Establishing Raw Acceleration Thresholds to Classify Sedentary and Stationary Behaviour in Children

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometrics
2.3. Sedentary Behaviour
2.3.1. Calibration Study Protocol
2.3.2. Free-Living Protocol
2.4. Accelerometers
2.5. Data Reduction
2.6. Data Analysis
3. Results
3.1. Description of the Population
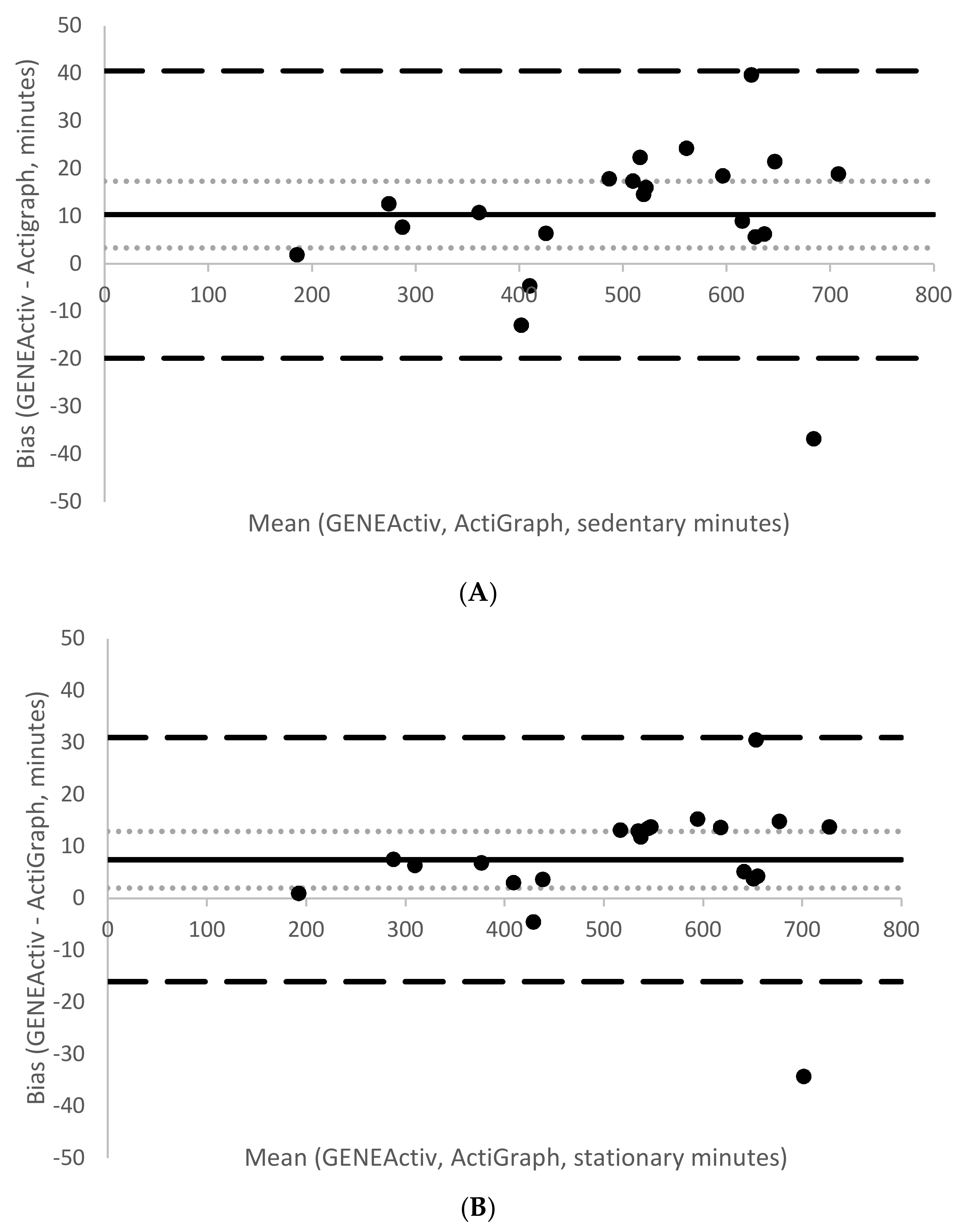
3.2. Comparison of Activities, Accelerometer Brands and Placements
3.3. Threshold Generation
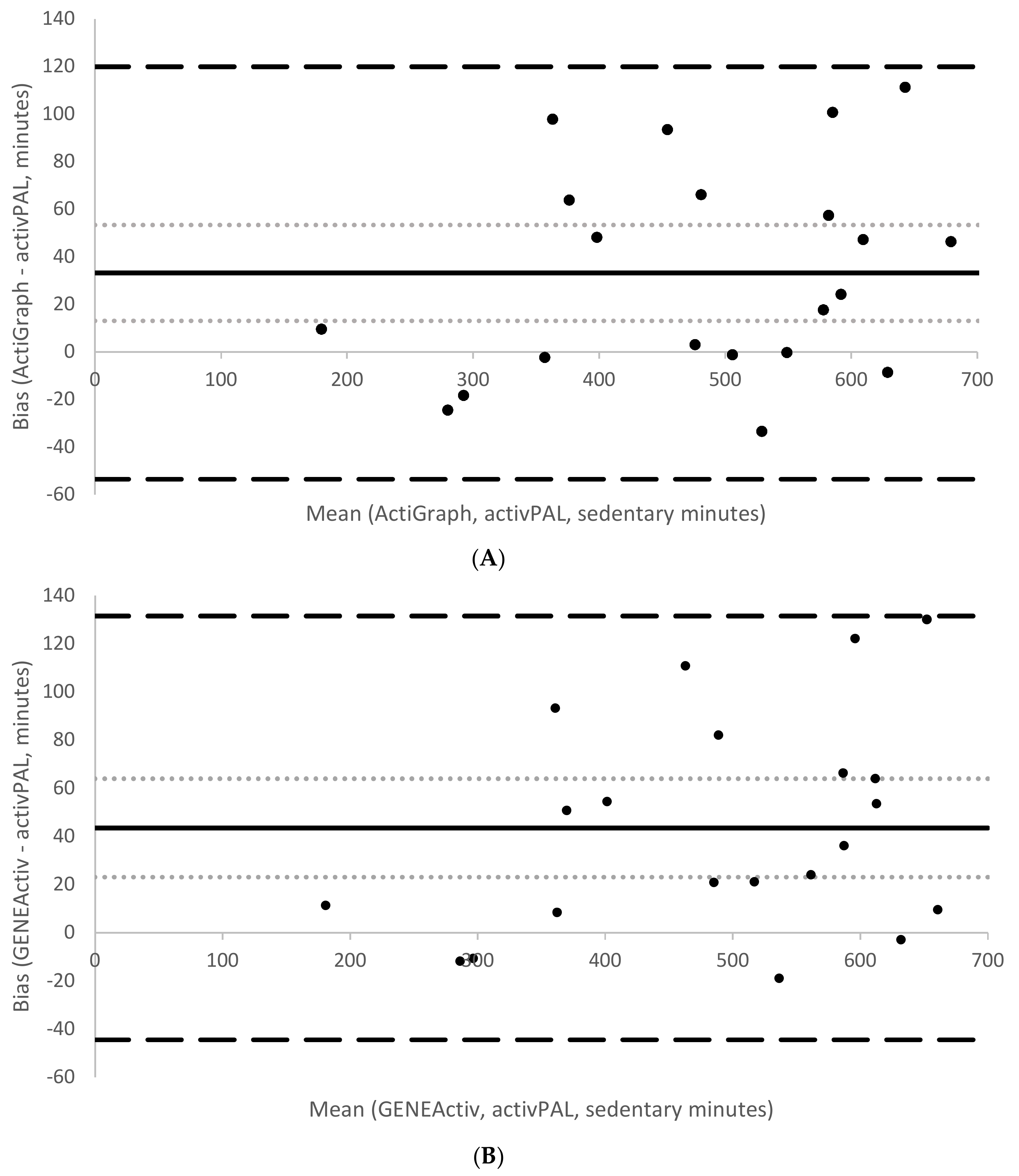
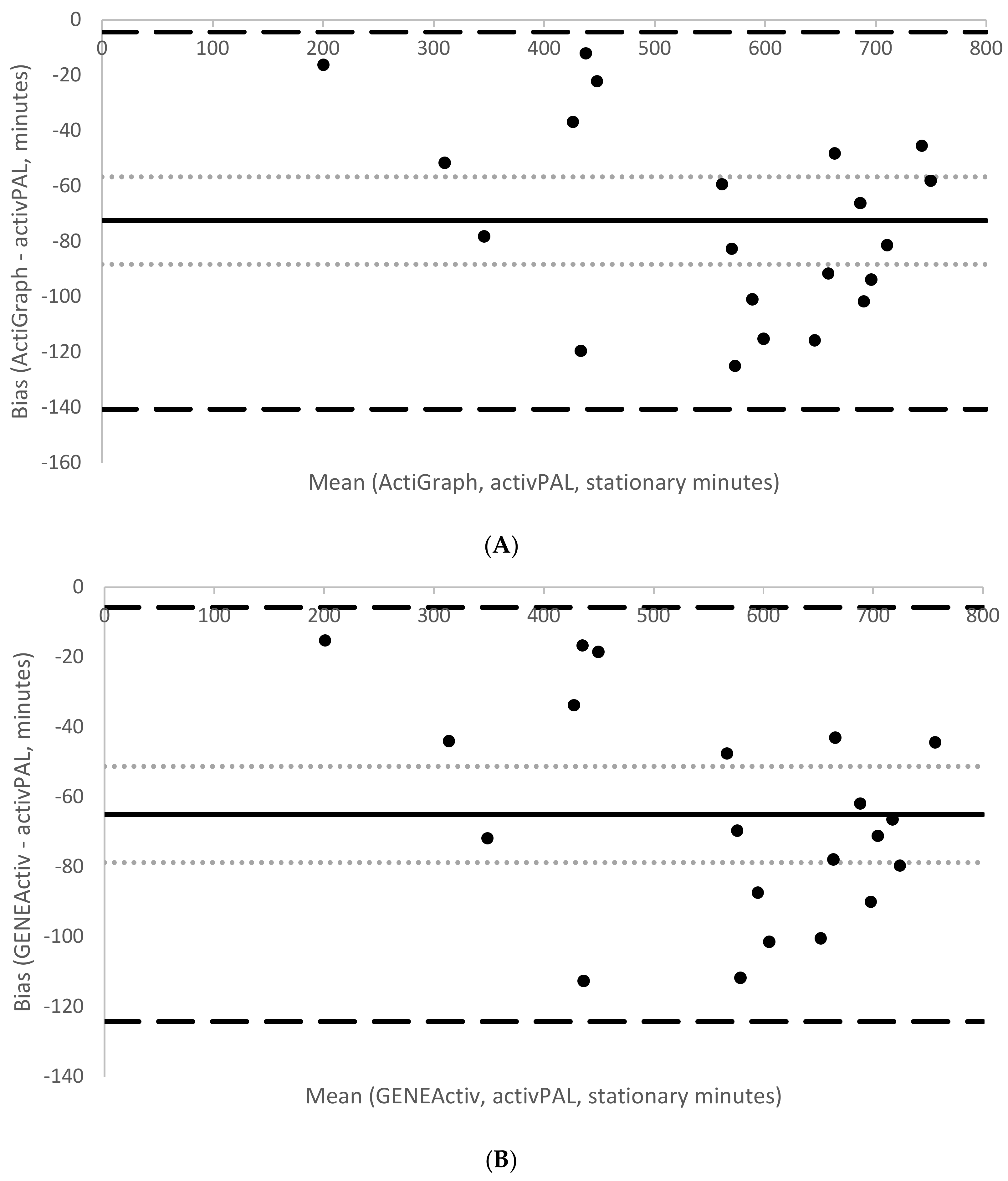
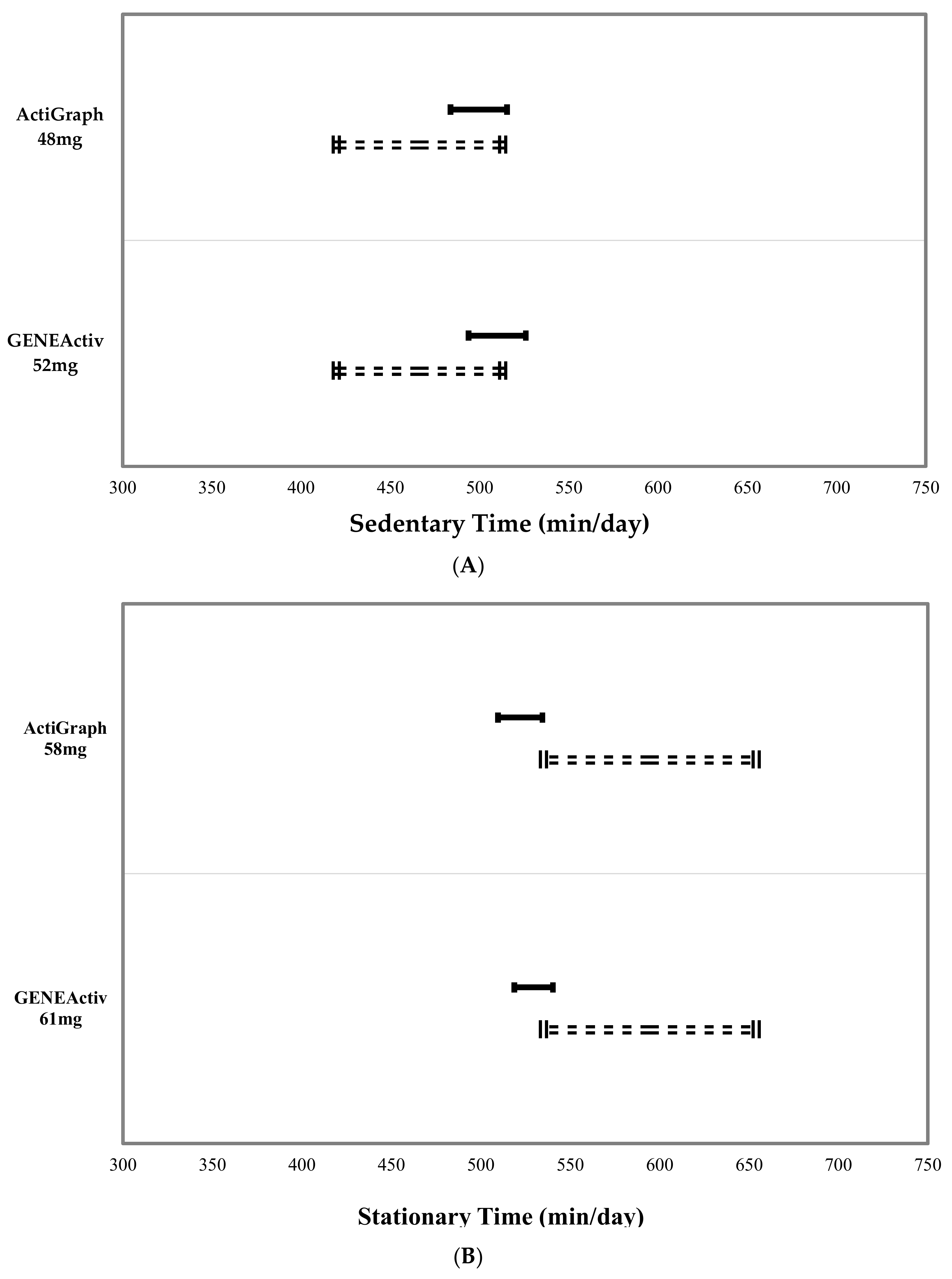
3.4. Validation of Thresholds during Free-Living Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Biddle, S.J.H. Sedentary behavior. Am. J. Prev. Med. 2007, 33, 502–504. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; O’Neill, J.R.; Lobelo, F. The evolving definition of “sedentary”. Exerc. Sport Sci. Rev. 2008, 36, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Kim, Y.; Welk, G.J.; Gaesser, G.A. Kids are not little adults: What MET threshold captures sedentary behavior in children? Eur. J. Appl. Physiol. 2016, 116, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Salmon, J.; Ridley, K.; O’Connell, E.; Arundell, L.; Timperio, A. Agreement between activPAL and ActiGraph for assessing children’s sedentary time. Int. J. Behav. Nutr. Phys. 2012, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.P.; Hedge, A.; Yates, T.; Copeland, R.J.; Loosemore, M.; Hamer, M.; Bradley, G.; Dunstan, D.W. The sedentary office: An expert statement on the growing case for change towards better health and productivity. Br. J. Sports Med. 2015, 49, 1357–1362. [Google Scholar] [CrossRef]
