
Exploring Aneurysmal Bone Cysts of the Skull: Insights from a Review of the Literature and a Case Report

 ,
,  , , , ,
, , , ,  ,
,
Abstract

1. Introduction
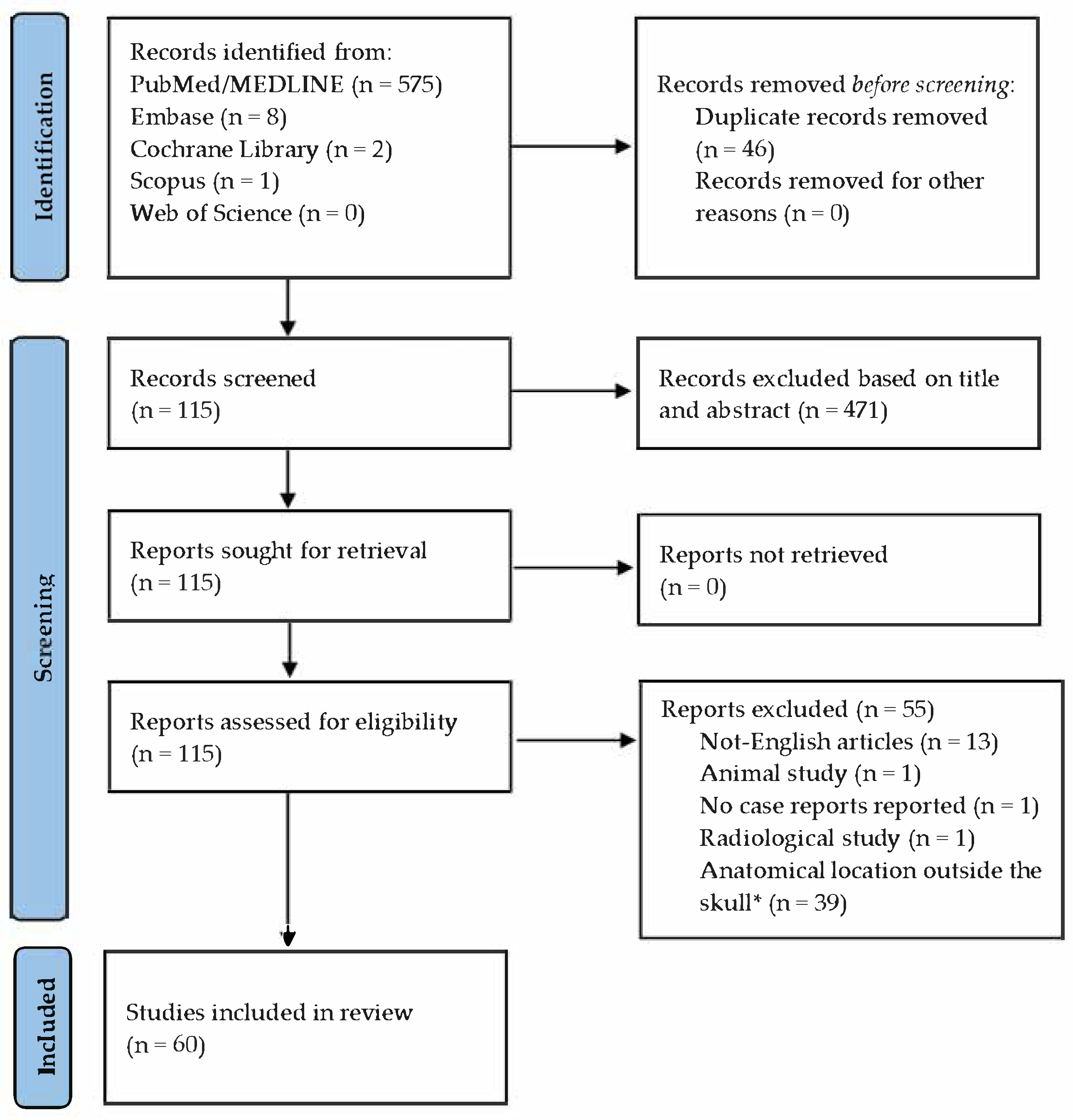
2. Materials and Methods
2.1. Objectives
2.2. Literature Search
2.3. Study Selection
2.4. Outcomes
2.5. Analyzed Data
- Patient demographics, including gender, age, presence of known genetic disorders, and history of previous head trauma;
- ABC characteristics, including lesion location, size (measured in millimeters), growth trend, symptoms and their relation to the lesion, and etiopathogenesis;
- Management characteristics, including type of treatment, type of surgery, use of preoperative embolization, short- and long-term complications, duration of follow-up (in months), and presence of recurrence.
2.6. Statistical Analysis
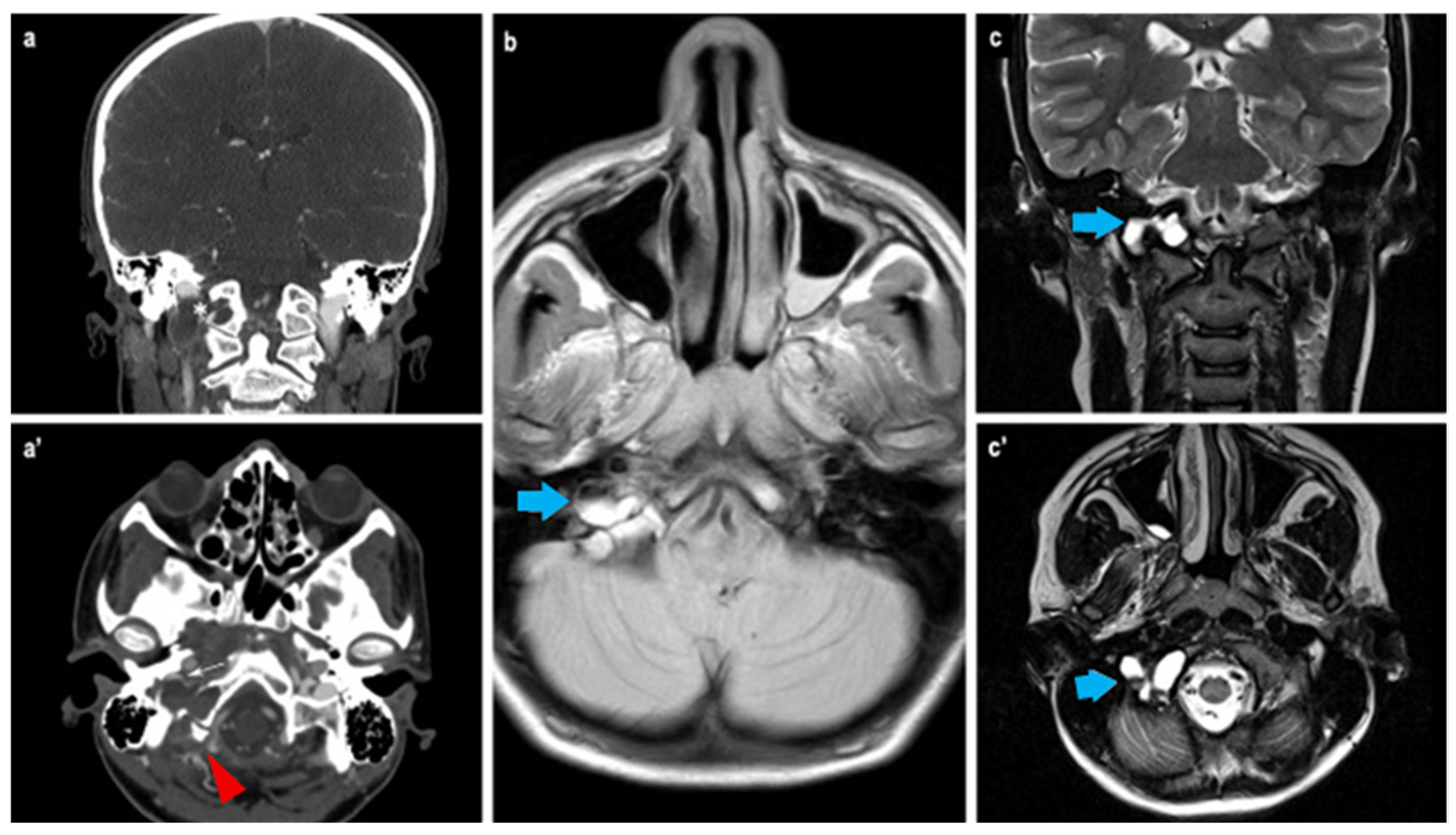
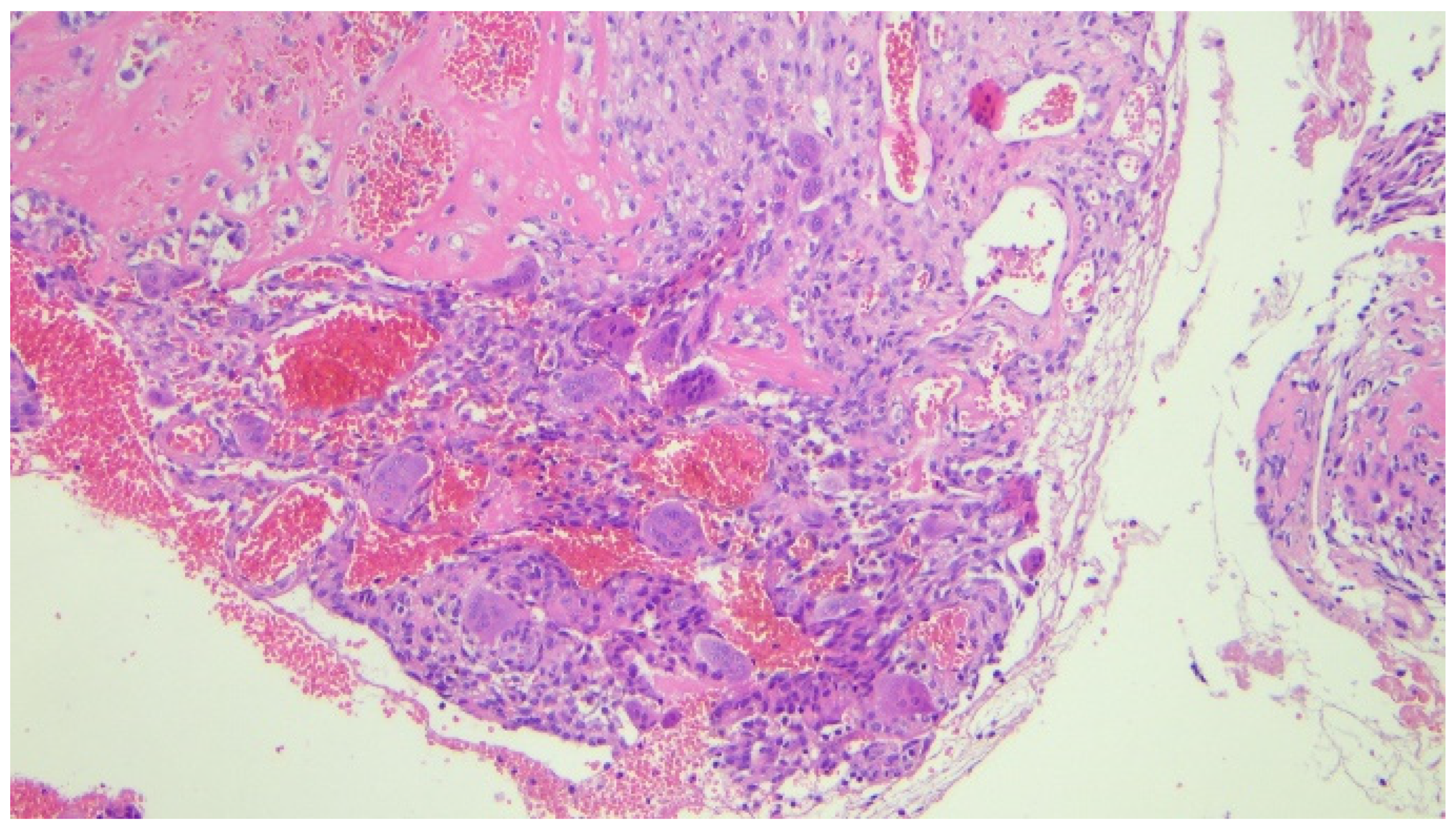
3. Case Report
4. Results
- One underwent an open biopsy, with residual pathological tissue left due to adherence to the clivus and cerebellar structures. This case was managed with corticosteroids and a hormonal blocker [33].
- One underwent a Subtotal Resection (STR) followed by radiation therapy and interferon alfa-2a treatment [37].
- Wound infection [41];
- Headaches and nuchal pressure [33];
- Early recurrence [29];
- Cerebrospinal fluid leakage [54];
- Conductive hearing loss and facial nerve deficit [56];
- Visual deterioration [16];
- Hemifacial numbness [62];
- Cerebral sinus thrombosis [6];
- Cardiac arrest with fatal outcome [7].
4.1. Parietal and Occipital Bone Localization
4.2. Early Complications and Etiopathogenesis
5. Discussion
6. Conclusions
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| ABC | aneurysmal bone cysts |
| FD | fibrous dysplasia |
| GH | Growth Hormone |
| ALL | Acute Lymphoblastic Leukemia |
| HME | Hereditary Multiple Exostosis |
| PCA | Posterior Cerebral Artery |
| PICA | Posterior Inferior Cerebellar Artery |
| CCJ | CranioCervical Junction |
| OCF | OccipitoCervical Fixation |
| GTR | Gross Total Resection |
| STR | Sub Total Resection |
| MRI | Magnetic Resonance Imagining |
| MC | multi-country |
| CT | computed tomography |
| DWI | Diffusion-Weighted Imaging |
References
- Mankin, H.J.; Hornicek, F.J.; Ortiz-Cruz, E.; Villafuerte, J.; Gebhardt, M.C. Aneurysmal bone cyst: A review of 150 patients. J. Clin. Oncol. 2005, 23, 6756–6762. [Google Scholar] [CrossRef] [PubMed]
- Saccomanni, B. Aneurysmal bone cyst of spine: A review of literature. Arch. Orthop. Trauma Surgery 2008, 128, 1145–1147. [Google Scholar] [CrossRef] [PubMed]
- Gan, Y.C.; Hockley, A.D. Aneurysmal bone cysts of the cranium in children: Report of three cases and brief review of the literature. J. Neurosurg. Pediatr. 2007, 106, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bhende, Y.M.; Kothare, S.N. Aneurysmal bone cyst; a case report. Ind. Med. Gaz. 1950, 85, 544–546. [Google Scholar] [PubMed] [PubMed Central]
- Blundell, J.E. Aneurysmal bone cysts. A Report of six cases, including a fatal case associated with a non-ossifying fibroma. Australas. Radiol. 1965, 9, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Odeku, E.L.; Mainwaring, A.R. Unusual aneurysmal bone cyst: A case report. J. Neurosurg. 1965, 22, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Costantini, F.E.; Iraci, G.; Benedetti, A.; Melanotte, P.L. Aneurysmal bone cyst as an intracranial space-occupying lesion. Case report. J. Neurosurg. 1966, 25, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Cacdac, M.A.; Malis, L.I.; Anderson, P.J. Aneurysmal parietal bone cyst. Case report. J. Neurosurg. 1972, 37, 237–241. [Google Scholar] [CrossRef] [PubMed]
- O’Gorman, A.M.; Kirkham, T.H. Aneurysmal bone cyst of the orbit with unusual angiographic features. Am. J. Roentgenol. 1976, 126, 896–899. [Google Scholar] [CrossRef] [PubMed]
- Chalapati Rao, K.V.; Rao, B.S.; Reddy, C.P.; Sundareshwar, B.; Reddy, C.R. Aneurysmal bone cyst of the skull. Case report. J. Neurosurg. 1977, 47, 633–636. [Google Scholar] [PubMed]
- Mufti, S.T. Aneurysmal bone cyst of the skull. Case report. J. Neurosurg. 1978, 49, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Luccarelli, G.; Fornari, M.; Savoiardo, M. Angiography and computerized tomography in the diagnosis of aneurysmal bone cyst of the skull: Case report. J. Neurosurg. 1980, 53, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Keuskamp, P.A.; Horoupian, D.S.; Fein, J.M. Aneurysmal bone cyst of the temporal bone presenting as a spontaneous intracerebral hemorrhage: Case report. Neurosurgery 1980, 7, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Komjátszegi, S. Aneurysmal bone cyst of the skull. J. Neurosurg. 1981, 55, 497. [Google Scholar] [PubMed]
- Kimmelman, C.P.; Potsic, W.P.; Schut, L. Aneurysmal bone cyst of the sphenoid in a child. Ann. Otol. Rhinol. Laryngol. 1982, 91, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Baker, H.L.; Papsidero, M.J.; Batsakis, J.G.; Krause, C.J. Aneurysmal bone cyst of the ethmoid. Head Neck Surg. 1982, 5, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Sanerkin, N.G.; Mott, M.G.; Roylance, J. An unusual intraosseous lesion with fibroblastic, osteoclastic, osteoblastic, aneurysmal and fibromyxoid elements. “Solid” variant of aneurysmal bone cyst. Cancer 1983, 51, 2278–2286. [Google Scholar] [CrossRef] [PubMed]
- Bilge, T.; Coban, O.; Ozden, B.; Turantan, I.; Türker, K.; Bahar, S. Aneurysmal bone cysts of the occipital bone. Surg. Neurol. 1983, 20, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Ameli, N.O.; Abbassioun, K.; Azod, A.; Saleh, H. Aneurysmal bone cyst of the skull. Can. J. Neurol. Sci. 1984, 11, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Calliauw, L.; Roels, H.; Caemaert, J. Aneurysmal bone cysts in the cranial vault and base of skull. Surg. Neurol. 1985, 23, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.; Guilburd, J.N.; Borovich, B.; Goldsher, D.; Mendelson, H.; Kerner, H. Occipital aneurysmal bone cyst: CT features. J. Comput. Assist. Tomogr. 1987, 11, 880–883. [Google Scholar] [CrossRef] [PubMed]
