
A Prospective Study on the Systematic Application of the Safe Insertion Umbilical Venous Catheter (SIUVeC) Bundle

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
- (1)
- Preprocedural Evaluation
- (2)
- Preassembled Insertion Kits
- (3)
- Appropriate aseptic techniques (hand hygiene, maximal barrier precautions, and skin antisepsis with 2% chlorhexidine in 70% isopropyl alcohol)
- (4)
- Vein cannulation using the smallest catheter that meets the infusion requirements and choosing wisely between single- or double-lumen UVCs
- (5)
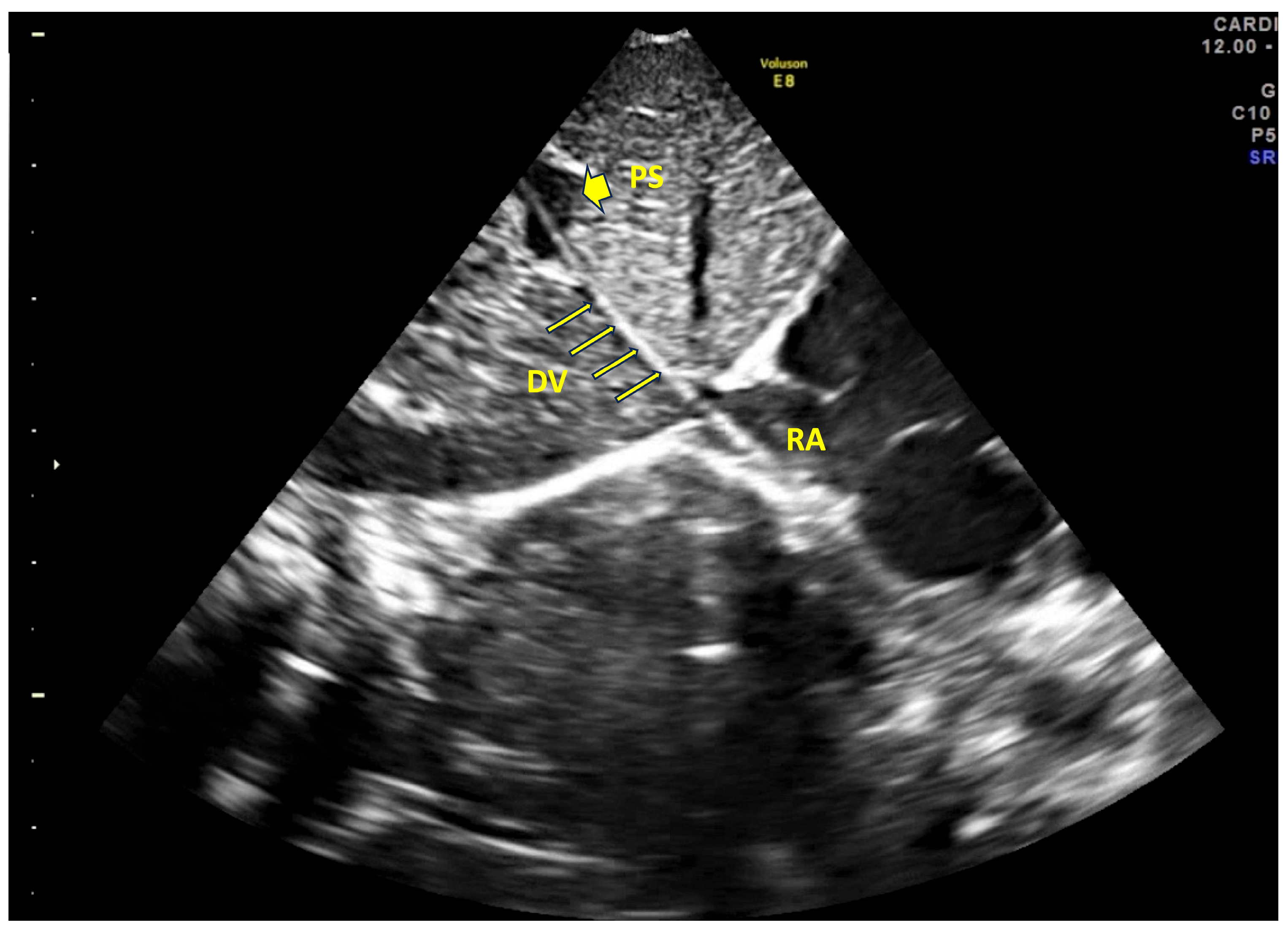
- Real-time tip navigation and tip location by US (according to the NeoECHOTIP protocol [17])
- (6)
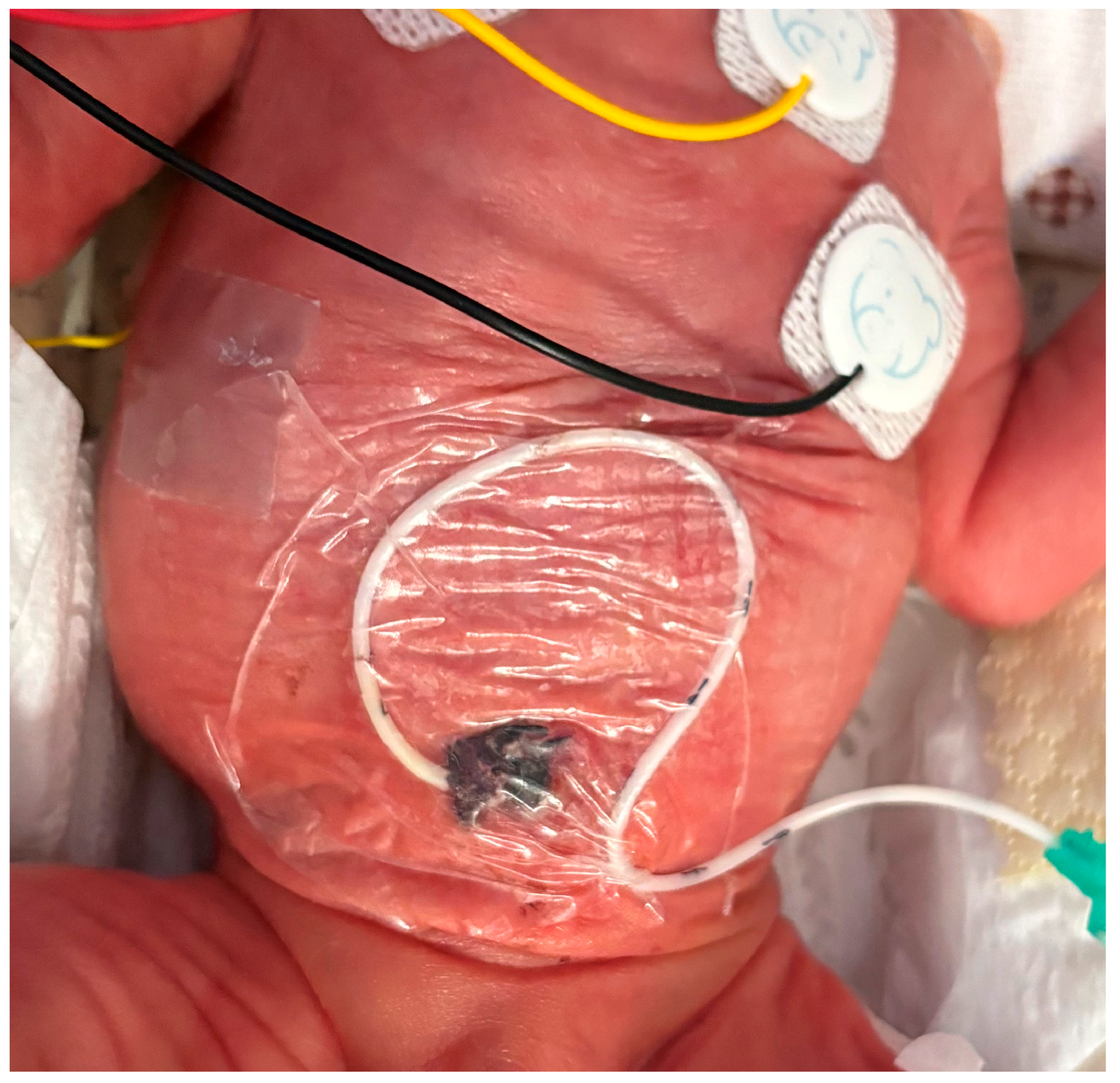
- Securement of the catheter and protection of the exit site (combining sutureless devices, cyanoacrylate glue, and semipermeable transparent membranes)
- (7)
- Post-procedural serial assessment of tip location by US
- (8)
- Early removal of the device (within 4–5 days)
3. Results
4. Discussion
- •
- Umbilical venous catheters (UVCs) are widely used in NICUs to provide central venous access, but are associated with a high risk of complications, including malposition, infection, and thrombosis.
- •
- Proper tip location using US and securement strategies are essential in minimizing these risks.
- •
- This prospective study demonstrates that the implementation of a structured protocol (SIUVeC), which includes real-time ultrasound (NeoECHOTIP) and cyanoacrylate glue for securement, results in high rates of optimal tip placement (90.6%) and low complication rates.
