
Effectiveness of Custom-Made Foot Orthoses vs. Heel-Lifts in Children with Calcaneal Apophysitis (Sever’s Disease): A CONSORT-Compliant Randomized Trial

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Interventions
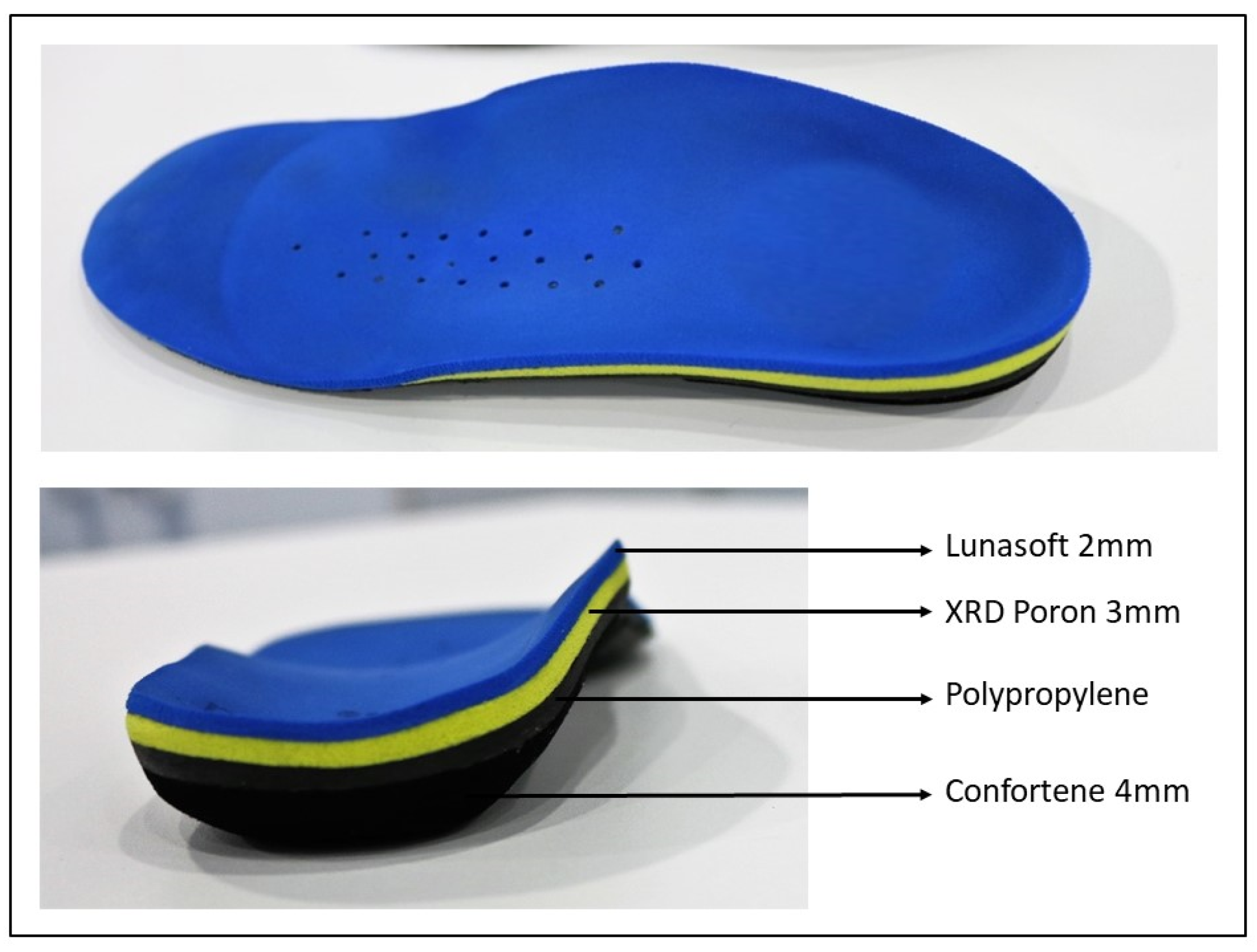
2.2.1. Treatment A Group (TA)
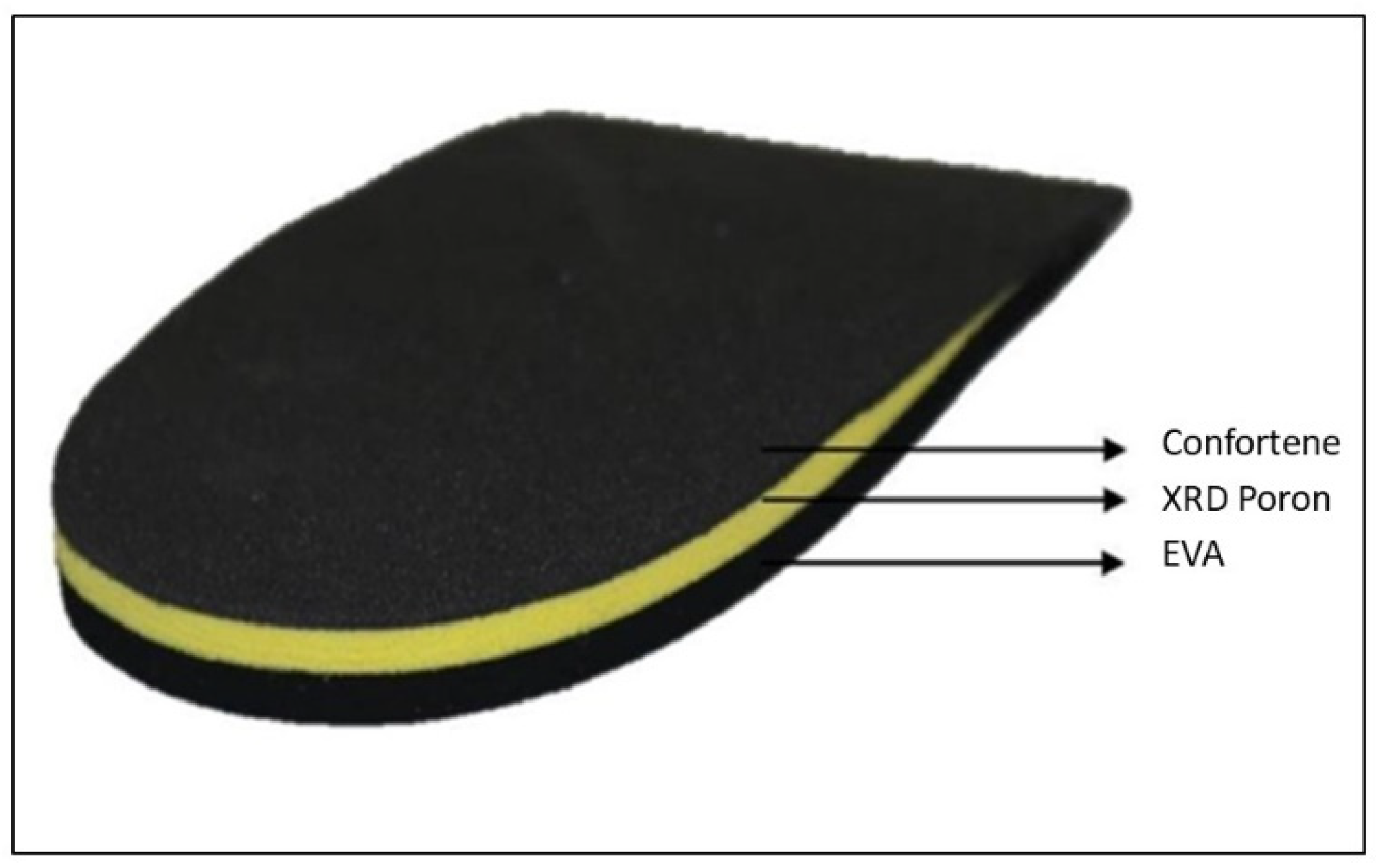
2.2.2. Treatment B Group (TB)
2.3. Outcome Measures
2.4. Data Analysis
3. Results
