
The Association Between Preoperative Malnutrition and Early Postoperative Outcomes in Children with Congenital Heart Disease: A 2-Year Retrospective Study at a Lebanese Tertiary Medical Center

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
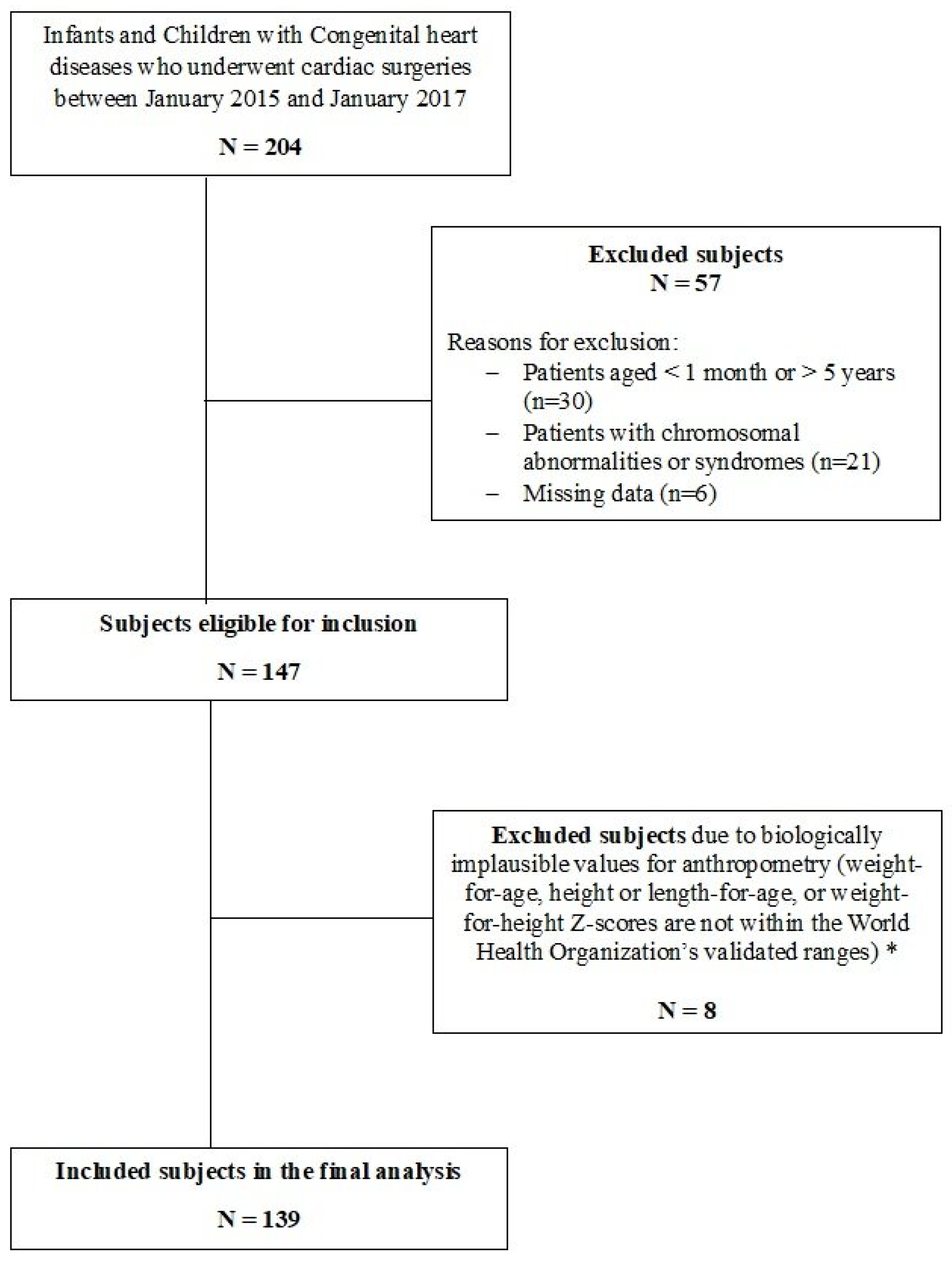
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Anthropometric Measurements
2.4. Definitions and Categorization
2.5. Statistical Analysis
3. Results
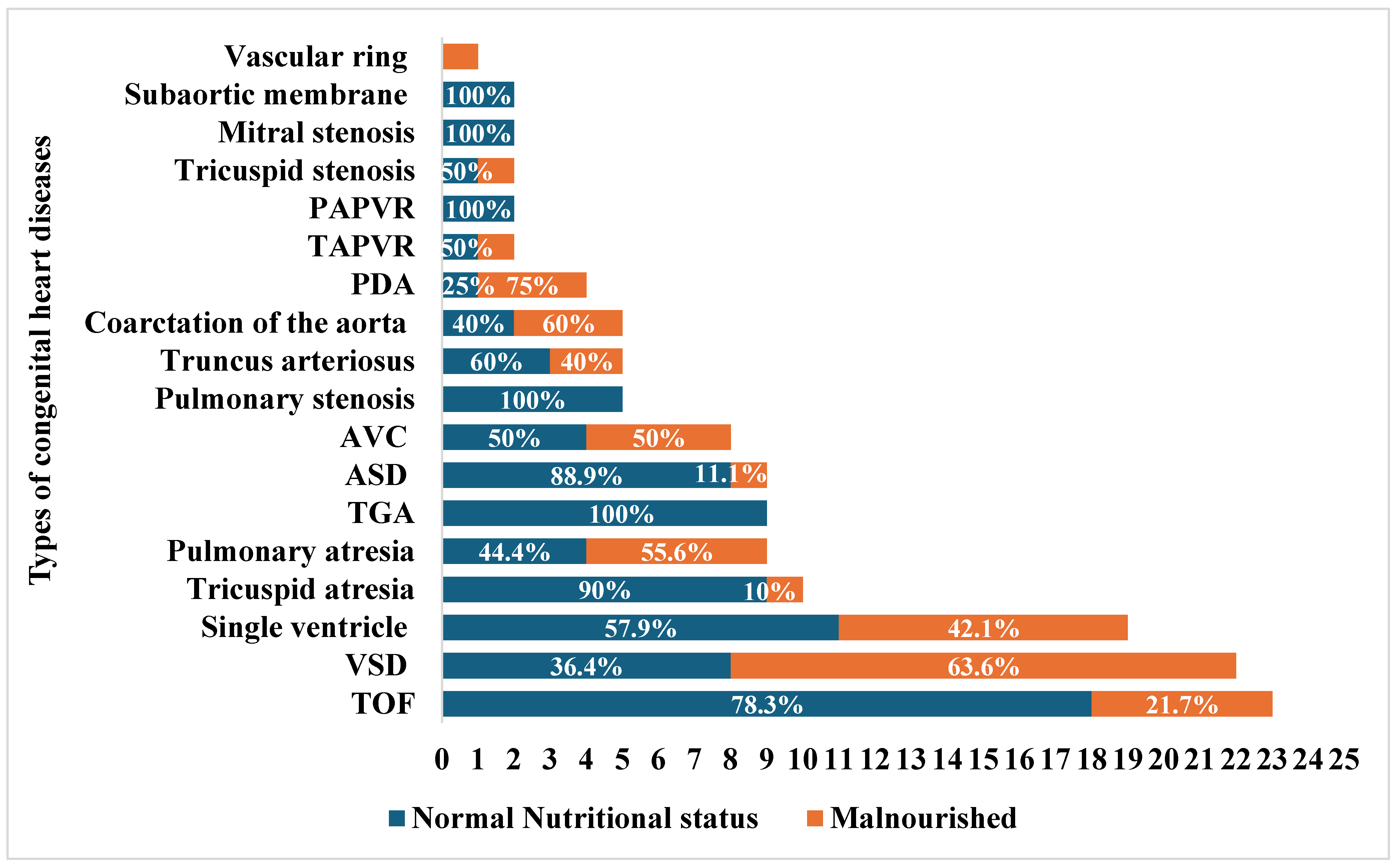
3.1. Demographic and Clinical Characteristics
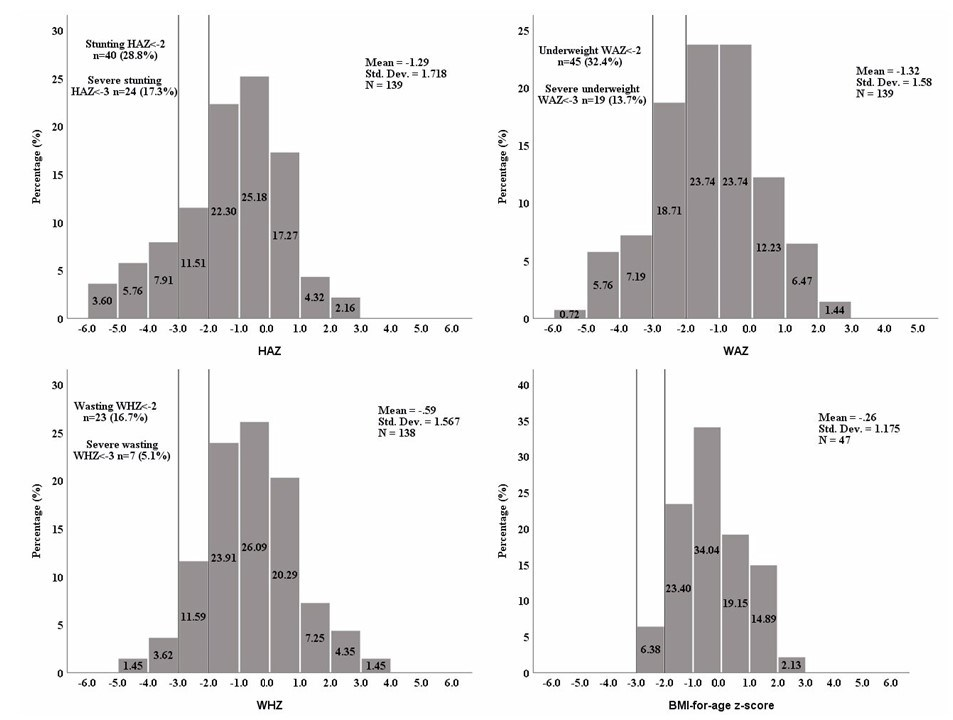
3.2. Anthropometric Measurements
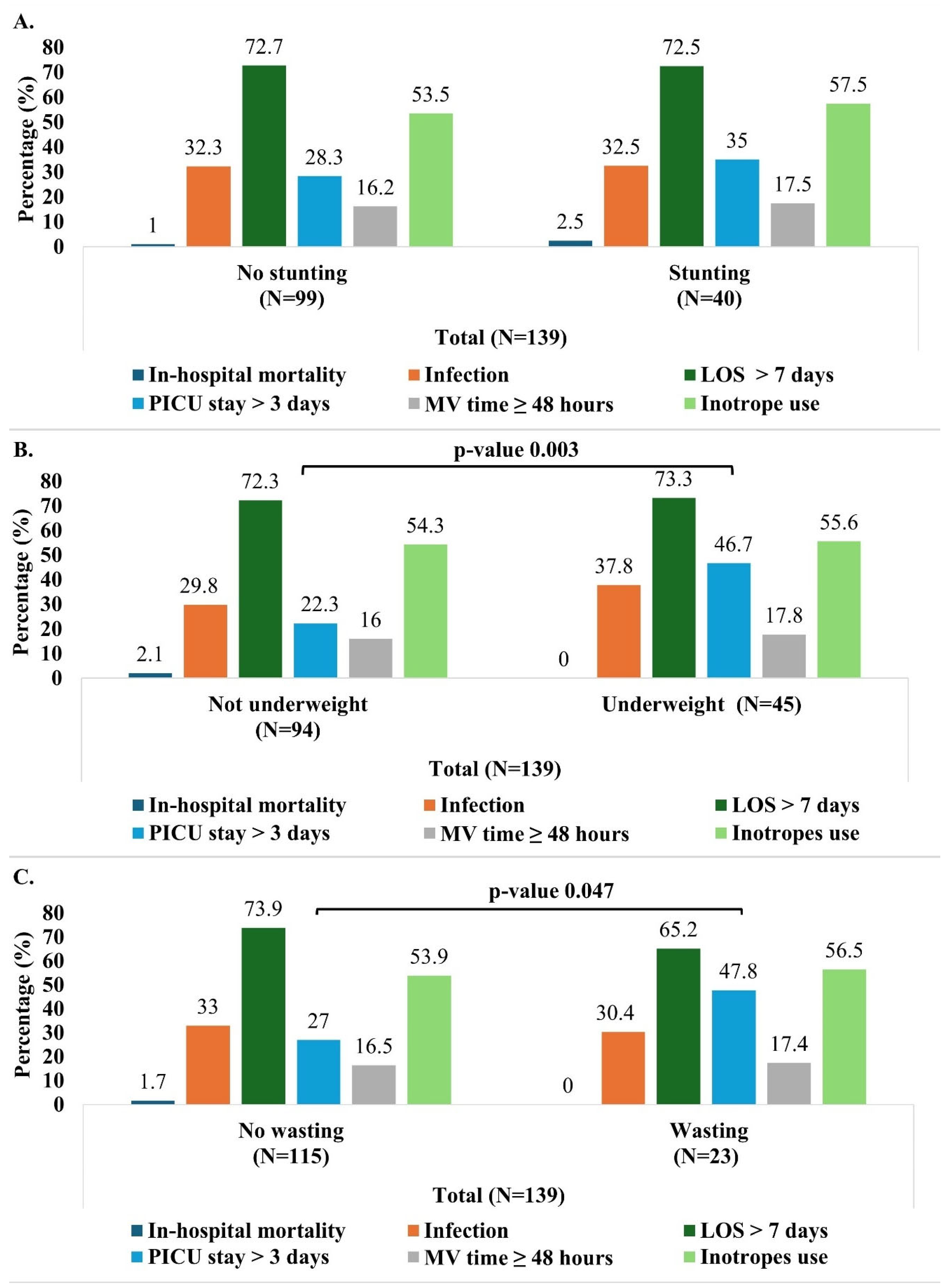
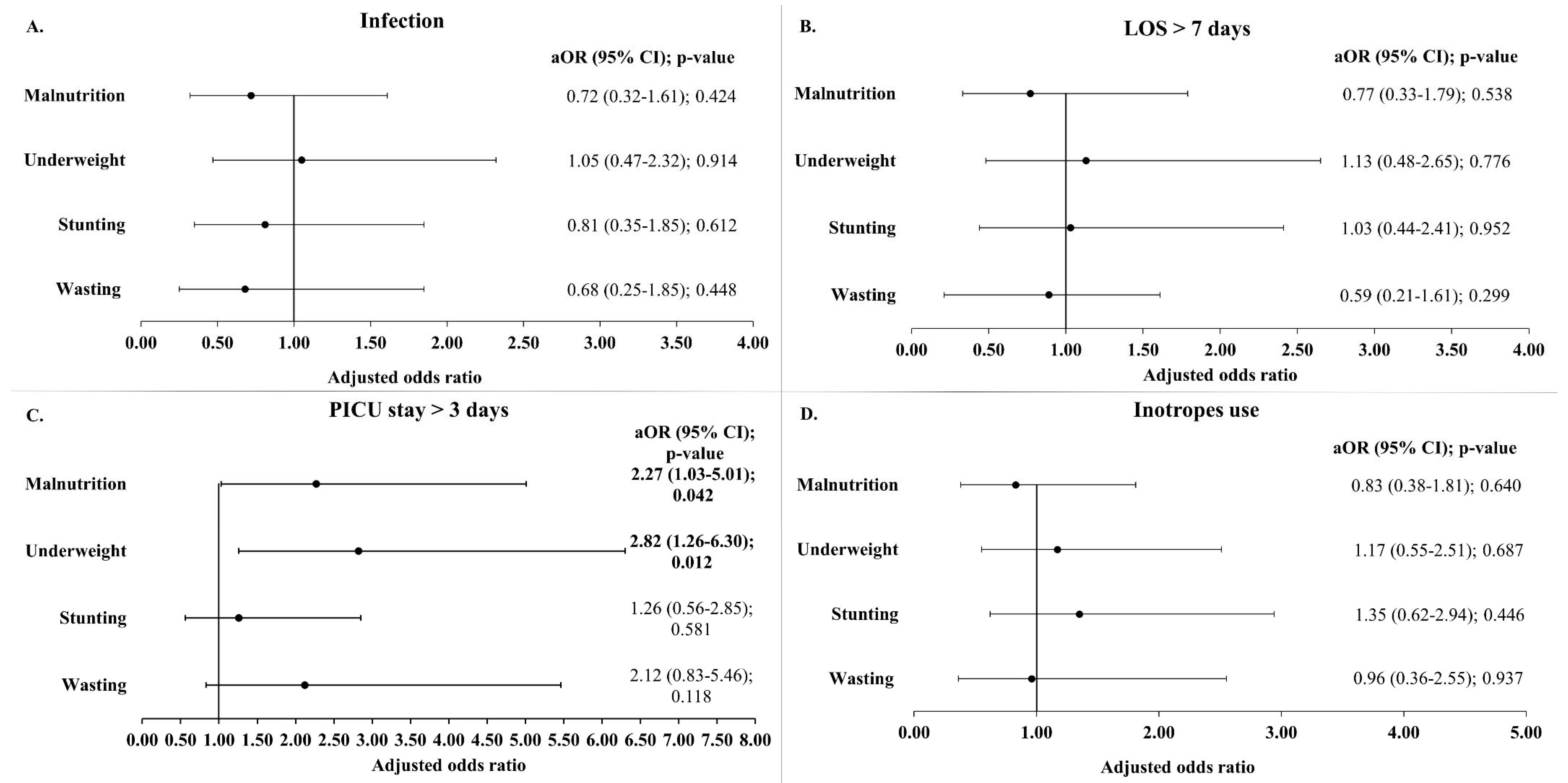
3.3. Association Between Malnutrition and Early Postoperative Outcomes
3.3.1. In-Hospital Mortality
3.3.2. Postoperative Infection
3.3.3. LOS and Duration of PICU Stay
3.3.4. Mechanical Ventilation Time and INOTROPES
