Video Modeling and Social Skills Learning in ASD-HF

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedures and Tasks
3. Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); Psychiatric Association: Arlington, VA, USA, 2013; pp. 1–947. [Google Scholar]
- Wang, S.-Y.; Cui, Y.; Parrila, R. Examining the effectiveness of peer-mediated and video-modeling social skills interventions for children with autism spectrum disorders: A meta-analysis in single-case research using HLM. Res. Autism Spectr. Disord. 2011, 5, 562–569. [Google Scholar] [CrossRef]
- Lawrence, D.H.; Alleckson, D.A.; Bjorklund, P. Beyond the Roadblocks: Transitioning to Adulthood With Asperger’s Disorder. Arch. Psychiatr. Nurs. 2010, 24, 227–238. [Google Scholar] [CrossRef]
- Bass, J.D.; Mulick, J.A. Social play skill enhancement of children with autism using peers and siblings as therapists. Psychol. Sch. 2007, 44, 727–735. [Google Scholar] [CrossRef]
- Matson, J.L.; Matson, M.L.; Rivet, T.T. Social-skills treatments for children with autism spectrum disorders: An overview. Behav. Modif. 2007, 31, 682–707. [Google Scholar] [CrossRef] [PubMed]
- Nikopoulos, C.; Keenan, M. Effects of video modeling on social initiations by children with autism. J. Appl. Behav. Anal. 2004, 37, 93–96. [Google Scholar] [CrossRef]
- Scattone, D. Social skills interventions for children with autism. Psychol. Sch. 2007, 44, 717–726. [Google Scholar] [CrossRef]
- Rayner, C.; Denholm, C.; Sigafoos, J. Video-based intervention for individuals with autism: Key questions that remain unanswered. Res. Autism Spectr. Disord. 2009, 3, 291–303. [Google Scholar] [CrossRef]
- Charlop, M.H.; Milstein, J.P. Teaching Autistic Children Conversational Speech Using Video Modeling. J. Appl. Behav. Anal. 1989, 22, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Sherer, M.; Pierce, K.L.; Paredes, S.; Kisacky, K.L.; Ingersoll, B.; Schreibman, L. Enhancing conversation skills in children with autism via video technology: Which is better,“self” or “other” as a model? Behav. Modif. 2001, 25, 140–158. [Google Scholar] [CrossRef]
- Apple, A.; Billingsley, F.; Schwartz, I. Effects of video modeling alone and with self-management on compliment-giving behaviours of children with highfunctioning ASD. J. Posit. Behav. Interv. 2005, 7, 33–46. [Google Scholar] [CrossRef]
- Gena, A.; Couloura, S.; Kymissis, E. Modifying the affective behaviour of preschoolers with autism using in-vivo or video modeling and reinforcement contingencies. J. Autism Dev. Disord. 2005, 35, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Nikopoulos, C.K.; Keenan, M. Promoting social initiation in children with autism using video modeling. Behav. Interv. 2003, 18, 87–108. [Google Scholar] [CrossRef]
