
Head Growth and Neurodevelopment of Preterm Infants with Surgical Necrotizing Enterocolitis and Spontaneous Intestinal Perforation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures and Outcomes
2.3. Statistical Analysis
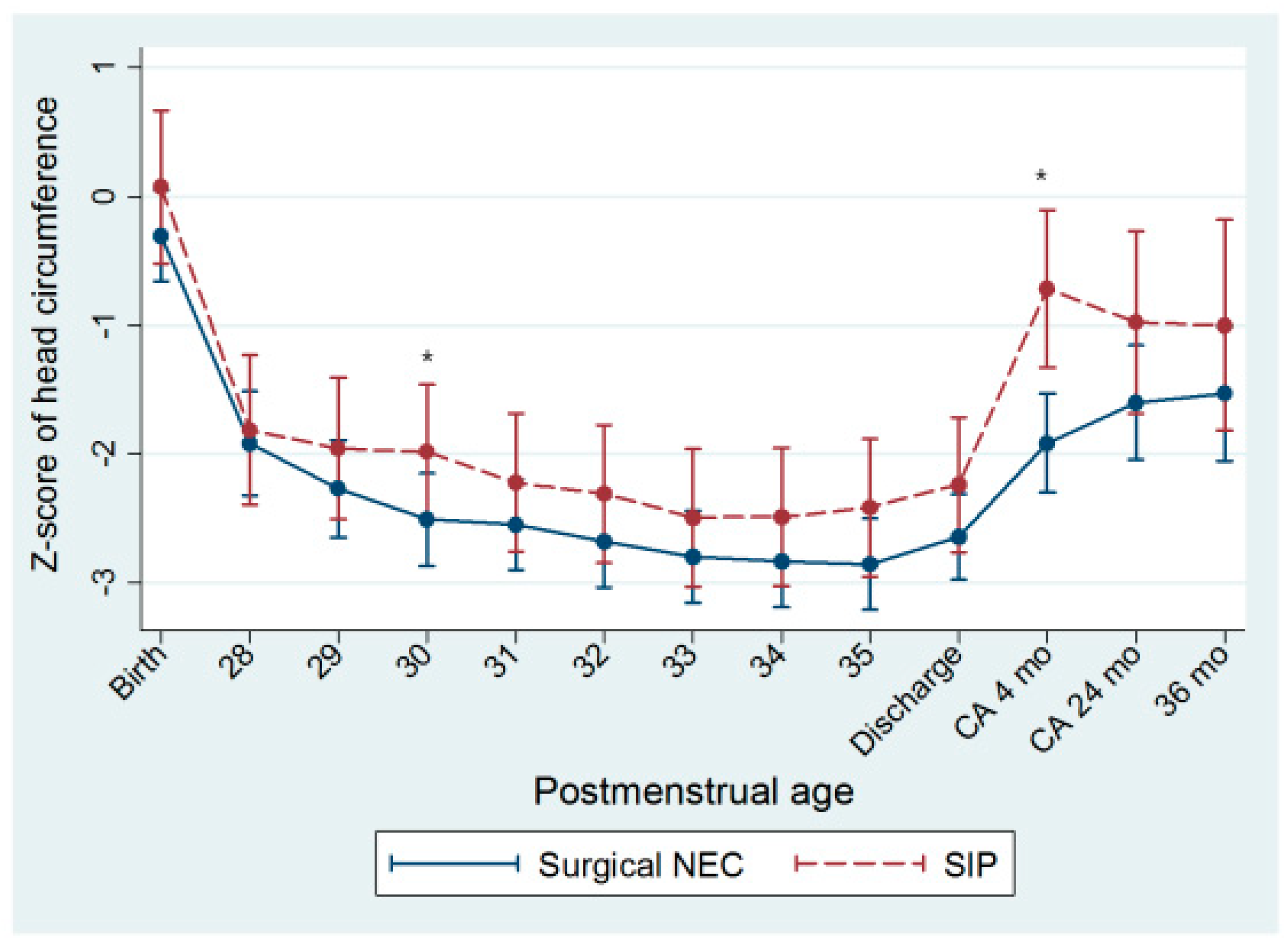
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yee, W.H.; Soraisham, A.S.; Shah, V.S.; Aziz, K.; Yoon, W.; Lee, S.K.; Network, C.N. Incidence and Timing of Presentation of Necrotizing Enterocolitis in Preterm Infants. Pediatrics 2012, 129, E298–E304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillet, R.; Stoll, B.J.; Cotten, C.M.; Gantz, M.; McDonald, S.; Poole, W.K.; Phelps, D.L.; Dev, N.I.C.H.H. Association of H2-blocker therapy and higher incidence of necrotizing enterocolitis in very low birth weight infants. Pediatrics 2006, 117, E137–E142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holman, R.C.; Stoll, B.J.; Curns, A.T.; Yorita, K.L.; Steiner, C.A.; Schonberger, L.B. Necrotising enterocolitis hospitalisations among neonates in the United States. Paediatr. Perinat. Epidemiol. 2006, 20, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.C.; Kliegman, R.M.; Hack, M. Severity of Necrotizing Enterocolitis—Influence on Outcome at 2 Years of Age. Pediatrics 1989, 84, 808–814. [Google Scholar] [PubMed]
- Hintz, S.R.; Kendrick, D.E.; Stoll, B.J.; Vohr, B.R.; Fanaroff, A.A.; Donovan, E.F.; Poole, W.K.; Blakely, M.L.; Wright, L.; Higgins, R.; et al. Neurodevelopmental and growth outcomes of extremely low birth weight infants after necrotizing enterocolitis. Pediatrics 2005, 115, 696–703. [Google Scholar] [CrossRef]
- Schulzke, S.M.; Deshpande, G.C.; Patole, S.K. Neurodevelopmental outcomes of very low-birth-weight infants with necrotizing enterocolitis—A systematic review of observational studies. Arch. Pediat. Adolesc. Med. 2007, 161, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Rees, C.M.; Pierro, A.; Eaton, S. Neurodevelopmental outcomes of neonates with medically and surgically treated necrotizing enterocolitis. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F193–F198. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.R.; Rellinger, E.J.; Hatch, L.D.; Weitkamp, J.H.; Speck, K.E.; Danko, M.; Blakely, M.L. Surgical necrotizing enterocolitis. Semin. Perinatol. 2017, 41, 70–79. [Google Scholar] [CrossRef] [Green Version]
- Pumberger, W.; Mayr, M.; Kohlhauser, C.; Weninger, M. Spontaneous localized intestinal perforation in very-low-birth-weight infants: A distinct clinical entity different from necrotizing enterocolitis. J. Am. Coll. Surg. 2002, 195, 796–803. [Google Scholar] [CrossRef]
- Zozaya, C.; Shah, J.; Pierro, A.; Zani, A.; Synnes, A.; Lee, S.; Shah, P.S.; CNN, C.N.N.; Networ, C.N.F.-U. Neurodevelopmental and growth outcomes of extremely preterm infants with necrotizing enterocolitis or spontaneous intestinal perforation. J. Pediatr. Surg. 2021, 56, 309–316. [Google Scholar] [CrossRef]
