

Socio-Economic Disparities in Pediatric Viral Gastroenteritis: A Comparative Study of Clinical Outcomes and Management in Hospitalized Children with Rotavirus, Adenovirus, and Norovirus Infections

 ,
,
Abstract
1. Introduction
2. Materials and Methods
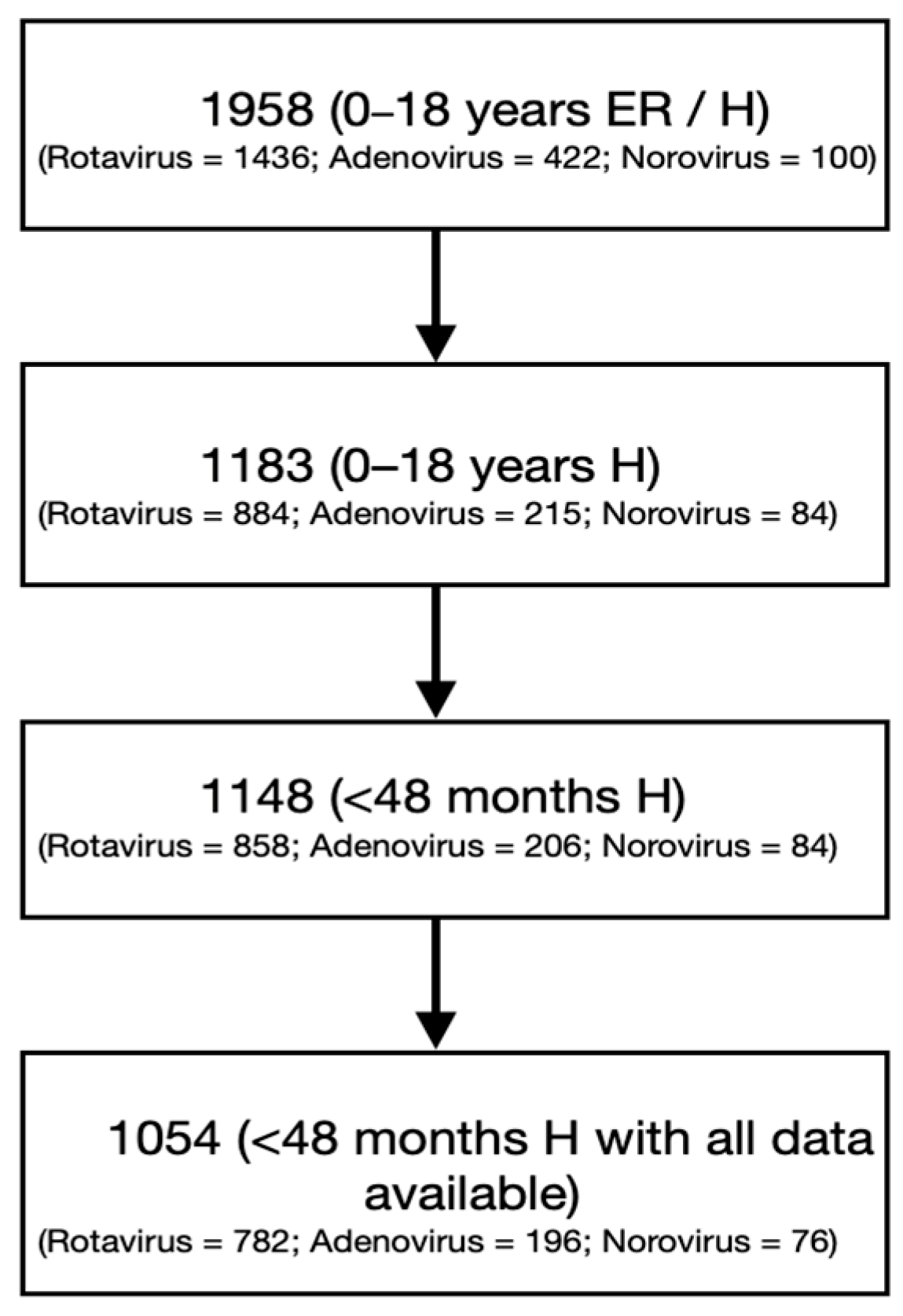
2.1. Study Design
2.2. Laboratory Diagnostics
2.3. Ethics
2.4. Definitions
2.5. Statistic Analysis
3. Results
3.1. Study Population Characteristics
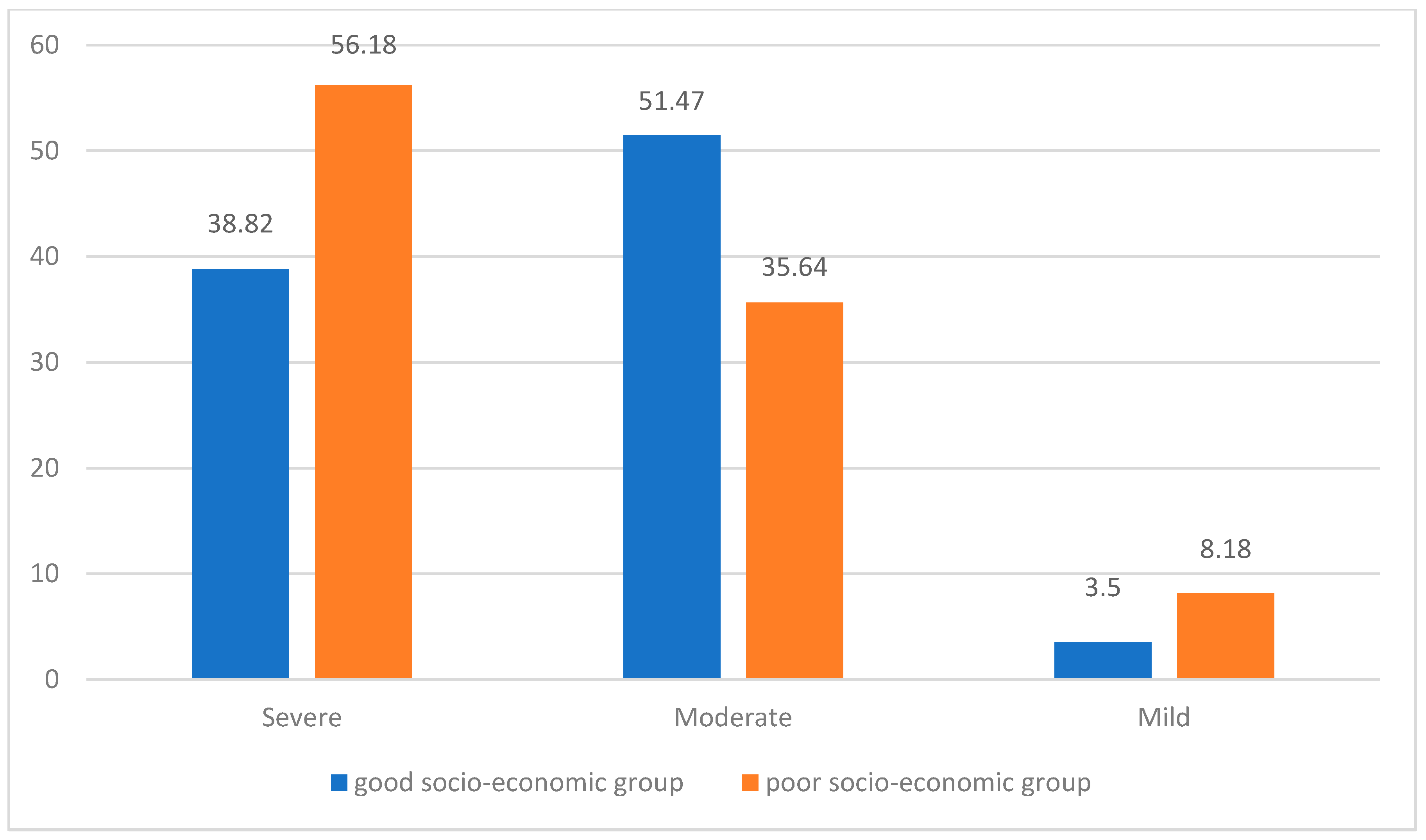
3.2. Treatment and Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AVG | Acute Viral Gastroenteritis |
References
- Rivera-Dominguez, G.; Ward, R. Pediatric Gastroenteritis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Bartram, J. New water forum will repeat old message. Bull. World Health Organ. 2003, 81, 158. [Google Scholar] [PubMed]
- Badur, S.; Öztürk, S.; Pereira, P.; AbdelGhany, M.; Khalaf, M.; Lagoubi, Y.; Ozudogru, O.; Hanif, K.; Saha, D. Systematic review of the rotavirus infection burden in the WHO-EMRO region. Hum. Vaccin. Immunother. 2019, 15, 2754–2768. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cohen, R.; Martinón-Torres, F.; Posiuniene, I.; Benninghoff, B.; Oh, K.