
Evaluation of the Psychometric Properties of the Portuguese Peabody Developmental Motor Scales-2 Edition: A Study with Children Aged 12 to 48 Months

 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedures
2.4. Statistical Analysis
3. Results
3.1. Preliminary Analysis
3.2. Test-Retest Reliability
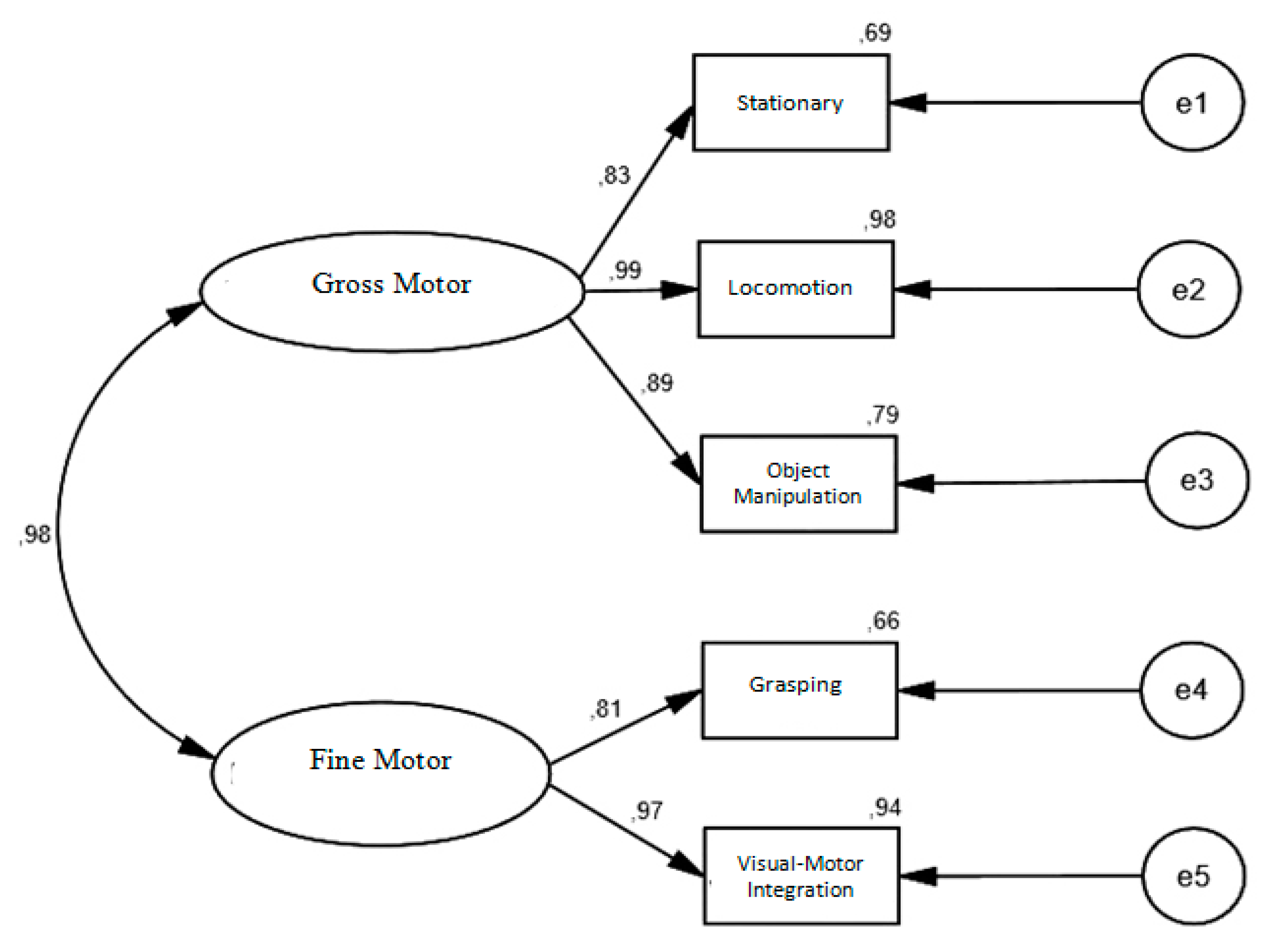
3.3. Construct Validity
4. Discussion
4.1. Preliminary Analysis
4.2. Test–Retest Reliability
4.3. Construct Validity
5. Study Limitations
6. Conclusions
7. Practical Applications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barreiros, J.; Neto, C. O Desenvolvimento Motor e o Género. Lisb. Edições FMH. 2005. Available online: http://analfabetismomotor.com.br/o-desenvolvimento-motor-e-o-genero/ (accessed on 5 September 2021).
