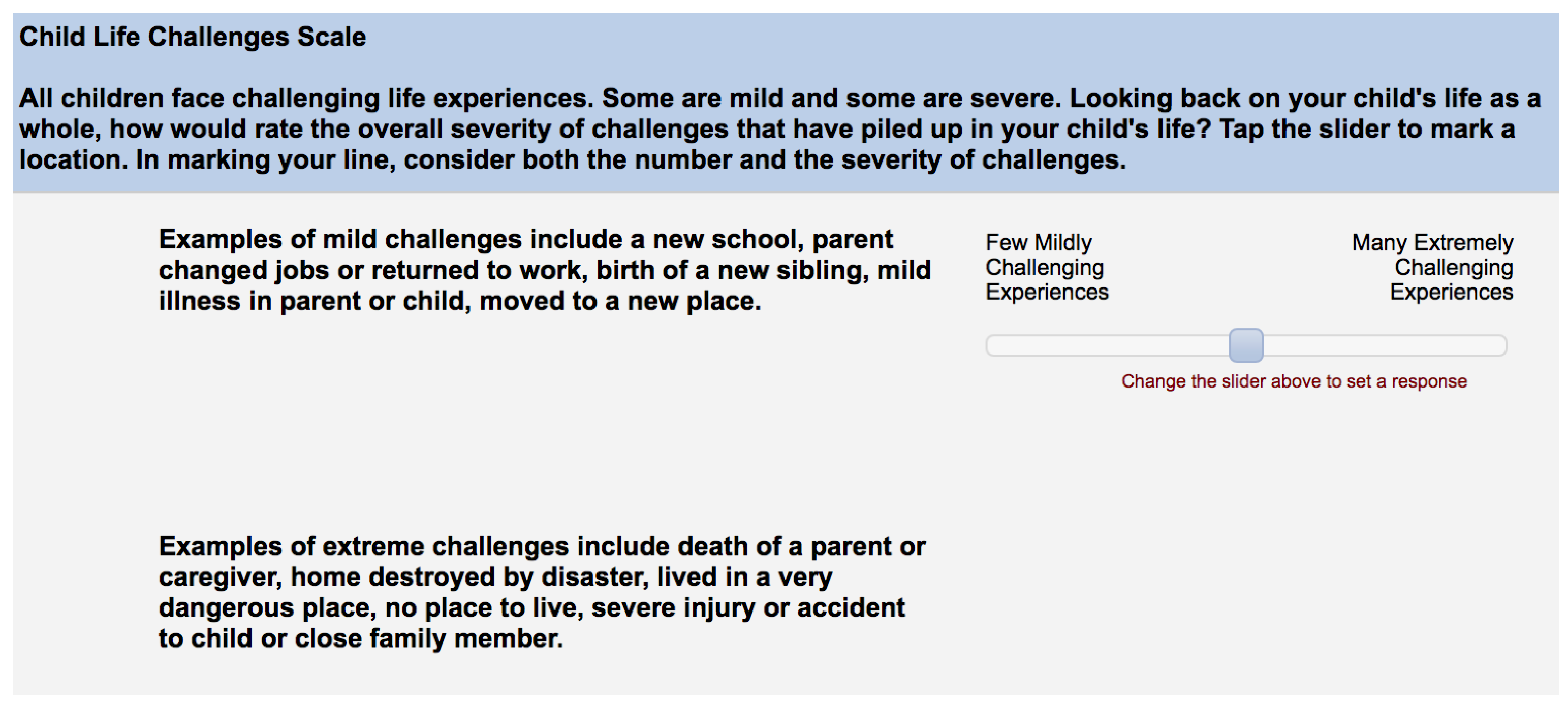
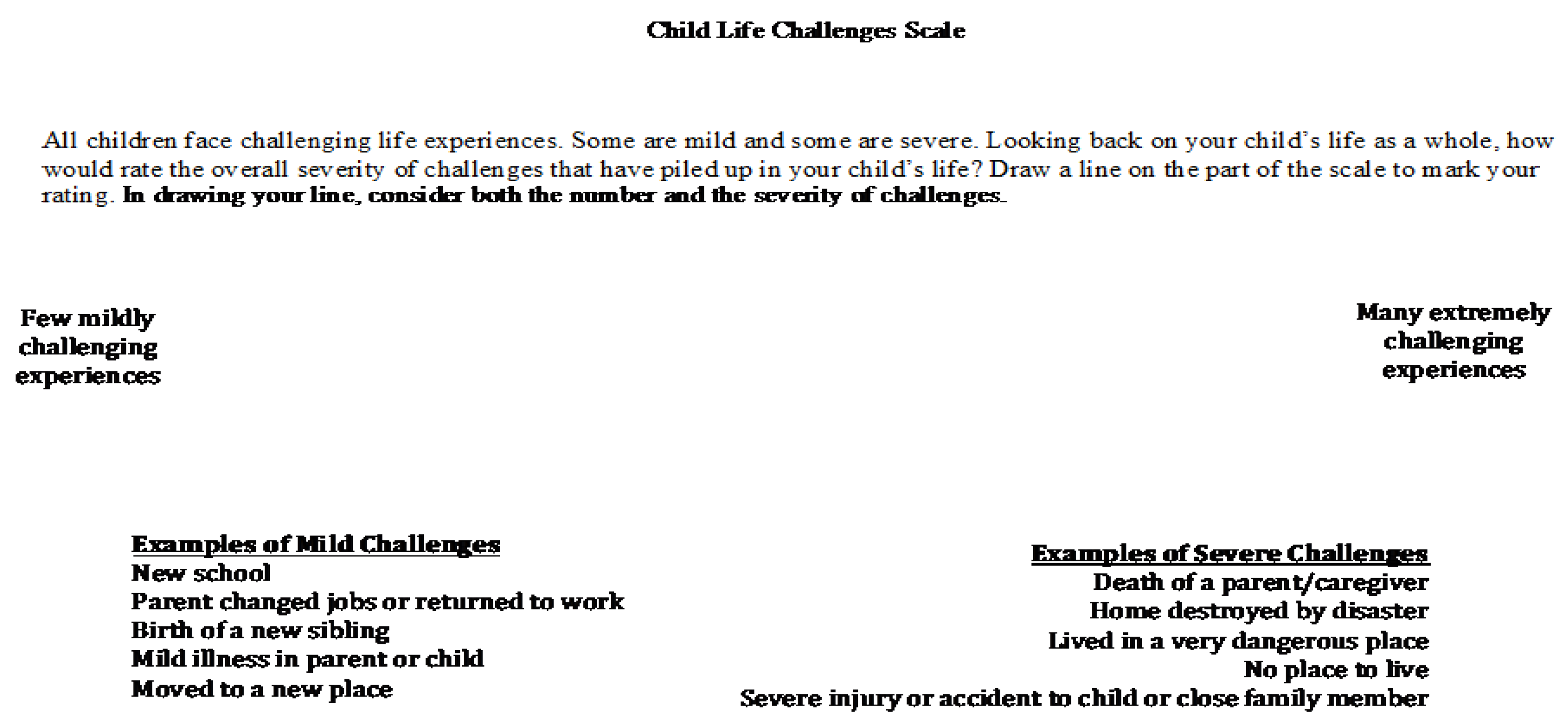
The Child Life Challenges Scale (CLCS): Associations of a Single-Item Rating of Global Child Adversity with Children’s Total Life Stressors and Parents’ Childhood Adversity

 , and
, and 
Abstract
1. Introduction
The Present Study
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analytic Plan and Missing Data
3. Results
4. Discussion
4.1. Strengths, Limitations, and Future Directions
4.2. Implications and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shonkoff, J.P.; Garner, A.S.; Siegel, B.S.; Dobbins, M.I.; Earls, M.F.; McGuinn, L.; Pascoe, J.; Wood, D.L.; Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care. The Lifelong Effects of Early Childhood Adversity and Toxic Stress. Pediatrics 2012, 129, e232–e246. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, E.G.; Thompson, R.; Litrownik, A.J.; Theodore, A.; English, D.J.; Black, M.M.; Wike, T.; Whimper, L.; Runyan, D.K.; Dubowitz, H. Effect of Early Childhood Adversity on Child Health. Arch. Pediatrics Adolesc. Med. 2006, 160, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, E.G.; Thompson, R.; Dubowitz, H.; Harvey, E.M.; English, D.J.; Proctor, L.J.; Runyan, D.K. Adverse Childhood Experiences and Child Health in Early Adolescence. JAMA Pediatrics 2013, 167, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Schilling, E.A.; Aseltine, R.H.; Gore, S. The Impact of Cumulative Childhood Adversity on Young Adult Mental Health: Measures, Models, and Interpretations. Soc. Sci. Med. 2008, 66, 1140–1151. [Google Scholar] [CrossRef] [PubMed]
- Adverse Childhood Experiences (ACEs). Available online: https://www.cdc.gov/violenceprevention/childabuseandneglect/acestudy/ (accessed on 20 December 2019).