-B.; Poelaert, D. The Value of Rotavirus Vaccination in Europe: A Call for Action. Infect. Dis. Ther. 2023, 12, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Rotavirus Vaccines: WHO Position Paper. [World Health Organization Web Site]. Available online: https://www.who.int/publications/i/item/WHO-WER9628 (accessed on 12 February 2025).
- About Rotavirus. Rotavirus. [CDC Web Site]. Available online: https://www.cdc.gov/rotavirus/about/index.html (accessed on 12 February 2025).
- Crawford, S.E.; Ramani, S.; Tate, J.E.; Parashar, U.D.; Svensson, L.; Hagbom, M.; Franco, M.A.; Greenberg, B.H.; O’Ryan, M.; Kang, G.; et al. Rotavirus infection. Nat. Rev. Dis. Primers 2017, 3, 17083. [Google Scholar] [CrossRef]
- Tate, J.E.; Burton, A.H.; Boschi-Pinto, C.; Parashar, U.D.; Agocs, M.; Serhan, F.; de Oliveira, L.; Mwenda, J.M.; Mihigo, R.; Wijesinghe, P.R.; et al. Global, Regional, and National Estimates of Rotavirus Mortality in Children <5 Years of Age, 2000–2013. Clin. Infect. Dis. 2016, 62 (Suppl. 2), S96–S105. [Google Scholar] [CrossRef] [PubMed]
- Bloch, D.; Chahroudi, A. Poverty and chronic illness: Why safety net programs matter. Pediatr. Res. 2019, 85, 743–744. [Google Scholar] [CrossRef]