- Carvalho, D. A Competência Motora Fina da Criança em Idade PRé-Escolar: UM Estudo Exploratório. Master’s Dissertation, Escola Superior de Educação do Instituto Politécnico de Viana do Castelo, Viana do Castelo, Portugal, 2007. [Google Scholar]
- Fernandes, M. Estudo Exploratório da Peabody Developmental Motor Scales-2 (PDMS-2), Dos 36 Aos 71 Meses de Idade. Master’s Dissertation, Faculdade de Motricidade Humana, Lisboa, Portugal, 2011. [Google Scholar]
- Folio, R.; Fewell, R. Peabody Developmental Motor Scales-2; PRO-Ed: Austin, TX, USA, 2000. [Google Scholar]
- Saraiva, L.; Rodrigues, L. Peabody developmental motor scales-2 (PDMS-2): Definição e aplicabilidade no contexto educativo, clínico e científico. In Desenvolvimento Motor da Criança; Barreiros, J., Cordovil, S., Carvalheiro, S., Eds.; Edições FMH: Lisboa, Portugal, 2007; pp. 285–292. [Google Scholar]
- Folio, R.; Fewell, R. Peabody Developmental Motor Scales and Activity Cards Manual; DLM Teaching Resources: Allen, TX, USA; Austin, TX, USA, 1983. [Google Scholar]
- Dusing, S.C.; Thorpe, D.; Rosenberg, A. Gross motor abilities in children with Hurler syndrome. Dev. Med. Child Neurol. 2006, 48 (Suppl. S11), 927–930. [Google Scholar] [CrossRef] [PubMed]
- Maring, J.R.; Courcelle-Carter, K.J. Comparison of Gross Motor Subtest scores of the Peabody Developmental Motor Scale-2 in children with Down Syndrome. Pediatrics Phys. Ther. 2004, 16 (Suppl. S1), 49–68. [Google Scholar]
- Mitchell, W.G.; Brumm, V.L.; Azen, C.G.; Patterson, K.E.; Aller, S.K.; Rodriguez, J. Longitudinal neurodevelopmental evaluation of children with opsoclonus-ataxia. Pediatrics 2005, 116 (Suppl. S4), 901–907. [Google Scholar] [CrossRef] [PubMed]
- Provost, B.; Lopez, B.; Heimerl, S.A. Comparison of motor delays in young children: Autism spectrum disorder, developmental delay, and developmental concerns. J. Autism Dev. Disord. 2007, 37 (Suppl. S2), 321–328. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Danoff, J.; Parks, R. Motor skills development of children with HIV infection measured with Peabody Developmental Motor Scale. Pediatric Phys. Ther. 2002, 14 (Suppl. S2), 74–84. [Google Scholar] [CrossRef] [PubMed]
- Angelsen, N.; Jacobsen, G.; Bakketeig, L.S. Breast feeding and cognitive development at age 1 and 5 years. Arch. Dis. Child. 2001, 85 (Suppl. S3), 183–188. [Google Scholar] [CrossRef]
- Arendt, R.; Angelopoulos, J.; Salvator, A.; Singer, L. Motor development of cocaineexposed children at age two years. Pediatrics 1999, 103, 86–92. [Google Scholar] [CrossRef]
- Evensen, K.A.I.; Skranes, J.; Brubakk, A.M.; Vik, T. Predictive value of early motor evaluation in preterm very low birth weight and term small for gestational age children. Early Hum. Dev. 2009, 85 (Suppl. S8), 511–518. [Google Scholar] [CrossRef][Green Version]
- Fetters, L.; Tronick, E. Neuromotor development of cocaine-exposed and control infants from birth through 15 months: Poor and poorer performance. Pediatrics 1996, 98 (Suppl. S5), 938–943. [Google Scholar]
- Majnemer, A.; Barr, R.G. Association between sleep position and early motor development. J. Pediatrics 2006, 149 (Suppl. S5), 623–629. [Google Scholar] [CrossRef]
- Miller-Loncar, C.; Lester, B.M.; Seifer, R.; Lagasse, L.L.; Bauer, C.R.; Shankaran, S.; Bada, H.S.; Wright, L.L.; Smeriglio, V.L.; Bigsby, R.; et al. Predictors of motor development in children prenatally exposed to cocaine. Neurotoxicology Teratol. 2005, 27 (Suppl. S2), 213–220. [Google Scholar] [CrossRef] [PubMed]
