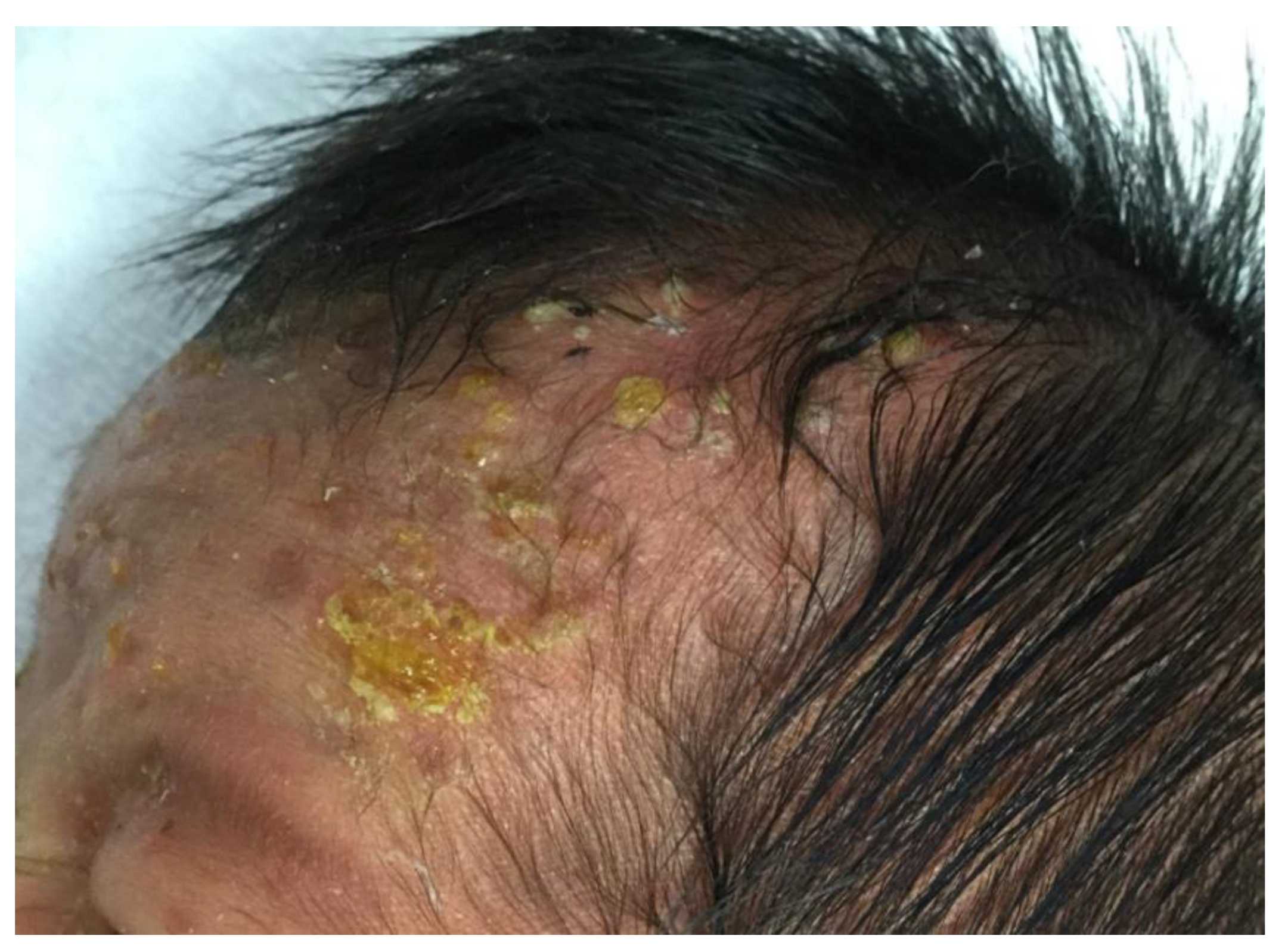
A Case of Eosinophilic Pustular Folliculitis since Birth

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
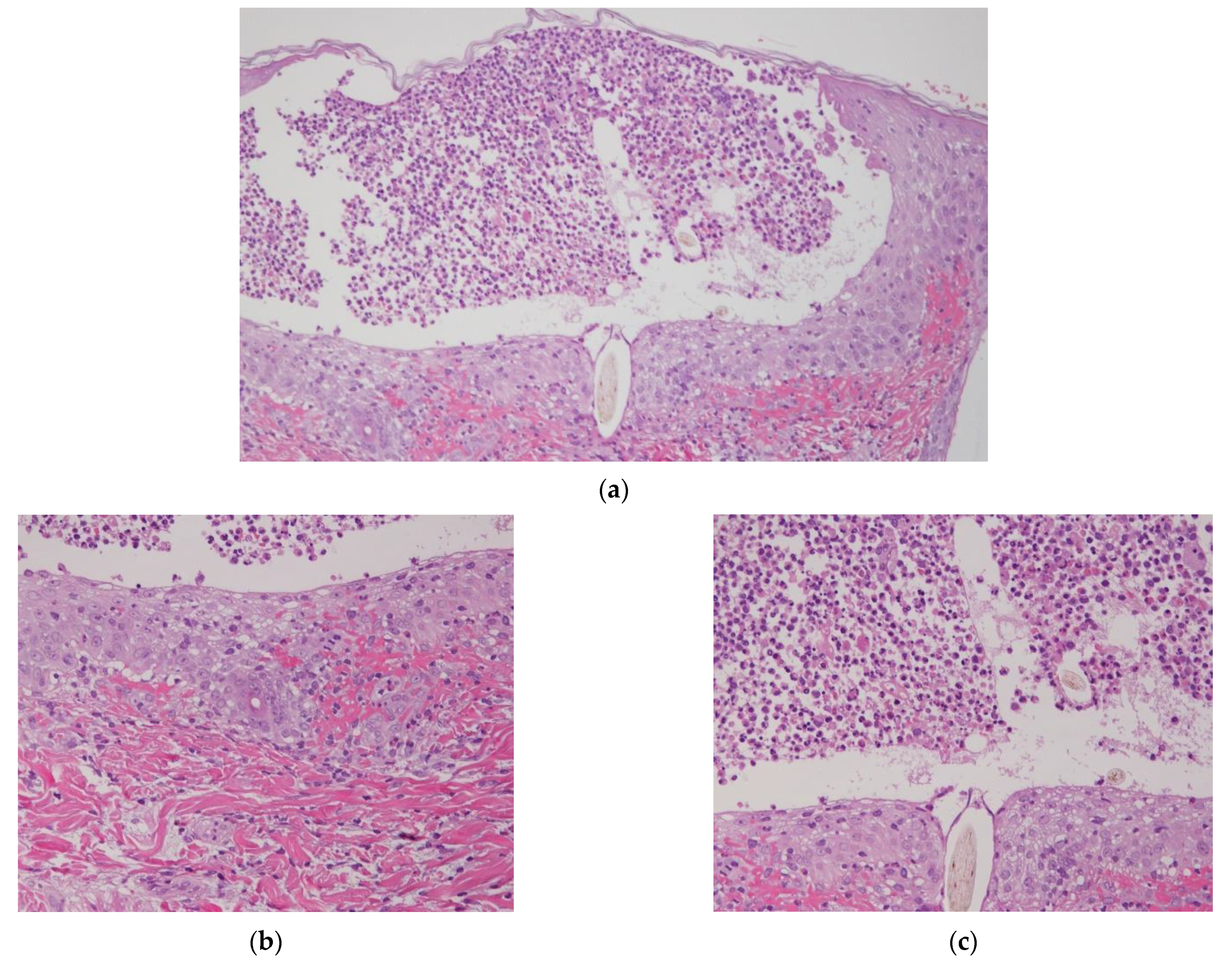
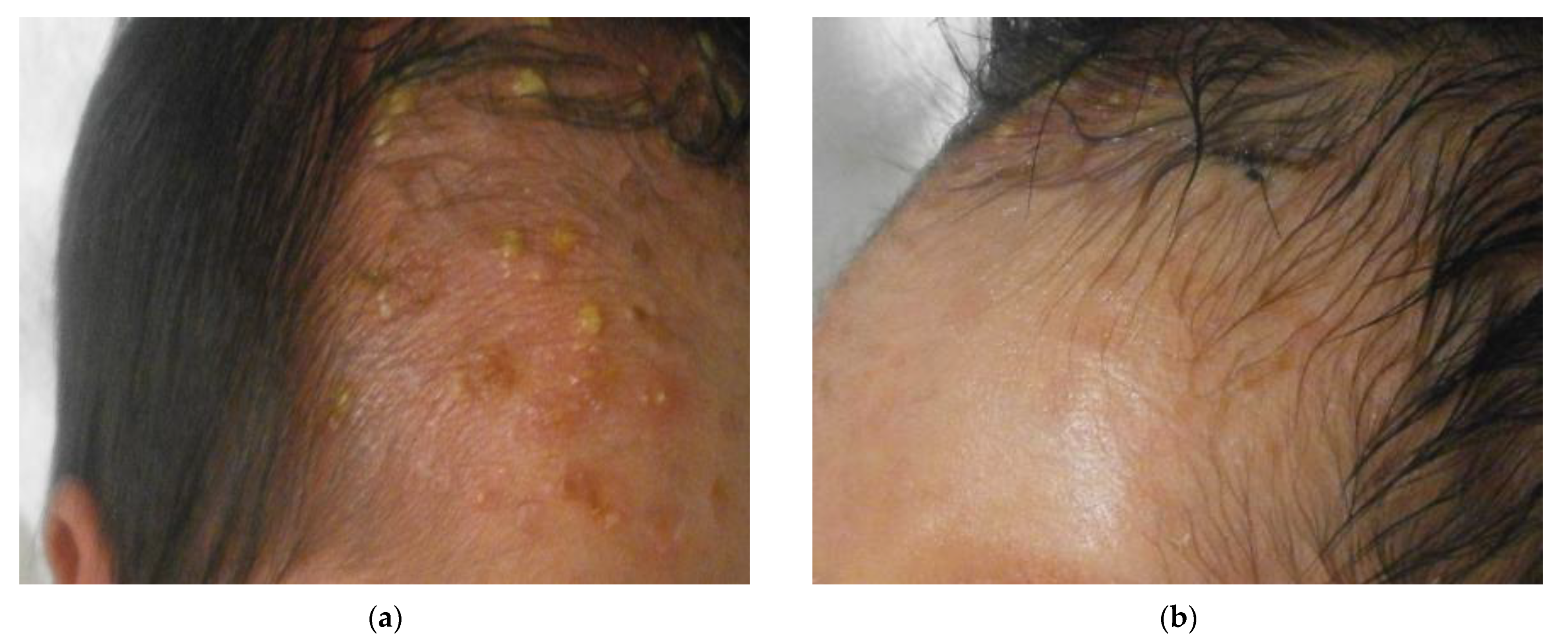
2. Case Presentation
3. Discussion
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghosh, S. Neonatal Pustular Dermatosis: An Overview. Indian J. Dermatol. 2015, 60, 211. [Google Scholar] [PubMed]
- Hidano, A.; Purwoko, R.; Jitsukawa, K. Statistical Survey of Skin Changes in Japanese Neonates. Pediatr. Dermatol. 1986, 3, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Reginatto, F.P.; de Villa, D.; Muller, F.M.; Peruzzo, J.; Peres, L.P.; Steglich, R.B.; Cestari, T.F. Prevalence and characterization of neonatal skin disorders in the first 72h of life. J Pediatr. 2017, 93, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K. Erythema toxicum neonatorum present at birth. J. Singap. Paediatr. Soc. 1986, 28, 163–166. [Google Scholar]
- Marchini, G.; Nelson, A.; Edner, J.; Lonne-Rahm, S.; Stavreus-Evers, A.; Hultenby, K.; Stavr, A. Erythema Toxicum Neonatorum Is an Innate Immune Response to Commensal Microbes Penetrated into the Skin of the Newborn Infant. Pediatr. Res. 2005, 58, 613–616. [Google Scholar] [CrossRef] [PubMed]