- Arthur, R.J.; Brunelle, F. Computerised tomography in the evaluation of expansile lesions arising from the skull vault in childhood—A report of 5 cases. Pediatr. Radiol. 1988, 18, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Rappaport, Z.H. Aneurysmal bone cyst associated with fibrous dysplasia of the skull. Neurochirurgia 1989, 32, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.V.; Yokoyama, C.; Moseley, I.F.; Wright, J.E. Aneurysmal bone cyst of the sphenoid with orbital involvement. Br. J. Ophthalmol. 1990, 74, 505–508. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dávid, K.; Horváth, Z.; Horváth, A.; Illés, T. Aneurysmal bone cyst of the occipital bone: Case report. Surg. Neurol. 1993, 40, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.Y.; Ragland, R.L.; Weaver, J.P.; Smith, T.W.; Knorr, J.R.; Weyreuther, M. Epidural mass related to calvarial aneurysmal bone cyst: Computed tomographic and magnetic resonance demonstration. J. Neuroimaging 1995, 5, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Chateil, J.F.; Dousset, V.; Meyer, P.; Pedespan, J.M.; San-Galli, F.; Rivel, J.; Caillé, J.M.; Diard, F. Cranial aneurysmal bone cysts presenting with raised intracranial pressure: Report of two cases. Neuroradiology 1997, 39, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Park, A.H.; Phillips, J.; Forte, V. Aneurysmal bone cyst of the temporal bone. Otolaryngol. Head Neck Surg. 1999, 120, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Petro, M.L.; Lancon, J.A. Occipital aneurysmal bone cyst. Pediatr. Neurosurg. 2001, 34, 45–46. [Google Scholar] [CrossRef] [PubMed]
- Roncaroli, F.; Consales, A.; Galassi, E.; Bernardi, B.; Valeri, B. Occipital aneurysmal bone cyst secondary to eosinophilic granuloma. Pediatr. Neurosurg. 2001, 35, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Itshayek, E.; Spector, S.; Gomori, M.; Segal, R. Fibrous dysplasia in combination with aneurysmal bone cyst of the occipital bone and the clivus: Case report and review of the literature. Neurosurgery 2002, 51, 815–817. [Google Scholar] [CrossRef] [PubMed]
- Mattei, T.A.; Mattei, J.A.; Ramina, R.; Aguiar, P.H. Fibrous dysplasia in combination with aneurysmal bone cyst presenting as a subarachnoid haemorrhage. Neurol. Sci. 2005, 26, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Iseri, P.K.; Efendi, H.; Demirci, A.; Komsuoglu, S. Fibrous dysplasia of the cranial bones: A case report and review of the literature. Yale J. Biol. Med. 2005, 78, 141–145. [Google Scholar] [PubMed] [PubMed Central]
- Lin, S.P.; Fang, Y.C.; Chu, D.C.; Chang, Y.C.; Hsu, C.I. Characteristics of cranial aneurysmal bone cyst on computed tomography and magnetic resonance imaging. J. Formos. Med. Assoc. 2007, 106, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Dong, Y.; Sun, K.; Lu, Y. A huge occipital osteoblastoma accompanied with aneurysmal bone cyst in the posterior cranial fossa. Clin. Neurol. Neurosurg. 2008, 110, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Segall, L.; Cohen-Kerem, R.; Ngan, B.Y.; Forte, V. Aneurysmal bone cysts of the head and neck in pediatric patients: A case series. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishnan, C.V.; Rao, B.R.; Nair, S.; Radhakrishnan, V.V.; Kesavadas, C. Intracranial intradural aneurysmal bone cyst: A unique case. Pediatr. Neurosurg. 2009, 45, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Kim, J.H.; Han, S.H.; Kang, H.I. Fibrous Dysplasia with Aneurysmal Bone Cyst Presenting as Painful Solitary Skull lesion. J. Korean Neurosurg. Soc. 2010, 48, 551–554. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abuzayed, B.; Dashti, R.; Turk, O.; Kaynar, M.Y. Aneurysmal frontal bone cyst in a child with history of acute lymphoblastic leukemia: A case of rare location and history. J. Pediatr. Hematol. Oncol. 2010, 32, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, C. Langerhans cell histiocytosis masquerading as aneurysmal bone cyst. J. Clin. Oncol. 2011, 29, e688–e690. [Google Scholar] [CrossRef] [PubMed]
- Genizi, J.; Srugo, I.; Attias, D.; Ben-Sira, L.; Braun, J.; Bamberger, E.S.; Margalit, N.; Constantini, S. Giant pediatric aneurysmal bone cysts of the occipital bone: Case report and review of the literature. Pediatr. Neurol. 2011, 45, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Umredkar, A.; Srinivasa, R. Giant pediatric aneurysmal bone cyst of the occipital bone: Case report and review of the literature. Neurol. India 2012, 60, 126–128. [Google Scholar] [CrossRef] [PubMed]
- Curtis, B.R.; Petteys, R.J.; Rossi, C.T.; Keating, R.F.; Magge, S.N. Large occipital aneurysmal bone cyst causing obstructive hydrocephalus in a pediatric patient. J. Neurosurg. Pediatr. 2012, 10, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Garber, S.T.; Riva-Cambrin, J.K. Occipital aneurysmal bone cyst rupture following head trauma: Case report. J. Neurosurg. Pediatr. 2015, 15, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Kalina, P.; Wetjen, N. Aneurysmal Bone Cyst of the Occipital Bone. J. Pediatr. 2015, 167, 496–496.e2. [Google Scholar] [CrossRef] [PubMed]
- Urgun, K.; Yılmaz, B.; Toktaş, Z.O.; Akakın, A.; Konya, D.; Demir, M.K.; Kılıç, T. Craniospinal Polyostotic Fibrous Dysplasia, Aneurysmal Bone Cysts, and Chiari Type 1 Malformation Coexistence in a Patient with McCune-Albright Syndrome. Pediatr. Neurosurg. 2016, 51, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Spina, A.; Boari, N.; Gagliardi, F.; Giudice, L.; Mortini, P. Atlanto-occipital dislocation due to aneurysmal bone cyst of the occipital condyle. Acta Neurochir. Wien. 2016, 158, 1637–1638. [Google Scholar] [CrossRef] [PubMed]
- Mete, M.; Duransoy, Y.K.; Çinar, C.; Ovali, G.; Temiz, P.; Selcuki, M. Giant occipital aneurysmal bone cyst caused to hydrocephalus in a child. Childs Nerv. Syst. 2017, 33, 1871–1873. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, C.; Bipin, C.; Rabiul, K.; Ananth Kumar, B.; Nazmin, A.; Raushan Kumar, C.; Ranjit Kumar, C. Aneurysmal Bone Cyst of the Occipital Bone. EC Neurol. 2018, 10, 1047–1051. [Google Scholar]