- Wadhawan, R.; Oh, W.; Hintz, S.R.; Blakely, M.L.; Das, A.; Bell, E.F.; Saha, S.; Laptook, A.R.; Shankaran, S.; Stoll, B.J.; et al. Neurodevelopmental outcomes of extremely low birth weight infants with spontaneous intestinal perforation or surgical necrotizing enterocolitis. J. Perinatol. 2014, 34, 64–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, T.A.; Meinzen-Derr, J.; Gratton, T.; Steichen, J.; Donovan, E.F.; Yolton, K.; Alexander, B.; Narendran, V.; Schibler, K.R. Hospital and neurodevelopmental outcomes of extremely low-birth-weight infants with necrotizing enterocolitis and spontaneous intestinal perforation. J. Perinatol. 2012, 32, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Adesanya, O.A.; O’Shea, T.M.; Turner, C.S.; Amoroso, R.M.; Morgan, T.M.; Aschner, J.L. Intestinal perforation in very low birth weight infants: Growth and neurodevelopment at 1 year of age. J. Perinatol. 2005, 25, 583–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hack, M.; Breslau, N.; Weissman, B.; Aram, D.; Klein, N.; Borawski, E. Effect of Very-Low-Birth-Weight and Subnormal Head Size on Cognitive-Abilities at School Age. N. Engl. J. Med. 1991, 325, 231–237. [Google Scholar] [CrossRef]
- Shin, S.H.; Kim, E.K.; Yoo, H.; Choi, Y.H.; Kim, S.; Lee, B.K.; Jung, Y.H.; Kim, H.Y.; Kim, H.S.; Choi, J.H. Surgical Necrotizing Enterocolitis versus Spontaneous Intestinal Perforation in White Matter Injury on Brain Magnetic Resonance Imaging. Neonatology 2016, 110, 148–154. [Google Scholar] [CrossRef]
- Blakely, M.L.; Lally, K.P.; McDonald, S.; Brown, R.L.; Barnhart, D.C.; Ricketts, R.R.; Thompson, W.R.; Scherer, L.R.; Klein, M.D.; Letton, R.W.; et al. Postoperative outcomes of extremely low birth-weight infants with necrotizing enterocolitis or isolated intestinal perforation: A prospective cohort study by the NICHD Neonatal Research Network. Ann. Surg. 2005, 241, 984–989. [Google Scholar] [CrossRef]
- Kliegman, R.M.; Walsh, M.C. Neonatal necrotizing enterocolitis: Pathogenesis, classification, and spectrum of illness. Curr. Probl. Pediatr. 1987, 17, 213–288. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary Dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Johnson, S.; Moore, T.; Marlow, N. Using the Bayley-III to assess neurodevelopmental delay: Which cut-off should be used? Pediatr. Res. 2014, 75, 670–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilbride, H.W.; Aylward, G.P.; Doyle, L.W.; Singer, L.T.; Lantos, J. Prognostic neurodevelopmental testing of preterm infants: Do we need to change the paradigm? J. Perinatol. 