- Goyen, T.; Lui, K. Longitudinal motor development of “apparently normal” high-risk infants at 18 months, 3 and 5 years. Early Hum. Dev. 2002, 70, 103–115. [Google Scholar] [CrossRef]
- Nelson, S.; Lerner, E.; Needlman, R.; Salvator, A.; Singer, L. Cocaine, anemia, and neurodevelopmental outcomes in children: A longitudinal study. Dev. Behav. Pediatrics 2004, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Trasti, N.; Vik, T.; Jacobsen, G.; Bakketeig, L.S. Smoking in pregnancy and children’s mental and motor development at age 1 and 5 years. Early Hum. Dev. 1999, 55 (Suppl. S2), 137–147. [Google Scholar] [CrossRef]
- Sommerfelt, K.; Sonnander, K.; Skranes, J.; Andersson, H.W.; Ahlsten, G.; Ellertsen, B.; Markestad, T.; Jacobsen, G.; Hoffman, H.J.; Bakketeig, L.S. Neuropsychologic and motor function in small-for-gestation preschoolers. Pediatric Neurol. 2002, 26 (Suppl. S3), 186–191. [Google Scholar] [CrossRef]
- Rodrigues, L. Development and Validation of the AHEMD-SR Affordances in the Home Environment for Motor Development-Self Report. Ph.D. Thesis, Texas A&M University, College Station, TX, USA, 2005. [Google Scholar]
- Santos, D.; Tolocka, R.; Carvalho, J.; Heringer, L.; Almeida, C.; Miquelote, A. Desempenho motor grosso e sua associação com fatores neonatais, familiares e de exposição à creche em crianças até três anos de idade. Rev. Bras. De Fisioter. 2009, 13, 173–179. [Google Scholar] [CrossRef][Green Version]
- Saraiva, L.; Rodrigues, L.P.; Barreiros, J. Adaptação e validação da versão portuguesa Peabody Developmental Motor Scales-2: Um estudo com crianças préescolares. J. Phys. Educ. UEM 2011, 22 (Suppl. S4), 511–521. [Google Scholar] [CrossRef]
- Chien, C.; Bond, T. Measurement properties of fine motor scale of Peabody Development Motor Scales-second edition: Rasch Analysis. Am. J. Phys. Med. Rehabil. 2009, 88 (Suppl. S5), 376–382. [Google Scholar] [CrossRef]
- Bean, J.; Breaux, G.; Hymel, E.; Kinler, E.; Monti, D.; Rome, B. Concurrent validity of the Alberta Infant Motor Scale (AIMS) and the Peabody Developmental Motor Scale II (PDMS-II). Pediatric Phys. Ther. 2004, 16, 49–50. [Google Scholar]
- Valentini, N.; Saccani, R. Escala Motora Infantil de Alberta: validação para uma população gaúcha. Rev. Paul. De Pediatr. 2011, 29 (Suppl. S2), 231–238. [Google Scholar] [CrossRef]
- Connolly, B.H.; Dalton, L.; Smith, J.B.; Lamberth, N.G.; McCay, B.; Murphy, W. Concurrent validity of the Bayley Scales of Infant Development II (BSID-II) Motor Scale and the Peabody Developmental Motor Scale II (PDMS-2) in 12-Month-Old Infants. Pediatric Phys. Ther. 2006, 18 (Suppl. S3), 190–196. [Google Scholar] [CrossRef]
- Wang, H.; Liao, H.; Hsieh, C. Reliability, sensitivity to change, and responsiveness of the Peabody Developmental Motor Scales-second edition for children with Cerebral Palsy. Phys. Ther. 2006, 86 (Suppl. S10), 1351–1359. [Google Scholar] [CrossRef]
- Palisano, R.J.; Kolobe, T.H.; Haley, S.M.; Pax Lowes, L.; Jones, S.L. Validity of the Peabody Developmental Gross Motor Scale as an evaluative measure of Infants receiving physical therapy. Phys. Ther. 1995, 75 (Suppl. S11), 939–948. [Google Scholar] [CrossRef] [PubMed]
- Crowe, T.; Mcclain, C.; Provost, B. Motor Development of Native American children on the Peabody Developmental Motor Scales. Am. J. Occup. Ther. 1999, 53 (Suppl. S5), 514–518. [Google Scholar] [CrossRef] [PubMed]
- Provost, B.; Heimerl, S.; McClain, C.; Kim, N.H.; Lopez, B.R.; Kodituwakku, P. Concurrent Validity of the Bayley Scales of Infant Development II Motor Scale and the Peabody Developmental Motor Scales-2 in children with developmental delays. Pediatric Phys. Ther. 2004, 16, 149–156. [Google Scholar] [CrossRef]
