
Controversies in Parenteral Protein Intake in Preterm Infants


Abstract
1. Introduction
2. Biochemical Basis of Adverse Effects from Excessive Protein Intake
2.1. High Protein and Later Obesity
2.2. High Protein and Metabolic Acidosis
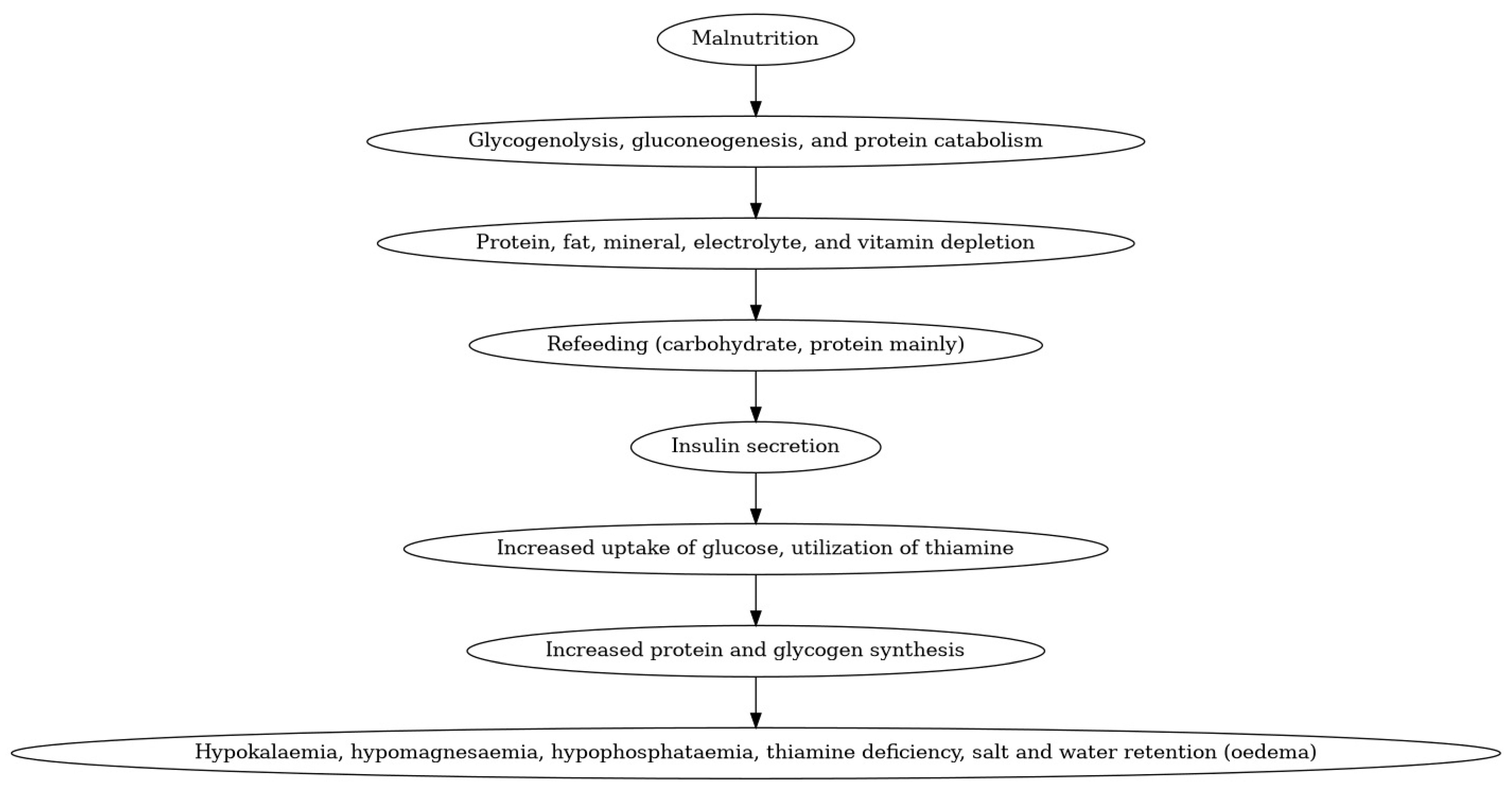
2.3. High Protein and Refeeding Syndrome
3. Studies Looking at Varying Protein Administration [Table 1]

{kind=link}
| Study | Finding |
|---|---|
| [47] | Higher Amino Acid (HAA, receiving 3 g/kg/day of amino acids as compared to Low Amino Acid group (LAA) receiving 1 g/kg/d of amino acids) group had significantly higher plasma Leucine, Isoleucine, Phenylalanine, Methionine, Proline, Arginine, and Ornithine levels. |
| [51] | Significantly lower z scores for head circumference in the high AA group (which started with a dose of 2 g/kg/day of parenteral AA on DOL 1 and was increased by 1 g/kg/day to a maximum of 4 g/kg/day, which continued till DOL 7, as compared to the Standard AA group which received 0.5 g/kg/day of parenteral AA starting the day of life (DOL) 1, increased by 0.5 g/kg/day daily to a maximum of 3 g/kg/day, which continued till DOL7) at 6, 12, 18, and 24 months |
| [52] | High AA group with significantly higher levels of individual amino acids as compared to levels in second-trimester fetuses. |
| [53] | Propensity score-matched analysis of infants enrolled in the EPIPAGE-2 study-primary outcome of Full Scale IQ greater than −1 SD (i.e., ≥93 points) at age 5 years was more frequent in the exposed (high amino acid intake (3.51–4.50 g/kg/d) 7 days after birth) vs. the unexposed group (243 infants [61.4%] vs. 206 infants [54.4%], respectively; odds ratio [OR], 1.33 [95% CI, 1.00–1.71]). |
| [54] | Significantly lower head circumference growth velocity on postnatal day 28 in High AA group (3 g/kg/day of parenteral amino acids on day 1, and the dose increased to 4 g/kg/day the next day) as compared to Low Amino Acid group (receiving 1 g/kg/day of parenteral amino acids on day 1 and dose increased by 1 g/kg every day till a maximum of 4 g/kg/day) |
| [55] | Moderate to severe neuro disability was more common in the intervention group who received more than 1 g per day of parenteral protein over the first four postnatal days and more than a mean of 3.5 g per kilogram per day on postnatal days 3, 4, and 5 as compared to the control group (adjusted relative risk, 1.95; 95% CI, 1.09 to 3.48) |