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 2019, 56, 774–786. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.; Flaherty, E.G.; English, D.J.; Litrownik, A.J.; Dubowitz, H.; Kotch, J.B.; Runyan, D.K. Trajectories of Adverse Childhood Experiences and Self-Reported Health at Age 18. Acad. Pediatrics 2015, 15, 503–509. [Google Scholar] [CrossRef]
- Janus, M.; Duku, E. The School Entry Gap: Socioeconomic, Family, and Health Factors Associated with Children’s School Readiness to Learn. Early Educ. Dev. 2007, 18, 375–403. [Google Scholar] [CrossRef]
- Johnson, J.G.; Cohen, P.; Gould, M.S.; Kasen, S.; Brown, J.; Brook, J.S. Childhood Adversities, Interpersonal Difficulties, and Risk for Suicide Attempts during Late Adolescence and Early Adulthood. Arch. Gen. Psychiatry 2002, 59, 741–749. [Google Scholar] [CrossRef]
- Hughes, K.; Lowey, H.; Quigg, Z.; Bellis, M.A. Relationships between Adverse Childhood Experiences and Adult Mental Well-Being: Results from an English National Household Survey. BMC Public Health 2016, 16, 222. [Google Scholar] [CrossRef]
- Mersky, J.P.; Topitzes, J.; Reynolds, A.J. Impacts of Adverse Childhood Experiences on Health, Mental Health, and Substance Use in Early Adulthood: A Cohort Study of an Urban, Minority Sample in the US. Child Abus. Negl. 2013, 37, 917–925. [Google Scholar] [CrossRef]
- Metzler, M.; Merrick, M.T.; Klevens, J.; Ports, K.A.; Ford, D.C. Adverse Childhood Experiences and Life Opportunities: Shifting the Narrative. Child. Youth Serv. Rev. 2017, 72, 141–149. [Google Scholar] [CrossRef]
- Labella, M.H.; Johnson, W.F.; Martin, J.; Ruiz, S.K.; Shankman, J.L.; Englund, M.M.; Collins, W.A.; Roisman, G.I.; Simpson, J.A. Multiple Dimensions of Childhood Abuse and Neglect Prospectively Predict Poorer Adult Romantic Functioning. Personal. Soc. Psychol. Bull. 2018, 44, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Narayan, A.J.; Englund, M.M.; Carlson, E.A.; Egeland, B. Adolescent Conflict as a Developmental Process in the Prospective Pathway from Exposure to Interparental Violence to Dating Violence. J. Abnorm. Child Psychol. 2014, 42, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Narayan, A.J.; Englund, M.M.; Egeland, B. Developmental Timing and Continuity of Exposure to Interparental Violence and Externalizing Behavior as Prospective Predictors of Dating Violence. Dev. Psychopathol. 2013, 25, 973–990. [Google Scholar] [CrossRef]
- Belsky, J.; Conger, R.; Capaldi, D.M. The Intergenerational Transmission of Parenting: Introduction to the Special Section. Dev. Psychol. 2009, 45, 1201. [Google Scholar] [CrossRef]
- Labella, M.H.; Raby, K.L.; Martin, J.; Roisman, G.I. Romantic Functioning Mediates Prospective Associations between Childhood Abuse and Neglect and Parenting Outcomes in Adulthood. Dev. Psychopathol. 2019, 31, 95–111. [Google Scholar] [CrossRef]
- Chung, E.K.; Mathew, L.; Rothkopf, A.C.; Elo, I.T.; Coyne, J.C.; Culhane, J.F. Parenting Attitudes and Infant Spanking: The Influence of Childhood Experiences. Pediatrics 2009, 124, e278–e286. [Google Scholar] [CrossRef]
- Narayan, A.J.; Kalstabakken, A.W.; Labella, M.H.; Nerenberg, L.S.; Monn, A.R.; Masten, A.S. Intergenerational Continuity of Adverse Childhood Experiences in Homeless Families: Unpacking Exposure to Maltreatment versus Family Dysfunction. Am. J. Orthopsychiatry 2017, 87, 3. [Google Scholar] [CrossRef]
- Evans, G.W.; Li, D.; Whipple, S.S. Cumulative Risk and Child Development. Psychol. Bull. 2013, 139, 1342. [Google Scholar] [CrossRef]
- Obradović, J.; Shaffer, A.; Masten, A.S. The Cambridge Handbook of Environment in Human Development; Cambridge University Press: Cambridge, UK, 2012; pp. 35–57. [Google Scholar]