- Alves Filho, A.C.; Porfírio, A.S.; Ribeiro, W.C.S.; de Oliveira Fonseca, D.; Malta, M.V.; Camelo, R.C.; Camelo, R.M. Aneurysmal Bone Cyst of the Skull Base—Case Report. Arq. Bras. Neurocir. 2019, 38, 51–55. [Google Scholar] [CrossRef]
- Brohi, S.R.; Dilber, M.; Mallah, F.A. Secondary Aneurysmal Bone Cyst of Base of Skull Associated with Chondroblastoma. J. Coll. Physicians Surg. Pak. 2019, 29, 906–907. [Google Scholar] [CrossRef] [PubMed]
- Tse, G.H.; Jiang, F.Y.; Radatz, M.W.R.; Sinha, S.; Zaki, H. Skull base aneurysmal bone cyst presenting with hydrocephalus: Progressive residuum obliterated by Gamma Knife stereotactic radiosurgery in a pediatric patient. J. Neurosurg. Pediatr. 2020, 26, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Gotecha, S.; Punia, P.; Chugh, A.; Patil, A.; Kashyap, D.; Raghu, V.; Chhabra, S.; Patel, A.; Kotecha, M. A Rare Case of an Aneurysmal Bone Cyst of the Temporal Bone. Asian J. Neurosurg. 2020, 15, 699–702. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Farouk, A.G.; Mohammed, B.; Umar, U.H.; Wala, S.; Ahidjo, A. Giant pediatric aneurysmal bone cyst of the occipital bone: A case report and review of the literature. Med. J. Islam. World Acad. Sci. 2020, 28, 24–31. [Google Scholar] [CrossRef]
- Canzano, F.; Giombelli, E.; Cerasti, D.; Corradi, D.; Falcioni, M. Capillary Venous Malformation With Secondary Aneurysmal Bone Cyst of Temporal Bone. J. Int. Adv. Otol. 2021, 17, 471–474. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Borni, M.; Kolsi, F.; Cherif, I.; Boudawara, M.Z. Spontaneous rapid regression of a juvenile primary aneurysmal bone cyst of the skull: A case report and literature review. Radiol. Case Rep. 2022, 17, 1634–1639. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Woldow, A.; Foy, V.M. Aneurysmal bone cyst of the skull: A case report. SAGE Open Med. Case Rep. 2022, 10, 2050313X221117727. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- An, P.; Gao, P.; Liu, J.; Feng, G. Epithelioid Osteoblastoma Combined with Aneurysmal Bone Cyst Originating from the Right Temporal Bone and the Greater Wing of the Sphenoid Bone. Balkan Med. J. 2023, 40, 300–302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koketsu, Y.; Tanei, T.; Kuwabara, K.; Hasegawa, T.; Kato, T.; Maesawa, S.; Nishimura, Y.; Araki, Y.; Saito, R. Secondary aneurysmal bone cyst of the frontal bone with fibrous dysplasia showing rapid expansion: A case report. Nagoya J. Med. Sci. 2023, 85, 395–401. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alsabbagh, B.M.; Alessa, A.; Aljohani, H.; Alhammad, O. Large skull osteoblastoma presented as aneurysmal bone cyst (ABC). Neurosciences 2023, 28, 277–280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shen, C.F.; Yang, C.C.; Liu, S.Y.; Shen, C.C. Middle cranial fossa tumor presenting as chronic otitis media: Rare case of aneurysmal bone cyst. Int. J. Surg. Case Rep. 2023, 112, 108996. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mousavinejad, S.A.; Eraghi, M.M.; Tavasol, H.H.; Salarinezhad, Z.; Ansari, M.; Ebrahimzadeh, K.; Kazemi, R.; Sharifi, G.; Samadian, M.; Rezaei, O. A rare case of aneurysmal bone cyst of the frontal bone, and an overlook of literature. Interdiscip. Neurosurg. 2023, 34, 101859. [Google Scholar] [CrossRef]
- Oki, S.; Shima, T.; Uozumi, T.; Kodama, T. Aneurysmal bone cyst of the skull-A case report-(Author’s transl). No Shinkei Geka 1978, 6, 1197–1201. (In Japanese) [Google Scholar] [PubMed]
- Mima, S.; Taguchi, Y.; Sekino, H.; Inomata, I. Case of aneurysmal bone cyst of the skull. No Shinkei Geka 1984, 12, 825–831. (In Japanese) [Google Scholar] [PubMed]
- Ikeda, H.; Niizuma, H.; Suzuki, J.; Nagamine, Y.; Kameyama, M. Chemical embolization using estrogen for aneurysmal bone cyst of the skull: Case report. No Shinkei Geka 1985, 13, 203–208. (In Japanese) [Google Scholar] [PubMed]
- Tokarz, F.; Jankowski, R.; Zukiel, R.; Nowak, S. Torbiele tetniakowate czaski i kregosłupa leczone operacyjnie [Aneurysmal bone cyst of the skull and vertebral column treated operatively]. Neurol. Neurochir. Pol. 1993, 27, 533–540. (In Polish) [Google Scholar] [PubMed]
- Arnaldsson, O.S.; Ragnarsson, T. Aneurysmal bone cyst, following a skull trauma. A case report. Laeknabladid 1995, 81, 799–802. (In Icelandic) [Google Scholar] [PubMed]
- Clavel Escribano, M.; Robles Balibrea, A.; Clavel Laria, P.; Robles Cano, V. Quiste óseo aneurismático del hueso frontal. Caso clínico [Frontal bone aneurysmal cyst. Case report]. Neurocirugia 2001, 12, 166–169. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Nakaoka, T.; Matsuura, H.; Kamada, H.; Yamamoto, Y.; Itoh, K. A case of calvarial aneurysmal bone cyst: Transcranial contrast sonographic examination with pulse inversion harmonic imaging method. No To Shinkei 2002, 54, 1075–1080. (In Japanese) [Google Scholar] [PubMed]
- Mazlout, O.; Dfouni, N.; Ladeb, M.F.; Becker, M. Kyste osseux anévrismal de l’ethmoïde [Aneurysmal bone cyst of the ethmoid bone]. J. Radiol. 2005, 86, 948–950. (In French) [Google Scholar] [CrossRef] [PubMed]
- Broc-Haro, G.G.; Rodríguez-Valencia, F.; Manrique-Guzmán, S. Quiste óseo aneurismático de cráneo con resolución espontánea. Reporte de un caso [Spontaneous regression of aneurysmal bone cyst of the skull. Case report]. Cir. Cir. 2007, 75, 49–51. (In Spanish) [Google Scholar] [PubMed]
- Wendt, S.; Flügel, W.; Spuler, A.; Mairinger, T.; Hoch, H.; Bloching, M. Aneurysmatische Knochenzyste der Rhinobasis bei einem 3-jährigen Kind: Seltene Lokalisation einer benignen Knochenläsion [Aneurysmal bone cyst of the ethmoid sinus and skull base in a 3-year old child: A rare location of a benign bone lesion]. HNO 2010, 58, 57–62. (In German) [Google Scholar] [CrossRef] [PubMed]