- Wert, B.Y.; Neisworth, J.T. Effects of Video Self-Modeling on Spontaneous Requesting in Children with Autism. J. Posit. Behav. Interv. 2003, 5, 30–34. [Google Scholar] [CrossRef]
- Buggey, T. Video Self-Modeling Applications With Students With Autism Spectrum Disorder in a Small Private School Setting. Focus Autism Other Dev. Disabil. 2005, 20, 52–63. [Google Scholar] [CrossRef]
- Bellini, S.; Akullian, J. A Meta-Analysis of Video Modeling and Video Self-Modeling Interventions for Children and Adolescents with Autism Spectrum Disorders. Except. Child. 2007, 73, 264–287. [Google Scholar] [CrossRef]
- Hayes, G.R.; Custodio, V.E.; Haimson, O.L.; Nguyen, K.; Ringland, K.E.; Ulgado, R.R.; Waterhouse, A.; Weiner, R. Mobile video modeling for employment interviews for individuals with autism. J. Vocat. Rehabilitation 2015, 43, 275–287. [Google Scholar] [CrossRef]
- Williams, J.H.; Whiten, A.; Singh, T. A Systematic Review of Action Imitation in Autistic Spectrum Disorder. J. Autism Dev. Disord. 2004, 34, 285–299. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Belmonte, M.K. AUTISM: A Window Onto the Development of the Social and the Analytic Brain. Annu. Rev. Neurosci. 2005, 28, 109–126. [Google Scholar] [CrossRef]
- Gallese, V.; Migone, P.; Eagle, M.N. La simulazione incarnata: I neuroni specchio, le basi neurofisiologiche dell’intersoggettività ed alcune implicazioni per la psicoanalisi. Psicoterapia e Scienze Umane. 2006, 40, 543–580. [Google Scholar]
- Cattaneo, L.; Fabbri-Destro, M.; Boria, S.; Pieraccini, C.; Monti, A.; Cossu, G.; Rizzolatti, G. Impairment of actions chains in autism and its possible role in intention understanding. Proc. Natl. Acad. Sci. USA 2007, 104, 17825–17830. [Google Scholar] [CrossRef]
- Frolli, A.; ILa Penna Cavallaro, A.; Ricci, M.C. Theory of Mind: Autism and Typical Developmental. Acad. J. Ped. Neonatol. 2019, 8, 555799. [Google Scholar] [CrossRef]
- Orsini, A.; Pezzuti, L.; Picone, L. WISC-IV: Contributo alla taratura Italiana; Giunti O. S. Organizzazioni Specialib: Florence, Italy, 2012; pp. 1–140. [Google Scholar]
- IBM to Acquire SPSS Inc. to Provide Clients Predictive Analytics Capabilities. Available online: https://newsroom.ibm.com/2009-07-28-IBM-to-Acquire-SPSS-Inc-to-Provide-Clients-Predictive-Analytics-Capabilities (accessed on 28 August 2020).