- Goodman, L.A.; Corcoran, C.; Turner, K.; Yuan, N.; Green, B.L. Assessing Traumatic Event Exposure: General Issues and Preliminary Findings for the Stressful Life Events Screening Questionnaire. J. Trauma. Stress Off. Publ. Int. Soc. Trauma. Stress Stud. 1998, 11, 521–542. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S.; Miliotis, D.; Graham-Bermann, S.A.; Ramirez, M.; Neemann, J. Children in Homeless Families: Risks to Mental Health and Development. J. Consult. Clin. Psychol. 1993, 61, 335. [Google Scholar] [CrossRef]
- Berens, A.E.; Kumar, S.; Tofail, F.; Jensen, S.K.G.; Alam, M.; Haque, R.; Kakon, S.H.; Petri, W.A.; Nelson, C.A. Cumulative Psychosocial Risk and Early Child Development: Validation and Use of the Childhood Psychosocial Adversity Scale in Global Health Research. Pediatric Res. 2019, 86, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Life Stressor Checklist—Revised. Available online: https://www.ptsd.va.gov/professional/assessment/documents/LSC-R.pdf (accessed on 20 December 2019).
- Coddington, R.D. The Significance of Life Events as Etiologic Factors in the Diseases of Children: I. A Survey of Professional Workers. J. Psychosom. Res. 1972, 16, 205–213. [Google Scholar] [CrossRef]
- Masten, A.S.; Garmezy, N.; Tellegen, A.; Pellegrini, D.S.; Larkin, K.; Larsen, A. Competence and Stress in School Children: The Moderating Effects of Individual and Family Qualities. J. Child Psychol. Psychiatry 1988, 29, 745–764. [Google Scholar] [CrossRef]
- Greenwald, R.; Rubin, A. Assessment of Posttraumatic Symptoms in Children: Development and Preliminary Validation of Parent and Child Scales. Res. Soc. Work Pract. 1999, 9, 61–75. [Google Scholar] [CrossRef]
- Traumatic Events Screening Inventory—Parent Report Revised—Long Version. Available online: http://www.icctc.org/PMM%20Handouts/TESI-prr-final1.pdf (accessed on 20 December 2019).
- Johnson, J.H.; McCutcheon, S.M. Assessing life stress in older children and adolescents: Preliminary findings with the Life Events Checklist. Stress Anxiety 1980, 7, 111–125. [Google Scholar]
- Masten, A.S.; Neemann, J.; Andenas, S. Life Events and Adjustment in Adolescents: The Significance of Event Independence, Desirability, and Chronicity. J. Res. Adolesc. 1994, 4, 71–97. [Google Scholar] [CrossRef]
- Realmuto, G.M.; Masten, A.; Carole, L.F.; Hubbard, J.; Groteluschen, A.; Chhun, B. Adolescent Survivors of Massive Childhood Trauma in Cambodia: Life Events and Current Symptoms. J. Trauma. Stress 1992, 5, 589–599. [Google Scholar] [CrossRef]
- Evans, G.W.; Kim, P. Multiple Risk Exposure as a Potential Explanatory Mechanism for the Socioeconomic Status–Health Gradient. Ann. N. Y. Acad. Sci. 2010, 1186, 174–189. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary Magic: Resilience Processes in Development. Am. Psychol. 2001, 56, 227. [Google Scholar] [CrossRef]
- Sameroff, A. The Jacobs Foundation Series on Adolescence. Families Count: Effects on Child and Adolescent Development; Cambridge University Press: Cambridge, UK, 2006; pp. 15–36. [Google Scholar]
- Sameroff, A.J.; Seifer, R.; Barocas, R.; Zax, M.; Greenspan, S. Intelligence Quotient Scores of 4-Year-Old Children: Social-Environmental Risk Factors. Pediatrics 1987, 79, 343–350. [Google Scholar] [PubMed]
- Schmidt, M.R.; Narayan, A.J.; Atzl, V.M.; Rivera, L.M.; Lieberman, A.F. Childhood Maltreatment on the Adverse Childhood Experiences (Aces) Scale versus the Childhood Trauma Questionnaire (Ctq) in a Perinatal Sample. J. Aggress. Maltreatment Trauma 2018. [Google Scholar] [CrossRef]