- Abdoulkader, F.; Aammou, K.; Siwane, A.; Essodegui, F. Une localisation rare au sphénoïde d’un kyste osseux anévrysmal [Rare localization of aneurysmal bone cyst in the sphenoid bone]. Pan Afr. Med. J. 2017, 27, 231. (In French) [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, M.; Zhu, X.Y.; Wang, L.H.; Zhang, T.; Zhang, X.L.; Rao, X.S. Primary osteosarcoma of the skull with aneurysmal bone cyst like change: Report of a case. Zhonghua Bing Li Xue Za Zhi 2021, 50, 1382–1384. (In Chinese) [Google Scholar] [PubMed]
- Ao, J.W.; Chen, Q.R. Aneurysmal bone cyst of mandible: Report of a case. Zhonghua Bing Li Xue Za Zhi 2022, 51, 564–566. (In Chinese) [Google Scholar] [PubMed]
- Bull, I.; MBell, C.; Storli, S.H. Maxillary Aneurysmal Bone Cyst in a Young Dog-A Case Report. J. Vet. Dent. 2024, 41, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Syed, A.N.; Talwar, D.; Kell, D.; Arkader, A. Predicting Blood Loss in Aneurysmal Bone Cyst Surgery. J. Pediatr. Orthop. 2025, 45, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Hino, N.; Ohtsuka, K.; Hashimoto, M.; Sakata, M. Radiographic features of an aneurysmal bone cyst of the orbit. Ophthalmologica 1998, 212, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Yarington, C.T., Jr.; Abbott, J.; Raines, D. Aneurysmal bone cyst of the maxilla; association with giant cell reparative granuloma. Arch. Otolaryngol. 1964, 80, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Fite, J.D.; Schwartz, J.F.; Calhoun, F.P., Jr. Aneurysmal bone cyst of the orbit (a clinicopathologic case report). Trans. Am. Acad. Ophthalmol. Otolaryngol. 1968, 72, 614–618. [Google Scholar] [PubMed]
- Eveson, J.W.; Moos, K.F.; MacDonald, D.G. Aneurysmal bone cyst of the zygomatic arch. Br. J. Oral Surg. 1978, 15, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Rasi, H.B.; Swamy, P.T.; Alpert, L.I.; Bochetto, J.; Giovanniello, J. Aneurysmal bone cyst of zygoma. N. Y. State J. Med. 1978, 78, 1937–1941. [Google Scholar] [PubMed]
- Matt, B.H. Aneurysmal bone cyst of the maxilla: Case report and review of the literature. Int. J. Pediatr. Otorhinolaryngol. 1993, 25, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Winters, V.; Schraepen, T.; Geusens, E.; Vanwijck, R.; Broeckx, J. Aneurysmal bone cyst of the zygomatic arch. J. Belge. Radiol. 1998, 81, 7–8. [Google Scholar] [PubMed]
- Senol, U.; Karaali, K.; Akyüz, M.; Gelen, T.; Tuncer, R.; Lüleci, E. Aneurysmal bone cyst of the orbit. AJNR Am. J. Neuroradiol. 2002, 23, 319–321. [Google Scholar] [PubMed] [PubMed Central]
- Sánchez, A.P.; Diaz-Lopez, E.O.; Rojas, S.K.; Neri, H.A.; Valle, P.L.; Pine, S.S. Aneurysmal bone cyst of the maxilla. Craniofac. Surg. 2004, 15, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Perrotti, V.; Rubini, C.; Fioroni, M.; Piattelli, A. Solid aneurysmal bone cyst of the mandible. Int. J. Pediatr. Otorhinolaryngol. 2004, 68, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Smolka, W.; Lieger, O.; Balmer, M.C.; Brekenfeld, C.; Iizuka, T.; Smolka, K. Aneurysmal bone cyst of the tuberculum articulare of the temporomandibular joint: A case report. Quintessence Int. 2008, 39, 679–683. [Google Scholar] [PubMed]
- Pelo, S.; Gasparini, G.; Boniello, R.; Moro, A.; Amoroso, P.F. Aneurysmal bone cyst located in the mandibular condyle. Head Face Med. 2009, 5, 8. [Google Scholar] [PubMed] [PubMed Central]
- Roychoudhury, A.; Rustagi, A.; Bhatt, K.; Bhutia, O.; Seith, A. Aneurysmal bone cyst of the mandible: Report of 3 cases. J. Oral Maxillofac. Surg. 2009, 67, 1996–2004. [Google Scholar] [CrossRef] [PubMed]
- Bozbuğa, M.; Süslü, H.T. Aneurysmal bone cyst of the sphenoid bone extending into the ethmoid sinus, nasal cavity and orbita in a child. Turk. Neurosurg. 2009, 19, 172–176. [Google Scholar] [PubMed]
- Sun, Z.J.; Sun, H.L.; Yang, R.L.; Zwahlen, R.A.; Zhao, Y.F. Aneurysmal bone cysts of the jaws. Int. J. Surg. Pathol. 2009, 17, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Breuer, C.; Paul, H.; Zimmermann, A.; Braunstein, S.; Schaper, J.; Mayatepek, E.; Oh, J. Mandibular aneurysmal bone cyst in a child misdiagnosed as acute osteomyelitis: A case report and a review of the literature. Eur. J. Pediatr. 2010, 169, 1037–1040. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.J.; Choi, S.C.; Kwon, Y.D.; Drew, S.J. Aneurysmal bone cyst causing a pathologic fracture of the mandibular condyle. J. Oral Maxillofac. Surg. 2011, 69, 2995–3000. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.M.; Cho, K.S.; Choi, K.U.; Roh, H.J. Aggressive aneurysmal bone cyst of the maxilla confused with telangiectatic osteosarcoma. Auris Nasus Larynx 2012, 39, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.K.; Kumar, R.; Bal, A.; Panda, N.K. Aneurysmal bone cyst of maxilla with ectopic molar tooth—a case report. Otolaryngol. Pol. 2013, 67, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Simsek, G.; Saka, C.; Sonbay, D.N.; Akin, I.; Koybasioglu, F. Aneurysmal bone cyst in the middle turbinate: A case report. Ear Nose Throat J. 2013, 92, E47. [Google Scholar] [CrossRef] [PubMed]
- Lerant, G.; Ivanyi, E.; Toth, E.; Levai, A.; Godeny, M. Aneurysmal bone cyst of the zygomatic arch: A case report. Clin. Imaging 2013, 37, 957–961. [Google Scholar] [CrossRef] [PubMed]
- Janjua, N.; Cresswell, M.; Sharma, R.; Maheshwar, A. Aneurysmal bone cyst of the ethmoid bone. BMJ Case Rep. 2014, 2014, bcr2013202319. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, J.Y.; Ko, Y.I.; Kwon, H.; Jung, S.N. Aneurysmal bone cyst of the zygomatic bone. J. Craniofac. Surg. 2014, 25, e148–e149. [Google Scholar] [CrossRef] [PubMed]
- Neuschl, M.; Reinert, S.; Gülicher, D.; Neuschl, J.; Hoffmann, J. Aneurysmal bone cyst of the ascending ramus mandible. A case report. J. Craniomaxillofac. Surg. 2014, 42, e36–e38. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, A.; Sharma, R.; Muralidharan, C.G. Sagittal split ramus osteotomy for aneurysmal bone cyst of the mandibular condyle. J. Craniofac. Surg. 2015, 26, e38–e39. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Zhang, M.; Zhao, X.X. Aneurysmal bone cyst of the orbit. Chin. Med. J. 2015, 128, 562–563. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, K.; Guo, C.; Guo, R.; Meng, J. A Giant Aneurysmal Bone Cyst in the Mandibular Condyle. J. Craniofac. Surg. 2017, 28, e148–e151. [Google Scholar] [CrossRef] [PubMed]
