
Trauma in Children during Lockdown for SARS-CoV-2 Pandemic. A Brief Report

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
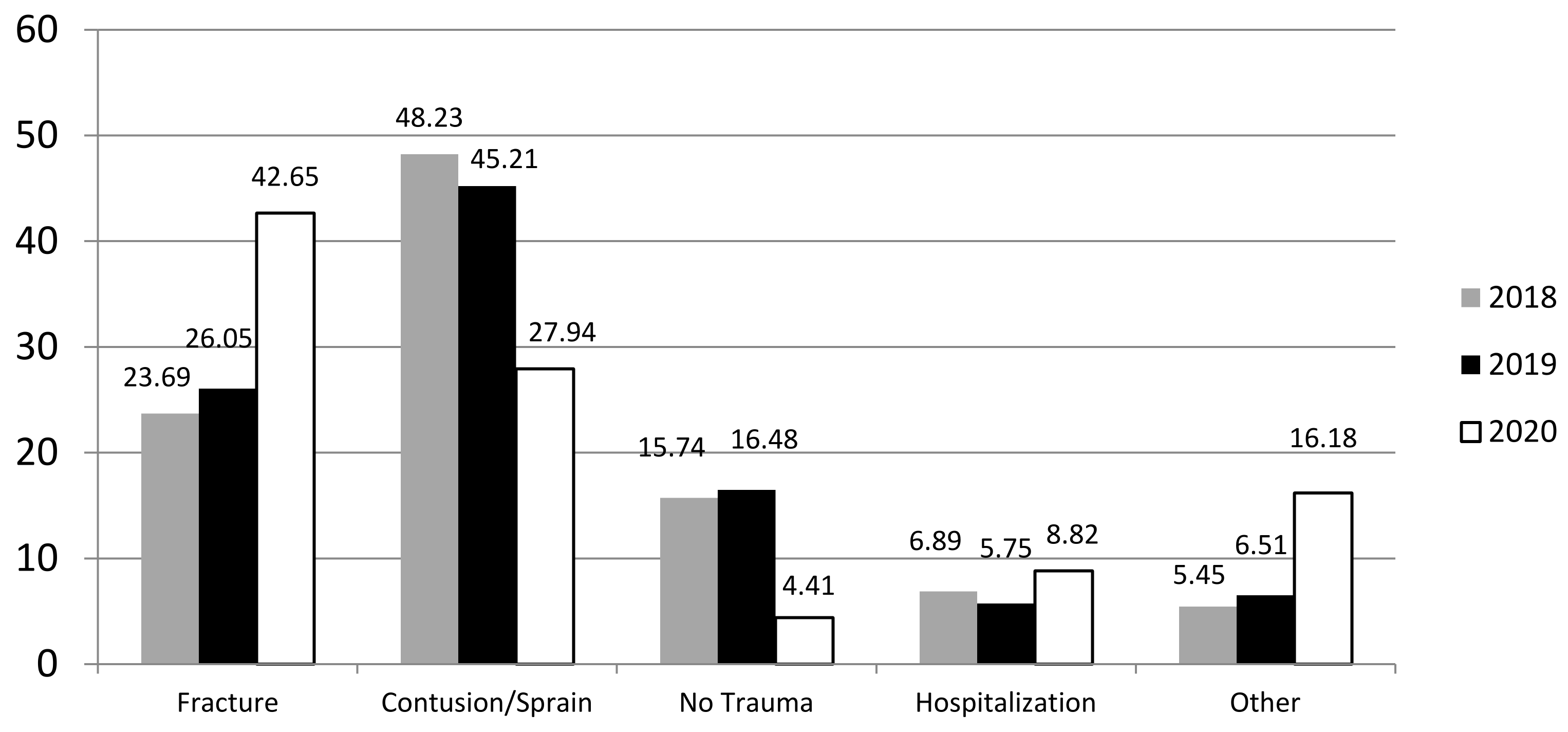
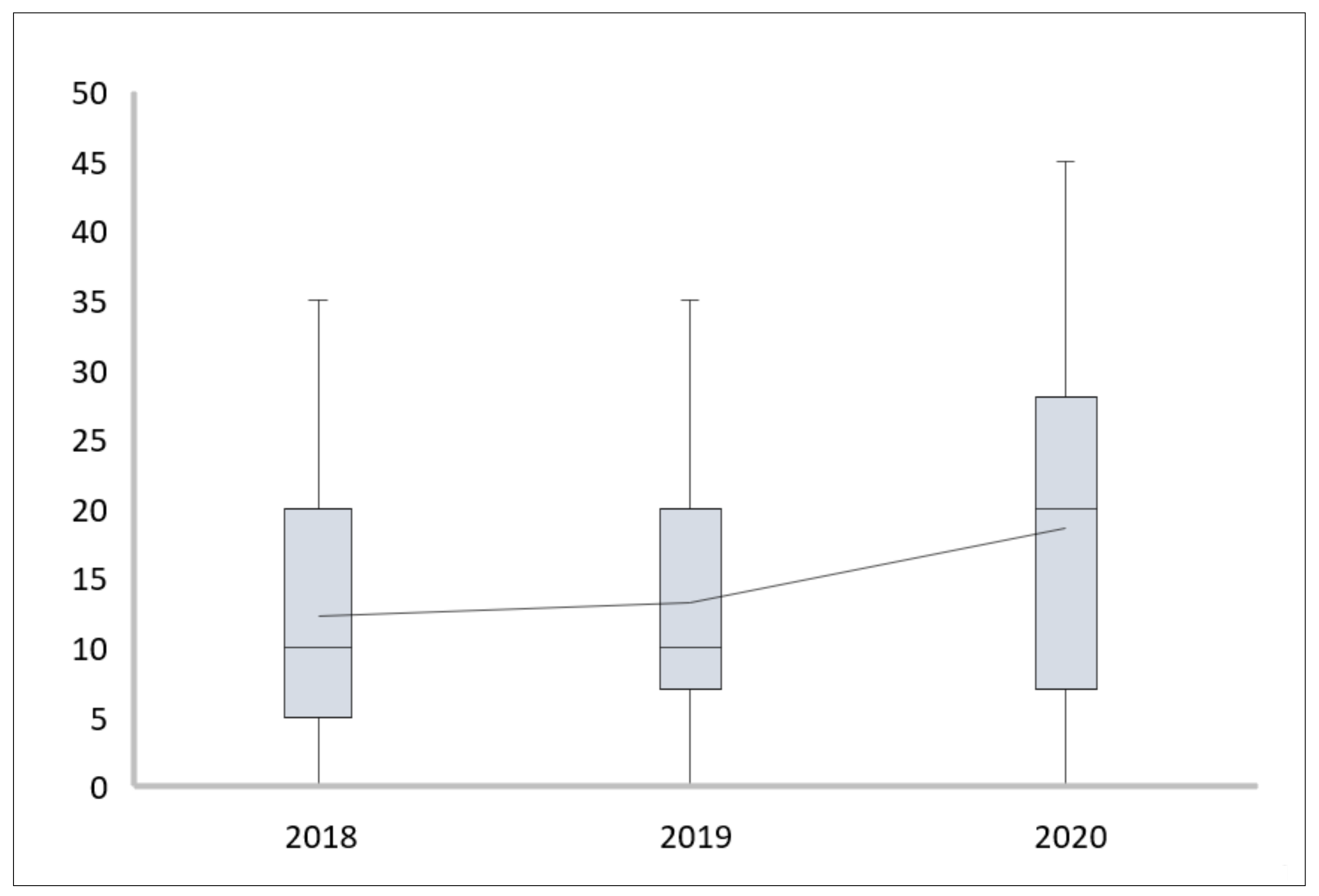
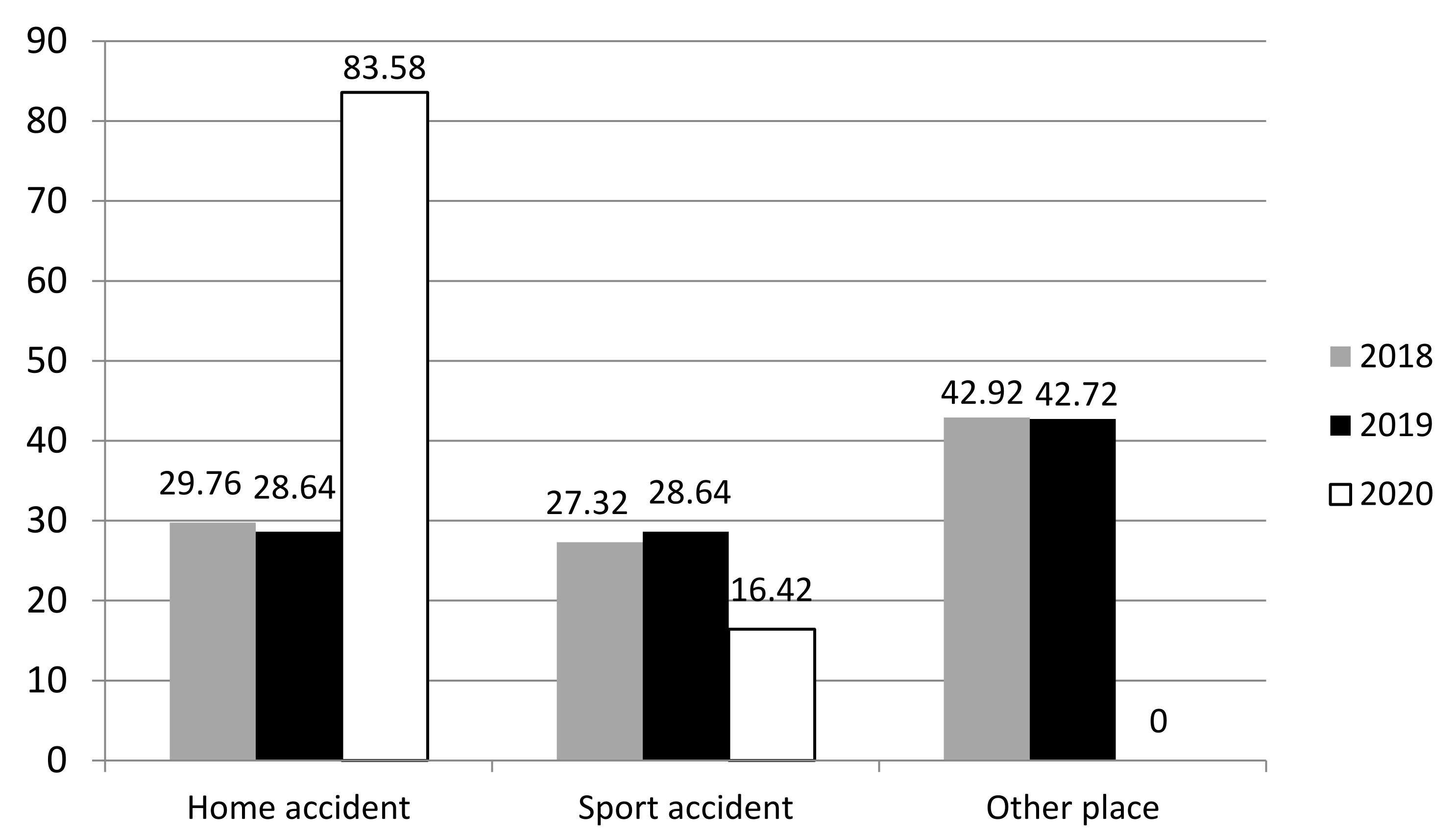