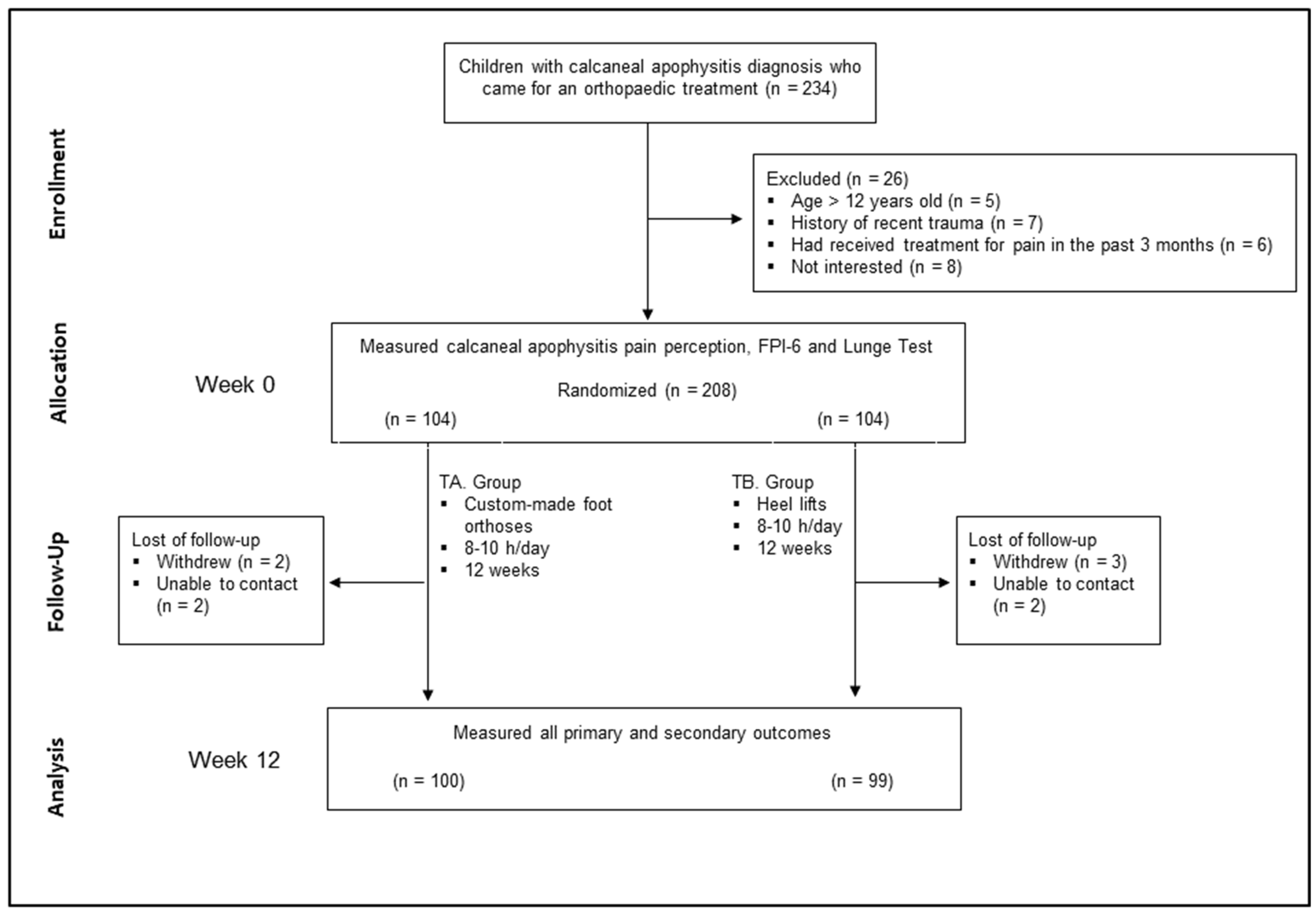
3.1. Enrollment and Characteristics of the Participants
3.2. Compliance with Study Protocol
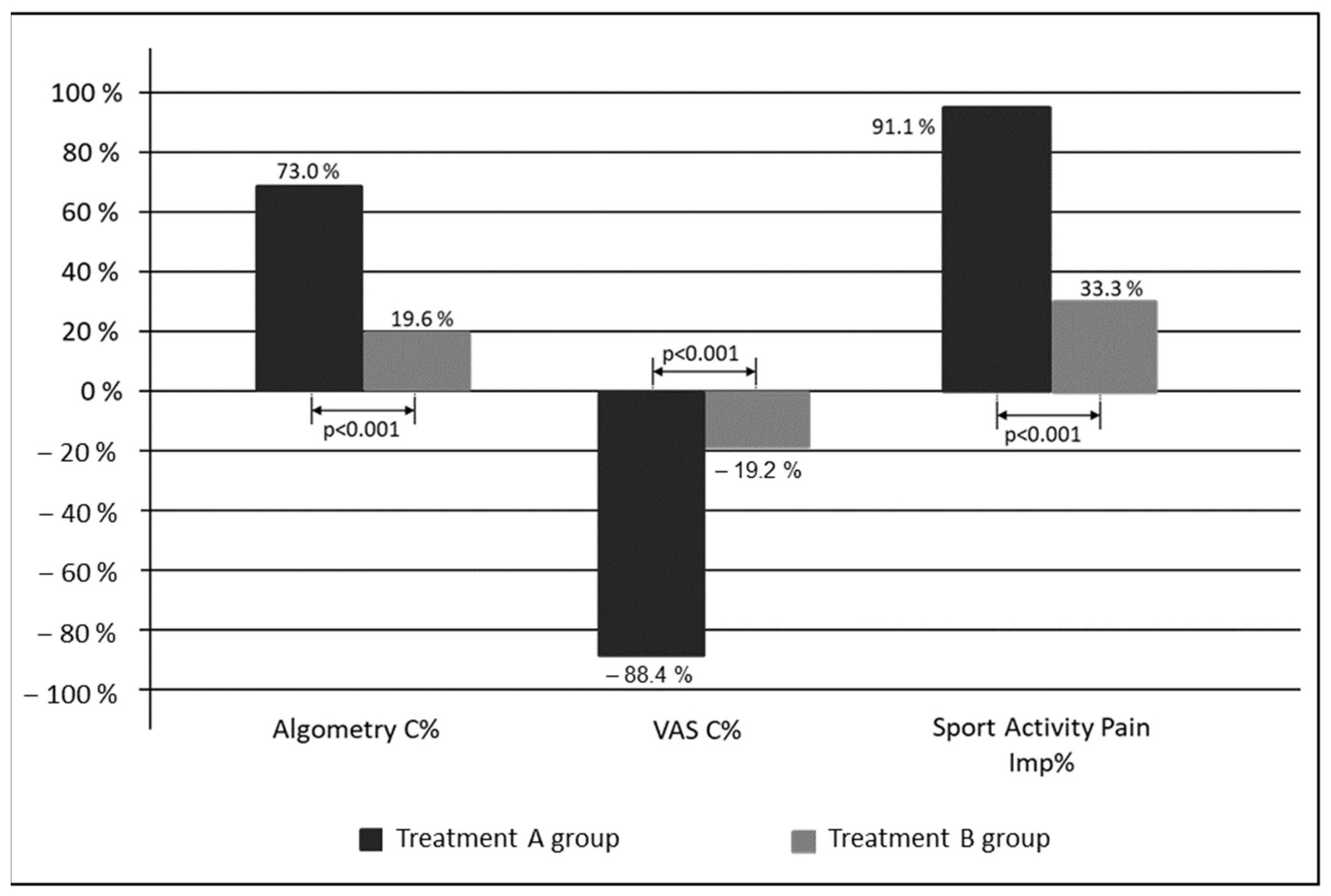
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Madden, C.C.; Mellion, M.B. Sever’s disease and other causes of heel pain in adolescents. Am. Fam. Physician 1996, 54, 1995–2000. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8900359 (accessed on 4 April 2019).