- Tripathi, R.; Joshua, A.M.; Kotian, M.S.; Tedla, J.S. Normal motor development of Indian children on Peabody Developmental Motor Scales-2 (PDMS-2). Pediatric Phys. Ther. 2008, 20 (Suppl. S2), 167–172. [Google Scholar] [CrossRef] [PubMed]
- Van Hartingsveldt, M.; Cup, E.; Oostendorp, R. Reliability and validity of the fine motor scale of the Peabody Developmental Motor Scales-2. Occup. Ther. Int. 2005, 12, 1–13. [Google Scholar] [CrossRef]
- Leitão, P. Contributo Para a Validação de Uma Escala Pediátrica, Peabody Developmental Motor Scale-2 (Versão Portuguesa). Master’s Dissertation, Instituto Politécnico de Lisboa, Lisboa, Portugal, 2014. [Google Scholar]
- Tuckman, B. Manual de Investigação em Educação Lisboa; Fundação Calouste Gulbenkian: Lisboa, Portugal, 1994. [Google Scholar]
- Tuckman, B. Manual de Investigação em Educação; Fundação Calouste Gulbenkian: Lisboa, Portugal,, 2000. [Google Scholar]
- Hambleton, R.K.; Merenda, P.; Spielberger, C. Adapting Educational and Psychological Tests for Cross-Cultural Assessment; Hillsdale, N.J., Lawrence, S., Eds.; Erlbaum Publishers: Mahwah, NJ, USA, 2005. [Google Scholar]
- AERA; APA; NCME. Standards for Educational and Psychological Testing; American Educational Research Association: Washington, DC, USA, 1999. [Google Scholar]
- Byrne, B. Structural equation modeling with AMOS. In Basic Concepts, 529 Applications, and Programming, 2nd ed.; Taylor & Francis Group: New York, NY, USA, 2010. [Google Scholar]
- Byrne, B. Structural equation modeling with AMOS. In Basic Concepts, 532 Applications, and Programming, 3rd ed.; Taylor & Francis Group: New York, NY, USA, 2016. [Google Scholar]
- Hair, J.F.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2014. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 25.0; IBM Corp: Armonk, NY, USA, 2017. [Google Scholar]
- Hair, J.F.; Ringle, C.M.; Gudergan, S.P.; Fischer, A.; Nitzl, C.; Menictas, C. Partial least squares structural equation modeling-based discrete choice modeling: An illustration in modeling retailer choice. Bus. Res. 2019, 12, 115–142. [Google Scholar] [CrossRef]
- Kline, R. Principles and Practices of Structural Equation Modeling, 3rd ed.; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Kline, R. Principles and Practices of Structural Equation Modeling, 4th ed.; The Guildford Press: New York, NY, USA, 2016. [Google Scholar]
- Marsh, H.; Hau, K.; Wen, Z. In search of golden rules: Comment on hypothesis testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Struct. Equ. Modeling 2004, 11 (Suppl. S3), 320–341. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18 (Suppl. S1), 39–50. [Google Scholar] [CrossRef]
- Raykov, T. Estimation of composite reliability for congeneric measures. Appl. Psychol. Meas. 1997, 21 (Suppl. S2), 173–184. [Google Scholar] [CrossRef]
- Vanvuchelen, M.; Mulders, H.; Smeyers, K. Onderzoek naar de bruikbaarheid van de recente Amerikaanse Peabody Developmental Scales-2 voor vijfjarige, Vlaamse kinderen. Signaal 2003, 45, 24–41. [Google Scholar]
- Kolobe, T.; Bulanda, M.; Susman, L. Predicting Motor outcome at preschool age for infants tested at 7, 30, 60, and 90 days after term age using the test of infant motor performance. Phys. Ther. 2004, 84 (Suppl. S12), 1144–1156. [Google Scholar] [CrossRef] [PubMed]
- Li-Tsang, C.W.; Lee, H.C.; Hung, L.K. Validation of chopsticks manipulation test for screening Chinese with fine motor dysfunction. Hong Kong J. Pediatrics 2006, 11 (Suppl. S2), 103–109. [Google Scholar]
