
COVID-19 in Pediatric Inpatients: A Multi-Center Observational Study of Factors Associated with Negative Short-Term Outcomes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Statistical Analyses
3. Results
3.1. Demographics
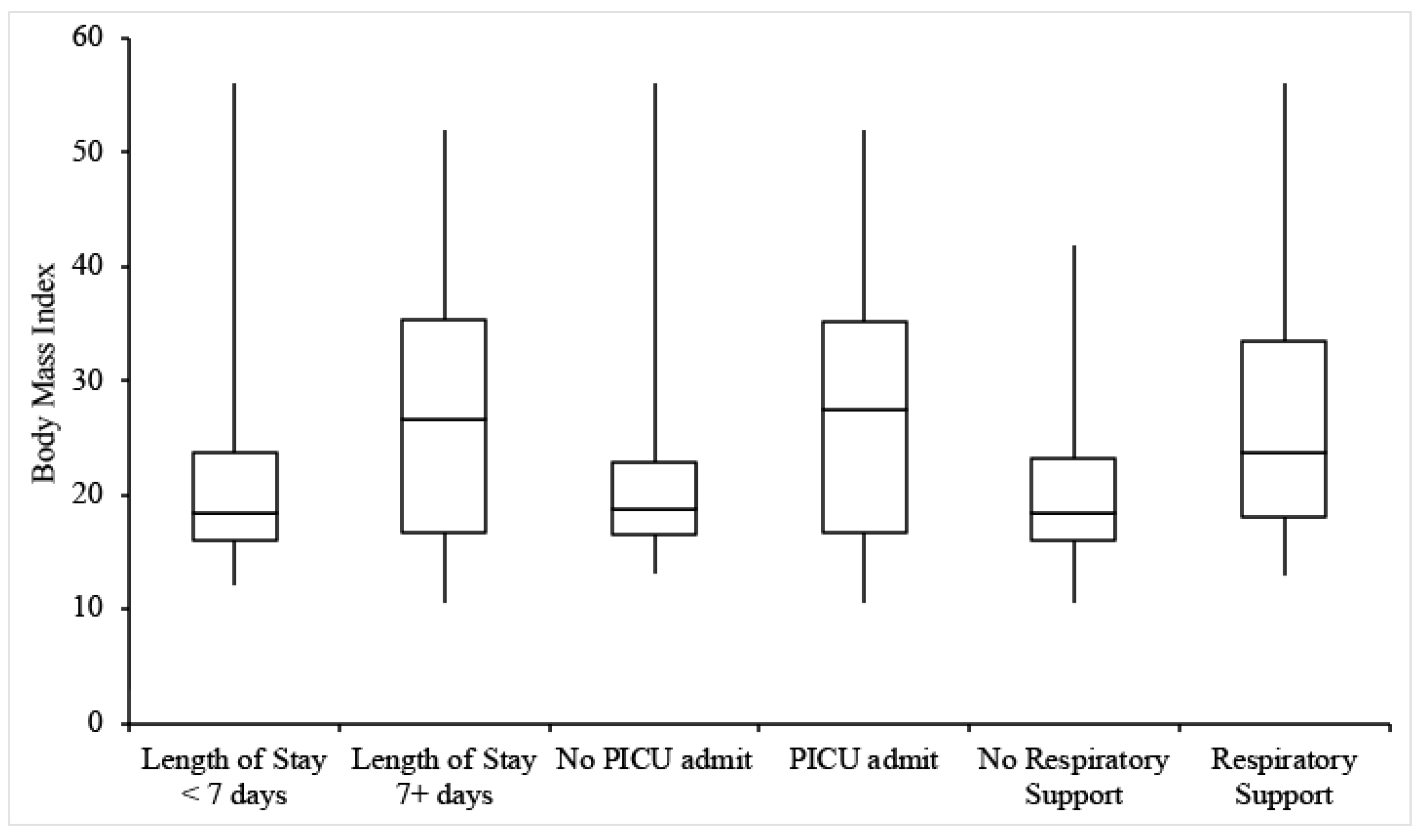
3.2. Length of Stay
3.3. PICU Admission
3.4. Respiratory Support and Imaging
4. Discussion
4.1. Age
4.2. BMI
4.3. Relevant Medical History
4.4. Ethnicity
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID-19 Weekly Cases and Deaths per 100,000 Population by Age, Race/Ethnicity, and Sex. Available online: https://covid.cdc.gov/covid-data-tracker/#demographicsovertime (accessed on 21 September 2021).