- Wong, C.; Odom, S.L.; Hume, K.A.; Cox, A.W.; Fettig, A.; Kucharczyk, S.; Brock, M.E.; Plavnick, J.B.; Fleury, V.P.; Schultz, T.R. Evidence-Based Practices for Children, Youth, and Young Adults with Autism Spectrum Disorder: A Comprehensive Review. J. Autism Dev. Disord. 2015, 45, 1951–1966. [Google Scholar] [CrossRef] [PubMed]
- Delano, M. Video Modeling Interventions for Individuals with Autism. Remedial Spéc. Educ. 2007, 28, 33–42. [Google Scholar] [CrossRef]
- Wang, P.; Spillane, A. Evidence-based social skills interventions for children with autism: A meta-analysis. Educ. Train. Dev. Disabil. 2009, 44, 318–342. [Google Scholar]
- McCoy, K.; Hermansen, E. Video Modeling for Individuals with Autism: A Review of Model Types and Effects. Educ. Treat. Child. 2007, 30, 183–213. [Google Scholar] [CrossRef]
- Chartrand, T.L.; van Baaren, R. Human mimicry. Adv. Exp. Soc. Psychol. 2009, 41, 219–274. [Google Scholar]
- Heyes, C.M. What’s social about social learning? J. Comp. Psychol. 2012, 126, 193–202. [Google Scholar] [CrossRef]
- Van Baaren, R.; Janssen, L.; Chartrand, T.L.; Dijksterhuis, A. Where is the love? The social aspects of mimicry. Philos. Trans. R. Soc. B: Biol. Sci. 2009, 364, 2381–2389. [Google Scholar] [CrossRef] [PubMed]
- Rizzolatti, G.; Fadiga, L.; Gallese, V.; Fogassi, L. Premotor cortex and the recognition of motor actions. Cogn. Brain Res. 1996, 3, 131–141. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Craighero, L. THE MIRROR-NEURON SYSTEM. Annu. Rev. Neurosci. 2004, 27, 169–192. [Google Scholar] [CrossRef]
- Iacoboni, M.; Dapretto, M. The mirror neuron system and the consequences of its dysfunction. Nat. Rev. Neurosci. 2006, 7, 942–951. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, L.; Rizzolatti, G. The Mirror Neuron System. Arch. Neurol. 2009, 66, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Rizzolatti, G.; Fabbri-Destro, M.; Cattaneo, L. Mirror neurons and their clinical relevance. Nat. Clin. Pr. Neurol. 2009, 5, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Rizzolatti, G.; Sinigaglia, C. The functional role of the parieto-frontal mirror circuit: Interpretations and misinterpretations. Nat. Rev. Neurosci. 2010, 11, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Perkins, T.; Stokes, M.; McGillivray, J.; Bittar, R. Mirror neuron dysfunction in autism spectrum disorders. J. Clin. Neurosci. 2010, 17, 1239–1243. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.S.; Oberman, L.M. Broken Mirrors: A Theory of Autism. Sci. Am. 2006, 295, 62–69. [Google Scholar] [CrossRef]