3.4. Secondary Analysis: Malnutrition as a Continuous Variable and Its Impact on Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, W.; He, J.; Shao, X. Incidence and mortality trend of congenital heart disease at the global, regional, and national level, 1990–2017. Medicine 2020, 99, e20593. [Google Scholar] [CrossRef]
- Zimmerman, M.S.; Smith, A.G.C.; Sable, C.A.; Echko, M.M.; Wilner, L.B.; Olsen, H.E.; Atalay, H.T.; Awasthi, A.; Bhutta, Z.A.; Boucher, J.L.; et al. Global, regional, and national burden of congenital heart disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Child Adolesc. Health 2020, 4, 185–200. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Huang, R.; Kong, R.; Li, H.; Zhang, H.; Li, Y.; Liang, L.; Xiong, D.; Han, S.; Zhou, L.; et al. Prevalence and risk factors for congenital heart defects among children in the Multi-Ethnic Yunnan Region of China. Transl. Pediatr. 2022, 11, 813–824. [Google Scholar] [CrossRef]
- Knowles, R.L.; Ridout, D.; Crowe, S.; Bull, C.; Wray, J.; Tregay, J.; Franklin, R.C.; Barron, D.J.; Cunningham, D.; Parslow, R.C.; et al. Ethnic and socioeconomic variation in incidence of congenital heart defects. Arch. Dis. Child. 2017, 102, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Ha, K.S.; Park, C.M.; Lee, J.; Shin, J.; Choi, E.K.; Choi, M.; Kim, J.; Shin, H.J.; Choi, B.M.; Kim, S.-J. Nationwide Birth Prevalence of Crucial Congenital Heart Defects From 2014 to 2018 in Korea. Korean Circ. J. 2024, 54, 838–850. [Google Scholar] [CrossRef]
- Nikyar, B.; Sedehi, M.; Qorbani, M.; Nikyar, A.; Golalipour, M.J. Ethnical variations in the incidence of congenital heart defects in gorgan, northern iran: A single-center study. J. Tehran Heart Cent. 2014, 9, 9–14. [Google Scholar]
- Rossano, J.W. Congenital heart disease: A global public health concern. Lancet Child Adolesc. Health 2020, 4, 168–169. [Google Scholar] [CrossRef]