- Yasuhara, J.; Kuno, T.; Takagi, H.; Sumitomo, N. Clinical characteristics of COVID-19 in children: A systematic review. Pediatr. Pulmonol. 2020, 55, 2565–2575. [Google Scholar] [CrossRef] [PubMed]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F.I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Liguoro, I.; Pilotto, C.; Bonanni, M.; Ferrari, M.E.; Pusiol, A.; Nocerino, A.; Vidal, E.; Cogo, P. SARS-COV-2 infection in children and newborns: A systematic review. Eur. J. Pediatr. 2020, 179, 1029–1046. [Google Scholar] [CrossRef] [PubMed]
- Bhalala, U.S.; Gist, K.M.; Tripathi, S.; Boman, K.; Kumar, V.K.; Retford, L.; Chiotos, K.; Blatz, A.M.; Dapul, H.; Verma, S.; et al. Characterization and outcomes of hospitalized children with Coronavirus Disease 2019: A report from a multicenter, viral infection and respiratory illness universal study (Coronavirus Disease 2019) registry. Crit. Care Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.K.; Simpson, J.N.; Boyle, M.D.; Badolato, G.M.; Delaney, M.; McCarter, R.; Cora-Bramble, D. Racial and/or Ethnic and Socioeconomic Disparities of SARS-CoV-2 Infection Among Children. Pediatrics 2020, 146, e2020009951. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem Inflammatory Syndrome in U.S. children and adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Bhavsar, S.M.; Clouser, K.N.; Gadhavi, J.; Anene, O.; Kaur, R.; Lewis, R.; Naganathan, S.; Michalak, Z.; Chen, C.Q.; Shah, P.; et al. COVID-19 in Pediatrics: Characteristics of Hospitalized Children in New Jersey. Hosp. Pediatr. 2021, 11, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Chao, J.Y.; Derespina, K.R.; Herold, B.C.; Goldman, D.L.; Aldrich, M.; Weingarten, J.; Ushay, H.M.; Cabana, M.D.; Medar, S.S. Clinical characteristics and outcomes of hospitalized and critically ill children and adolescents with coronavirus disease 2019 at a tertiary care medical center in New York City. J. Pediatr. 2020, 223, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Zachariah, P.; Johnson, C.L.; Halabi, K.C.; Ahn, D.; Sen, A.I.; Fischer, A.; Banker, S.L.; Giordano, M.; Manice, C.S.; Diamond, R.; et al. Epidemiology, clinical features, and disease severity in patients with coronavirus disease 2019 (COVID-19) in a children’s hospital in New York City, New York. JAMA Pediatr. 2020, 174, e202430. [Google Scholar] [CrossRef] [PubMed]
- Graff, K.; Smith, C.; Silveira, L.; Jung, S.; Curran-Hays, S.; Jarjour, J.; Carpenter, L.; Pickard, K.; Mattiucci, M.; Fresia, J.; et al. Risk factors for severe COVID-19 in children. Pediatric Infect. Dis. J. 2021, 40, e137–e145. [Google Scholar] [CrossRef] [PubMed]
- Dhochak, N.; Singhal, T.; Kabra, S.K.; Lodha, R. Pathophysiology of COVID-19: Why children fare better than adults? Indian J. Pediatr. 2020, 87, 537–546. [Google Scholar] [CrossRef]
- Abrams, J.Y.; Godfred-Cato, S.E.; Oster, M.E.; Chow, E.; Koumans, E.H.; Bryant, B.; Leung, J.W.; Belay, E.D. Multisystem Inflammatory Syndrome in Children associated with Severe Acute Respiratory Syndrome Coronavirus 2: A systematic review. J. Pediatr. 2020, 226, 45–54. [Google Scholar] [CrossRef]