- Santafé, J.A.; Gómez Bernal, A.; Santafé, J.-V.A.; Cerzócimo, C.L.; Galindo, V.-L.E.; Almenar, A.-J. Relación de Lunge y Jack Test en la apófisis calcánea (Talalgia de Sever) en futbolistas jóvenes. Rev. Int. Cienc. Podol. 2017, 11, 117–123. [Google Scholar] [CrossRef][Green Version]
- Tu, P. Heel Pain: Diagnosis and Management. Am. Fam. Physician 2018, 97, 86–93. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29365222 (accessed on 4 April 2019). [PubMed]
- Micheli, L.J.; Fehlandt, A.F. Overuse injuries to tendons and apophyses in children and adolescents. Clin. Sports Med. 1992, 11, 713–726. Available online: http://www.ncbi.nlm.nih.gov/pubmed/1423694 (accessed on 4 April 2019). [CrossRef]
- Hendrix, C.L. Calcaneal apophysitis (Sever´s disease). Clin. Podiatr. Med. Surg. 2005, 22, 55–62. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0891842204000783 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Pascual Huerta, J. The effect of the gastrocnemius on the plantar fascia. Foot Ankle Clin. 2014, 19, 701–718. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1083751514001004 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Anderson, J.G.; Bohay, D.R.; Eller, E.B.; Witt, B.L. Gastrocnemius recession. Foot Ankle Clin. 2014, 19, 767–786. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1083751514001028 (accessed on 4 April 2019). [CrossRef]
- Perhamre, S.; Lundin, F.; Norlin, R.; Klässbo, M. Sever’s injury; treat it with a heel cup: A randomized, crossover study with two insole alternatives. Scand. J. Med. Sci. Sports 2011, 21, e42–e47. Available online: http://doi.wiley.com/10.1111/j.1600-0838.2010.01140.x (accessed on 4 April 2019). [CrossRef] [PubMed]
- Perhamre, S.; Janson, S.; Norlin, R.; Klässbo, M. Sever’s injury: Treatment with insoles provides effective pain relief. Scand. J. Med. Sci. Sports 2011, 21, 819–823. Available online: http://doi.wiley.com/10.1111/j.1600-0838.2010.01051.x (accessed on 4 April 2019). [CrossRef]
- Wiegerinck, J.I.; Zwiers, R.; Sierevelt, I.N.; van Weert, H.C.P.M.; van Dijk, C.N.; Struijs, P.A.A. Treatment of Calcaneal Apophysitis: Wait and See Versus Orthotic Device Versus Physical Therapy: A Pragmatic Therapeutic Randomized Clinical Trial. J. Pediatr. Orthop. 2016, 36, 152–157. Available online: http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=01241398-201603000-00008 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Micheli, L.J.; Ireland, M.L. Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J. Pediatr. Orthop. 1987, 7, 34–38. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3793908 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Gijon-Nogueron, G.; Cortes-Jeronimo, E.; Cervera-Marin, J.A.; García-de-la-Peña, R.; Benhamu-Benhamu, S.; Luque-Suarez, A. Foot orthoses custom-made by vacuum forming on the non-load-bearing foot: Preliminary results in male children with calcaneal apophysitis (Sever’s disease). Prosthet. Orthot. Int. 2013, 37, 495–498. Available online: http://journals.sagepub.com/doi/10.1177/0309364613482844 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Reilly, J.J.; Jackson, D.M.; Montgomery, C.; Kelly, L.A.; Slater, C.; Grant, S.; Paton, J.Y. Total energy expenditure and physical activity in young Scottish children: Mixed longitudinal study. Lancet 2004, 363, 211–212. Available online: http://www.ncbi.nlm.nih.gov/pubmed/14738795 (accessed on 4 April 2019). [CrossRef]
- James, A.M.; Williams, C.M.; Haines, T.P. Effectiveness of footwear and foot orthoses for calcaneal apophysitis: A 12-month factorial randomised trial. Br. J. Sports Med. 2016, 50, 1268–1275. Available online: http://bjsm.bmj.com/lookup/doi/10.1136/bjsports-2015-094986 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Scharfbillig, R.W.; Jones, S.; Scutter, S.D. Sever’s disease: What does the literature really tell us? J. Am. Podiatr. Med. Assoc. 2008, 98, 212–223. Available online: http://www.ncbi.nlm.nih.gov/pubmed/18487595 (accessed on 4 April 2019). [CrossRef] [PubMed]