- •
- This study has significantly expanded the body of evidence supporting the systematic use of US before, during, and after UVC insertion to enhance both the safety and efficacy of the procedure. The consistent application of the DAV-expert algorithm and the SIUVeC protocol proved to be valuable tools in minimizing the risks traditionally associated with UVC use in the NICU setting.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Andrea, V.; Prontera, G.; Rubortone, S.A.; Pezza, L.; Pinna, G.; Barone, G.; Pittiruti, M.; Vento, G. Umbilical Venous Catheter Update: A Narrative Review Including Ultrasound and Training. Front. Pediatr. 2021, 9, 774705. [Google Scholar] [CrossRef] [PubMed]
- Gibson, K.; Sharp, R.; Ullman, A.; Morris, S.; Kleidon, T.; Esterman, A. Adverse events associated with umbilical catheters: A systematic review and meta-analysis. J. Perinatol. 2021, 41, 2505–2512. [Google Scholar] [CrossRef] [PubMed]
- Hermansen, M.C.; Hermansen, M.G. Intravascular catheter complications in the neonatal intensive care unit. Clin. Perinatol. 2005, 32, 141–156. [Google Scholar] [CrossRef]
- Oestreich, A.E. Umbilical vein catheterization--appropriate and inappropriate placement. Pediatr. Radiol. 2010, 40, 1941–1949. [Google Scholar] [CrossRef]
- Rubortone, S.A.; Costa, S.; Perri, A.; D’Andrea, V.; Vento, G.; Barone, G. Real-time ultrasound for tip location of umbilical venous catheter in neonates: A pre/post intervention study. Ital. J. Pediatr. 2021, 47, 68. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, V.; Prontera, G.; Cota, F.; Perri, A.; Russo, R.; Barone, G.; Vento, G. Real-Time Ultrasound Tip Location Reduces Malposition and Radiation Exposure during Umbilical Venous Catheter Placement in Neonates: A Retrospective, Observational Study. Neonatology 2025, 122, 32–37. [Google Scholar] [CrossRef]
- Pittiruti, M.; Annetta, M.G.; D’Andrea, V. Point-of-care ultrasound for vascular access in neonates and children. Eur. J. Pediatr. 2024, 183, 1073–1078. [Google Scholar] [CrossRef]
- Piersigilli, F.; Iacona, G.; Yazami, S.; Carkeek, K.; Hocq, C.; Auriti, C.; Danhaive, O. Cyanoacrylate glue as part of a new bundle to decrease neonatal PICC-related complications. Eur. J. Pediatr. 2023, 182, 5607–5613. [Google Scholar] [CrossRef]
- Capasso, A.; Paonessa, A.; Ferrara, T.; Grasso, F.; Capasso, L.; Migliaro, F.; Illiano, A.; Salome, S.; Zollo, M.; Amitrano, A.; et al. Use of 2% chlorhexidine gluconate in 70% isopropyl alcohol for skin disinfection during central catheter insertion in premature neonates. J. Vasc. Access 2025. [Google Scholar] [CrossRef]
- Tumuhamye, J.; Sommerfelt, H.; Tumwine, J.K.; Mukunya, D.; Ndeezi, G.; Namugga, O.; Bwanga, F.; Steinsland, H.; Nankabirwa, V. Umbilical Cord Stump Infections in Central Uganda: Incidence, Bacteriological Profile, and Risk Factors. Int. J. Environ. Res. Public Health 2022, 19, 16055. [Google Scholar] [CrossRef]
- Barone, G.; Pittiruti, M.; Prontera, G.; Ancora, G.; D’Andrea, V. A novel neonatal protocol for Safe Insertion of Umbilical Venous Catheters (SIUVeC): Minimizing complications in placement and management. J. Vasc. Access 2025, 26, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Payne, V.; Hall, M.; Prieto, J.; Johnson, M. Care bundles to reduce central line-associated bloodstream infections in the neonatal unit: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F422–F429. [Google Scholar] [CrossRef] [PubMed]
- Barone, G.; D’Andrea, V.; Ancora, G.; Cresi, F.; Maggio, L.; Capasso, A.; Mastroianni, R.; Pozzi, N.; Rodriguez-Perez, C.; Romitti, M.G.; et al. The neonatal DAV-expert algorithm: A GAVeCeLT/GAVePed consensus for the choice of the most appropriate venous access in newborns. Eur. J. Pediatr. 2023, 182, 3385–3395. [Google Scholar] [CrossRef] [PubMed]