- Jaffe, A.E.; DiLillo, D.; Hoffman, L.; Haikalis, M.; Dykstra, R.E. Does It Hurt to Ask? A Meta-Analysis of Participant Reactions to Trauma Research. Clin. Psychol. Rev. 2015, 40, 40–56. [Google Scholar] [CrossRef]
- Johnson, L.E.; Benight, C.C. Effects of Trauma-focused Research on Recent Domestic Violence Survivors. J. Trauma. Stress Off. Publ. Int. Soc. Trauma. Stress Stud. 2003, 16, 567–571. [Google Scholar] [CrossRef]
- Newman, E.; Kaloupek, D.G. The Risks and Benefits of Participating in Trauma-focused Research Studies. J. Trauma. Stress Off. Publ. Int. Soc. Trauma. Stress Stud. 2004, 17, 383–394. [Google Scholar] [CrossRef]
- Carlson, E.B.; Newman, E.; Daniels, J.W.; Armstrong, J.; Roth, D.; Loewenstein, R. Distress in Response to and Perceived Usefulness of Trauma Research Interviews. J. Trauma Dissociation 2003, 4, 131–142. [Google Scholar] [CrossRef]
- Disch, E. Research as Clinical Practice: Creating a Positive Research Experience for Survivors of Sexual Abuse by Professionals. Sociol. Pract. 2001, 3, 221–239. [Google Scholar] [CrossRef]
- Newman, E.; Risch, E.; Kassam-Adams, N. Ethical Issues in Trauma-Related Research: A Review. J. Empir. Res. Hum. Res. Ethics 2006, 1, 29–46. [Google Scholar] [CrossRef] [PubMed]
- DePrince, A.P.; Freyd, J.J. Costs and Benefits of Being Asked about Trauma History. J. Trauma Pract. 2006, 3, 23–35. [Google Scholar] [CrossRef]
- Goldstein, E.; Athale, N.; Sciolla, A.F.; Catz, S.L. Patient Preferences for Discussing Childhood Trauma in Primary Care. Perm. J. 2017, 21, 16–55. [Google Scholar] [CrossRef] [PubMed]
- Newman, E.; Walker, E.A.; Gefland, A. Assessing the Ethical Costs and Benefits of Trauma-Focused Research. Gen. Hosp. Psychiatry 1999, 21, 187–196. [Google Scholar] [CrossRef]
- Walker, E.A.; Newman, E.; Koss, M.; Bernstein, D. Does the Study of Victimization Revictimize the Victims? Gen. Hosp. Psychiatry 1997, 19, 403–410. [Google Scholar] [CrossRef]
- Barnes, A.J.; Anthony, B.J.; Karatekin, C.; Lingras, K.A.; Mercado, R.; Thompson, L.A. Identifying Adverse Childhood Experiences in Pediatrics to Prevent Chronic Health Conditions. Pediatric Res. 2019, 87, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.; Woodward, A.; Swenson, S.; Weis, C.; Gunderson, M.; Deling, M.; Cristiani, V.; Lynch, B. Parents’ Adverse Childhood Experiences and Mental Health Screening Using Home Visiting Programs: A Pilot Study. Public Health Nurs. 2017, 34, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, L.; Savageau, J.A.; Candib, L.M.; Reed, G.W.; Fletcher, K.E.; Hargraves, J.L. Screening for Childhood Trauma in Adult Primary Care Patients: A Cross-Sectional Survey. Prim. Care Companion J. Clin. Psychiatry 2010, 12. [Google Scholar] [CrossRef]
- Kerker, B.D.; Storfer-Isser, A.; Szilagyi, M.; Stein, R.E.; Garner, A.S.; O’Connor, K.G.; Hoagwood, K.E.; Horwitz, S.M. Do Pediatricians Ask about Adverse Childhood Experiences in Pediatric Primary Care? Acad. Pediatrics 2016, 16, 154–160. [Google Scholar] [CrossRef]
- Kalmakis, K.A.; Chandler, G.E.; Roberts, S.J.; Leung, K. Nurse Practitioner Screening for Childhood Adversity among Adult Primary Care Patients: A Mixed-method Study. J. Am. Assoc. Nurse Pract. 2017, 29, 35–45. [Google Scholar] [CrossRef]
- Tink, W.; Tink, J.C.; Turin, T.C.; Kelly, M. Adverse Childhood Experiences: Survey of Resident Practice, Knowledge, and Attitude. Fam. Med. 2017, 49, 7–13. [Google Scholar]
- Addressing Adverse Childhood Experiences and Other Types of Trauma in the Primary Care Setting. Available online: https://www.aap.org/en-us/Documents/ttb_addressing_aces.pdf (accessed on 20 December 2019).