- Dumitru, S.; Corad, B.; Iamandi-Cioinaru, C.; Titus-Cristian, M.; Monica, M.; Ciprian, M.; Georgiana, N.; Emil Daniel, T.; Vlad Alexandru, G.; Manuela Sofia, S. Atlas Marginalized Rural Areas and Local Human Development in Romania. [World Bank Group Web Site]. Available online: http://documents.worldbank.org/curated/en/847151467202306122 (accessed on 11 March 2025).
- Ogilvie, I.; Khoury, H.; Goetghebeur, M.M.; El Khoury, A.C.; Giaquinto, C. Burden of community-acquired and nosocomial rotavirus gastroenteritis in the pediatric population of Western Europe: A scoping review. BMC Infect. Dis. 2012, 12, 62. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2021 (Stockholm: ECDC). 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2021 (accessed on 30 March 2025).
- World Health Organization. Evidence Brief for Policy—Strengthening Romania’s Health System to Address Antimicrobial Resistance. [World Health Organization Web Site]. Available online: https://www.who.int/europe/publications/i/item/WHO-EURO-2020-5545-45310-64851 (accessed on 13 April 2025).
- ReAct. Address Antibiotic Resistance and Poverty—to Empower Children and Their Families. [ReAct Group Web Site]. Available online: https://www.reactgroup.org/news-and-views/news-and-opinions/year-2019/address-antibiotic-resistance-and-poverty-to-empower-children-their-families/ (accessed on 21 January 2025).