4. Current Recommendation [Table 2]
| Institution | Recommendation | |
|---|---|---|
| American Society for Parenteral and Enteral Nutrition [61] | Parenteral AA doses at a minimum of 3 g/kg/day without increasing beyond 3.5 g/kg/day. | |
| European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) [57] | Parenteral AA intake ranging between 2.5 and 3.5 g/kg/day, accompanied by non-protein calorie intake of 65 kcal/kg/day. | |
| American Academy of Pediatrics Committee on Nutrition [62] | <1000 g birth weight/kg/day | 1000–1500 g birth weight/kg/day |
| Starting Phase | 1.5–2.5 g | 3.0–3.5 g |
| Stable Phase | 3.0–3.5 g | 3.0–3.5 g |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poindexter, B.B.; Langer, J.C.; Dusick, A.M.; Ehrenkranz, R.A. Early provision of parenteral amino acids in extremely low birth weight infants: Relation to growth and neurodevelopmental outcome. J. Pediatr. 2006, 148, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Thureen, P.J.; Anderson, A.H.; Baron, K.A.; Melara, D.L.; Hay, W.W.; Fennessey, P.V. Protein balance in the first week of life in ventilated neonates receiving parenteral nutrition. Am. J. Clin. Nutr. 1998, 68, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Bellagamba, M.P.; Carmenati, E.; D’Ascenzo, R.; Malatesta, M.; Spagnoli, C.; Biagetti, C.; Burattini, I.; Carnielli, V.P. One Extra Gram of Protein to Preterm Infants From Birth to 1800 g: A Single-Blinded Randomized Clinical Trial. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Premji, S.S.; Al-Wassia, H.; Sauve, R.S. Higher versus lower protein intake in formula-fed low birth weight infants. Cochrane Database Syst. Rev. 2014, 2014, CD003959. [Google Scholar] [CrossRef]
- van den Akker, C.H.; Braake, F.W.T.; Weisglas-Kuperus, N.; van Goudoever, J.B. Observational outcome results following a randomized controlled trial of early amino acid administration in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 714–719. [Google Scholar] [CrossRef]
- Cormack, B.E.; Jiang, Y.; Harding, J.E.; Crowther, C.A.; Bloomfield, F.H.; for the ProVIDe Trial Group. Neonatal refeeding syndrome and clinical outcome in extremely low-birth-weight babies: Secondary cohort analysis from the ProVIDe trial. J. Parenter. Enter. Nutr. 2021, 45, 65–78. [Google Scholar] [CrossRef]
- Amissah, E.A.; Brown, J.; Harding, J.E. Protein supplementation of human milk for promoting growth in preterm infants. Cochrane Database Syst. Rev. 2020, 2020, CD000433. [Google Scholar] [CrossRef]
