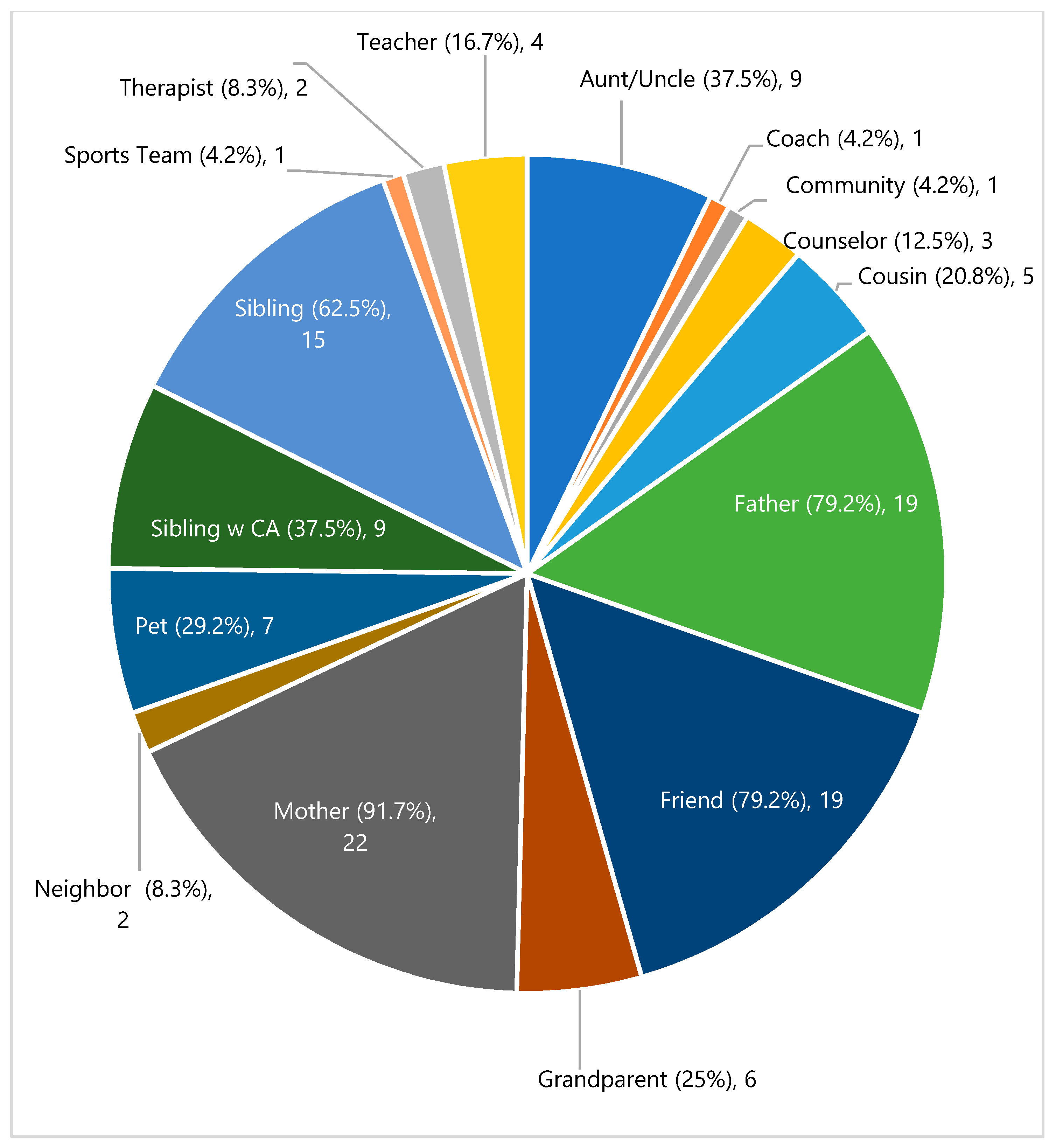
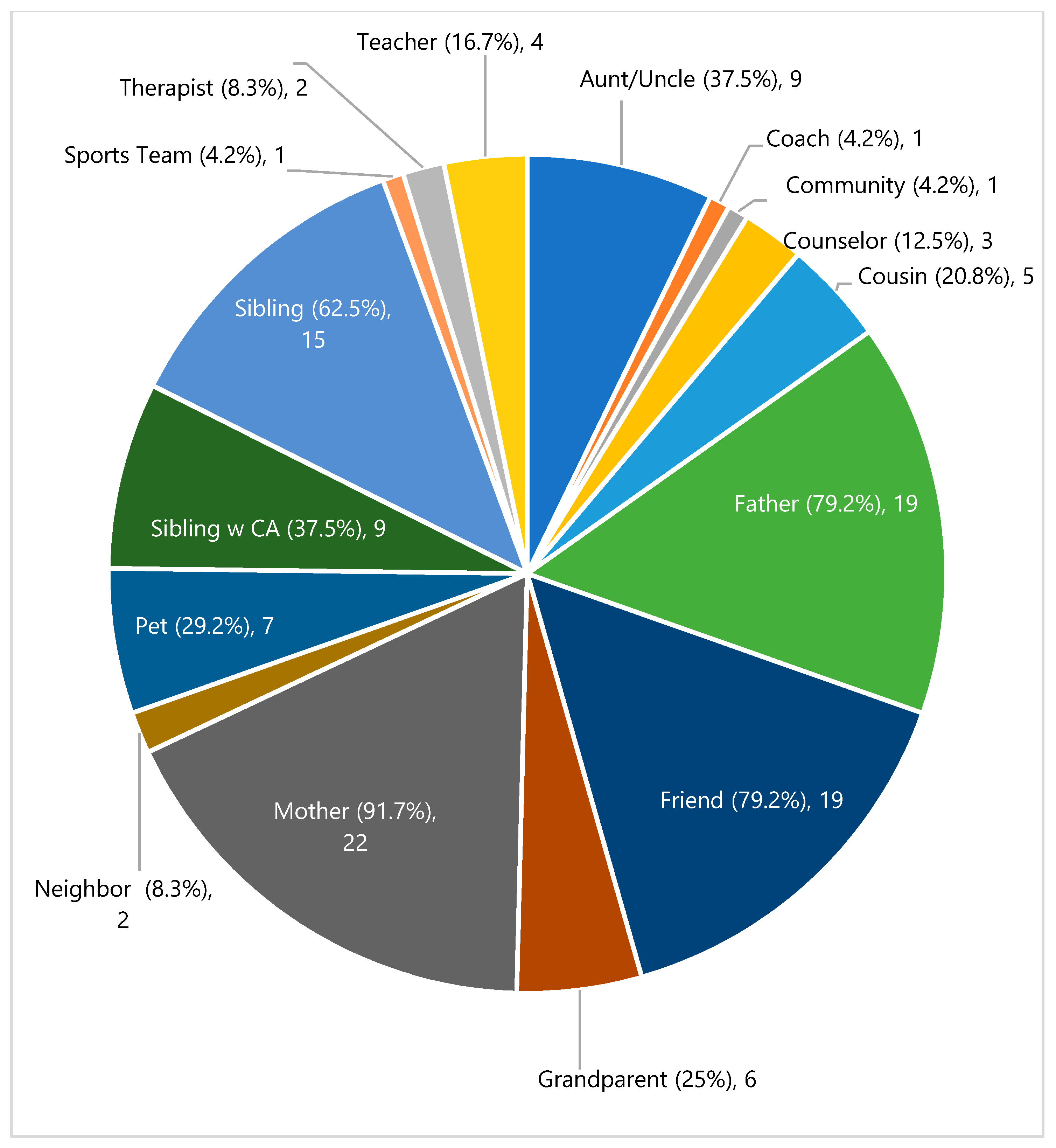
3.2. Sources of Support
3.3. Types of Social Support Received
3.4. Hardest Things and Most Helpful Supports Reported by Siblings
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| ECO-MAPPING INTERVIEW GUIDE |
|---|
| In this interview we are going to talk about the people in your life that provide you with support and help you. First, think about the people in your life who have supported you. This can be people that you see in person every day, or people that you text, talk or chat with online. We’re going to make a list of people you feel have supported you the most throughout your sibling’s cancer diagnosis and treatments. Together, we are going to make a diagram of your relationships with these people. Each circle will represent a person that you feel supports you. We are going to put your name in the center circle. Next let’s add the names of the people and relationships you have been thinking about. We are going to talk about each person on your map here. I’m going to ask you a few questions about each person, including their relationship with you, and how they support you. As we go, you can make changes to the map, by adding or subtracting people from your map. For each person identified in the siblings eco-map ask the following questions:
|
References
- Kobayashi, K.; Hayakawa, A.; Hohashi, N. Interrelations between siblings and parents in families living with children with cancer. J. Fam. Nurs. 2015, 21, 119–148. [Google Scholar] [CrossRef] [PubMed]
- Woodgate, R.L. Siblings’ Experiences with Childhood Cancer: A Different Way of Being in the Family. Cancer Nurs. 2006, 29, 406–414. [Google Scholar] [CrossRef]