- Toescu, S.M.; Alalade, A.F.; Steele, L.; Bhargava, D.; Hunter, R. Frontal skull osteoblastoma with aneurysmal bone cyst-like changes associated with trauma during pregnancy: A case report. Acta Neurochir. 2017, 159, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Arocho-Quinones, E.V.; Self, S.; Suchi, M.; Zwagerman, N.T.; Lew, S.M. Spheno-Orbital Aneurysmal Bone Cyst in a 10-Month-Old Infant. World Neurosurg. 2018, 117, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Asi, K.W.; Abdelmeguid, A.; Bell, D.; Hanna, E.Y. Massive aneurysmal bone cyst of the skull base treated with denosumab. Head Neck 2018, 40, E107–E113. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, M.; Pardhe, N.; Vijay, P. Aneurysmal Bone Cyst of Mandible with Classical Histopathological Presentation. J. Coll. Physicians Surg. Pak. 2018, 28, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Rațiu, C.; Ilea, A.; Gal, F.A.; Ruxanda, F.; Boşca, B.A.; Miclăuș, V. Mandibular aneurysmal bone cyst in an elderly patient: Case report. Gerodontology 2018, 35, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.J.; Choby, G.; Van Gompel, J.J.; Link, M.J.; Van Abel, K.M. Aneurysmal Bone Cysts of the Paranasal Sinuses: The Mayo Clinic Experience and Review of the Literature. Laryngoscope 2021, 131, E2525–E2533. [Google Scholar] [CrossRef] [PubMed]
- Foo, M.I.; Nicol, K.; Murakami, J.W. Skull base chondroblastoma with aneurysmal bone cyst-like changes treated with percutaneous radiofrequency ablation and doxycycline sclerotherapy: Illustrative case. J. Neurosurg. Case Lessons 2022, 4, CASE22436. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yahaya, J.J.; Morgan, E.D.; Abraham, Z.S.; Othieno, E. Aneurysmal bone cyst of the mandible: A rare case report and literature review. Ann. Med. Surg. 2023, 85, 5133–5137. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mo, J.T.; Darrow, M.A.; Sharma, J.D. Langerhans cell histiocytosis with aneurysmal bone cyst-like changes: A case-based literature review. Childs Nerv. Syst. 2023, 39, 3057–3064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Phan, T.; Tong, J.; Krivanek, M.; Graf, N.; Dexter, M.; Tumuluri, K. Aneurysmal Bone Cyst of the Orbit With USP6 Gene Rearrangement. Ophthalmic Plast. Reconstr. Surg. 2023, 39, 206–210. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.; Hayat, F.; Amasa, S.; Ammar Haider, M.; Akram Asbeutah, S.; AlDallal, U.; Barrie, U.; Ismail, M. Rare Aneurysmal Bone Cyst Presentation in the Orbit: A Systematic Review of the Literature with an Illustrative Case Report. World Neurosurg. 2024, 191, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Han, S.I.; Lim, S.C. Intraosseous hemangioma with aneurysmal bone cyst-like changes of the hyoid bone: Case report and literature review. Medicine 2024, 103, e37137. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jaffe, H.L.; Lichtenstein, L. Solitary unicameral bone cyst: With emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch. Surg. 1942, 44, 1004–1025. [Google Scholar] [CrossRef]
- Lichtenstein, L. Aneurysmal Bone Cyst: Pathological Entity Commonly Mistaken for Giant-Cell Tumor and Occasionally for Hemangioma and Osteogenic Sarcoma. Cancer 1950, 3, 279–289. [Google Scholar] [CrossRef]
- Lau, A.W.; Pringle, L.M.; Quick, L.; Riquelme, D.N.; Ye, Y.; Oliveira, A.M.; Chou, M.M. TRE17/ubiquitin-specific protease 6 (USP6) oncogene translocated in aneurysmal bone cyst blocks osteoblastic maturation via an autocrine mechanism involving bone morphogenetic protein dysregulation. J. Biol. Chem. 2010, 285, 37111–37120. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cottalorda, J.; Bourelle, S. Modern concepts of primary aneurysmal bone cyst. Arch. Orthop. Trauma Surg. 2007, 127, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, L.S.; Shenker, A.; Gejman, P.V.; Merino, M.J.; Friedman, E.; Spiegel, A.M. Activating mutations of the stimulatory G protein in the McCune-Albright syndrome. N. Engl. J. Med. 1991, 325, 1688–1695. [Google Scholar] [CrossRef] [PubMed]
- Riminucci, M.; Saggio, I.; Robey, P.G.; Bianco, P. Fibrous dysplasia as a stem cell disease. J. Bone Miner. Res. 2006, 21, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Rehman, R.; Dekhou, A.; Osto, M.; Agemy, J.; Chaaban, A.; Yuhan, B.; Thorpe, E. Aneurysmal Bone Cysts of the Craniofacial Origin: A Systematic Review. OTO Open 2021, 5, 2473974X211052950. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caro, P.A.; Mandell, G.A.; Stanton, R.P. Aneurysmal bone cyst of the spine in children. MRI imaging at 0.5 tesla. Pediatr. Radiol. 1991, 21, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Muratori, F.; Mondanelli, N.; Rizzo, A.R.; Beltrami, G.; Giannotti, S.; Capanna, R.; Campanacci, D.A. Aneurysmal Bone Cyst: A Review of Management. Surg. Technol. Int. 2019, 35, 325–335. [Google Scholar] [PubMed]
- Hauschild, O.; Lüdemann, M.; Engelhardt, M.; Baumhoer, D.; Baumann, T.; Elger, T.; Südkamp, N.P.; Herget, G.W. Aneurysmal bone cyst (ABC): Treatment options and proposal of a follow-up regime. Acta Orthop. Belg. 2016, 82, 474–483. [Google Scholar] [PubMed]
- Parker, J.; Soltani, S.; Boissiere, L.; Obeid, I.; Gille, O.; Kieser, D.C. Spinal Aneurysmal Bone Cysts (ABCs): Optimal Management. Orthop. Res. Rev. 2019, 1, 159–166. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yildiz, C.; Erler, K.; Atesalp, A.S.; Basbozkurt, M. Benign bone tumors in children. Curr. Opin. Pediatr. 2003, 15, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Strohm, J.A.; Strohm, P.C.; Kühle, J.; Schmal, H.; Zwingmann, J. Management of juvenile and aneurysmal bone cysts: A systematic literature review with meta-analysis. Eur. J. Trauma Emerg. Surg. 2023, 49, 361–372. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Döring, K.; Puchner, S.; Vertesich, K.; Funovics, P.T.; Hobusch, G.; Sulzbacher, I.; Chiari, C.; Windhager, R. Results in the surgical treatment of aneurysmal bone cysts-A retrospective data analysis. Orthop. Traumatol. Surg. Res. 2022, 108, 103095. [Google Scholar] [CrossRef] [PubMed]