- Braake, F.T.; Akker, C.v.D.; Riedijk, M.; van Goudoever, J. Parenteral amino acid and energy administration to premature infants in early life. In Seminars in Fetal and Neonatal Medicine; Elsevier: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Das, S.; McClintock, T.; Cormack, B.E.; Bloomfield, F.H.; Harding, J.E.; Lin, L. High protein intake on later outcomes in preterm children: A systematic review and meta-analysis. Pediatr. Res. 2025, 97, 67–80. [Google Scholar] [CrossRef]
- Embleton, N.D.; van den Akker, C.H. Protein intakes for preterm infants, and the need for a multi-nutrient holistic approach. Pediatr. Res. 2024, 97, 8–10. [Google Scholar] [CrossRef]
- Würtz, P.; Soininen, P.; Kangas, A.J.; Rönnemaa, T.; Lehtimäki, T.; Kähönen, M.; Viikari, J.S.; Raitakari, O.T.; Ala-Korpela, M. Branched-chain and aromatic amino acids are predictors of insulin resistance in young adults. Diabetes Care 2013, 36, 648–655. [Google Scholar] [CrossRef]
- Yoon, M.-S. The emerging role of branched-chain amino acids in insulin resistance and metabolism. Nutrients 2016, 8, 405. [Google Scholar] [CrossRef] [PubMed]
- Żebrowska, E.; Maciejczyk, M.; Żendzian-Piotrowska, M.; Zalewska, A.; Chabowski, A. High protein diet induces oxidative stress in rat cerebral cortex and hypothalamus. Int. J. Mol. Sci. 2019, 20, 1547. [Google Scholar] [CrossRef] [PubMed]
- Yudkoff, M.; Daikhin, Y.; Nissim, I.; Horyn, O.; Luhovyy, B.; Lazarow, A.; Nissim, I. Brain Amino Acid Requirements and Toxicity: The Example of Leucine. J. Nutr. 2005, 135, 1531S–1538S, Erratum in J. Nutr. 2005, 135, 2009. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Agosti, M.; Group, M. Nutrition in the first 1000 days: Ten practices to minimize obesity emerging from published science. Int. J. Environ. Res. Public Health 2017, 14, 1491. [Google Scholar] [CrossRef]
- Brambilla, P.; Bedogni, G.; Pietrobelli, A.; Cianfarani, S.; Agostoni, C. Predictors of blood pressure at 7–13 years: The “new millennium baby” study. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 706–712. [Google Scholar] [CrossRef]
- Rudolf, M. Predicting babies’ risk of obesity. Arch. Dis. Child. 2011, 96, 995–997. [Google Scholar] [CrossRef]