- Coombs, N.A.; Stamatakis, E. Associations between objectively assessed and questionnaire-based sedentary behaviour with BMI-defined obesity among general population children and adolescents living in England. BMJ Open 2015, 5, e007172. [Google Scholar] [CrossRef]
- Salmon, J.; Tremblay, M.S.; Marshall, S.J.; Hume, C. Health risks, correlates, and interventions to reduce sedentary behavior in young people. Am. J. Prev. Med. 2011, 41, 197–206. [Google Scholar] [CrossRef]
- Martinez-Gomez, D.; Eisenmann, J.C.; Gomez-Martinez, S.; Veses, A.; Marcos, A.; Veiga, O.L. Sedentary behavior, adiposity and cardiovascular risk factors in adolescents. The AFINOS study. Rev. Esp. Cardiol. 2010, 63, 277–285. [Google Scholar] [CrossRef]
- Carson, V.; Janssen, I. Volume, patterns, and types of sedentary behavior and cardio-metabolic health in children and adolescents: A cross-sectional study. BMC Public Health 2011, 11, 274. [Google Scholar] [CrossRef]
- Rowlands, A.V. Accelerometer assessment of physical activity in children: An update. Pediatr. Exerc. Sci. 2007, 19, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Gorely, T.; Clemes, S.A.; Yates, T.; Edwardson, C.; Brage, S.; Salmon, J.; Marshall, S.J.; Biddle, S.J. Methods of measurement in epidemiology: Sedentary behaviour. Int. J. Epidemiol. 2012, 41, 1460–1471. [Google Scholar] [CrossRef] [PubMed]
- Hart, T.L.; McClain, J.J.; Tudor-Locke, C. Controlled and free-living evaluations of objective measures of sedentary and active behaviors. J. Phys. Act. Health 2011, 8, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Kozey-Keadle, S.; Libertine, A.; Lyden, K.; Staudenmayer, J.; Freedson, P.S. Validation of wearable monitors for assessing sedentary behavior. Med. Sci. Sports Exerc. 2011, 43, 1561–1567. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Olds, T.S.; Hillsdon, M.; Pulsford, R.; Hurst, T.L.; Eston, R.G.; Gomersall, S.R.; Johnston, K.; Langford, J. Assessing sedentary behavior with the GENEActiv: Introducing the sedentary sphere. Med. Sci. Sports Exerc. 2014, 46, 1235–1247. [Google Scholar] [CrossRef] [PubMed]