- Alderfer, M.A.; Labay, L.E.; Kazak, A.E. Brief report: Does posttraumatic stress apply to siblings of childhood cancer survivors? J. Pediatr. Psychol. 2003, 28, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Alderfer, M.A.; Long, K.A.; Lown, E.A.; Marsland, A.L.; Ostrowski, N.L.; Hock, J.M.; Ewing, L.J. Psychosocial adjustment of siblings of children with cancer: A systematic review. Psycho-Oncology 2010, 19, 789–805. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.M.; Kaal, K.J.; Bradley, L.; Alderfer, M.A. Cancer-related traumatic stress reactions in siblings of children with cancer. Fam. Syst. Health 2013, 31, 205–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, K.A.; Lehmann, V.; Gerhardt, C.A.; Carpenter, A.L.; Marsland, A.L.; Alderfer, M.A. Psychosocial functioning and risk factors among siblings of children with cancer: An updated systematic review. Psycho-Oncol. 2018, 27, 1467–1479. [Google Scholar] [CrossRef]
- Gerhardt, C.A.; Lehmann, V.; Long, K.A.; Alderfer, M.A. Supporting Siblings as a Standard of Care in Pediatric Oncology. Pediatr. Blood Cancer 2015, 62 (Suppl. 5), S750–S804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychological Association. Dictionary of Psychology. Available online: https://dictionary.apa.org/social-support (accessed on 12 July 2021).
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef]
- Barrera, M.; Fleming, C.F.; Khan, F.S. The role of emotional social support in the psychological adjustment of siblings of children with cancer. Child Care Health Dev. 2004, 30, 103–111. [Google Scholar] [CrossRef]