- Fraser, A.; Macdonald-Wallis, C.; Tilling, K.; Boyd, A.; Golding, J.; Smith, G.D.; Henderson, J.; Macleod, J.; Molloy, L.; Ness, A.; et al. Cohort profile: The Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int. J. Epidemiol. 2013, 42, 97–110. [Google Scholar] [CrossRef]
- Tang, M. Protein intake during the first two years of life and its association with growth and risk of overweight. Int. J. Environ. Res. Public Health 2018, 15, 1742. [Google Scholar] [CrossRef]
- Rolland-Cachera, M.F.; Akrout, M.; Péneau, S. Nutrient intakes in early life and risk of obesity. Int. J. Environ. Res. Public Health 2016, 13, 564. [Google Scholar] [CrossRef]
- Lind, M.V.; Larnkjær, A.; Mølgaard, C.; Michaelsen, K.F. Dietary protein intake and quality in early life: Impact on growth and obesity. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 71–76. [Google Scholar] [CrossRef]
- Zheng, M.; Lamb, K.E.; Grimes, C.; Laws, R.; Bolton, K.; Ong, K.K.; Campbell, K. Rapid weight gain during infancy and subsequent adiposity: A systematic review and meta-analysis of evidence. Obes. Rev. 2018, 19, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Druet, C.; Stettler, N.; Sharp, S.; Simmons, R.K.; Cooper, C.; Smith, G.D.; Ekelund, U.; Lévy-Marchal, C.; Jarvelin, M.; Kuh, D.; et al. Prediction of childhood obesity by infancy weight gain: An individual-level meta-analysis. Paediatr. Perinat. Epidemiol. 2012, 26, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Laplante, M.; Sabatini, D.M. mTOR signaling in growth control and disease. Cell 2012, 149, 274–293. [Google Scholar] [CrossRef]
- Weber, M.; Grote, V.; Closa-Monasterolo, R.; Escribano, J.; Langhendries, J.-P.; Dain, E.; Giovannini, M.; Verduci, E.; Gruszfeld, D.; Socha, P.; et al. Lower protein content in infant formula reduces BMI and obesity risk at school age: Follow-up of a randomized trial. Am. J. Clin. Nutr. 2014, 99, 1041–1051. [Google Scholar] [CrossRef]
- Luque, V.; Closa-Monasterolo, R.; Escribano, J.; Ferré, N. Early programming by protein intake: The effect of protein on adiposity development and the growth and functionality of vital organs. Nutr. Metab. Insights 2015, 8, NMI. S29525. [Google Scholar] [CrossRef]
- Brown, L.D.; Hay, W.W. The nutritional dilemma for preterm infants: How to promote neurocognitive development and linear growth, but reduce the risk of obesity. J. Pediatr. 2013, 163, 1543–1545. [Google Scholar] [CrossRef]
- Trophamine (10% Amino Acid Injection)[Package Insert]; Braun Medical Inc.: Bethlehem, PA, USA, 2020.