- James, A.M.; Williams, C.M.; Haines, T.P. Effectiveness of interventions in reducing pain and maintaining physical activity in children and adolescents with calcaneal apophysitis (Sever’s disease): A systematic review. J. Foot Ankle Res. 2013, 6, 16. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23641779 (accessed on 10 April 2019). [CrossRef]
- McKay, M.J.; Baldwin, J.N.; Ferreira, P.; Simic, M.; Vanicek, N.; Burns, J.; 1000 Norms Project Consortium. Normative reference values for strength and flexibility of 1,000 children and adults. Neurology 2017, 88, 36–43. [Google Scholar] [CrossRef] [PubMed]
- James, A.M.; Williams, C.M.; Luscombe, M.; Hunter, R.; Haines, T.P. Factors Associated with Pain Severity in Children with Calcaneal Apophysitis (Sever´s disease). J. Pediatr. 2015, 167, 455–459. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0022347615004370 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Jensen, M.P.; Chen, C.; Brugger, A.M. Interpretation of visual analog scale ratings and change scores: A reanalysis of two clinical trials of postoperative pain. J. Pain 2003, 4, 407–414. [Google Scholar] [CrossRef]
- Caravaggi, P.; Giangrande, A.; Lullini, G.; Padula, G.; Berti, L.; Leardini, A. In shoe pressure measurements during different motor tasks while wearing safety shoes: The effect of custom made insoles vs. prefabricated and off-the-shelf. Gait Posture 2016, 50, 232–238. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27662483 (accessed on 26 June 2019). [CrossRef]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. Available online: http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00006396-201110000-00031 (accessed on 4 April 2019). [CrossRef]
- Aun, C.; Lam, Y.M.; Collett, B. Evaluation of the use of visual analogue scale in Chinese patients. Pain 1986, 25, 215–221. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3725409 (accessed on 4 April 2019). [CrossRef]
- Graven-Nielsen, T.; Vaegter, H.B.; Finocchietti, S.; Handberg, G.; Arendt-Nielsen, L. Assessment of musculoskeletal pain sensitivity and temporal summation by cuff pressure algometry: A reliability study. Pain 2015, 156, 2193–2202. Available online: http://insights.ovid.com/crossref?an=00006396-201511000-00013 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Chesterton, L.S.; Sim, J.; Wright, C.C.; Foster, N.E. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters. Clin. J. Pain 2007, 23, 760–766. Available online: https://pubmed.ncbi.nlm.nih.gov/18075402/ (accessed on 27 January 2021). [CrossRef] [PubMed]
- Redmond, A.C.; Crosbie, J.; Ouvrier, R.A. Development and validation of a novel rating system for scoring standing foot posture: The Foot Posture Index. Clin. Biomech. 2006, 21, 89–98. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0268003305001804 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Hawke, F.; Rome, K.; Evans, A.M. The relationship between foot posture, body mass, age and ankle, lower-limb and whole-body flexibility in healthy children aged 7 to 15 years. J. Foot Ankle Res. 2016, 9, 14. Available online: http://jfootankleres.biomedcentral.com/articles/10.1186/s13047-016-0144-7 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Evans, A.M.; Rome, K.; Peet, L. The foot posture index, ankle lunge test, Beighton scale and the lower limb assessment score in healthy children: A reliability study. J. Foot Ankle Res. 2012, 5, 1. Available online: https://jfootankleres.biomedcentral.com/articles/10.1186/1757-1146-5-1 (accessed on 4 April 2019). [CrossRef]