- van Praag, M.C.; van Rooij, R.W.; Folkers, E.; Spritzer, R.; Menke, H.E.; Oranje, A.P. Diagnosis and treatment of pustular disorders in the neonate. Pediatr Dermatol. 1997, 14, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Wyre, H.W.; Murphy, M.O. Transient neonatal pustular melanosis. Arch. Dermatol. 1979, 115, 458. [Google Scholar] [CrossRef] [PubMed]
- Merlob, P.; Metzker, A.; Reisner, S.H. Transient Neonatal Pustular Melanosis. Arch. Pediatr. Adolesc. Med. 1982, 136, 521. [Google Scholar] [CrossRef] [PubMed]
- Ferrándiz, C.; Coroleu, W.; Ribera, M.; Lorenzo, J.; Natal, A. Sterile Transient Neonatal Pustulosis Is a Precocious Form of Erythema toxicum neonatorum. Dermatology 1992, 185, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Lucky, A.W.; Esterly, N.B.; Heskel, N.; Krafchik, B.R.; Solomon, L.M. Eosinophilic pustular folliculitis in infancy. Pediatr. Dermatol. 1984, 1, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Buckley, D.A.; Munn, S.E.; Higgins, E.M. Neonatal eosinophilic pustular folliculitis. Clin. Exp. Dermatol. 