- Kornitzer, J.; Johnson, J.; Yang, M.; Pecor, K.; Cohen, N.; Jiang, C.; Ming, X. A systematic review of characteristics associated with COVID-19 in children with typical presentation and with Multisystem Inflammatory Syndrome. Int. J. Ennviron. Res. Public Health 2020, 18, 8269. [Google Scholar] [CrossRef]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B.; Ludwig, D.S. Obesity and impaired metabolic health in patients with COVID-19. Nat. Rev. Endocrinol. 2020, 16, 341–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Ma, Z.; Lei, Y. A meta-analysis of the association between obesity and COVID-19. Epidemiol. Infect. 2020, 149, e11. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Lu, Y.; Huang, Y.-M.; Wang, M.; Ling, W.; Sui, Y.; Zhao, H.-L. Obesity in patients with COVID-19: A systematic review and meta-analysis. Metabolism 2020, 113, 154378. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, S.; Christison, A.L.; Levy, E.; McGravery, J.; Tekin, A.; Bolliger, D.; Kumar, V.K.; Bansal, V.; Chiotos, K.; Gist, K.M.; et al. The impact of obesity on disease severity and outcomes among hospitalized children with COVID-19. Hosp Pediatr. 2021. [Google Scholar] [CrossRef]
- Nogueira-de-Almeida, C.A.; Del Ciampo, L.A.; Ferraz, I.S.; Del Ciampo, I.R.L.; Contini, A.A.; Ued, F.D.V. COVID-19 and obesity in childhood and adolescence: A clinical review. J. Pediatr. 2020, 96, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Fearnbach, S.N.; Johannsen, N.M.; Martin, C.K.; Katzmarzyk, P.T.; Beyl, R.A.; Hsia, D.S. A pilot study of cardiorespiratory fitness, adiposity, and cardiometabolic health in youth with overweight and obesity. Pediatr. Exerc. Sci. 2020, 32, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Al-Shorman, A.; Al-Domi, H.; Faqih, A. Markers of subclinical atherosclerosis in schoolchildren with obesity and metabolic syndrome. Swiss Med. Wkly. 2020, 147, w14446. [Google Scholar] [CrossRef] [PubMed]
- Kelishadi, R.; Roufarshbaf, M.; Soheili, S.; Payghambarzadeh, F.; Masjedi, M. Association of childhood obesity and the immune system: A systematic review of reviews. Child Obes. 2017, 13, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Ding, M.; Dong, X.; Zhang, J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- 2019 Community Health Needs Assessment. Arkansas Children’s Hospital. Available online: https://www.archildrens.org/-/media/Files/resources/community-needs-assessment/ach-chna-2019.pdf (accessed on 8 June 2021).
- 2019 Community Health Needs Assessment Report. Hackensack University Medical Center. Available online: https://www.hackensackmeridianhealth.org/wp-content/uploads/2019/12/2019-Hackensack-University-Medical-Center-CHNA-Report-v2.pdf?x56982 (accessed on 8 June 2021).
- 2019 Community Health Needs Assessment Summary Report. St. Joseph’s University Medical Center. Available online: https://www.stjosephshealth.org/images/pdf/2019%20SJUMC%20CHNA%20Summary%20Report.pdf (accessed on 8 June 2021).