- Bonsante, F.; Gouyon, J.-B.; Robillard, P.-Y.; Gouyon, B.; Iacobelli, S.; Simeoni, U. Early optimal parenteral nutrition and metabolic acidosis in very preterm infants. PLoS ONE 2017, 12, e0186936. [Google Scholar] [CrossRef]
- Notz, L.; Adams, M.; Bassler, D.; Boos, V. Association between early metabolic acidosis and bronchopulmonary dysplasia/death in preterm infants born at less than 28 weeks’ gestation: An observational cohort study. BMC Pediatr. 2024, 24, 605. [Google Scholar] [CrossRef]
- Yang, S.; Lee, B.S.; Park, H.; Choi, Y.; Jeong, S.; Kim, J.; Kim, E.A.; Kim, K. Effect of high vs standard early parenteral amino acid supplementation on the growth outcomes in very low birth weight infants. J. Parenter. Enter. Nutr. 2013, 37, 327–334. [Google Scholar] [CrossRef]
- Leenders, E.K.; de Waard, M.; van Goudoever, J.B. Low-versus high-dose and early versus late parenteral amino-acid administration in very-low-birth-weight infants: A systematic review and meta-analysis. Neonatology 2018, 113, 187–205. [Google Scholar] [CrossRef]
- Goswami, I.R.; Mehrem, A.A.; Scott, J.; Esser, M.J.; Mohammad, K. Metabolic acidosis rather than hypo/hypercapnia in the first 72 hours of life associated with intraventricular hemorrhage in preterm neonates. J. Matern.-Fetal Neonatal Med. 2021, 34, 3874–3882. [Google Scholar] [CrossRef] [PubMed]
- da Silva, J.S.; Seres, D.S.; Sabino, K.; Adams, S.C.; Berdahl, G.J.; Citty, S.W.; Cober, M.P.; Evans, D.C.; Greaves, J.R.; Gura, K.M.; et al. ASPEN consensus recommendations for refeeding syndrome. Nutr. Clin. Pract. 2020, 35, 178–195. [Google Scholar] [CrossRef] [PubMed]
- Moltu, S.J.; Strømmen, K.; Blakstad, E.W.; Almaas, A.N.; Westerberg, A.C.; Brække, K.; Rønnestad, A.; Nakstad, B.; Berg, J.P.; Veierød, M.B.; et al. Enhanced feeding in very-low-birth-weight infants may cause electrolyte disturbances and septicemia–a randomized, controlled trial. Clin. Nutr. 2013, 32, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Boubred, F.; Herlenius, E.; Bartocci, M.; Jonsson, B.; Vanpée, M. Extremely preterm infants who are small for gestational age have a high risk of early hypophosphatemia and hypokalemia. Acta Paediatr. 2015, 104, 1077–1083. [Google Scholar] [CrossRef]
- Sung, S.I.; Chang, Y.S.; Choi, J.H.; Ho, Y.; Kim, J.; Ahn, S.Y.; Park, W.S. Increased risk of refeeding syndrome–like hypophosphatemia with high initial amino acid intake in small-for-gestational-age, extremely-low-birthweight infants. PLoS ONE 2019, 14, e0221042. [Google Scholar] [CrossRef]
- Bradford, C.V.; Cober, M.P.; Miller, J.L. Refeeding syndrome in the neonatal intensive care unit. J. Pediatr. Pharmacol. Ther. 2021, 26, 771–782. [Google Scholar] [CrossRef]
- Al-Mouqdad, M.M.; Alshaikh, B.; Sumaily, H.H.; Almotiri, A.A.; Alodhaidan, N.A.; AlMahmoud, L.; Abdelrahim, A.; Yousif, T.E.; Alghamdi, A.S.; Albarrak, Y.A.; et al. Impact of Refeeding Syndrome on the Short-Term Clinical Outcomes of Very-Premature Infants. Nutrients 2024, 16, 3445. [Google Scholar] [CrossRef]
- Ross, J.R.; Finch, C.; Ebeling, M.; Taylor, S.N. Refeeding syndrome in very-low-birth-weight intrauterine growth-restricted neonates. J. Perinatol. 2013, 33, 717–720. [Google Scholar] [CrossRef]