2001, 26, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Asgari, M.; Leiferman, K.M.; Piepkorn, M.; Kuechle, M.K. Neonatal eosinophilic pustulosis*. Int. J. Dermatol. 2004, 45, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Hashida, Y.; Higuchi, T.; Nakajima, S.; Nakajima, K.; Ujihara, T.; Kabashima, K.; Sano, S.; Daibata, M. Human Polymavirus 6 Detected in Cases of Eosinophilic Pustular Folliculitis. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kang, J.H.; Cho, B.K.; Park, H.J. Generalized Eosinophilic Pustular Folliculitis of Infancy Responding to Hy-droxyzine. Ann. Dermatol. 2015, 27, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Ooi, C.G.; Walker, P.; Sidhu, S.K.; Gordon, L.A.; Marshman, G. Allopurinol induced generalized eosinophilic pustular fol-liculitis. Australas. J. Dermatol. 2006, 47, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Ezoe, K.; Yokozeki, H.; Katayama, I.; Nishioka, K. A case of eosinophilic pustular folliculitis (Ofuji’s disease) in-duced by patch and challenge tests with indeloxazine hydrochloride. J. Dermatol. 1996, 23, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Izumi, Y.; Hidaka, Y.; Tada, H.; Takano, T.; Kashiwai, T.; Tatsumi, K.-I.; Ichihara, K.; Amino, N. Simple and practical parameters for differentiation between destruction-induced thyrotoxicosis and Graves’ thyrotoxicosis. Clin. Endocrinol. 2002, 57, 51–58. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, S.; Yatsuzuka, K.; Chigyo, K.; Kuroo, Y.; Takemoto, K.; Sayama, K. A Case of Eosinophilic Pustular Folliculitis since Birth. Children 2021, 8, 30. https://doi.org/10.3390/children8010030
Yoshida S, Yatsuzuka K, Chigyo K, Kuroo Y, Takemoto K, Sayama K. A Case of Eosinophilic Pustular Folliculitis since Birth. Children. 2021; 8(1):30. https://doi.org/10.3390/children8010030
Chicago/Turabian StyleYoshida, Satoshi, Kazuki Yatsuzuka, Kenji Chigyo, Yuta Kuroo, Koji Takemoto, and Koji Sayama. 2021. "A Case of Eosinophilic Pustular Folliculitis since Birth" Children 8, no. 1: 30. https://doi.org/10.3390/children8010030
APA StyleYoshida, S., Yatsuzuka, K., Chigyo, K., Kuroo, Y., Takemoto, K., & Sayama, K. (2021). A Case of Eosinophilic Pustular Folliculitis since Birth. Children, 8(1), 30. https://doi.org/10.3390/children8010030