{kind=link}
{kind=link}
| Sex | Age (Years) | Ethnicity | Admitting Hospital | ||||
|---|---|---|---|---|---|---|---|
| Female | 40 (48.7%) | <1 | 22 (26.8%) | African American | 11 (13.4%) | Arkansas | 22 (23.9%) |
| Male | 42 (51.2%) | 1–5 | 11 (13.4%) | Hispanic/Latino | 37 (45.1%) | Hackensack | 46 (56.1%) |
| 5–10 | 9 (10.9%) | White/Caucasian | 16 (19.5%) | St. Joseph’s | 14 (17.1%) | ||
| 10–15 | 16 (19.5%) | Asian | 3 (3.7%) | ||||
| 15–21 | 24 (29.3%) | Other/Unknown | 15 (18.3%) | ||||
| Length of Stay | n | Wald | p | OR | OR 95% CI |
|---|---|---|---|---|---|
| Age | 77 | 5.08 | 0.02 | 1.09 | 1.01–1.17 |
| Sex | 77 | 0.05 | 0.83 | 0.9 | 0.33–2.41 |
| BMI | 60 | 3.31 | 0.07 | 1.05 | 1–1.11 |
| Medical History | 77 | 0.35 | 0.56 | 1.35 | 0.5–3.67 |
| PICU Admission | n | Wald | p | OR | OR 95% CI |
| Age | 81 | 1.96 | 0.16 | 1.04 | 0.98–1.11 |
| Sex | 81 | 0.1 | 0.75 | 0.87 | 0.36–2.1 |
| BMI | 63 | 4.01 | 0.05 | 1.06 | 1–1.11 |
| Medical History | 81 | 0.51 | 0.48 | 1.39 | 0.56–3.42 |
| Respiratory Support | n | Wald | p | OR | OR 95% CI |
| Age | 81 | 11.41 | 0.001 | 1.13 | 1.05–1.21 |
| Sex | 81 | 0.6 | 0.44 | 0.7 | 0.28 1.74 |
| BMI | 63 | 4.86 | 0.03 | 1.07 | 1.01–1.13 |
| Medical History | 81 | 5.78 | 0.02 | 3.187 | 1.24–8.2 |
| Length of Stay | PICU Admission | Respiratory Support | ||||
|---|---|---|---|---|---|---|
| <7 Days | 7+ Days | No | Yes | No | Yes | |
| Age (years) a | 6.5 | 13.5 | 6.8 | 12.2 | 3.9 | 14.0 |
| Sex | ||||||
| Female | 70.3% | 29.7% | 57.5% | 42.5% | 60.0% | 40.0% |
| Male | 72.5% | 27.5% | 61.0% | 39.0% | 68.3% | 31.7% |
| BMI a | 18.5 | 26.7 | 18.8 | 27.6 | 18.5 | 23.7 |
| Medical History | ||||||
| No | 73.9% | 26.1% | 62.5% | 37.5% | 75.0% | 25.0% |
| Yes | 67.7% | 32.3% | 54.5% | 45.5% | 48.5% | 51.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubenstein, S.; Grew, E.; Clouser, K.; Kwok, A.; Veerapandiyan, A.; Kornitzer, J.; Pecor, K.; Ming, X. COVID-19 in Pediatric Inpatients: A Multi-Center Observational Study of Factors Associated with Negative Short-Term Outcomes. Children 2021, 8, 951. https://doi.org/10.3390/children8110951
Rubenstein S, Grew E, Clouser K, Kwok A, Veerapandiyan A, Kornitzer J, Pecor K, Ming X. COVID-19 in Pediatric Inpatients: A Multi-Center Observational Study of Factors Associated with Negative Short-Term Outcomes. Children. 2021; 8(11):951. https://doi.org/10.3390/children8110951
Chicago/Turabian StyleRubenstein, Sara, Emily Grew, Katharine Clouser, Alexander Kwok, Aravindhan Veerapandiyan, Jeffrey Kornitzer, Keith Pecor, and Xue Ming. 2021. "COVID-19 in Pediatric Inpatients: A Multi-Center Observational Study of Factors Associated with Negative Short-Term Outcomes" Children 8, no. 11: 951. https://doi.org/10.3390/children8110951
APA StyleRubenstein, S., Grew, E., Clouser, K., Kwok, A., Veerapandiyan, A., Kornitzer, J., Pecor, K., & Ming, X. (2021). COVID-19 in Pediatric Inpatients: A Multi-Center Observational Study of Factors Associated with Negative Short-Term Outcomes. Children, 8(11), 951. https://doi.org/10.3390/children8110951