- Corder, K.; Ekelund, U.; Steele, R.M.; Wareham, N.J.; Brage, S. Assessment of physical activity in youth. J. Appl. Physiol. 2008, 105, 977–987. [Google Scholar] [CrossRef]
- Hildebrand, M.; Van Hees, V.T.; Hansen, B.H.; Ekelund, U. Age group comparability of raw accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sports Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Noonan, R.; Rowlands, A.V.; Van Hees, V.; Knowles, Z.; Boddy, L.M. Wear compliance and activity in children wearing wrist- and hip-mounted accelerometers. Med. Sci. Sports Exerc. 2016, 48, 245–253. [Google Scholar] [CrossRef]
- Esliger, D.W.; Rowlands, A.V.; Hurst, T.L.; Catt, M.; Murray, P.; Eston, R.G. Validation of the GENEA Accelerometer. Med. Sci. Sports Exerc. 2011, 43, 1085–1093. [Google Scholar] [CrossRef]
- Phillips, L.R.S.; Parfitt, G.; Rowlands, A.V. Calibration of the GENEA accelerometer for assessment of physical activity intensity in children. J. Sci. Med. Sport 2013, 16, 124–128. [Google Scholar] [CrossRef]
- Schaefer, C.A.; Nigg, C.R.; Hill, J.O.; Brink, L.A.; Browning, R.C. Establishing and evaluating wrist cutpoints for the GENEActiv accelerometer in youth. Med. Sci. Sports Exerc. 2014, 46, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Aittasalo, M.; Vaha-Ypya, H.; Vasankari, T.; Husu, P.; Jussila, A.M.; Sievanen, H. Mean amplitude deviation calculated from raw acceleration data: A novel method for classifying the intensity of adolescents’ physical activity irrespective of accelerometer brand. BMC Sports Sci. Med. Rehabil. 2015, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Vaha-Ypya, H.; Vasankari, T.; Husu, P.; Suni, J.; Sievanen, H. A universal, accurate intensity-based classification of different physical activities using raw data of accelerometer. Clin. Physiol. Funct. Imaging 2015, 35, 64–70. [Google Scholar] [CrossRef]