- Tarkhashvili, N. Does poverty increase antibiotic prescribing rates through underlying health conditions? Ecological study using parallel mediation analysis. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e21. [Google Scholar] [CrossRef]
- Toby Laboratories Int. Rotavirus and Adenovirus Combo Rapid Test Cassette (Feces) Package Insert. [Tody Laboratories Int Web Site]. Available online: https://www.todylaboratories.com/document/C61RT1026-Adenovirus-Rotavirus-Combo-TLI-IFU-RO-2020-EN (accessed on 18 June 2021).
- Nal Von Minden GmbH, NADAL. Norovirus GI/GII Test Cassette. [Nal Von Minden GmbH Web Site]. Available online: https://nal-vonminden.com/eng/nadal-norovirus-g1-g2-testkassette-10.html?srsltid=AfmBOorRNO5YYdW3igUn_y1cBFDn0sglC45TUDAQom6_MbFHsRi3B9T_ (accessed on 18 March 2024).
- Miller, J.M.; Binnicker, M.J.; Campbell, S.; Carroll, K.C.; Chapin, K.C.; Gonzalez, M.D.; Harrington, A.; Jerris, R.C.; Kehl, S.C.; Leal, S.M., Jr.; et al. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clin. Infect. Dis. 2024, 5, ciae104. [Google Scholar] [CrossRef] [PubMed]
- Kotloff, K.L. Acute gastroenteritis in children. In Nelson Textbook of Pediatrics, 21st ed.; Kliegman, R.M., Stanton, B., St. Geme, J., Schor, N.F., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; Chapter 366. [Google Scholar]
- Ruuska, T.; Vesikari, T. Rotavirus Disease in Finnish Children: Use of Numerical Scores for Clinical Severity of Diarrhoeal Episodes. Scand. J. Infect. Dis. 1990, 22, 259–267. [Google Scholar] [CrossRef]
- Stuempfig, N.D.; Seroy, J. Viral Gastroenteritis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Black, R.E.; Perin, J.; Yeung, D.; Rajeev, T.; Miller, J.; Elwood, S.E.; Platts-Mills, J.A. Estimated global and regional causes of deaths from diarrhoea in children younger than 5 years during 2000-21: A systematic review and Bayesian multinomial analysis. Lancet Glob. Health 2024, 12, e919–e928. [Google Scholar] [CrossRef]
- Guarino, A.; Aguilar, J.; Berkley, J.; Broekaert, I.; Vazquez-Frias, R.; Holtz, L.; Vecchio, A.L.; Meskini, T.; Moore, S.; Medina, J.F.R.; et al. Acute Gastroenteritis in Children of the World: What Needs to Be Done? J. Pediatr. Gastroenterol. Nutr. 2020, 70, 694–701. [Google Scholar] [CrossRef]
- Arbanas, I.; Monescu, V.; Dragomir, N.; Sauciuc, L.D.; Cojocaru, E.; Csutak, K.; Popovici, B.E.; Andreea, P.; Elena-Daniela, S.; Lixandru, R.-I.; et al. A 7-Year Survey (2015–2021) in One Pediatric Hospital (Brasov, Romania) on Rotavirus Gastroenteritis Specified as Community- or Hospital-Acquired Infection in Young Children. Trop. Med. Infect. Dis. 2023, 8, 509. [Google Scholar] [CrossRef] [PubMed]
- Poverty Rate in Romania 2023, by Region. [Database Online]. Statista Research Department. 2023. Published April 2025. Available online: https://www.statista.com/statistics/1191538/romania-poverty-rate-by-region/ (accessed on 10 April 2025).
- Podewils, L.J.; Mintz, E.D.; Nataro, J.P.; Parashar, U.D. Acute, infectious diarrhea among children in developing countries. Semin. Pediatr. Infect. Dis. 2004, 15, 155–168. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2021 (Stockholm: ECDC). 2023. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2022 (accessed on 25 March 2025).