- Cheng, Y.; Li, X.; Lou, C.; Sonenstein, F.L.; Kalamar, A.; Jejeebhoy, S.; Delany-Moretlwe, S.; Brahmbhatt, H.; Olumide, A.O.; Ojengbede, O. The association between social support and mental health among vulnerable adolescents in five cities: Findings from the study of the well-being of adolescents in vulnerable environments. J. Adolesc. Health 2014, 55, S31–S38. [Google Scholar] [CrossRef] [Green Version]
- Kerres Malecki, C.; Kilpatrick Demary, M. Measuring perceived social support: Development of the child and adolescent social support scale (CASSS). Psychol. Sch. 2002, 39, 1–18. [Google Scholar] [CrossRef]
- Uchino, B.N. Understanding the Links Between Social Support and Physical Health: A Life-Span Perspective With Emphasis on the Separability of Perceived and Received Support. Perspect. Psychol. Sci. 2009, 4, 236–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alderfer, M.A.; Hodges, J.A. Supporting Siblings of Children with Cancer: A Need for Family-School Partnerships. Sch. Ment. Health 2010, 2, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Samson, K.; Rourke, M.T.; Alderfer, M.A. A qualitative analysis of the impact of childhood cancer on the lives of siblings at school, in extracurricular activities, and with friends. Clin. Pract. Pediatric Psychol. 2016, 4, 362–372. [Google Scholar] [CrossRef]
- Wawrzynski, S.E.; Schaefer, M.R.; Schvaneveldt, N.; Alderfer, M.A. Social support and siblings of children with cancer: A scoping review. Psycho-Oncology 2021, 30, 1232–1245. [Google Scholar] [CrossRef]
- Barrera, M.; Chung, J.Y.Y.; Fleming, C.F. A Group Intervention for Siblings of Pediatric Cancer Patients. J. Psychosoc. Oncol. 2004, 22, 21–39. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoom Video Communications for Healthcare, Inc. Zoom Cloud Meeting (Version 4.6.9) [Software]. 2020. Available online: https://explore.zoom.us/en/healthcare/ (accessed on 12 July 2021).