- Diao, J.; Chen, L.; Wei, J.; Shu, J.; Li, Y.; Li, J.; Zhang, S.; Wang, T.; Qin, J. Prevalence of Malnutrition in Children with Congenital Heart Disease: A Systematic Review and Meta-Analysis. J. Pediatr. 2022, 242, 39–47.e34. [Google Scholar] [CrossRef]
- Mehta, N.M.; Corkins, M.R.; Lyman, B.; Malone, A.; Goday, P.S.; Carney, L.; Monczka, J.L.; Plogsted, S.W.; Schwenk, W.F.; the American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). Board of Directors. Defining Pediatric Malnutrition. J. Parenter. Enter. Nutr. 2013, 37, 460–481. [Google Scholar] [CrossRef]
- WHO. Malnutrition. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 12 January 2025).
- Vaidyanathan, B.; Roth, S.J.; Rao, S.G.; Gauvreau, K.; Shivaprakasha, K.; Kumar, R.K. Outcome of ventricular septal defect repair in a developing country. J. Pediatr. 2002, 140, 736–741. [Google Scholar] [CrossRef]
- Schipper, M.; Slieker, M.G.; Schoof, P.H.; Breur, J.M.P.J. Surgical Repair of Ventricular Septal Defect; Contemporary Results and Risk Factors for a Complicated Course. Pediatr. Cardiol. 2017, 38, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.Y.J.; Wee, R.W.B.; Gandhi, M.; Lim, Y.P.; Tan, L.N.M.; Quek, S.C.; Aw, M.M.; Chen, C.K. The Associations Between Preoperative Anthropometry and Postoperative Outcomes in Infants Undergoing Congenital Heart Surgery. Front. Cardiovasc. Med. 2022, 9, 812680. [Google Scholar] [CrossRef] [PubMed]
- Ross, F.; Latham, G.; Joffe, D.; Richards, M.; Geiduschek, J.; Eisses, M.; Thompson, D.; Radman, M. Preoperative malnutrition is associated with increased mortality and adverse outcomes after paediatric cardiac surgery. Cardiol. Young 2017, 27, 1716–1725. [Google Scholar] [CrossRef]
- Wittenberg, R.E.; Gauvreau, K.; Duggan, C.P.; Du, X.; Giang, D.; Jayanthi, K.; Sandoval, N.; Sivalingam, S.; Zhao, X.; Jenkins, K.J. Preoperative Malnutrition Increases Risk of In-Hospital Mortality, Major Infection, and Longer Intensive Care Unit Stay After Ventricular Septal Defect Closure. J. Am. Heart Assoc. 2024, 13, e032662. [Google Scholar] [CrossRef]
- Costello, C.L.; Gellatly, M.; Daniel, J.; Justo, R.N.; Weir, K. Growth Restriction in Infants and Young Children with Congenital Heart Disease. Congenit. Heart Dis. 2015, 10, 447–456. [Google Scholar] [CrossRef]
- Marino, L.V.; Johnson, M.J.; Davies, N.J.; Kidd, C.S.; Fienberg, J.; Richens, T.; Bharucha, T.; Beattie, R.M.; Darlington, A.E. Improving growth of infants with congenital heart disease using a consensus-based nutritional pathway. Clin. Nutr. 2020, 39, 2455–2462. [Google Scholar] [CrossRef]
- WHO. Child Growth Standards. Available online: https://www.who.int/tools/child-growth-standards/standards (accessed on 20 February 2025).
- CDC. Use of World Health Organization and CDC Growth Charts for Children Aged 0–59 Months in the United States. 2010. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5909a1.htm (accessed on 20 February 2025).