- Omar, M.; Kassem, E.; Anis, E.; Abu-Jabal, R.; Mwassi, B.; Shulman, L.; Cohen, D.; Muhsen, K. Factors associated with antibiotic use in children hospitalized for acute viral gastroenteritis and the relation to rotavirus vaccination. Hum. Vaccin. Immunother. 2024, 20, 2396707. [Google Scholar] [CrossRef] [PubMed]
- Hossain, S.; Islam, F.; Arka, P.B.; Rohman, M.; Ahmed, T.S.; Ahammed, T.; Chowdhury, M.A.B.; Uddin, J. Antibiotic prescription from qualified sources for children with fever/cough: Cross-sectional study from 59 low- and middle-income countries. eClinicalMedicine 2023, 61, 102055. [Google Scholar] [CrossRef]
- McGurn, A.; Watchmaker, B.; Adam, K.; Ni, J.; Babinski, P.; Friedman, H.; Boyd, B.; Dugas, L.R.; Markossian, T. Socioeconomic Status and Determinants of Pediatric Antibiotic Use. Clin. Pediatr. 2020, 60, 32–41. [Google Scholar] [CrossRef]
- Quadri, F.; Nasrin, D.; Khan, A.; Bokhari, T.; Tikmani, S.S.; Nisar, M.I.; Bhatti, Z.; Kotloff, K.; Levine, M.M.; Zaidi, A.K.M. Health care use patterns for diarrhea in children in low-income periurban communities of Karachi, Pakistan. Am. J. Trop. Med. Hyg. 2013, 89 (Suppl. 1), 49–55. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- A Quee, F.; A de Hoog, M.L.; Schuurman, R.; Bruijning-Verhagen, P. Community burden and transmission of acute gastroenteritis caused by norovirus and rotavirus in the Netherlands (RotaFam): A prospective household-based cohort study. Lancet Infect. Dis. 2020, 20, 598–606. [Google Scholar] [CrossRef]
- Wolters, P.; A Holtman, G.; Weghorst, A.A.H.; Knoester, M.; Berger, M.Y. Rotavirus and illness severity in children presenting with acute gastroenteritis at the primary care out-of-hours service. Eur. J. Gen. Pr. 2021, 27, 346–353. [Google Scholar] [CrossRef]
- Gheorghita, S.; Birca, L.; Donos, A.; Wasley, A.; Birca, I.; Cojocaru, R.; Melnick, A.; Ciobanu, S.; Mosina, L.; Cortese, M.M.; et al. Impact of Rotavirus Vaccine Introduction and Vaccine Effectiveness in the Republic of Moldova. Clin. Infect. Dis. 2016, 62 (Suppl. 2), S140–S146. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bencina, G.; Costantino, C.; Mameli, C.; Sabale, U.; Murtagh, J.; Newman, R.; Ahern, A.; Bhaila, R.; Sanchez, A.O.; Martinon-Torres, F.; et al. Real-world impact of rotavirus vaccination in European healthcare settings: A systematic literature review. Expert Rev. Vaccin. 2022, 21, 1121–1136. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Good Socio-Economic Backgrounds | Poor Socio-Economic Backgrounds | Total | p Value (Chi-Square) | |||
|---|---|---|---|---|---|---|
| Virus | No. Cases | % Within Group | No. Cases | % Within Group | No. Cases | |
| Rotavirus | 421 | 72.9 | 361 | 75.7 | 782 | 0.351 |
| Adenovirus | 102 | 17.7 | 94 | 19.7 | 196 | 0.445 |
| Norovirus | 54 | 9.4 | 22 | 4.60 | 76 | 0.004 |
| Total | 577 | 477 | 1054 | |||
| Good Socio-Economic Backgrounds | Poor Socio-Economic Backgrounds | Total | p Value (FET; Chi-Squared) | |||
|---|---|---|---|---|---|---|