- Cohen, J.A.; Kelleher, K.J.; Mannarino, A.P. Identifying, Treating, and Referring Traumatized Children: The Role of Pediatric Providers. Arch. Pediatrics Adolesc. Med. 2008, 162, 447–452. [Google Scholar] [CrossRef]
- Garner, A.S.; Shonkoff, J.P.; Siegel, B.S.; Dobbins, M.I.; Earls, M.F.; McGuinn, L.; Pascoe, J.; Wood, D.L.; Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care. Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science into Lifelong Health. Pediatrics 2012, 129, e224–e231. [Google Scholar] [PubMed]
- Glowa, P.T.; Olson, A.L.; Johnson, D.J. Screening for Adverse Childhood Experiences in a Family Medicine Setting: A Feasibility Study. J. Am. Board Fam. Med. 2016, 29, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Merrick, J.S.; Labella, M.; Desjardins, C.D.; Barnes, A.; Masten, A.S. Child Life Challenges Scale: Evidence of Validity as a Lifetime Adversity Measure; Society for Research on Child Development: Austin, TX, USA, 2017. [Google Scholar]
- Cohodes, E.; Hagan, M.; Narayan, A.; Lieberman, A. Matched Trauma: The Role of Parents’ and Children’s Shared History of Childhood Domestic Violence Exposure in Parents’ Report of Children’s Trauma-Related Symptomatology. J. Trauma Dissociation 2016, 17, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Colman, I.; Kingsbury, M.; Garad, Y.; Zeng, Y.; Naicker, K.; Patten, S.; Jones, P.; Wild, T.; Thompson, A. Consistency in Adult Reporting of Adverse Childhood Experiences. Psychol. Med. 2016, 46, 543–549. [Google Scholar] [CrossRef]
- Masten, A.S.; Kalstabakken, A.W. APA Handbook of Psychopathology: Child and Adolescent Psychopathology; American Psychological Association: Washington, DC, USA, 2018; Volume 2, pp. 15–36. [Google Scholar]
- Mcewen, B.; Wingfield, J. Allostasis and Allostatic Load. Encycl. Stress 2007, 1, 135–141. [Google Scholar]
- Masten, A.S.; Hubbard, J.J.; Gest, S.D.; Tellegen, A.; Garmezy, N.; Ramirez, M. Competence in the Context of Adversity: Pathways to Resilience and Maladaptation from Childhood to Late Adolescence. Dev. Psychopathol. 1999, 11, 143–169. [Google Scholar] [CrossRef]
- Dube, S.R.; Anda, R.F.; Felitti, V.J.; Chapman, D.P.; Williamson, D.F.; Giles, W.H. Childhood Abuse, Household Dysfunction, and the Risk of Attempted Suicide throughout the Life Span: Findings from the Adverse Childhood Experiences Study. JAMA 2001, 286, 3089–3096. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E. Screening for Serious Mental Illness in the General Population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Cook, R.D.; Weisberg, S. Residuals and Influence in Regression; Chapman and Hall: New York, NY, USA, 1982. [Google Scholar]
- Rawlings, J.O. Applied Regression Analysis: A Research Tool; Wadsworth & Brooks: Pacific Grove, CA, USA, 1988. [Google Scholar]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- Schafer, J.L.; Graham, J.W. Missing Data: Our View of the State of the Art. Psychol. Methods 2002, 7, 147. [Google Scholar] [CrossRef]
- Willis, G.B. Cognitive Interviewing: A Tool for Improving Questionnaire Design; Sage Publications: Thousand Oaks, CA, USA, 2004. [Google Scholar]