- O’Toole, M.T. Miller-Keane Encyclopedia and Dictonary of Medicine, Nusing and Allied Health; Elsevier: Amsterdam, The Netherlands, 2003. [Google Scholar]
- Reblin, M.; Ketcher, D.; Forsyth, P.; Mendivil, E.; Kane, L.; Pok, J.; Meyer, M.; Wu, Y.P.; Agutter, J. Outcomes of an electronic social network intervention with neuro-oncology patient family caregivers. J. Neurooncol. 2018, 139, 643–649. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, 25; IBM Corp: Armonk, NY, USA, 2017. [Google Scholar]
- Dedoose Version 8.0.35 Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data; SocioCulturual Research Consultants, LLC.: Los Angeles, CA, USA, 2018.
- Bernard, H.R.; Ryan, G.W. Analyzing Qualitative Data: Systematic Approaches; Sage Publications: Thousand Oaks, CA, USA, 2010; pp. 287–300. [Google Scholar]
- Saldaña, J. The Coding Manual for Qualitative Researchers, 3rd ed.; Sage: Los Angeles, CA, USA; London, UK, 2016. [Google Scholar]
- Miles, M.B.; Huberman, A.M.; Saldana, J. Qualitative Data Analysis: A Methods Sourcebook, 3rd ed.; Sage Publishing: Thousand Oaks, CA, USA, 2014; p. 381. [Google Scholar]
- Birks, M.; Chapman, Y.; Francis, K. Memoing in qualitative research. J. Res. Nurs. 2008, 13, 68–75. [Google Scholar] [CrossRef]
- Mays, N.; Pope, C. Qualitative research in health care. Assessing quality in qualitative research. BMJ 2000, 320, 50–52. [Google Scholar] [CrossRef]
- Brosnan, P.; Davis, K.A.; Mazzenga, M.; Oberoi, A.R.; Sharkey, C.M.; Buchbinder, D.; Alderfer, M.A.; Long, K.A. Psychosocial care providers’ perspectives: Barriers to implementing services for siblings of children with cancer. Pediatric Blood Cancer 2021, 69, e29418. [Google Scholar] [CrossRef] [PubMed]
- Long, K.A.; Pariseau, E.M.; Muriel, A.C.; Chu, A.; Kazak, A.E.; Leon, M.; Alderfer, M.A. Psychosocial screening for siblings of children with cancer: Barriers and preferences. Clin. Pract. Pediatric Psychol. 2017, 5, 364–375. [Google Scholar] [CrossRef]
- Jammu, A.S.; Chasen, M.R.; Lofters, A.K.; Bhargava, R. Systematic rapid living review of the impact of the COVID-19 pandemic on cancer survivors: Update to August 27, 2020. Supportive Care Cancer 2021, 29, 2841–2850. [Google Scholar] [CrossRef]
- Williams, L.R.; Anthony, E.K. A Model of Positive Family and Peer Relationships on Adolescent Functioning. J. Child Fam. Stud. 2015, 24, 658–667. [Google Scholar] [CrossRef]
- Gray, S.; Romaniuk, H.; Daraganova, G. Adoleacent’s Relationships with their peers. In LSAC Annual Statistical Report 2017; Austrailian Institute of Family Studies: Melbourne, Australia, 2018; pp. 47–58. [Google Scholar]
- Kazak, A.E. Comprehensive Care for Children With Cancer and Their Families: A Social Ecological Framework Guiding Research, Practice, and Policy. Child. Serv. 2001, 4, 217–233. [Google Scholar] [CrossRef]
- Lewandowska, A. Influence of a Child’s Cancer on the Functioning of Their Family. Children 2021, 8, 592. [Google Scholar] [CrossRef]
- Kazak, A.E.; Hwang, W.-T.; Chen, F.F.; Askins, M.A.; Carlson, O.; Argueta-Ortiz, F.; Barakat, L.P. Screening for Family Psychosocial Risk in Pediatric Cancer: Validation of the Psychosocial Assessment Tool (PAT) Version 3. J. Pediatric Psychol. 2018, 43, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Kazak, A.E.; Simms, S.; Rourke, M.T. Family Systems Practice in Pediatric Psychology. J. Pediatric Psychol. 2002, 27, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, K.; Simon, S.R. Feeling heard: A support group for siblings of children with developmental disabilities. Soc. Work Groups 2011, 34, 320–329. [Google Scholar] [CrossRef]