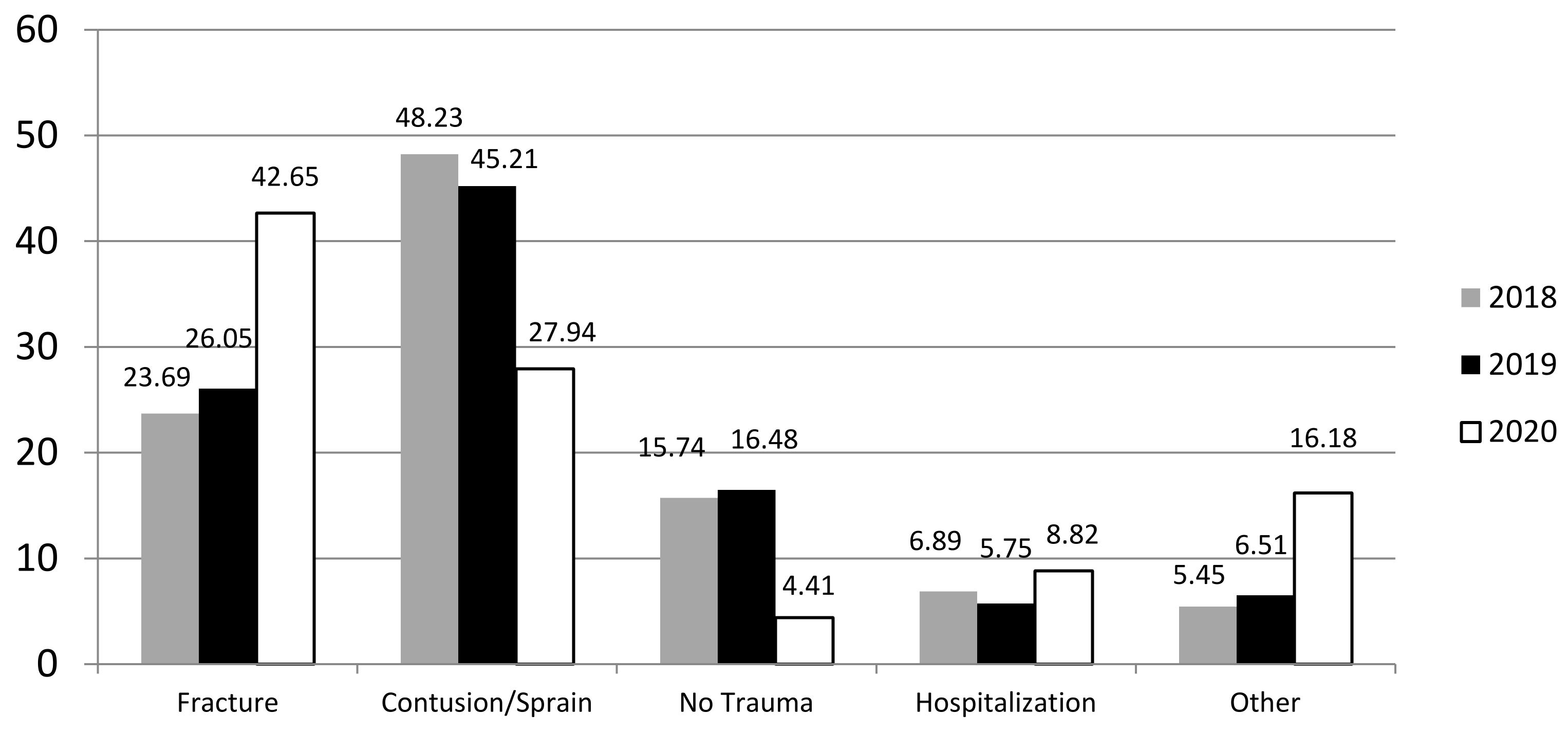
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mamoowala, N.; Johnson, N.A.; Dias, J.J. Trends in paediatric distal radius fractures: An eight-year review from a large UK trauma unit. Ann. R. Coll. Surg. Engl. 2019, 101, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Segal, D.; Slevin, O.; Aliev, E.; Borisov, O.; Khateeb, B.; Faour, A.; Palmanovich, E.; Brin, Y.S.; Weigl, D. Trends in the seasonal variation of paediatric fractures. J. Child. Orthop. 2018, 12, 614–621. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: Rolling Update on Coronavirus Disease (COVID 19). 2020. Available online: https://www.who.int/emergencies/diseass/novel-coronavirus2019/events-as-they-happen (accessed on 18 May 2021).