- Stover, C.S.; Hahn, H.; Im, J.J.; Berkowitz, S. Agreement of Parent and Child Reports of Trauma Exposure and Symptoms in the Early Aftermath of a Traumatic Event. Psychol. Trauma Theory Res. Pract. Policy 2010, 2, 159–168. [Google Scholar] [CrossRef]
- Sullivan, M.M.; Fiat, A.E.; Merrick, J.S.; Labella, M.H.; Nelson, K.M.; Masten, A.E. Validity of the Life Challenges Scale: A Single-Item Scale to Assess Lifetime Adversity. In Proceedings of the Annual Meeting of the Society for Prevention Research, San Diego, CA, USA, 30 May 2019. [Google Scholar]



{kind=link}
{kind=link}
| Primary Variable | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Child Life Challenges Scale (CLCS)—tablet version | -- | ||||
| 2. Children’s total life stressors | 0.44 ** | -- | |||
| 3. Total parental ACEs | 0.29 * | 0.35 ** | -- | ||
| 4. Total parental distress | −0.13 | −0.39 ** | −0.26 * | -- | |
| 5. Child age | −0.04 | 0.21 | 0.05 | 0.07 | -- |
| Child Life Challenges Scale | ||||||
|---|---|---|---|---|---|---|
| B | SE | ß | R2 | F | ∆R2 | |
| Step 1 | 0.12 | 1.74 | 0.12 | |||
| Total parental ACEs | 2.38 | 1.07 | 0.27 * | |||
| Total parental distress | −0.84 | 0.66 | −0.16 | |||
| Child age | −2.14 | 4.17 | −0.06 | |||
| Child sex | 1.81 | 6.66 | 0.03 | |||
| Parent education | 0.16 | 6.84 | 0.00 | |||
| Step 2 | 0.27 | 3.74 ** | 0.15 ** | |||
| Total parental ACEs | 1.28 | 1.04 | 0.15 | |||
| Total parental distress | −0.06 | 0.65 | −0.01 | |||
| Child age | −4.29 | 3.89 | −0.13 | |||
| Child sex | 4.29 | 6.18 | 0.08 | |||
| Parent education | −2.32 | 6.34 | −0.04 | |||
| Children’s total life stressors | 3.23 | 0.93 | 0.45 ** | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merrick, J.S.; Labella, M.H.; Narayan, A.J.; Desjardins, C.D.; Barnes, A.J.; Masten, A.S. The Child Life Challenges Scale (CLCS): Associations of a Single-Item Rating of Global Child Adversity with Children’s Total Life Stressors and Parents’ Childhood Adversity. Children 2020, 7, 33. https://doi.org/10.3390/children7040033
Merrick JS, Labella MH, Narayan AJ, Desjardins CD, Barnes AJ, Masten AS. The Child Life Challenges Scale (CLCS): Associations of a Single-Item Rating of Global Child Adversity with Children’s Total Life Stressors and Parents’ Childhood Adversity. Children. 2020; 7(4):33. https://doi.org/10.3390/children7040033
Chicago/Turabian StyleMerrick, Jillian S., Madelyn H. Labella, Angela J. Narayan, Christopher D. Desjardins, Andrew J. Barnes, and Ann S. Masten. 2020. "The Child Life Challenges Scale (CLCS): Associations of a Single-Item Rating of Global Child Adversity with Children’s Total Life Stressors and Parents’ Childhood Adversity" Children 7, no. 4: 33. https://doi.org/10.3390/children7040033
APA StyleMerrick, J. S., Labella, M. H., Narayan, A. J., Desjardins, C. D., Barnes, A. J., & Masten, A. S. (2020). The Child Life Challenges Scale (CLCS): Associations of a Single-Item Rating of Global Child Adversity with Children’s Total Life Stressors and Parents’ Childhood Adversity. Children, 7(4), 33. https://doi.org/10.3390/children7040033