- Souza, S.C.; Leone, C.; Takano, O.A.; Moratelli, H.B. Desenvolvimento de pré-escolares na educação infantil em Cuiabá, Mato Grosso, Brasil. Cad Saúde Pública 2008, 24, 1917–1926. [Google Scholar] [CrossRef] [PubMed][Green Version]


{kind=link}
| 12–23 Months (n = 96) | 24–35 Months (n = 153) | 36–47 Months (n = 143) | Totals (n = 392) | ||
|---|---|---|---|---|---|
| Age (Average ± SD) | 18.66 ± 3.91 | 28.07 ± 3.35 | 39.30 ± 3.55 | 29.86 ± 8.79 | |
| Sex (%) | Male | 44 (45.8) | 79 (51.6) | 76 (51.6) | 199 (50.8) |
| Female | 52 (54.2) | 74 (48.4) | 67 (48.4) | 193 (49.2) | |
| Residence (%) | Urban | 60 (62.5) | 132 (86.3) | 125 (87.4) | 317 (80.9) |
| SemiUrban | 21 (15.6) | 3 (2.0) | 16 (11.2) | 40 (10.2) | |
| Rural | 15 (21.9) | 18 (11.8) | 2 (1.4) | 35(8.9) |
| Subtests | 12–23 Months (n = 96) | 24–35 Months (n = 153) | 36–48 Months (n = 143) | Sig. | |
|---|---|---|---|---|---|
| Stationary | Mean (SD) | 39.4 (2.3) | 43.3 (2.8) | 48.9 (3.8) | |
| Min–Max * | 36–46 * | 38–51 * | 41–56 * | <0.001 | |
| Amplitude | 10 | 13 | 15 | ||
| Locomotion | Mean (SD) | 81.4 (13.5) | 111.6 (13.5) | 137.8 (10.1) | |
| Min–Max * | 50–100 * | 87–136 * | 115–158 * | <0.001 | |
| Amplitude | 50 | 49 | 43 | ||
| Object Manipulation | Mean (SD) | 13.2 (5.5) | 21.1 (5.8) | 30.0 (5.1) | |
| Min–Max * | 1–26 * | 8–35 * | 20–42 * | <0.001 | |
| Amplitude | 25 | 27 | 22 | ||
| Grasping | Mean (SD) | 39.9 (3.8) | 43.3 (1.7) | 48.2 (2.7) | |
| Min–Max * | 34–46 * | 40–47* | 42–52 * | <0.001 | |
| Amplitude | 12 | 7 | 10 | ||
| Visual–Motor Integration | Mean (SD) | 79.7 (9.83) | 99.9 (11.1) | 121 (8.8) | |
| Min–Max * | 53–96 * | 79–122 * | 109–139 * | <0.001 | |
| Amplitude | 43 | 43 | 30 |
| Subtest | Internal Consistency (α Cronbach) n = 392 | Test–Retest Reliability (ICC) n = 30 |
|---|---|---|
| Stationary | 0.86 | 0.98 |
| Locomotion | 0.97 | 0.99 |
| Object Manipulation | 0.93 | 0.98 |
| Grasping | 0.84 | 0.99 |
| Visual–Motor Integration | 0.96 | 0.99 |
| Gross Motricity | 0.71 | 0.75 |
| Fine Motricity | 0.69 | 0.71 |
| Total Motricity | 0.85 | 0.87 |
| Index | χ2 | χ2/DF | SRMR | TLI | CFI | RMSEA | 90%IC |
|---|---|---|---|---|---|---|---|
| M 1 | 55.614 | 13.904 | 0.065 | 0.992 | 0.998 | 0.68 | 0.000–0.138 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rebelo, M.; Serrano, J.; Duarte-Mendes, P.; Monteiro, D.; Paulo, R.; Marinho, D.A. Evaluation of the Psychometric Properties of the Portuguese Peabody Developmental Motor Scales-2 Edition: A Study with Children Aged 12 to 48 Months. Children 2021, 8, 1049. https://doi.org/10.3390/children8111049
Rebelo M, Serrano J, Duarte-Mendes P, Monteiro D, Paulo R, Marinho DA. Evaluation of the Psychometric Properties of the Portuguese Peabody Developmental Motor Scales-2 Edition: A Study with Children Aged 12 to 48 Months. Children. 2021; 8(11):1049. https://doi.org/10.3390/children8111049
Chicago/Turabian StyleRebelo, Miguel, João Serrano, Pedro Duarte-Mendes, Diogo Monteiro, Rui Paulo, and Daniel Almeida Marinho. 2021. "Evaluation of the Psychometric Properties of the Portuguese Peabody Developmental Motor Scales-2 Edition: A Study with Children Aged 12 to 48 Months" Children 8, no. 11: 1049. https://doi.org/10.3390/children8111049
APA StyleRebelo, M., Serrano, J., Duarte-Mendes, P., Monteiro, D., Paulo, R., & Marinho, D. A. (2021). Evaluation of the Psychometric Properties of the Portuguese Peabody Developmental Motor Scales-2 Edition: A Study with Children Aged 12 to 48 Months. Children, 8(11), 1049. https://doi.org/10.3390/children8111049