- Knecht, C.; Hellmers, C.; Metzing, S. The perspective of siblings of children with chronic illness: A literature review. J. Pediatric Nurs. 2015, 30, 102–116. [Google Scholar] [CrossRef]
- Council of Economic Advisers. 15 Economic Facts about Millennials; Council of Economic Advisors, Executive Office of the President: Washington, DC, USA, 2014. [Google Scholar]
- Rosenberg-Yunger, Z.R.S.; Granek, L.; Sung, L.; Klaassen, R.; Dix, D.; Cairney, J.; Klassen, A.F. Single-Parent Caregivers of Children with Cancer: Factors Assisting with Caregiving Strains. J. Pediatric Oncol. Nurs. 2013, 30, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, A.R.; Cardona, N.D.; Davis, K.A.; Pariseau, E.M.; Berk, D.; Muriel, A.C.; Long, K.A. Parent decision-making about support for siblings of children with cancer: Sociodemographic influences. Clin. Pract. Pediatric Psychol. 2020, 8, 115. [Google Scholar] [CrossRef]
| Range | Mean (SD) | N | (%) | |
|---|---|---|---|---|
| Age | 12–17 | 14.2 (1.6) | ||
| Gender | Female | 12 | 50 | |
| Male | 12 | 50 | ||
| Race | Asian | 1 | 4.2 | |
| Black | 3 | 12.5 | ||
| White | 20 | 83.3 | ||
| Ethnicity | Hispanic or Latinx | 6 | 25 | |
| Family Situation | Traditional | 21 | 87.5 | |
| Blended | 3 | 12.5 | ||
| Family Income 1 | Less than 500,000 | 6 | 25 | |
| 50,000–99,000 | 3 | 12.5 | ||
| 150,000–199,999 | 7 | 29.2 | ||
| 200,000–249,999 | 3 | 12.5 | ||
| 250,000–299,999 | 2 | 8.3 | ||
| More than 300,000 | 1 | 4.2 | ||
| Time since | 0–3 months | 2 | 8.3 | |
| Diagnosis | 3–6 months | 5 | 20.8 | |
| 6–12 months | 5 | 20.8 | ||
| 12–18 months | 3 | 12.5 | ||
| 18–24 months | 4 | 16.7 | ||
| Over 2 years | 5 | 20.8 | ||
| Diagnosis | Leukemia | 11 | 45.8 | |
| Lymphoma | 6 | 25 | ||
| Sarcoma | 4 | 16.7 | ||
| Solid Organ | 2 | 8.3 | ||
| Brain | 1 | 4.2 | ||
| Parent Education | Some College | 5 | 20.8 | |
| Vocational or Specialized Training | 3 | 12.5 | ||
| Bachelor’s Degree | 11 | 45.8 | ||
| Master’s Degree | 4 | 16.7 | ||
| Doctoral Degree | 1 | 4.2 | ||
| Social Support | Codebook Definition | Example Quote |
|---|---|---|
| Emotional | Receive empathy, caring, reassurance, or encouragement. Knowing you have someone available who cares about you. | “She would ask questions about my feelings and stuff. Because, as a sibling,—it feels bad to think that you’re going through something, rather than your sibling’s going through something. So, like it was easy to talk to her.” (16 y/F, talking about a cousin) |
| Informational | Receiving knowledge, recommendations, or advice. | “He was kind of like—it’s going to be okay. He was the one—more than my mom, he was the one who kind of gave me the info on his cancer and he kind of like informed me what was going on and he did it in a nice way and everything.” (15 y/F, talking about her dad) |
| Instrumental | Receipt of services such as transportation, money, or help with household chores, homework, and skill building. | “She helped me by cooking for me and providing me meals.” (13 y/M, talking about his grandmother) “yeah, and still helping me with homework even though he’s busy.” (12 y/M, talking about his dad) |
| Companionship | Spending time together for distraction an escape from cancer, offers reprieve and fun. | “I would say that he just like—he’s so tiny that he doesn’t really understand it fully yet. So, he just helps me just get my mind off of it and just like “Hey, [brother], you want to play Legos or something?” I’m like “Okay, sure.” (14 y/M, talking about younger sibling) |