- Tillman, B.P.; Dahlin, D.C.; Lipscomb, P.R.; Stewart, J.R. Aneurysmal bone cyst: An analysis of ninety-five cases. Mayo Clin. Proc. 1968, 43, 478–495. [Google Scholar] [PubMed]
- Ruiter, D.J.; van Rijssel, T.G.; van der Velde, E.A. Aneurysmal bone cysts: A clinicopathological study of 105 cases. Cancer 1977, 39, 2231–2239. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.T.; Jiang, S.; Cen, Y. Fibrous dysplasia of skull. J. Craniofac. Surg. 2010, 21, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.M.; Perez-Atayde, A.R.; Inwards, C.Y.; Medeiros, F.; Derr, V.; Hsi, B.L.; Gebhardt, M.C.; Rosenberg, A.E.; Fletcher, J.A. USP6 and CDH11 oncogenes identify the neoplastic cell in primary aneurysmal bone cysts and are absent in so-called secondary aneurysmal bone cysts. Am. J. Pathol. 2004, 165, 1773–1780. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Oliveira, A.M.; Hsi, B.L.; Weremowicz, S.; Rosenberg, A.E.; Dal Cin, P.; Joseph, N.; Bridge, J.A.; Perez-Atayde, A.R.; Fletcher, J.A. USP6 (Tre2) fusion oncogenes in aneurysmal bone cyst. Cancer Res. 2004, 64, 1920–1923. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.M.; Chou, M.M.; Perez-Atayde, A.R.; Rosenberg, A.E. Aneurysmal bone cyst: A neoplasm driven by upregulation of the USP6 oncogene. J. Clin. Oncol. 2006, 24, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Antonescu, C.R.; Yoshida, A.; Guo, T.; Chang, N.E.; Zhang, L.; Agaram, N.P.; Qin, L.X.; Brennan, M.F.; Singer, S.; Maki, R.G. KDR activating mutations in human angiosarcomas are sensitive to specific kinase inhibitors. Cancer Res. 2009, 69, 7175–7179. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Panoutsakopoulos, G.; Pandis, N.; Kyriazoglou, I.; Gustafson, P.; Mertens, F.; Mandahl, N. Recurrent t(16;17)(q22;p13) in aneurysmal bone cysts. Genes. Chromosomes Cancer 1999, 26, 265–266. [Google Scholar] [CrossRef] [PubMed]
- Behjati, S.; Tarpey, P.S.; Presneau, N.; Scheipl, S.; Pillay, N.; Van Loo, P.; Wedge, D.C.; Cooke, S.L.; Gundem, G.; Davies, H.; et al. Distinct H3F3A and H3F3B driver mutations define chondroblastoma and giant cell tumor of bone. Nat. Genet. 2013, 45, 1479–1482, Erratum in Nat. Genet. 2014, 46, 316. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) | Year | Country | N° Patient | Age | Gender | Affected Bone | Symptoms and Signs | Trauma | FD | Treatment | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bhende [5] | 1950 | India | 1 | 9 | M | Temporal bone | Painless nodule | Yes | No | Resection | - |
| Blundell [6] | 1965 | Australia | 1 | 53 | M | Parietal bone | Paralysis of left leg weaking of left arm | No | No | Resection | Deceased |
| Odeku [7] | 1965 | Nigeria | 1 | 6 | M | Occipital bone | Fever Severe occipital headaches Transient vomit | No | No | Resection | Deceased |
| Costantini [8] | 1966 | Italy | 1 | 14 | F | Frontal bone | Vomit Continuous bilateral frontal headaches Bilateral sixth cranial nerve paresis Slight right hemiparesis Papilledema | No | No | Resection | 5 yrs |
| Cacdac [9] | 1972 | USA | 1 | 17 | F | Parietal bone | Occasional headaches | No | No | Resection | N/A |
| O’Gorman [10] | 1976 | Canada | 1 | 1 | M | Ethmoid bone | Left proptosis Restriction of eyes movement | No | No | Resection | 2 yrs |
| Rao [11] | 1977 | India | 1 | 14 | M | Temporal bone | Headache and neck pain | No | No | Biopsy, resection | N/A |
| Mufti [12] | 1978 | Iraq | 1 | 25 | F | Frontal bone | Symptomless | Yes | No | Resection | N/A |
| Luccarelli [13] | 1980 | Italy | 1 | 19 | F | Occipital bone | Pulsating headache and vertigo Right sixth nerve palsy Ataxic gait | No | No | Resection | 1 yr |
| Keuskamp [14] | 1980 | USA | 1 | 62 | M | Temporal bone | Cheyne-Stokes breathing Decerebrate posture Left oculomotor palsy | No | No | Resection | 2 mos |
| Komjátszegi [15] | 1981 | Romania | 1 | 11 | M | Occipital bone | Symptomless | Yes | No | Resection | 5 yrs |
| Kimmelman [16] | 1982 | USA | 1 | 10 | M | Sphenoid bone | Decreased vision | No | No | Two stages resection | 4 mos |
| Baker [17] | 1982 | USA | 1 | 20 | F | Ethmoid bone | Nasal obstruction Periorbital swelling with mild proptosis Blurred vision and occasional diplopia | No | No | Biopsy, resection | 2 yrs |
| Sanerkin [18] | 1983 | UK | 1 | 5 | M | Ethmoid bone | Proptosis right eye | No | No | Resection | 3 yrs |
| Bilge [19] | 1983 | Turkey | 2 | 3, 18 | F, M | Occipital bone | Headaches, vomit and vertigo Papilledema Bilateral sixth nerve palsies, cerebellar signs | No | No | Resection | 1.5 yrs, 1 yr |
| Ameli [20] | 1984 | Albania | 4 | 13, 16, 25, 20 | F, F, M, M | Frontal, sphenoid, frontal, parietal bone | Headache Exophthalmos | Yes, no, no, yes | No | Resection | 5 yrs, 6 yrs, N/A, 1 yr |
| Calliauw [21] | 1985 | Belgium | 3 | 2 mos, 36, 19 | M, M, F | Parietal, temporal, temporal bone | Deafness Facial palsy and sensory loss Pain | No | No | Resection | 2 yrs, 2.5 yrs, 1.5 yrs |
| Braun [22] | 1987 | Israel | 1 | 4 | F | Occipital bone | Symptomless | No | No | Resection, radiotherapy | 4 mos |
| Arthur [23] | 1988 | France | 2 | 9, 9 | F, M | Occipital, frontal bone | Ophthalmoplegia, exophthalmos, papilledema | Yes, no | No | Resection, embolization and resection | N/A |
| Rappaport [24] | 1989 | Israel | 1 | 25 | M | Occipital bone | Pain | Yes | Yes | Resection | N/A |
| Hunter [25] | 1990 | UK | 1 | 7 | M | Sphenoid bone | Periorbital swelling and proptosis | No | No | Biopsy, resection | 1 yr |
| Dávid [26] | 1993 | Hungary | 1 | 21 | M | Occipital bone | Headaches, nausea, dizziness, and vomiting | No | No | Resection | 3 yrs |
| Lau [27] | 1995 | USA | 1 | 15 | M | Occipital bone | Nausea and visual changes | No | No | Resection | N/A |