- Hildebrand, M.; Hansen, B.H.; van Hees, V.T.; Ekelund, U. Evaluation of raw acceleration sedentary thresholds in children and adults. Scand. J. Med. Sci. Sports 2016, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bakrania, K.; Yates, T.; Rowlands, A.V.; Esliger, D.W.; Bunnewell, S.; Sanders, J.; Davies, M.; Khunti, K.; Edwardson, C.L. Intensity thresholds on raw acceleration data: Euclidean Norm Minus One (ENMO) and Mean Amplitude Deviation (MAD) approaches. PLoS ONE 2016, 11, e0164045. [Google Scholar] [CrossRef] [PubMed]
- Boddy, L.M.; Noonan, R.J.; Kim, Y.; Rowlands, A.V.; Welk, G.J.; Knowles, Z.R.; Fairclough, S.J. Comparability of children’s sedentary time estimates derived from wrist worn GENEActiv and hip worn ActiGraph accelerometer thresholds. J. Sci. Med. Sport 2018. [Google Scholar] [CrossRef] [PubMed]
- Mirwald, R.L.; Baxter-Jones, D.G.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [PubMed]
- Van Hees, V.T.; Gorzelniak, L.; Dean Leon, E.C.; Eder, M.; Pias, M.; Taherian, S.; Ekelund, U.; Renstrom, F.; Franks, P.W.; Horsch, A.; et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE 2013, 8, e61691. [Google Scholar] [CrossRef]
- van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; da Silva, I.C.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef]
- Rowlands, A.V.; Yates, T.; Olds, T.S.; Davies, M.; Khunti, K.; Edwardson, C.L. Sedentary sphere: Wrist-worn accelerometer-brand independent posture classification. Med. Sci. Sports Exerc. 2016, 48, 748–754. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; p. 413. [Google Scholar]