2017, 37, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Kwun, Y.; Park, H.W.; Kim, M.J.; Lee, B.S.; Kim, E.A. Validity of the ages and stages questionnaires in Korean compared to Bayley Scales of infant development-II for screening preterm infants at corrected age of 18–24 months for neurodevelopmental delay. J. Korean Med. Sci. 2015, 30, 450–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, C.H.; Kim, S.W.; Jeon, H.R.; Jung, D.W.; Cho, H.E.; Kim, J.; Lee, J.W. Clinical Usefulness of the Korean Developmental Screening Test (K-DST) for Developmental Delays. Ann. Rehabil. Med. 2019, 43, 490–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.; Kim, E.K.; Song, I.G.; Heo, J.S.; Shin, S.H.; Kim, H.S. Head growth during neonatal intensive care unit stay is related to the neurodevelopmental outcomes of preterm small for gestational age infants. Pediatr. Neonatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Song, I.G.; Kim, E.K.; Cho, H.; Shin, S.H.; Sohn, J.A.; Kim, H.S. Differential Effect of Growth on Development between AGA and SGA Preterm Infants. Int. J. Environ. Res. Public Health 2020, 17, 3022. [Google Scholar] [CrossRef] [PubMed]
- Regev, R.H.; Arnon, S.; Litmanovitz, I.; Bauer-Rusek, S.; Boyko, V.; Lerner-Geva, L.; Reichman, B.; Israel Neonatal Network. Association between neonatal morbidities and head growth from birth until discharge in very-low-birthweight infants born preterm: A population-based study. Dev. Med. Child Neurol. 2016, 58, 1159–1166. [Google Scholar] [CrossRef]
- Claas, M.J.; de Vries, L.S.; Koopman, C.; Uniken Venema, M.M.; Eijsermans, M.J.; Bruinse, H.W.; Verrijn Stuart, A.A. Postnatal growth of preterm born children ≤750 g at birth. Early Hum. Dev. 2011, 87, 495–507. [Google Scholar] [CrossRef]
- Cooke, R.W.; Foulder-Hughes, L. Growth impairment in the very preterm and cognitive and motor performance at 7 years. Arch. Dis. Child. 2003, 88, 482–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kan, E.; Roberts, G.; Anderson, P.J.; Doyle, L.W. The association of growth impairment with neurodevelopmental outcome at eight years of age in very preterm children. Early Hum. Dev. 2008, 84, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Shin, S.H. Extrauterine growth restriction in extremely preterm infants based on the Intergrowth-21st Project Preterm Postnatal Follow-up Study growth charts and the Fenton growth charts. Eur. J. Pediatr. 2021, 180, 817–824. [Google Scholar] [CrossRef]
- Löfqvist, C.; Engström, E.; Sigurdsson, J.; Hård, A.-L.; Niklasson, A.; Ewald, U.; Holmström, G.; Smith, L.E.H.; Hellström, A. Postnatal Head Growth Deficit Among Premature Infants Parallels Retinopathy of Prematurity and Insulin-like Growth Factor-1 Deficit. Pediatrics 2006, 117, 1930. [Google Scholar] [CrossRef] [Green Version]