- Nifong, T.P.; McDevitt, T.J. The effect of catheter to vein ratio on blood flow rates in a simulated model of peripherally inserted central venous catheters. Chest 2011, 140, 48–53. [Google Scholar] [CrossRef]
- Nickel, B.; Gorski, L.; Kleidon, T.; Kyes, A.; DeVries, M.; Keogh, S.; Meyer, B.; Sarver, M.J.; Crickman, R.; Ong, J.; et al. Infusion Therapy Standards of Practice, 9th Edition. J. Infus. Nurs. 2024, 47, S1–S285. [Google Scholar] [CrossRef]
- Muller, M.; Bryant, K.A.; Espinosa, C.; Jones, J.A.; Quach, C.; Rindels, J.R.; Stewart, D.L.; Zangwill, K.M.; Sanchez, P.J. SHEA Neonatal Intensive Care Unit (NICU) White Paper Series: Practical approaches for the prevention of central-line-associated bloodstream infections. Infect. Control Hosp. Epidemiol. 2023, 44, 550–564. [Google Scholar] [CrossRef]
- Barone, G.; Pittiruti, M.; Biasucci, D.G.; Elisei, D.; Iacobone, E.; La Greca, A.; Zito Marinosci, G.; D’Andrea, V. Neo-ECHOTIP: A structured protocol for ultrasound-based tip navigation and tip location during placement of central venous access devices in neonates. J. Vasc. Access 2022, 23, 679–688. [Google Scholar] [CrossRef]
- Kishigami, M.; Shimokaze, T.; Enomoto, M.; Shibasaki, J.; Toyoshima, K. Ultrasound-Guided Umbilical Venous Catheter Insertion with Alignment of the Umbilical Vein and Ductus Venosus. J. Ultrasound Med. 2020, 39, 379–383. [Google Scholar] [CrossRef]
- D’Andrea, V.; Prontera, G.; Pinna, G.; Cota, F.; Fattore, S.; Costa, S.; Migliorato, M.; Barone, G.; Pittiruti, M.; Vento, G. Securement of Umbilical Venous Catheter Using Cyanoacrylate Glue: A Randomized Controlled Trial. J. Pediatr. 2023, 260, 113517. [Google Scholar] [CrossRef]
- Hoellering, A.; Tshamala, D.; Davies, M.W. Study of movement of umbilical venous catheters over time. J. Paediatr. Child. Health 2018, 54, 1329–1335. [Google Scholar] [CrossRef]
- Dubbink-Verheij, G.H.; Visser, R.; Tan, R.; Roest, A.A.W.; Lopriore, E.; Te Pas, A.B. Inadvertent Migration of Umbilical Venous Catheters Often Leads to Malposition. Neonatology 2019, 115, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Gibson, K.; Smith, A.; Sharp, R.; Ullman, A.; Morris, S.; Esterman, A. Adverse events associated with umbilical vascular catheters in neonatal intensive care: Development of a risk prediction model. Aust. Crit. Care 2025, 38, 101146. [Google Scholar] [CrossRef] [PubMed]
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.; Sherertz, R.J.; Warren, D.K. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 49, 1–45. [Google Scholar] [CrossRef] [PubMed]
- Chaves, F.; Garnacho-Montero, J.; Del Pozo, J.L.; Bouza, E.; Capdevila, J.A.; de Cueto, M.; Dominguez, M.A.; Esteban, J.; Fernandez-Hidalgo, N.; Fernandez Sampedro, M.; et al. Diagnosis and treatment of catheter-related bloodstream infection: Clinical guidelines of the Spanish Society of Infectious Diseases and Clinical Microbiology and (SEIMC) and the Spanish Society of Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC). Med. Intensiv. (Engl. Ed.) 2018, 42, 5–36. [Google Scholar] [CrossRef]
- Levit, O.L.; Shabanova, V.; Bizzarro, M.J. Umbilical catheter-associated complications in a level IV neonatal intensive care unit. J. Perinatol. 2020, 40, 573–580. [Google Scholar] [CrossRef]
- Kim, M.J.; Yoo, S.Y.; Jeon, T.Y.; Kim, J.H.; Kim, Y.J. Imaging of Umbilical Venous Catheter-Related Hepatic Complications in Neonates. J. Korean Soc. Radiol. 2023, 84, 586–595. [Google Scholar] [CrossRef]