| Age (Months) | No. Cases | % Within Group | No. Cases | % Within Group | No. Cases | |
| 0–1 | 24 | 4.2 | 37 | 7.70 | 61 | 0.119 |
| 1–12 | 134 | 23.2 | 262 | 55 | 396 | <0.001 |
| ≥12 | 419 | 72.6 | 178 | 37.3 | 597 | <0.001 |
| Total | 577 | 477 | 1054 | |||
| Comorbidities | Good Socio-Economic Backgrounds | Poor Socio-Economic Backgrounds | p-Value (Chi-Square) | ||
|---|---|---|---|---|---|
| No. Cases | % Within Group | No. Cases | % Within Group | ||
| Allergies | 21 | 3.63 | 6 | 1.25 | 0.025 |
| Anemia | 61 | 10.5 | 73 | 15.3 | 0.027 |
| Malnutrition | 12 | 2.07 | 57 | 11.9 | <0.001 |
| Other (Renal/cardiac congenital malformation, neurological disorders, genetic disorders) | 61 | 10.5 | 31 | 6.49 | 0.026 |
| Treatment | Good Socio-Economic Backgrounds | Poor Socio-Economic Backgrounds | Total | p-Value | ||
|---|---|---|---|---|---|---|
| No. Cases | % Within Group | No. Cases | % Within Group | No. Cases | ||
| 1 | 1 | 0.18 | 0 | 0 | 1 | 1.0 |
| 2 | 3 | 0.52 | 25 | 5.20 | 28 | 0.001 |
| 3 | 347 | 60.2 | 268 | 56.2 | 615 | 0.307 |
| 4 | 226 | 39.1 | 184 | 38.6 | 410 | 0.951 |
| Average Vesikari Score | ||||||
|---|---|---|---|---|---|---|
| Virus | Adenovirus | Rotavirus | Norovirus | |||
| Good socio-economic backgrounds | Poor socio-economic backgrounds | Good socio-economic backgrounds | Poor socio-economic backgrounds | Good socio-economic backgrounds | Poor socio-economic backgrounds | |
| 11.2 | 11 | 11.6 | 11.8 | 11.1 | 10.5 | |
| p value (T-test) | 0.13 | 0.28 | 0.10 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbanas, I.; Coja, G.; Bilotta, A.; Lixandru, R.-I.; Patran, O.; Bleotu, L.; Falup-Pecurariu, O. Socio-Economic Disparities in Pediatric Viral Gastroenteritis: A Comparative Study of Clinical Outcomes and Management in Hospitalized Children with Rotavirus, Adenovirus, and Norovirus Infections. Children 2025, 12, 856. https://doi.org/10.3390/children12070856
Arbanas I, Coja G, Bilotta A, Lixandru R-I, Patran O, Bleotu L, Falup-Pecurariu O. Socio-Economic Disparities in Pediatric Viral Gastroenteritis: A Comparative Study of Clinical Outcomes and Management in Hospitalized Children with Rotavirus, Adenovirus, and Norovirus Infections. Children. 2025; 12(7):856. https://doi.org/10.3390/children12070856
Chicago/Turabian StyleArbanas, Ioana, Gabriela Coja, Alice Bilotta, Raluca-Ileana Lixandru, Oana Patran, Laura Bleotu, and Oana Falup-Pecurariu. 2025. "Socio-Economic Disparities in Pediatric Viral Gastroenteritis: A Comparative Study of Clinical Outcomes and Management in Hospitalized Children with Rotavirus, Adenovirus, and Norovirus Infections" Children 12, no. 7: 856. https://doi.org/10.3390/children12070856
APA StyleArbanas, I., Coja, G., Bilotta, A., Lixandru, R.-I., Patran, O., Bleotu, L., & Falup-Pecurariu, O. (2025). Socio-Economic Disparities in Pediatric Viral Gastroenteritis: A Comparative Study of Clinical Outcomes and Management in Hospitalized Children with Rotavirus, Adenovirus, and Norovirus Infections. Children, 12(7), 856. https://doi.org/10.3390/children12070856