- Raymaekers, R.; Wiersema, J.R.; Roeyers, H. EEG study of the mirror neuron system in children with high functioning autism. Brain Res. 2009, 1304, 113–121. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Fabbri-Destro, M. Mirror neurons: From discovery to autism. Exp. Brain Res. 2010, 200, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Iacoboni, M.; Molnar-Szakacs, I.; Gallese, V.; Buccino, G.; Mazziotta, J.C.; Rizzolatti, G. Grasping the intentions of others with one’s own mirror neuron system. PLoS Biol. 2005, 3, e79. [Google Scholar] [CrossRef] [PubMed]
- Gowen, E.; Poliakoff, E. How does visuomotor priming differ for biological and non-biological stimuli? A review of the evidence. Psychol. Res. 2012, 76, 407–420. [Google Scholar] [CrossRef]
- Klapper, A.; Ramsey, R.; Wigboldus, D.; Cross, E.S. The Control of Automatic Imitation Based on Bottom–Up and Top–Down Cues to Animacy: Insights from Brain and Behavior. J. Cogn. Neurosci. 2014, 26, 2503–2513. [Google Scholar] [CrossRef] [PubMed]
- Brass, M.; Heyes, C. Imitation: Is cognitive neuroscience solving the correspondence problem? Trends Cogn. Sci. 2005, 9, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Liepelt, R.; Brass, M. Top-Down Modulation of Motor Priming by Belief About Animacy. Exp. Psychol. 2010, 57, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Longo, M.R.; Bertenthal, B.I. Attention modulates the specificity of automatic imitation to human actors. Exp. Brain Res. 2008, 192, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.C.; Brass, M. Does the human motor system simulate Pinocchio’s actions? Coacting with a human hand versus a wooden hand in a dyadic interaction. Psychol. Sci. 2007, 18, 1058–1062. [Google Scholar] [CrossRef]
- Oberman, L.M.; Ramachandran, V.S.; Pineda, J.A. Modulation of mu suppression in children with autism spectrum disorders in response to familiar or unfamiliar stimuli: The mirror neuron hypothesis. Neuropsychologia 2008, 46, 1558–1565. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maintain a Conversation with a Peer | |
|---|---|
| (1) Keep ocular contact during the conversation | 0 = The subject does not maintain eye contact during the conversation 1 = The subject uses eye contact but in an inflexible way or in a limited number of exchanges 2 = The subject uses eye contact flexibly and during all conversational exchanges |
| (2) Direct facial expressions, such as a smile, frown, or other expressions consistent with the above, to show interest | 0 = The subject does not express interest in what was said in the conversation through facial expressions 1 = The subject directs other facial expressions in a limited or exaggerated way or uses only some facial expressions (e.g., smiles in hands is contextual, but does not use expressions to express disappointment, sadness, etc.) 2 = The subject uses a wide range of facial expressions in a flexible and coherent way with the speech |