- Perkins, N.J.; Schisterman, E.F. The inconsistency of “optimal” cutpoints obtained using two criteria based on the receiver operating characteristic curve. Am. J. Epidemiol. 2006, 163, 670–675. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- DeShaw, K.J.; Ellingson, L.; Bai, Y.; Lansing, J.; Perez, M.; Welk, G. Methods for Activity Monitor Validation Studies: An Example with the Fitbit Charge. J. Meas. Phys. Behav. 2018, 1, 130–135. [Google Scholar] [CrossRef]
- Noonan, R.J.; Boddy, L.M.; Kim, Y.; Knowles, Z.R.; Fairclough, S.J. Comparison of children’s free-living physical activity derived from wrist and hip raw accelerations during the segmented week. J. Sports Sci. 2016, 35, 2067–2072. [Google Scholar] [CrossRef]
- Welk, G.J.; Corbin, C.B.; Dale, D. Measurement issues in the assessment of physical activity in children. Res. Q. Exerc. Sport 2000, 71, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Cliff, D.P.; Fairclough, S.J.; Boddy, L.M.; Olds, T.S.; Parfitt, G.; Noonan, R.J.; Downs, S.J.; Knowles, Z.R.; Beets, M.W. Moving forward with backward compatibility: Translating wrist accelerometer data. Med. Sci. Sports Exerc. 2016, 48, 2142–2149. [Google Scholar] [CrossRef] [PubMed]
- Crouter, S.E.; Flynn, J.I.; Bassett, D.R., Jr. Estimating physical activity in youth using a wrist accelerometer. Med. Sci. Sports Exerc. 2015, 47, 944–951. [Google Scholar] [CrossRef]
- John, D.; Sasaki, J.; Staudenmayer, J.; Mavilia, M.; Freedson, P.S. Comparison of raw acceleration from the GENEA and ActiGraph GT3X+ activity monitors. Sensors 2013, 13, 14754–14763. [Google Scholar] [CrossRef]
- Davies, G.; Reilly, J.J.; McGowan, A.J.; Dall, P.M.; Granat, M.H.; Paton, J.Y. Validity, practical utility, and reliability of the activPAL in preschool children. Med. Sci. Sport Exerc. 2012, 44, 761–768. [Google Scholar] [CrossRef]