- Bonsante, F.; Iacobelli, S.; Latorre, G.; Rigo, J.; De Felice, C.; Robillard, P.Y.; Gouyon, J.B.; Chavatte-Palmer, P. Initial amino acid intake influences phosphorus and calcium homeostasis in preterm infants–it is time to change the composition of the early parenteral nutrition. PLoS ONE 2013, 8, e72880. [Google Scholar] [CrossRef]
- Brener Dik, P.; Galletti, M.F.; Jonusas, S.A.F.; Alonso, G.; Mariani, G.L.; Fustiñana, C.A. Early hypophosphatemia in preterm infants receiving aggressive parenteral nutrition. J. Perinatol. 2015, 35, 712–715. [Google Scholar] [CrossRef]
- Igarashi, A.; Okuno, T.; Ohta, G.; Tokuriki, S.; Ohshima, Y. Risk factors for the development of refeeding syndrome-like hypophosphatemia in very low birth weight infants. Dis. Markers 2017, 2017, 9748031. [Google Scholar] [CrossRef] [PubMed]
- Lozano, G.B.; Soriano-Ramos, M.; Martín, M.T.P.; Calzada, S.C.; Soria, C.E.G.; Pallás-Alonso, C.R. Early hypophosphatemia in high-risk preterm infants: Efficacy and safety of sodium glycerophosphate from first day on parenteral nutrition. J. Parenter. Enter. Nutr. 2019, 43, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Al-Wassia, H.; Lyon, A.W.; Rose, S.M.; Sauve, R.S.; Fenton, T.R. Hypophosphatemia is prevalent among preterm infants less than 1500 grams. Am. J. Perinatol. 2019, 36, 1412–1419. [Google Scholar] [CrossRef] [PubMed]
- Pająk, A.; Królak-Olejnik, B.; Szafrańska, A. Early hypophosphatemia in very low birth weight preterm infants. Adv. Clin. Exp. Med. 2018, 27, 841–847. [Google Scholar] [CrossRef]
- Thureen, P.J.; Melara, D.; Fennessey, P.V.; Hay, W.W. Effect of low versus high intravenous amino acid intake on very low birth weight infants in the early neonatal period. Pediatr. Res. 2003, 53, 24–32. [Google Scholar] [CrossRef]
- Van der Crabben, S.N.; Verhoeven-Duif, N.M.; Brilstra, E.H.; Van Maldergem, L.; Coskun, T.; Rubio-Gozalbo, E.; Berger, R.; de Koning, T.J. An update on serine deficiency disorders. J. Inherit. Metab. Dis. 2013, 36, 613–619. [Google Scholar] [CrossRef]
- Baker, P.R.; Friederich, M.W.; Swanson, M.A.; Shaikh, T.; Bhattacharya, K.; Scharer, G.H.; Aicher, J.; Creadon-Swindell, G.; Geiger, E.; MacLean, K.N.; et al. Variant non ketotic hyperglycinemia is caused by mutations in LIAS, BOLA3 and the novel gene GLRX5. Brain 2014, 137, 366–379. [Google Scholar] [CrossRef]
- Alfadhel, M.; Alrifai, M.T.; Trujillano, D.; Alshaalan, H.; Al Othaim, A.; Al Rasheed, S.; Assiri, H.; Alqahtani, A.A.; Alaamery, M.; Rolfs, A.; et al. Asparagine synthetase deficiency: New inborn errors of metabolism. JIMD Rep. 2015, 22, 11–16. [Google Scholar]
- Blanco, C.L.; Gong, A.K.; Schoolfield, J.; Green, B.K.; Daniels, W.; Liechty, E.A.; Ramamurthy, R. Impact of early and high amino acid supplementation on ELBW infants at 2 years. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 601–607. [Google Scholar] [CrossRef]
- Blanco, C.L.; Gong, A.K.; Green, B.K.; Falck, A.; Schoolfield, J.; Liechty, E.A. Early changes in plasma amino acid concentrations during aggressive nutritional therapy in extremely low birth weight infants. J. Pediatr. 2011, 158, 543–548.e1. [Google Scholar] [CrossRef]
- Rozé, J.-C.; Morel, B.; Lapillonne, A.; Marret, S.; Guellec, I.; Darmaun, D.; Bednarek, N.; Moyon, T.; Marchand-Martin, L.; Benhammou, V.; et al. Association between early amino acid intake and full-scale IQ at age 5 years among infants born at less than 30 weeks’ gestation. JAMA Netw. Open 2021, 4, e2135452. [Google Scholar] [CrossRef]