- Stoll, B.J.; Hansen, N.I.; Adams-Chapman, I.; Fanaroff, A.A.; Hintz, S.R.; Vohr, B.; Higgins, R.D. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 2004, 292, 2357–2365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuestas, E.; Aguilera, B.; Cerutti, M.; Rizzotti, A. Sustained Neonatal Inflammation Is Associated with Poor Growth in Infants Born Very Preterm during the First Year of Life. J. Pediatr. 2019, 205, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.Y.; Leung, F.W.; Lam, H.S.; Tam, Y.H.; To, K.F.; Cheung, H.M.; Leung, K.T.; Poon, T.C.; Lee, K.H.; Li, K.; et al. Immunoregulatory protein profiles of necrotizing enterocolitis versus spontaneous intestinal perforation in preterm infants. PLoS ONE 2012, 7, e36977. [Google Scholar] [CrossRef] [Green Version]
- Jammeh, M.L.; Adibe, O.O.; Tracy, E.T.; Rice, H.E.; Clark, R.H.; Smith, P.B.; Greenberg, R.G. Racial/ethnic differences in necrotizing enterocolitis incidence and outcomes in premature very low birth weight infants. J. Perinatol. 2018, 38, 1386–1390. [Google Scholar] [CrossRef] [PubMed]
- Cuna, A.; Sampath, V.; Khashu, M. Racial Disparities in Necrotizing Enterocolitis. Front. Pediatr. 2021, 9, 633088. [Google Scholar] [CrossRef]
- Singh, A.; Yeh, C.J.; Boone Blanchard, S. Ages and Stages Questionnaire: A global screening scale. Boletín Med. Hosp. Infant. Mex. 2017, 74, 5–12. [Google Scholar] [CrossRef]
- Han, S.; Kim, O.; Yoo, C.; Heo, J.S.; Lee, H.-S.; Jeon, J. Neurodevelopmental Correlations between the Korean Developmental Screening Test and Bayley Scale III in Very-Low-Birth-Weight Infants. Neonatal Med. 2020, 27, 167–173. [Google Scholar] [CrossRef]
- Schonhaut, L.; Armijo, I.; Schonstedt, M.; Alvarez, J.; Cordero, M. Validity of the ages and stages questionnaires in term and preterm infants. Pediatrics 2013, 131, e1468–e1474. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.J.; Lee, J.Y.; Sohn, J.A.; Lee, E.H.; Lee, J.A.; Choi, C.W.; Kim, E.K.; Kim, H.S.; Kim, B.I.; Choi, J.H. A Validity Study of the Korean Ages and Stages Questionnaires: Screening for Developmental Delay in Preterm Infant. J. Korean Soc. Neonatol. 2010, 17, 217–223. [Google Scholar] [CrossRef]
- Terrin, G.; Boscarino, G.; Gasparini, C.; Di Chiara, M.; Faccioli, F.; Onestà, E.; Parisi, P.; Spalice, A.; De Nardo, M.C.; Dito, L.; et al. Energy-enhanced parenteral nutrition and neurodevelopment of preterm newborns: A cohort study. Nutrition 2021, 89, 111219. [Google Scholar] [CrossRef] [PubMed]
- Boscarino, G.; Conti, M.G.; Gasparini, C.; Onestà, E.; Faccioli, F.; Dito, L.; Regoli, D.; Spalice, A.; Parisi, P.; Terrin, G. Neonatal Hyperglycemia Related to Parenteral Nutrition Affects Long-Term Neurodevelopment in Preterm Newborn: A Prospective Cohort Study. Nutrients 2021, 13, 1930. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, F.; Azari, N.; Ghiasvand, H.; Shahrokhi, A.; Rahmani, N.; Fatollahierad, S. Do NICU developmental care improve cognitive and motor outcomes for preterm infants? A systematic review and meta-analysis. BMC Pediatr. 2020, 20, 67. [Google Scholar] [CrossRef]