| Chateil [28] | 1997 | France | 2 | 7, 9 | M, F | Temporal, occipital bone | Diplopia, headache, vomit, sixth nerve palsy | No, yes | No | Resection, biopsy and resection | N/A |
| Park [29] | 1999 | Canada | 1 | 4 | M | Temporal bone | Otorrhea with otalgia | No | Yes | Resection | 1 yr |
| Petro [30] | 2001 | USA | 1 | 7 | F | Occipital bone | Headache and hydrocephalus | No | No | Resection | N/A |
| Roncaroli [31] | 2001 | Italy | 1 | 2 | M | Occipital bone | Symptomless | No | No | Resection | N/A |
| Itshayek [32] | 2002 | Israel | 1 | 19 | M | Occipital bone | Symptomless | No | Yes | Biopsy, embolization, resection | 1 yr |
| Mattei [33] | 2005 | Brazil | 1 | 19 | F | Parietal and occipital bone | Headache, nuchal rigidity, SAH | No | Yes | Subtotal resection, administration of Zumeta and a hormonal blocker | N/A |
| Iseri [34] | 2005 | Turkey | 1 | 35 | F | Occipital bone | Gait disturbance, swallowing difficulty, slurring of speech, vertigo, altered sensation of hands | No | Yes | Administration of Alendronate | N/A |
| Lin [35] | 2007 | Taiwan | 1 | 54 | F | Occipital bone | Symptomless | No | Yes | Resection | 5 mos |
| Gan [3] | 2007 | UK | 3 | 5, 8, 4 | F, M, F | Temporal, occipital, temporal bone | Exophthalmos, double vision | No | No | Biopsy and resection, resection, biopsy and resection | 3 yrs, 3 yrs, 4 yrs |
| Han [36] | 2008 | China | 1 | 20 | M | Occipital | Headache | No | No | Resection | 18 mos |
| Segall [37] | 2008 | Canada | 4 | 4, 7, 7, 5 mos | M, M, F, F | Temporal, parietal, frontal, ethmoid | Pain, facial paresis, visual loss with proptosis, orbital deformity | No | No | Resection, resection, embolization and resection, resection | 10 yrs, 5 yrs, 3 yrs, 2.5 yrs |
| Gopalakrishnan [38] | 2009 | India | 1 | 14 | M | Sphenoid bone | Headache, focal seizure | No | No | Resection | N/A |
| Lee [39] | 2010 | South Korea | 1 | 18 | F | Frontal bone | Headache | No | Yes | Resection | N/A |
| Abuzayed [40] | 2010 | Turkey | 1 | 11 | F | Frontal bone | Symptomless | No | No | Resection | N/A |
| Krishnan [41] | 2011 | USA | 1 | 8 | F | Occipital bone | Symptomless | No | No | Resection | 6 mos |
| Genizi [42] | 2011 | Israel | 1 | 2 | M | Occipital bone | Headache and stumbling | No | No | Resection | 6 mos |
| Umredkar [43] | 2012 | India | 1 | 8 | M | Occipital bone | Pain | No | No | Resection | 6 mos |
| Curtis [44] | 2012 | USA | 1 | 16 | M | Occipital bone | Obstructive hydrocephalus | No | No | Resection | N/A |
| Garber [45] | 2015 | USA | 1 | 3 | F | Occipital bone | Vomited, lethargic, GCS 10 | Yes | No | Resection | 6 mos |
| Kalina [46] | 2015 | USA | 1 | 9 | M | Occipital bone | Headache, emesis, dizziness | No | No | Resection | N/A |
| Urgun [47] | 2016 | USA | 1 | 14 | F | Occipital bone | Symptomless | No | Yes | Resection | N/A |
| Spina [48] | 2016 | Italy | 1 | 22 | N/A | Occipital condyle | Neck pain | No | No | Resection | 3 yrs |
| Mete [49] | 2017 | Turkey | 1 | 12 | F | Occipital bone | Headache and vomit | Yes | No | Resection | N/A |
| Chaurasia [50] | 2018 | Bangladesh | 1 | 19 | F | Occipital bone | Headache | No | No | Resection | N/A |
| Alves Filho [51] | 2019 | Brazil | 1 | 17 | F | Sphenoid bone | Headache | No | No | Biopsy | N/A |
| Brohi [52] | 2019 | Pakistan | 1 | 50 | M | Temporal bone | Headache, facial nerve palsy | No | No | Resection | 1 yr |
| Tse [53] | 2020 | MC * | 1 | 11 | F | Occipital bone | Headache, nystagmus | Yes | No | Resection, embolization, gamma knife | 8 yrs |
| Gotecha [54] | 2020 | India | 1 | 3 | M | Temporal bone | Symptomless | No | No | Resection | N/A |
| Farouk [55] | 2020 | Nigeria | 1 | 7 | M | Occipitoparietal bone | Headache | No | No | Resection | N/A |
| Canzano [56] | 2021 | Italy | 1 | 5 | M | Temporal bone | Facial palsy | No | No | Embolization, resection | 2 yrs |
| Borni [57] | 2022 | Tunisia | 1 | 7 | M | Frontal bone | Symptomless | No | No | Spontaneous regression | 3 mos |
| Woldow [58] | 2022 | USA | 1 | 14 | M | Temporal bone | Symptomless | No | No | Resection | N/A |
| An [59] | 2023 | China | 1 | 16 | F | Temporal bone | Headache and dizziness | No | No | Resection | 1 yr |
| Koketsu [60] | 2023 | Japan | 1 | 19 | F | Frontal bone | Symptomless | No | No | Resection | N/A |
| Alsabbagh [61] | 2023 | KSA | 1 | 9 | M | Occipital bone | Headache, nausea, vomit, hydrocephalus | No | No | EVD placement and resection | N/A |
| Shen [62] | 2023 | Taiwan | 1 | 34 | M | Temporal bone | Otorrhea, mild tinnitus, hearing loss, and occasional headache | No | No | Resection | N/A |
| Mousavinejad [63] | 2023 | Iran | 1 | 17 | M | Frontal bone | Symptomless | No | No | Resection | 2 yrs |
| Our case report | 2025 | Italy | 1 | 14 | M | Occipital condyle | Headache, dizziness, impaired vision, and fall | No | No | Resection | 1 yr |
| Author(s) | Year | Country | Reason for Exclusion |
|---|---|---|---|
| Oki [64] | 1978 | Japan | Not-English article |
| Mima [65] | 1984 | Japan | Not-English article |
| Ikeda [66] | 1985 | Japan | Not-English article |
| Tokarz [67] | 1993 | Poland | Not-English article |
| Arnaldsson [68] | 1995 | Iceland | Not-English article |
| Clavel [69] | 2001 | Spain | Not-English article |
| Nakaoka [70] | 2002 | Japan | Not-English article |
| Mazlout [71] | 2005 | France | Not-English article |
| Broc-Haro [72] | 2007 | Spain | Not-English article |
| Wendt [73] | 2010 | Germany | Not-English article |
| Abdoulkader [74] | 2017 | France | Not-English article |
| Zhang [75] | 2021 | China | Not-English article |
| Ao [76] | 2022 | China | Not-English article |
| Bull [77] | 2024 | USA | Animal study |
| Syed [78] | 2025 | USA | No case report reported |
| Hino [79] | 1998 | Japan | Radiological study |
| Yarington [80] | 1964 | USA | Anatomical location outside the skull |
| Fite [81] | 1968 | USA | Anatomical location outside the skull |
| O’Gorman [10] | 1976 | Canada | Anatomical location outside the skull |