- Landorf, K.; Keenan, A.M.; Rushworth, R.L. Foot orthosis prescription habits of Australian and New Zealand podiatric physicians. J. Am. Podiatr. Med. Assoc. 2001, 91, 174–183. Available online: http://www.ncbi.nlm.nih.gov/pubmed/11319247 (accessed on 4 April 2019). [CrossRef]
- Martínez-Nova, A.; Gijón-Noguerón, G.; Alfageme-García, P.; Montes-Alguacil, J.; Evans, A.M. Foot posture development in children aged 5 to11 years: A three-year prospective study. Gait Posture 2018, 62, 280–284. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0966636218302558 (accessed on 4 April 2019). [CrossRef] [PubMed]
- Gijon-Nogueron, G.; Montes-Alguacil, J.; Alfageme-Garcia, P.; Cervera-Marin, J.A.; Morales-Asencio, J.M.; Martinez-Nova, A. Establishing normative foot posture index values for the paediatric population: A cross-sectional study. J. Foot Ankle Res. 2016, 9, 24. Available online: http://jfootankleres.biomedcentral.com/articles/10.1186/s13047-016-0156-3 (accessed on 4 April 2019). [CrossRef]
- Evans, A.M.; Karimi, L. The relationship between paediatric foot posture and body mass index: Do heavier children really have flatter feet? J. Foot Ankle Res. 2015, 8, 46. Available online: http://jfootankleres.biomedcentral.com/articles/10.1186/s13047-015-0101-x (accessed on 4 April 2019). [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | TA (n = 104) | TB (n = 104) | ICC | p Value |
|---|---|---|---|---|
| Age (years.month) | 11.1 ± 1.0 | 11.3 ± 1.0 | 0.133 1 | |
| Male [n (%)] | 85 (82.2) | 88 (84.4) | 0.842 2 | |
| BMI (kg/m2) | 19.2 ± 2.3 | 19.4 ± 2.4 | 0.677 1 | |
| FPI-6 right | 8.3 ± 1.7 | 8.2 ± 1.7 | 0.477 3 | |
| FPI-6 left | 8.3 ± 1.7 | 8.2 ± 1.7 | 0.580 3 | |
| Lunge right (degrees) | 32.3 ± 3.5 | 32.1 ± 3.7 | 0.761 3 | |
| Lunge left (degrees) | 32.4 ± 3.5 | 32.0 ± 3.7 | 0.447 3 | |
| VAS (mm) | 80.1 ± 13.1 | 81.3 ± 13.2 | 0.559 3 | |
| Algometry (kgf) | 2.9 ± 0.4 | 2.7 ± 0.4 | 0.91 [0.88–0.94] | 0.026 3 |
| Outcome | Groups | β | Odds Ratio (95% CI) * | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| TA (n = 100) | TB (n = 99) | |||||||||
| Final | C % | Imp% | p-value | Final | C% | Imp% | p-value | |||
| VAS (mm) | 11.6 ± 17.4 | −88.4 ± 18.5 | <0.001 1 | 67.3 ± 21.2 | −19.2 ± 22.2 | <0.001 1 | −68.6 | (−74.5 to −62.7) | ||
| Algometry (kgf) | 4.9 ± 0.5 | 73.0 ± 23.6 | <0.001 1 | 3.3 ± 0.7 | 19.6 ± 18.7 | <0.001 1 | 53.4 | (47.1 to 59.7) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfaro-Santafé, J.; Gómez-Bernal, A.; Lanuza-Cerzócimo, C.; Alfaro-Santafé, J.-V.; Pérez-Morcillo, A.; Almenar-Arasanz, A.-J. Effectiveness of Custom-Made Foot Orthoses vs. Heel-Lifts in Children with Calcaneal Apophysitis (Sever’s Disease): A CONSORT-Compliant Randomized Trial. Children 2021, 8, 963. https://doi.org/10.3390/children8110963
Alfaro-Santafé J, Gómez-Bernal A, Lanuza-Cerzócimo C, Alfaro-Santafé J-V, Pérez-Morcillo A, Almenar-Arasanz A-J. Effectiveness of Custom-Made Foot Orthoses vs. Heel-Lifts in Children with Calcaneal Apophysitis (Sever’s Disease): A CONSORT-Compliant Randomized Trial. Children. 2021; 8(11):963. https://doi.org/10.3390/children8110963
Chicago/Turabian StyleAlfaro-Santafé, Javier, Antonio Gómez-Bernal, Carla Lanuza-Cerzócimo, José-Víctor Alfaro-Santafé, Aitor Pérez-Morcillo, and Alejandro-Jesús Almenar-Arasanz. 2021. "Effectiveness of Custom-Made Foot Orthoses vs. Heel-Lifts in Children with Calcaneal Apophysitis (Sever’s Disease): A CONSORT-Compliant Randomized Trial" Children 8, no. 11: 963. https://doi.org/10.3390/children8110963
APA StyleAlfaro-Santafé, J., Gómez-Bernal, A., Lanuza-Cerzócimo, C., Alfaro-Santafé, J.-V., Pérez-Morcillo, A., & Almenar-Arasanz, A.-J. (2021). Effectiveness of Custom-Made Foot Orthoses vs. Heel-Lifts in Children with Calcaneal Apophysitis (Sever’s Disease): A CONSORT-Compliant Randomized Trial. Children, 8(11), 963. https://doi.org/10.3390/children8110963