- Ehrenkranz, R.A.; Dusick, A.M.; Vohr, B.R.; Wright, L.L.; Wrage, L.A.; Poole, W.K. Growth in the Neonatal Intensive Care Unit Influences Neurodevelopmental and Growth Outcomes of Extremely Low Birth Weight Infants. Pediatrics 2006, 117, 1253. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Surgical NEC (n = 60) | SIP (n = 22) | p-Value | |
|---|---|---|---|
| Gestational age (weeks) | 26.6 (24.3–27.5) | 26.5 (25.1–27.3) | 0.695 |
| Birth weight (grams) | 710 (606.0–980.0) | 745 (620.0–920.0) | 0.917 |
| Birth weight z-score | −0.1 (−1.1–0.4) | −0.7 (−1.4–0.5) | 0.867 |
| Birth HC z-score | −0.2 (−1.2–0.4) | −0.1 (−1.1–0.5) | 0.617 |
| C/S | 31 (51.7) | 11 (50.0) | 1.000 |
| Female | 23 (38.3) | 9 (40.9) | 1.000 |
| Multiple birth | 32 (53.3) | 10 (45.5) | 0.621 |
| Outborn | 22 (36.7) | 8 (36.4) | 1.000 |
| Antenatal steroid use | 17 (85.0) | 57 (79.2) | 0.534 |
| SGA | 18 (30.0) | 9 (40.9) | 0.429 |
| RDS | 52 (86.7) | 18 (81.8) | 0.725 |
| Moderate-to-severe BPD | 37 (74.0) | 12 (57.1) | 0.173 |
| Sepsis | 35 (59.3) | 8 (36.4) | 0.082 |
| PDA operation | 25 (45.5) | 9 (40.9) | 0.802 |
| ROP operation | 26 (53.1) | 8 (38.1) | 0.303 |
| IVH ≥ grade 3 | 11 (18.6) | 4 (18.2) | 1.000 |
| PVL | 13 (23.6) | 3 (13.6) | 0.535 |
| Postnatal days at surgery | 15.5 (9.0–30.0) | 6 (3.0–10.0) | <0.001 |
| PMA at surgery (weeks) | 28.6 (26.7–31.1) | 27.6 (26.7–28.6) | 0.046 |
| PMA at discharge (weeks) | 42.0 (38.5–45.29) | 41.3 (39.0–43.1) | 0.766 |
| Antibiotics before surgery (days) | 8 (4–17) | 5 (2–7) | 0.042 |
| Last 7 days before surgery | |||
| Hydrocortisone | 6 (10) | 3 (13.6) | 0.696 |
| PDA medical treatment | 11 (18.3) | 4 (18.2) | 1.000 |
| Inotropic agents | 6 (10) | 3 (13.6) | 0.696 |
| Death/s | 11 (18.3) | 1 (4.6) | 0.166 |
| Surgical NEC (n = 60) | SIP (n = 22) | p-Value | |
|---|---|---|---|
| At PMA 34 weeks | |||
| weight z-score | −1.8 (−2.4–−1.4) | −1.9 (−2.6–−1.3) | 0.662 |
| HC z-score | −2.9 (−3.6–−1.9) | −2.6 (−3.2–−1.9) | 0.262 |
| CA 4 months | |||
| weight z-score | −1.8 (−3.1–−0.9) | −0.9 (−2.8–−0.2) | 0.089 |
| HC z-score | −2.2 (−3.3–−0.79) | −0.5 (−1.7–0.5) | 0.018 |
| CA 24 months | |||
| weight z-score | −1.2 (−1.9–−0.5) | −0.4 (−1.8–0.1) | 0.281 |
| HC z-score | −1.4 (−2.3–−0.4) | −0.9 (−2–0.4) | 0.234 |
| 36 months | |||
| weight z-score | −1.3 (−2.3–−0.6) | −0.9 (−2.7–−0.3) | 0.856 |
| HC z-score | −1.3 (−2.1–−0.9) | −0.9 (−2.2–−0.3) | 0.421 |
| Surgical NEC (n = 60) | SIP (n = 22) | p-value | |
|---|---|---|---|
| Weight z-score change | |||
| Birth to PMA 34 weeks | −1.5 (−2–−0.9) | −1.5 (−1.9–−1.0) | 0.896 |