- Prime Minister’s Decree of 11 March 2020 “Iorestoacasa/Istayathome” (20A01558) (GU n.62 del 9-3-2020). Available online: https://www.gazzettaufficiale.it/gazzetta/serie_generale/caricaDettaglio?dataPubblicazioneGazzetta=2020-03-09&numeroGazzetta=62 (accessed on 18 May 2021).
- Chamberlain, J.M.; Patel, K.M.; Pollack, M.M.; Brayer, A.; Macias, C.G.; Okada, P.; Schunk, J. Recalibration of the pediatric risk of admission score using a multi-institutional sample. Ann. Emerg. Med. 2004, 43, 461. [Google Scholar] [CrossRef]
- Khosla, S.; Melton, L.J.; Dekutoski, M.B.; Achenbach, S.J.; Oberg, A.L.; Riggs, B.L. Incidence of childhood distal forearm fractures over 30 years: A population-based study. JAMA 2003, 290, 1479. [Google Scholar] [CrossRef] [Green Version]
- Jones, I.E.; Williams, S.M.; Dow, N.; Goulding, A. How many children remain fracture-free during growth? A longitudinal study of children and adolescents participating in the Dunedin Multidisciplinary Health and Development Study. Osteoporos. Int. 2002, 13, 990. [Google Scholar] [CrossRef] [PubMed]
- Price, C.T.; Flynn, J.M. Management of fractures. In Lovell and Winter’s Pediatric Orthopaedics, 6th ed.; Morrissey, R.T., Weinstein, S.L., Eds.; Lippincott: Philadelphia, PA, USA, 2006; p. 1463. [Google Scholar]
- Rodríguez-Merchán, E.C. Pediatric fractures of the forearm. Clin. Orthop. Relat. Res. 2005, 432, 65–72. [Google Scholar] [CrossRef]
- Jones, I.E.; Cannan, R.; Goulding, A. Distal forearm fractures in New Zealand children: Annual rates in a geographically defined area. N. Zeal. Med. J. 2000, 113, 443. [Google Scholar]
- Pizzutillo, P.D. Pediatric orthopaedics. In Essentials of Musculoskeletal Care, 3rd ed.; Griffin, Y.L., Ed.; American Academy of Orthopaedic Surgeons: Rosemont, IL, USA, 2005; p. 863. [Google Scholar]
- Abraham, A.; Handoll, H.H.; Khan, T. Interventions for treating wrist fractures in children. Cochrane Database Syst. Rev. 2008, 12, CD004576. [Google Scholar]
- Testa, G.; Sapienza, M.; Rabuazzo, F.; Culmone, A.; Valenti, F.; Vescio, A.; Pavone, V. Comparative study between admission, orthopaedic surgery, and economic trends during Covid-19 and non-Covid-19 pandemic in an Italian tertiary hospital: A retrospective review. J. Orthop. Surg. Res. 2021, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Christey, G.; Amey, J.; Campbell, A.; Smith, A. Variation in volumes and characteristics of trauma patients admitted to a level one trauma centre during national level 4 lockdown for COVID-19 in New Zeland. N. Zeal. Med. J. 2020, 133, 81–88. [Google Scholar]
- Hernigou, J.; Morel, X.; Callewier, A.; Bath, O.; Hernigou, P. Staying home during “Covid-19” decreased fractures, but trauma did not quarantine in one hundred and twelve adultes and twenty eight children and the “tsunami of recommendations” could not lockdown twelve elective operations. Int. Orthop. 2020, 44, 1473–1480. [Google Scholar] [CrossRef]