- Rowlands, A.V.; Mirkes, E.M.; Yates, T.; Clemes, S.; Davies, M.; Khunti, K.; Edwardson, C.L. Accelerometer-assessed Physical Activity in Epidemiology: Are Monitors Equivalent? Med. Sci. Sports Exerc. 2017. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Station | Description |
|---|---|
| Resting | Lying on a soft gym mat, in a supine position, asked to avoid bodily movements. |
| TV viewing | Sitting comfortably on a couch, watching television. |
| Seated, tablet | Sitting comfortably on a couch, playing the Bike Race game on an iPad. |
| Seated, LEGO® | Sitting at a table, playing with LEGO®. |
| Seated, Homework | Sitting at a table, copying a piece of writing (mimicking homework). |
| Standing, phone | Standing while playing Subway Surf on a mobile phone. |
| Walking | Walking, at own pace, around a designated track. |
| Variable | Calibration Study (n = 27) | Free-Living Data (n = 21) |
|---|---|---|
| Age (years) | 10.2 (0.3) | 10.2 (0.3) |
| Stature (cm) | 141.5 (6.9) | 142.8 (7.4) |
| Sitting height (cm) | 70.9 (3.9) | 71.3 (3.3) |
| Waist circumference (cm) | 66.7 (10.9) | 70.3 (9.8) |
| Body mass (kg) | 37.3 (11.4) | 40.8 (10.6) |
| BMI (kg/m2) | 18.3 (3.9) | 19.8 (4) |
| Maturity offset (years) | -2.3 (1.1) | −2.1 (1) |
| APHV * (years) | 12.3 (1.1) | 12.3 (0.6) |
| Mean | 95% Confidence Interval | ||
|---|---|---|---|
| Activity | Acceleration (mg) | Lower Bound | Upper Bound |
| Walking | 190.7 | 188.4 | 193.0 |
| LEGO® | 31.0 | 30.6 | 31.4 |
| Seated, tablet | 20.5 | 20.0 | 21.0 |
| Resting | 19.6 | 19.0 | 20.2 |
| TV viewing | 15.0 | 14.5 | 15.5 |
| Standing, phone | 13.9 | 13.5 | 14.1 |
| Homework | 13.0 | 12.7 | 13.3 |