| (3) Answer several hectares on the turn taking during conversation | 0 = The subject is unable to respect the conversational rules, for example speaking while the other is completing the speech or responding only after long pauses 1 = The subject occasionally uses non-verbal elements that allow him to understand conversational exchanges 2 = The subject can read the main forms of non-verbal communication to regulate conversational shifts |
| (4) Provide additional comments or ask questions related to what the interlocutor said | 0 = The subject does not continue with comments or questions what the interlocutor said 1 = The subject provides additional comments on an occasional basis or not always in context with what was said by the interlocutor 2 = The subject provides additional comments or shows interest in what the interlocutor said with coherent questions. |
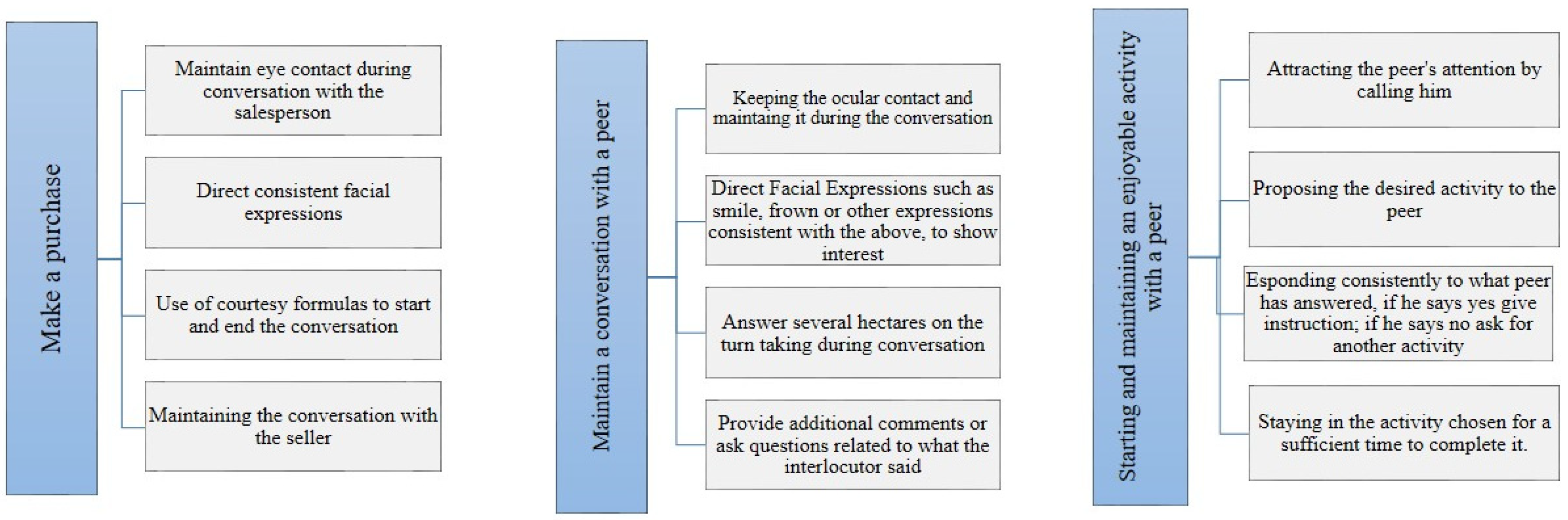
| Interacting with a salesperson while making a purchase |
|
| Initiating and maintaining a conversation with peers |
|
| Starting and maintaining an enjoyable activity with a peer |
|
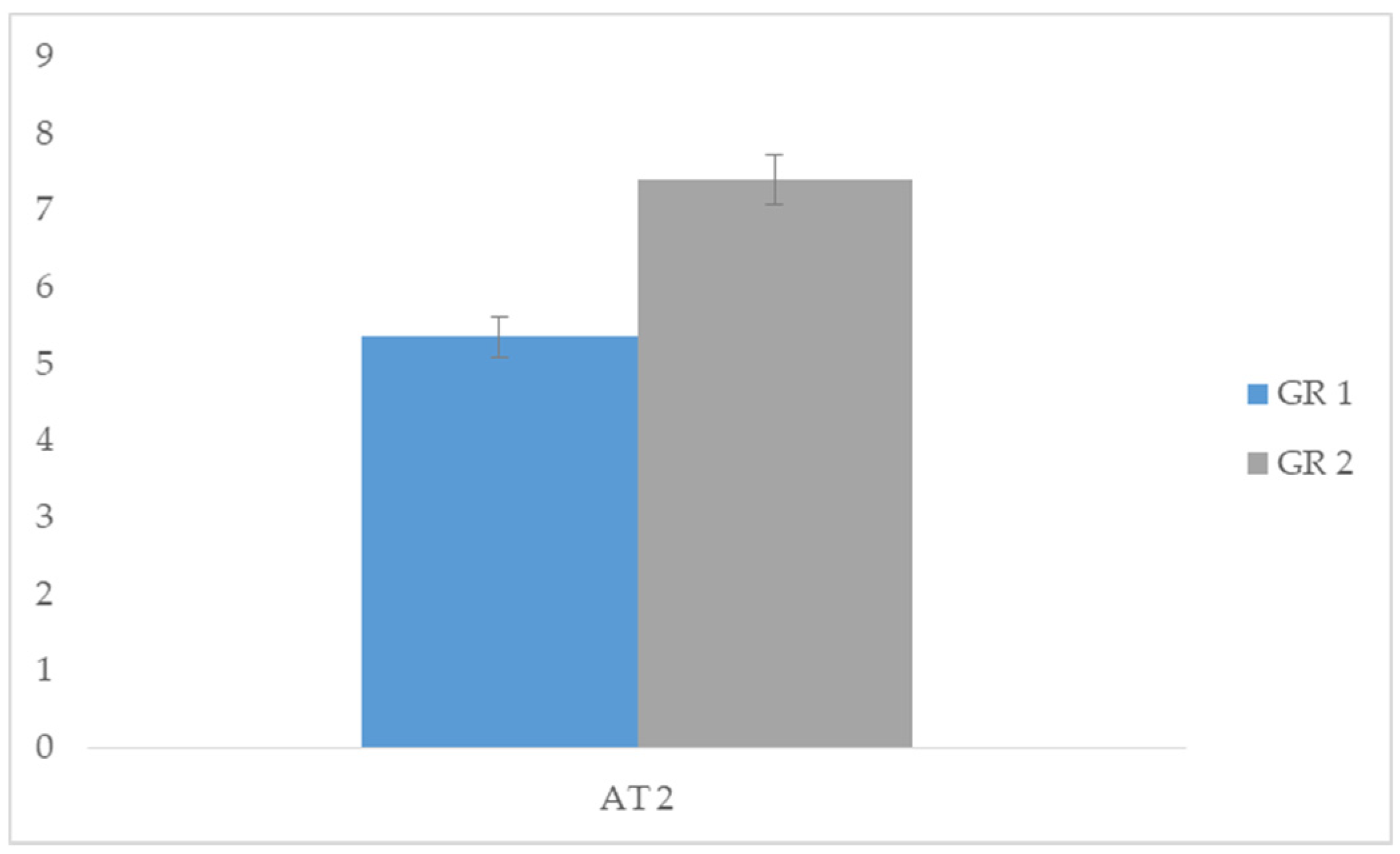
| Group 1 | Group 2 | |||||
|---|---|---|---|---|---|---|
| Means | SD | Means | SD | t | p | |
| AT 1 | 3.35 | 0.489 | 5.50 | 0.513 | −11.831 | 0.000 * |
| AT 2 | 5.35 | 0.489 | 7.40 | 0.503 | −11.105 | 0.000 * |
| AT 3 | 7.25 | 0.444 | 9.45 | 0.510 | −14.139 | 0.000 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frolli, A.; Ricci, M.C.; Bosco, A.; Lombardi, A.; Cavallaro, A.; Operto, F.F.; Rega, A. Video Modeling and Social Skills Learning in ASD-HF. Children 2020, 7, 279. https://doi.org/10.3390/children7120279
Frolli A, Ricci MC, Bosco A, Lombardi A, Cavallaro A, Operto FF, Rega A. Video Modeling and Social Skills Learning in ASD-HF. Children. 2020; 7(12):279. https://doi.org/10.3390/children7120279
Chicago/Turabian StyleFrolli, Alessandro, Maria Carla Ricci, Antonia Bosco, Agnese Lombardi, Antonella Cavallaro, Francesca Felicia Operto, and Angelo Rega. 2020. "Video Modeling and Social Skills Learning in ASD-HF" Children 7, no. 12: 279. https://doi.org/10.3390/children7120279
APA StyleFrolli, A., Ricci, M. C., Bosco, A., Lombardi, A., Cavallaro, A., Operto, F. F., & Rega, A. (2020). Video Modeling and Social Skills Learning in ASD-HF. Children, 7(12), 279. https://doi.org/10.3390/children7120279