- Clementsen, S.; Randsborg, P.H. School related fractures. Tidsskr. Nor. Laegeforen 2014, 134, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Del Papa, J.; Vittorini, P.; D’Aloisio, F.; Muselli, M.; Giuliani, A.R.; Mascitelli, A.; Fabiani, L. Retrospective Analysis of Injuries and Hospitalizations of Pazients Followig the 2009 Earthquake of L’Aquila City. Int. J. Environ. Res. Public Health 2019, 16, 1675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabian, M.H.; Vosoughi, F.; Najafi, F.; Khabiri, S.S.; Nafisi, M.; Veisi, J.; Rastgou, V.; Ghamari, S.; Aakhashi, A.; Bahrami, N.; et al. Epidemiological pattern of pediatric trauma in COVID-19 outbreak: Data from a tertiary trauma center in Iran. Injury 2020, 51, 2811–2815. [Google Scholar] [CrossRef] [PubMed]
- Bram, J.T.; Johnson, M.A.; Magee, L.C.; Mehta, N.N.; Fazal, F.Z.; Baldwin, K.D.; Riley, J.; Shah, A.S. Where have all the fractures gone? The epidemiology of pediatric fractures during the COVID-19 Pandemic. J. Pediatr. Orthop. 2020, 40, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Dolci, A.; Marongiu, G.; Leinardi, L.; Lombardo, M.; Dessì, G.; Capone, A. The epidemiology of fractures and muskulo-skeletal traumas during COVID-19 lockdown: A detailed survey of 17.591 patients in a wide Italian metropolitan area. Geriatr. Orthop. Surg. Rehabil. 2020, 11, 2151459320972673. [Google Scholar] [CrossRef] [PubMed]
- Rajput, K.; Sud, A.; Rees, M.; Rutka, O. Epidemiology of trauma presentations to a major trauma centre in the North West of England during the COVID-19 level 4 lockdown. Eur. J. Trauma Emerg. Surg. 2021, 47, 631–636. [Google Scholar] [CrossRef]
- Chiba, H.; Lewis, M.; Benjamin, E.R.; Jakob, D.A.; Liasidis, P.; Wong, M.D.; Navarrete, S.; Carreon, R.; Demetriades, D. “Safer at home”: The effect of the COVID-19 lockdown on epidemiology, resource utilization, and outcomes at a large urban trauma center. J. Trauma Acute Care Surg. 2021, 90, 708. [Google Scholar] [CrossRef] [PubMed]
- Neal, E. Comparison of splinting and casting in the management of torus fracture. Emerg. Nurse 2014, 21, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.A.; Alvarado, C.A.; Montoya-Williams, D.C.; Matthias, R.C.; Blakemore, L.C. Buckling down on torus fractures: Has evolving evidence affected practice? J. Child. Orthop. 2018, 12, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Manno, E.; Pesce, M.; Stralla, U.; Festa, F.; Geninatti, S.; Balzarro, M.F.; Di Leo, D.; Gelain, B. Specialized fast track: A sustainable model to improve emergency department patient flow. J. Hosp. Adm. 2015, 4, 40. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dibello, D.; Salvemini, M.; Amati, C.; Colella, A.; Graziano, G.; Vicenti, G.; Moretti, B.; Pederiva, F. Trauma in Children during Lockdown for SARS-CoV-2 Pandemic. A Brief Report. Children 2021, 8, 1131. https://doi.org/10.3390/children8121131
Dibello D, Salvemini M, Amati C, Colella A, Graziano G, Vicenti G, Moretti B, Pederiva F. Trauma in Children during Lockdown for SARS-CoV-2 Pandemic. A Brief Report. Children. 2021; 8(12):1131. https://doi.org/10.3390/children8121131
Chicago/Turabian StyleDibello, Daniela, Marcella Salvemini, Carlo Amati, Antonio Colella, Giusi Graziano, Giovanni Vicenti, Biagio Moretti, and Federica Pederiva. 2021. "Trauma in Children during Lockdown for SARS-CoV-2 Pandemic. A Brief Report" Children 8, no. 12: 1131. https://doi.org/10.3390/children8121131
APA StyleDibello, D., Salvemini, M., Amati, C., Colella, A., Graziano, G., Vicenti, G., Moretti, B., & Pederiva, F. (2021). Trauma in Children during Lockdown for SARS-CoV-2 Pandemic. A Brief Report. Children, 8(12), 1131. https://doi.org/10.3390/children8121131