| Validation | A sense of belonging and shared world view, having someone who understands you. | “She understands, and she needs people to talk to just as much as I do” (12 y/F, talking about a sibling) “He has a relative, I think, who had cancer, and it’s a different kind of cancer, of course, but he tells me all the time that he knows how hard it is, and he’s there to help.” (16 y/F, talking about a friend) |
| Appraisal | The provision of affirmation, or feedback for self-evaluation and social comparison. | “[brother w CA] was telling me about how for the past two years he was depressed because he was in and out of hospitals. He couldn’t get to see us, and that really inspired me to try my best for him.” (16 y/M talking about his older brother) “I was giving a speech to my prayer center, my mosque. And it went pretty well, and my dad gave me some feedback and told me how I could improve, what I did well, and he did it all in a very nice, friendly way.” (14 y/M talking about his dad) |
| Indirect | Supports siblings report has helpful to them but are not directed at them specifically. | “People in my ward, they would bring us dinner,—they mowed our lawn, and they are constantly visiting us, trying to help with anything…it helps me feel like people care, and we have help if we need it, and that’s comforting.” (16 y/F talking about her neighbors) |
| Social Support | Gender | |
|---|---|---|
| Male | Female | |
| Emotional | 61 | 83 |
| Informational | 20 | 30 |
| Instrumental | 24 | 29 |
| Companionship | 30 | 50 |
| Validation | 7 | 25 |
| Appraisal | 12 | 3 |
| Indirect | 4 | 5 |
| Hardest Things Since CA Dx | Overarching Themes | Most Helpful Supports |
|---|---|---|
| “When [brother w CA] is not feeling good, or when he starts feeling sick, during the chemo, or he’s weak, and he’s crying, like that’s the hardest thing, because I don’t like to see him in pain.” (P22) “Probably mostly just feeling bad for him, like just all the hard things that he’s had to go through.” (P19) “Just accepting that things won’t be the same for [sister w CA]…she is super tired and we can’t joke around and she is getting super serious.” (P14) “I think that’s the hardest thing is just seeing my mom not take care of herself, and I think the hardest thing is just thinking into the future.” (P1) | Involvement in Care and Family | “I try to like comfort him. Because usually, when he’s like feeling like that, he’ll ask for me. I’ll come and just lay with him, watch a movie with him, and just try to comfort him as best as I can.” (P22) “I think the thing that has helped me the most is that [my siblings] understand that like she’s sick and stuff, and they’ll help me make cards for her and things.” (P11) “Just hanging out with [sister w CA] more maybe.” (P14) |
| “A lot of the time my dad would be working and mom would take him to the hospital, so I’ll be by myself.” (P15) “I think probably feeling more alone because I was probably closer with my parents before my brother got diagnosed and obviously, my brother was in the hospital like a bunch of different times.” (P11) “I would say probably the attention, like less attention.” (P6) | Creating Connection and Presence | “When everybody’s together.” (P24) “[Aunt], she is just be there for us, to check up on us when we were down, and she was just there.” (P22) “Well, it’s always nice to like see people—see that people care and want to help you.” (P19) “Probably just them being open to talk, being like “Hey, if you want to hang-out we can hang-out.” (P15) |