- Kozyak, B.W.; Fraga, M.V.; Juliano, C.E.; Bhombal, S.; Munson, D.A.; Brandsma, E.; Stoller, J.Z.; Jain, A.; Kesman, R.; Meshkati, M.; et al. Real-Time Ultrasound Guidance for Umbilical Venous Cannulation in Neonates with Congenital Heart Disease. Pediatr. Crit. Care Med. 2022, 23, e257–e266. [Google Scholar] [CrossRef]
- Shahroor, M.; Maarouf, A.M.; Yang, J.; Yankanah, R.; Shah, P.S.; Mohamed, A. Complications Associated with Low Position versus Good Position Umbilical Venous Catheters in Neonates of ≤32 Weeks’ Gestation. Am. J. Perinatol. 2022, 39, 259–264. [Google Scholar] [CrossRef]
- Bersani, I.; Piersigilli, F.; Iacona, G.; Savarese, I.; Campi, F.; Dotta, A.; Auriti, C.; Di Stasio, E.; Garcovich, M. Incidence of umbilical vein catheter-associated thrombosis of the portal system: A systematic review and meta-analysis. World J. Hepatol. 2021, 13, 1802–1815. [Google Scholar] [CrossRef]
- Sulemanji, M.; Vakili, K.; Zurakowski, D.; Tworetzky, W.; Fishman, S.J.; Kim, H.B. Umbilical Venous Catheter Malposition Is Associated with Necrotizing Enterocolitis in Premature Infants. Neonatology 2017, 111, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Odada, D.; Munyi, H.; Gatuiku, J.; Thuku, R.; Nyandigisi, J.; Wangui, A.; Ashihundu, E.; Nyakiringa, B.; Kimeu, J.; Musumbi, M.; et al. Reducing the rate of central line-associated bloodstream infections; a quality improvement project. BMC Infect. Dis. 2023, 23, 745. [Google Scholar] [CrossRef] [PubMed]
- Bertini, G.; Elia, S.; Ceciarini, F.; Dani, C. Reduction of catheter-related bloodstream infections in preterm infants by the use of catheters with the AgION antimicrobial system. Early Hum. Dev. 2013, 89, 21–25. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Mean (SD)/Number (%) | Min–Max | |
|---|---|---|
| Gestational age | 32.7 ± 5.3 | 22–41.6 |
| Birth weight | 1922 ± 1098 | 350–4700 |
| Male | 230 (51.2%) | |
| Small for gestational age | 123 (27.3%) |
| Number (%) | |
|---|---|
| Prematurity | 176 (39.2%) |
| Severe respiratory distress syndrome | 95 (21.2%) |
| Hemodynamic instability | 87 (19.4%) |
| Difficult peripheral venous cannulation | 41 (9.1%) |
| Therapeutic hypothermia | 50 (11.1%) |
| Single-lumen catheter | 177 (39.4) |
| Double-lumen catheter | 272 (60.6%) |
| 3.5 Fr catheter | 145 (32.3%) |
| 4 Fr catheter | 258 (57.5%) |
| 5 Fr catheter | 46 (10.2%) |
| Mean (SD)/Number (%) | Min–Max | |
|---|---|---|
| Mean dwell time (days) | 4.2 ± 2 | 1–7 |
| No catheters in a safe position | 407/449 (90.6%) | |
| Electively removed | 366/407 (89.9%) | |
| CRBSI | 3/407 (0.7%) | |
| Thrombosis | 10/407 (2.4%) | |
| Secondary malposition | 28/407 (6.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barone, G.; Ancora, G.; Pittiruti, M.; Prontera, G.; Vento, G.; D’Andrea, V. A Prospective Study on the Systematic Application of the Safe Insertion Umbilical Venous Catheter (SIUVeC) Bundle. Children 2025, 12, 819. https://doi.org/10.3390/children12070819
Barone G, Ancora G, Pittiruti M, Prontera G, Vento G, D’Andrea V. A Prospective Study on the Systematic Application of the Safe Insertion Umbilical Venous Catheter (SIUVeC) Bundle. Children. 2025; 12(7):819. https://doi.org/10.3390/children12070819
Chicago/Turabian StyleBarone, Giovanni, Gina Ancora, Mauro Pittiruti, Giorgia Prontera, Giovanni Vento, and Vito D’Andrea. 2025. "A Prospective Study on the Systematic Application of the Safe Insertion Umbilical Venous Catheter (SIUVeC) Bundle" Children 12, no. 7: 819. https://doi.org/10.3390/children12070819
APA StyleBarone, G., Ancora, G., Pittiruti, M., Prontera, G., Vento, G., & D’Andrea, V. (2025). A Prospective Study on the Systematic Application of the Safe Insertion Umbilical Venous Catheter (SIUVeC) Bundle. Children, 12(7), 819. https://doi.org/10.3390/children12070819