| PMA 34 weeks to CA 4 months | 0.2 (−1–1.0) | 1.1 (−0.1–1.6) | 0.052 |
| CA 4 months to 24 months | 0.6 (−0.3–1.9) | −0.2 (−0.8–0.8) | 0.149 |
| HC z-score change | |||
| Birth to PMA 34 weeks | −2.3 (−3–−1.3) | −1.9 (−2.6–−1.5) | 0.689 |
| PMA 34 weeks to CA 4 months | 1.2 (0.1–1.9) | 2.1 (1.1–2.7) | 0.025 |
| CA 4 months to 24 months | 0.3 (0.0–0.6) | −0.4 (−0.6–0.2) | 0.154 |
| Surgical NEC (n = 49) | SIP (n = 21) | p-Value | Adjusted p-Value * | |
|---|---|---|---|---|
| At CA 24 months | n = 42 | n = 20 | ||
| CP | 7 (16.7) | 2 (10.0) | 0.705 | 0.860 |
| Hearing impairment | 5 (11.9) | 1 (5.3) | 0.655 | 0.649 |
| Blindness | 3 (7.1) | 0 (0.0) | 0.156 | 0.110 |
| Bayley-III (CA 18–24 months) | n = 31 | n = 13 | ||
| CA at exam (months) | 19.5 (18.8–22.5) | 20.3 (19.2–21.7) | 0.495 | |
| Cognitive | 85 (70–95) | 85 (80–90) | 0.979 | |
| Language | 77 (68–91) | 79 (77–86) | 0.486 | |
| Motor | 85 (70–91) | 88 (79–100) | 0.366 | |
| Cognitive & language < 85 | 12 (38.7) | 5 (38.5) | 1.000 | 0.654 |
| Motor < 85 | 15 (48.4) | 5 (38.5) | 0.742 | 0.889 |
| Development delay in Bayley-III | 16 (51.6) | 6 (46.2) | 1.000 | 0.915 |
| NDI | 22 (51.2) | 7 (35.0) | 0.284 | 0.347 |
| Death or NDI | 25 (58.1) | 9 (45.0) | 0.418 | 0.189 |
| At 36 months | ||||
| K-ASQ or K-DST | n = 27 | n = 8 | ||
| Language < cut-off | 14 (51.9) | 1 (12.5) | 0.101 | 0.083 |
| Gross motor < cut-off | 13 (48.2) | 0 (0.0) | 0.015 | 0.012 |
| Fine motor < cut-off | 11 (40.7) | 0 (0.0) | 0.037 | 0.043 |
| Cognitive < cut-off | 15 (55.6) | 1 (12.5) | 0.047 | 0.026 |
| Social < cut-off | 12 (44.4) | 0 (0.0) | 0.032 | 0.016 |
| Any < cut-off | 16 (59.3) | 2 (25) | 0.121 | 0.077 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.-H.; Kim, E.-K.; Kim, S.-H.; Kim, H.-Y.; Kim, H.-S. Head Growth and Neurodevelopment of Preterm Infants with Surgical Necrotizing Enterocolitis and Spontaneous Intestinal Perforation. Children 2021, 8, 833. https://doi.org/10.3390/children8100833
Shin S-H, Kim E-K, Kim S-H, Kim H-Y, Kim H-S. Head Growth and Neurodevelopment of Preterm Infants with Surgical Necrotizing Enterocolitis and Spontaneous Intestinal Perforation. Children. 2021; 8(10):833. https://doi.org/10.3390/children8100833
Chicago/Turabian StyleShin, Seung-Han, Ee-Kyung Kim, Seh-Hyun Kim, Hyun-Young Kim, and Han-Suk Kim. 2021. "Head Growth and Neurodevelopment of Preterm Infants with Surgical Necrotizing Enterocolitis and Spontaneous Intestinal Perforation" Children 8, no. 10: 833. https://doi.org/10.3390/children8100833
APA StyleShin, S.-H., Kim, E.-K., Kim, S.-H., Kim, H.-Y., & Kim, H.-S. (2021). Head Growth and Neurodevelopment of Preterm Infants with Surgical Necrotizing Enterocolitis and Spontaneous Intestinal Perforation. Children, 8(10), 833. https://doi.org/10.3390/children8100833