| “Selfishly, the hardest thing has been just my mental health getting really bad since then. It kind of just downward spiraled since he was diagnosed.” (P5) “Pretty much not being able to see people a lot and go places.” (P12) “Losing friends” (P21) “Dad would be working, and my mom will have to take [brother w CA] to the hospital, and so I’ll be by myself for a few weeks just at the house.” (P15) | Distraction | “I’d just say like going to practice gets my mind off it, like my dad taking me to practice. I don’t really think about it while I’m there.” (P23) “I really like hanging out with my cousins and with some of my friends online.” (P16) “You know, I could still do my music lessons…my theater classes. I had people to drive me to those. And I could do a show or something, because of that support that I had. Kept me feeling like, “Okay, my life is still going to go on. This just happened to my brother, but I can still live my life and do my things.” (P5) |
| “When by brother first got diagnosed they were open to me asking questions…but I guess they got tired of it” (P21) “When I didn’t know anything about it, I wasn’t sure if he was going to be okay.” (P17) “Well, I feel like if someone finds out that [my sister] has cancer, they’ll be like, “Oh, I’m so sorry”, and like feel all awkward if I tell them that like, “It’s really not a big deal”, and so I feel like that’s hard and I never really understood it all the way.” (P11) The hardest thing has probably been schoolwork … a result of distractions and stuff like that. You just don’t know what’s going to happen next, your mind is in a million different places. (P4) | Understanding | “I think the most helpful was knowing what was going on with my brother. I appreciate my mom the most for telling me straight-up what was going on with my brother. I felt like that kept me grounded the most.” (P21) “I don’t know, [my parents] gave me time and space and just like processing room. So, I feel like homework, I could have an extended amount of time or something or like with like different things, they’d be like “Oh, yeah, I understand.” (P10) “Probably just like having a few people that understand.” (P13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wawrzynski, S.E.; Alderfer, M.A.; Kvistad, W.; Linder, L.; Reblin, M.; Guo, J.-W.; Cloyes, K.G. The Social Networks and Social Support of Siblings of Children with Cancer. Children 2022, 9, 113. https://doi.org/10.3390/children9010113
Wawrzynski SE, Alderfer MA, Kvistad W, Linder L, Reblin M, Guo J-W, Cloyes KG. The Social Networks and Social Support of Siblings of Children with Cancer. Children. 2022; 9(1):113. https://doi.org/10.3390/children9010113
Chicago/Turabian StyleWawrzynski, Sarah E., Melissa A. Alderfer, Whitney Kvistad, Lauri Linder, Maija Reblin, Jia-Wen Guo, and Kristin G. Cloyes. 2022. "The Social Networks and Social Support of Siblings of Children with Cancer" Children 9, no. 1: 113. https://doi.org/10.3390/children9010113
APA StyleWawrzynski, S. E., Alderfer, M. A., Kvistad, W., Linder, L., Reblin, M., Guo, J.-W., & Cloyes, K. G. (2022). The Social Networks and Social Support of Siblings of Children with Cancer. Children, 9(1), 113. https://doi.org/10.3390/children9010113