- Balasubramanian, H.; Nanavati, R.N.; Kabra, N.S. Effect of two different doses of parenteral amino acid supplementation on postnatal growth of very low birth weight neonates—A randomized controlled trial. Indian Pediatr. 2013, 50, 1131–1136. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, F.H.; Jiang, Y.; Harding, J.E.; Crowther, C.A.; Cormack, B.E. Early amino acids in extremely preterm infants and neurodisability at 2 years. N. Engl. J. Med. 2022, 387, 1661–1672. [Google Scholar] [CrossRef]
- Lorthe, E.; Benhammou, V.; Marchand-Martin, L.; Pierrat, V.; Lebeaux, C.; Durox, M.; Goffinet, F.; Kaminski, M.; Ancel, P.-Y. Cohort profile: The etude Epidémiologique sur LES petits ages Gestationnels-2 (EPIPAGE-2) Preterm birth cohort. Int. J. Epidemiol. 2021, 50, 1428–1429m. [Google Scholar] [CrossRef]
- Van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; de Pipaon, M.S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Decsi, T.; Domellöf, M.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clin. Nutr. 2018, 37, 2315–2323. [Google Scholar] [CrossRef]
- Burattini, I.; Bellagamba, M.P.; Spagnoli, C.; D’AScenzo, R.; Mazzoni, N.; Peretti, A.; Cogo, P.E.; Carnielli, V.P. Targeting 2.5 versus 4 g/kg/day of amino acids for extremely low birth weight infants: A randomized clinical trial. J. Pediatr. 2013, 163, 1278–1282.e1. [Google Scholar]
- Morgan, C.; McGowan, P.; Herwitker, S.; Hart, A.E.; Turner, M.A. Postnatal head growth in preterm infants: A randomized controlled parenteral nutrition study. Pediatrics 2014, 133, e120–e128. [Google Scholar] [CrossRef]
- Huston, R.K.; Clark, R.H.; Chace, D.H. Ratio of non-protein calories to grams of amino acids and amino acid blood levels in preterm infants receiving parenteral nutrition. J. Neonatal-Perinat. Med. 2025, 18, 126–136. [Google Scholar] [CrossRef]
- Robinson, D.T.; Calkins, K.L.; Chen, Y.; Cober, M.P.; Falciglia, G.H.; Church, D.D.; Mey, J.; McKeever, L.; Sentongo, T. Guidelines for parenteral nutrition in preterm infants: The American Society for Parenteral and Enteral Nutrition. J. Parenter. Enter. Nutr. 2023, 47, 830–858. [Google Scholar] [CrossRef]
- Pediatrics, A.A.O. Pediatric Nutrition; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2025. [Google Scholar]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Alur, P.; Ramarao, S. Sex differences in preterm nutrition and growth: The evidence from human milk associated studies. J. Perinatol. 2022, 42, 987–992. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holla, I.; Alur, P. Controversies in Parenteral Protein Intake in Preterm Infants. Children 2025, 12, 759. https://doi.org/10.3390/children12060759
Holla I, Alur P. Controversies in Parenteral Protein Intake in Preterm Infants. Children. 2025; 12(6):759. https://doi.org/10.3390/children12060759
Chicago/Turabian StyleHolla, Ira, and Pradeep Alur. 2025. "Controversies in Parenteral Protein Intake in Preterm Infants" Children 12, no. 6: 759. https://doi.org/10.3390/children12060759
APA StyleHolla, I., & Alur, P. (2025). Controversies in Parenteral Protein Intake in Preterm Infants. Children, 12(6), 759. https://doi.org/10.3390/children12060759