| Device | Resting | TV Viewing | Seated, Tablet | Standing, Phone | Seated, LEGO® | Seated, Homework | Walking |
|---|---|---|---|---|---|---|---|
| AG hip | 8.9 (12.4) * | 5.5 (7.7) * | 8.4 (8.6) * | 3.9 (8.1) * | 6.5 (8.0) * | 5.3 (8.5) * | 148.2 (51.5) * |
| AG Dom | 23.5 (34.1) †,# | 15.2 (27.7) | 21.5 (28.7) † | 16.7 (19.2) †,# | 32.8 (25.7) †,# | 13.5 (19.8) †,# | 178.0 (139.3) †,# |
| GA Dom | 18.0 (38.6) | 14.5 (33.2) | 21.4 (32.6) † | 14.8 (18.9) † | 36.6 (29.9) † | 19.0 (23.4) † | 183.1 (115.4) † |
| AG Ndom | 18.7 (36.1) | 15.8 (27.8) # | 18.6 (29.3) # | 12.0 (23.5) | 21.8 (27.6) # | 9.3 (19.1) # | 199.3 (131.0) |
| GA Ndom | 17.9 (36.4) | 14.4 (27.8) | 20.4 (30.8) | 11.9 (21.8) | 32.6 (31.6) | 10.2 (20.5) | 202.1 (129.3) |
| Sedentary Behaviour | Stationary Behaviour | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Device | Sensitivity (TPR *) | Specificity (TNR †) | AUC | 95% CI | Threshold (mg) | Sensitivity (TPR) | Specificity (TNR) | AUC | 95% CI | Threshold (mg) |
| AG hip | 97% | 51% | 0.746 | 0.743–0.75 | 32.6 | 94% | 86% | 0.944 | 0.942–0.946 | 32.6 |
| AG Dom | 89% | 55% | 0.759 | 0.756–0.762 | 55.6 | 86% | 87% | 0.926 | 0.924–0.928 | 55.2 |
| AG Ndom | 87% | 60% | 0.797 | 0.788–0.793 | 48.1 | 87% | 89% | 0.940 | 0.939–0.942 | 57.5 |
| GA Dom | 84% | 57% | 0.752 | 0.749–0.755 | 56.5 | 82% | 85% | 0.888 | 0.886–0.891 | 59.1 |
| GA Ndom | 87% | 57% | 0.77 | 0.768–0.773 | 51.6 | 86% | 85% | 0.918 | 0.916–0.920 | 60.7 |
| Criterion | Comparison | Mean (SD) Minutes | MPE (SD) | MAPE (SD) | Limits of Agreement (Lower to Upper) | 95% CI of Mean Biases (Lower to Upper) | Correlation | p Value | Equivalency Analysis (Minutes) |
|---|---|---|---|---|---|---|---|---|---|
| Sedentary time | |||||||||
| activPAL (sit/lie) | 466.3 (131.9) | Zone of Equivalence: 419.6–512.9 | |||||||