| Eveson [82] | 1978 | UK | Anatomical location outside the skull |
| Rasi [83] | 1978 | USA | Anatomical location outside the skull |
| Matt [84] | 1993 | USA | Anatomical location outside the skull |
| Winters [85] | 1998 | Belgium | Anatomical location outside the skull |
| Senol [86] | 2002 | Turkey | Anatomical location outside the skull |
| Sánchez [87] | 2004 | Mexico | Anatomical location outside the skull |
| Perrotti [88] | 2004 | Italy | Anatomical location outside the skull |
| Smolka [89] | 2008 | Switzerland | Anatomical location outside the skull |
| Pelo [90] | 2009 | Italy | Anatomical location outside the skull |
| Roychoudhury [91] | 2009 | India | Anatomical location outside the skull |
| Bozbuğa [92] | 2009 | Turkey | Anatomical location outside the skull |
| Sun [93] | 2009 | China | Anatomical location outside the skull |
| Breuer [94] | 2010 | Germany | Anatomical location outside the skull |
| Choi [95] | 2011 | Republic of Korea | Anatomical location outside the skull |
| Lee [96] | 2012 | Republic of Korea | Anatomical location outside the skull |
| Verma [97] | 2013 | India | Anatomical location outside the skull |
| Simsek [98] | 2013 | Turkey | Anatomical location outside the skull |
| Lerant [99] | 2013 | Hungary | Anatomical location outside the skull |
| Janjua [100] | 2014 | UK | Anatomical location outside the skull |
| Lee [101] | 2014 | Republic of Korea | Anatomical location outside the skull |
| Neuschl [102] | 2014 | Germany | Anatomical location outside the skull |
| Bhandari [103] | 2015 | India | Anatomical location outside the skull |
| Wang [104] | 2015 | China | Anatomical location outside the skull |
| Liu [105] | 2017 | China | Anatomical location outside the skull |
| Toescu [106] | 2017 | UK | Anatomical location outside the skull |
| Arocho [107] | 2018 | USA | Anatomical location outside the skull |
| Asi [108] | 2018 | USA | Anatomical location outside the skull |
| Bajpai [109] | 2018 | India | Anatomical location outside the skull |
| Rațiu [110] | 2018 | Romania | Anatomical location outside the skull |
| Smith [111] | 2021 | USA | Anatomical location outside the skull |
| Foo [112] | 2022 | USA | Anatomical location outside the skull |
| Yahaya [113] | 2023 | Tanzania | Anatomical location outside the skull |
| Mo [114] | 2023 | USA | Anatomical location outside the skull |
| Phan [115] | 2023 | Australia | Anatomical location outside the skull |
| O’Leary [116] | 2024 | USA | Anatomical location outside the skull |
| Oh [117] | 2024 | Republic of Korea | Anatomical location outside the skull |
| N° Patients | Mean Age | Male(s) | Genetic Disorders | Fibrous Dysplasia | Previous Trauma | Growth Tendency |
|---|---|---|---|---|---|---|
| 74 | 14.8 ± 12.5 yrs | 42 | 2 | 13 | 10 | 39 |
| Symptomatic | Mean follow-up | GTR | STR | Biopsy | Conservative | Embolization |
| 52 | 24.7 ± 23.2 mos | 67 | 7 | 0 | 2 | 7 |
| N° early complications | Early complications | N° late complications | Recurrence | Time of recurrency | * Lesion size | |
| 9 | Occipital bone:
| 0 | 5 | 0.6 ± 2.5 mos | 64 mm | |
| Occipital bone | Temporal bone | Frontal bone | Parietal bone | Ethmoidal bone | Sphenoid bone | |
| 32 | 16 | 11 | 6 | 4 | 5 | |
| Contingency Tables | ||||
|---|---|---|---|---|
| Growth Trend: | ||||
| Location: | Gender: | No | Yes | Total |
| occipital | female | 10 | 6 | 16 |
| male | 7 | 9 | 16 | |
| Total | 17 | 15 | 32 | |
| temporal | female | 1 | 3 | 4 |
| male | 5 | 7 | 12 | |
| Total | 6 | 10 | 16 | |
| frontal | female | 3 | 4 | 7 |
| male | 3 | 1 | 4 | |
| Total | 6 | 5 | 11 | |
| parietal | female | 1 | 0 | 1 |
| male | 1 | 4 | 5 | |
| Total | 2 | 4 | 6 | |
| ethmoidal | female | 1 | 1 | 2 |
| male | 0 | 2 | 2 | |
| Total | 1 | 3 | 4 | |
| sphenoid | female | 1 | 1 | 2 |
| male | 2 | 1 | 3 | |
| Total | 3 | 2 | 5 | |
| Total | female | 17 | 15 | 32 |
| male | 18 | 24 | 42 | |
| Total | 35 | 39 | 74 | |
| Chi-Squared Tests | ||||
| Location: | Value | df | p | |
| occipital | Χ2 | 1.200 | 1 | 0.273 |
| N | 30 | |||
| temporal | Χ2 | 0.280 | 1 | 0.597 |
| N | 14 | |||
| frontal | Χ2 | 1.102 | 1 | 0.294 |
| N | 9 | |||
| parietal | Χ2 | 5.000 | 1 | 0.025 |
| N | 5 | |||
| ethmoidal | Χ2 | NaN | ||
| N | 3 | |||
| sphenoid | Χ2 | 0.000 | 1 | 1.000 |
| N | 4 | |||
| Total | Χ2 | 0.961 | 1 | 0.327 |
| N | 65 | |||
| Contingency Tables. | |||
|---|---|---|---|
| Early Complications: | |||
| Etiopathogenesis | No | Yes | Total |
| primary | 49 | 5 | 54 |
| secondary | 9 | 4 | 13 |
| Total | 58 | 9 | 67 |
| Chi-Squared Tests | |||
| Value | df | p | |
| Χ2 | 4.169 | 1 | 0.041 |
| N | 67 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panico, F.; Bradaschia, L.; Cardellicchio, P.; Cofano, F.; Lo Bue, E.; Colonna, S.; Morello, A.; Bianconi, A.; Garbossa, D.; Piatelli, G.; et al. Exploring Aneurysmal Bone Cysts of the Skull: Insights from a Review of the Literature and a Case Report. Children 2025, 12, 715. https://doi.org/10.3390/children12060715
Panico F, Bradaschia L, Cardellicchio P, Cofano F, Lo Bue E, Colonna S, Morello A, Bianconi A, Garbossa D, Piatelli G, et al. Exploring Aneurysmal Bone Cysts of the Skull: Insights from a Review of the Literature and a Case Report. Children. 2025; 12(6):715. https://doi.org/10.3390/children12060715
Chicago/Turabian StylePanico, Flavio, Leonardo Bradaschia, Pasquale Cardellicchio, Fabio Cofano, Enrico Lo Bue, Stefano Colonna, Alberto Morello, Andrea Bianconi, Diego Garbossa, Gianluca Piatelli, and et al. 2025. "Exploring Aneurysmal Bone Cysts of the Skull: Insights from a Review of the Literature and a Case Report" Children 12, no. 6: 715. https://doi.org/10.3390/children12060715
APA StylePanico, F., Bradaschia, L., Cardellicchio, P., Cofano, F., Lo Bue, E., Colonna, S., Morello, A., Bianconi, A., Garbossa, D., Piatelli, G., & Pavanello, M. (2025). Exploring Aneurysmal Bone Cysts of the Skull: Insights from a Review of the Literature and a Case Report. Children, 12(6), 715. https://doi.org/10.3390/children12060715