| ActiGraph (48 mg) | 499.5 (143.1) | −7.3% (10.5%) | 9.5% (8.5%) | from −54 to 120 | from 13 to 53 | 0.95 | 0.003 | 90% CI 483.6–515.3 | |
| GENEActiv (52 mg) | 509.8 (145.0) | −9.5% (10.1%) | 10.6% (8.8%) | from −44 to 132 | from 23 to 64 | 0.95 | <0.001 | 90% CI 493.8–525.9 | |
| Stationary time | |||||||||
| activPAL (sit/lie/stand) | 594.6 (161.2) | Zone of equivalence: 535.1–654 | |||||||
| ActiGraph (58 mg) | 522.1 (147.6) | 12.2% (5.6%) | 12.2% (5.6%) | from −141 to −4 | from −88 to −57 | 0.98 | <0.001 | 90% CI 509.6–534.5 | |
| GENEActiv (61 mg) | 529.6 (148.5) | 10.9% (4.9%) | 10.9% (4.9%) | from −124 to −6 | from −79 to −51 | 0.98 | <0.001 | 90% CI 518.7–540.4 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hurter, L.; Fairclough, S.J.; Knowles, Z.R.; Porcellato, L.A.; Cooper-Ryan, A.M.; Boddy, L.M. Establishing Raw Acceleration Thresholds to Classify Sedentary and Stationary Behaviour in Children. Children 2018, 5, 172. https://doi.org/10.3390/children5120172
Hurter L, Fairclough SJ, Knowles ZR, Porcellato LA, Cooper-Ryan AM, Boddy LM. Establishing Raw Acceleration Thresholds to Classify Sedentary and Stationary Behaviour in Children. Children. 2018; 5(12):172. https://doi.org/10.3390/children5120172
Chicago/Turabian StyleHurter, Liezel, Stuart J. Fairclough, Zoe R. Knowles, Lorna A. Porcellato, Anna M. Cooper-Ryan, and Lynne M. Boddy. 2018. "Establishing Raw Acceleration Thresholds to Classify Sedentary and Stationary Behaviour in Children" Children 5, no. 12: 172. https://doi.org/10.3390/children5120172
APA StyleHurter, L., Fairclough, S. J., Knowles, Z. R., Porcellato, L. A., Cooper-Ryan, A. M., & Boddy, L. M. (2018). Establishing Raw Acceleration Thresholds to Classify Sedentary and Stationary Behaviour in Children. Children, 5(12), 172. https://doi.org/10.3390/children5120172