- Chou, J.H.; Roumiantsev, S.; Singh, R. PediTools Electronic Growth Chart Calculators: Applications in Clinical Care, Research, and Quality Improvement. J. Med. Internet Res. 2020, 22, e16204. [Google Scholar] [CrossRef]
- Becker, P.; Carney, L.N.; Corkins, M.R.; Monczka, J.; Smith, E.; Smith, S.E.; Spear, B.A.; White, J.V. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: Indicators recommended for the identification and documentation of pediatric malnutrition (undernutrition). Nutr. Clin. Pract. 2015, 30, 147–161. [Google Scholar] [CrossRef]
- Jenkins, K.J.; Gauvreau, K.; Newburger, J.W.; Spray, T.L.; Moller, J.H.; Iezzoni, L.I. Consensus-based method for risk adjustment for surgery for congenital heart disease. J. Thorac. Cardiovasc. Surg. 2002, 123, 110–118. [Google Scholar] [CrossRef]
- Jenkins, K.J.; Koch Kupiec, J.; Owens, P.L.; Romano, P.S.; Geppert, J.J.; Gauvreau, K. Development and Validation of an Agency for Healthcare Research and Quality Indicator for Mortality After Congenital Heart Surgery Harmonized With Risk Adjustment for Congenital Heart Surgery (RACHS-1) Methodology. J. Am. Heart Assoc. 2016, 5, e003028. [Google Scholar] [CrossRef]
- WHO. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. 2006. Available online: https://www.who.int/publications/i/item/924154693X (accessed on 12 January 2025).
- Rukundo, K.; Benedict, S.M.L.N.; Croft, T. Evaluation of Implausible Anthropometric Values by Data Collection Team in Demographic and Health Surveys 2010–2020. 2022. Available online: https://dhsprogram.com/pubs/pdf/MR33/MR33.pdf (accessed on 4 March 2025).
- Herridge, J.; Tedesco-Bruce, A.; Gray, S.; Floh, A.A. Feeding the child with congenital heart disease: A narrative review. Pediatr. Med. 2021, 4, 7. [Google Scholar] [CrossRef]
- Rytter, M.J.; Kolte, L.; Briend, A.; Friis, H.; Christensen, V.B. The immune system in children with malnutrition—A systematic review. PLoS ONE 2014, 9, e105017. [Google Scholar] [CrossRef] [PubMed]
- Ross, F.J.; Radman, M.; Jacobs, M.L.; Sassano-Miguel, C.; Joffe, D.C.; Hill, K.D.; Chiswell, K.; Feng, L.; Jacobs, J.P.; Vener, D.F.; et al. Associations between anthropometric indices and outcomes of congenital heart operations in infants and young children: An analysis of data from the Society of Thoracic Surgeons Database. Am. Heart J. 2020, 224, 85–97. [Google Scholar] [CrossRef]
- Robyn, S.; Veronica, N.; Stephen, B.; Joanne, P. Undernutrition in young children with congenital heart disease undergoing cardiac surgery in a low-income environment. BMC Pediatr. 2024, 24, 73. [Google Scholar] [CrossRef]
- Woldesenbet, R.; Murugan, R.; Mulugeta, F.; Moges, T. Nutritional status and associated factors among children with congenital heart disease in selected governmental hospitals and cardiac center, Addis Ababa Ethiopia. BMC Pediatr. 2021, 21, 538. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, L.; Huang, R.; Sun, C.; Bao, N.; Xu, Z. Risk factors of malnutrition in Chinese children with congenital heart defect. BMC Pediatr. 2020, 20, 213. [Google Scholar] [CrossRef]
- Hubschman, L.E. Malnutrition in Congenital Heart Disease: Management to Improve Outcomes. ICAN Infant Child Adolesc. Nutr. 2013, 5, 170–176. [Google Scholar] [CrossRef]
- Palleri, D.; Bartolacelli, Y.; Balducci, A.; Bonetti, S.; Zanoni, R.; Ciuca, C.; Gesuete, V.; Bulgarelli, A.; Hasan, T.; Ragni, L.; et al. Moderate and Severe Congenital Heart Diseases Adversely Affect the Growth of Children in Italy: A Retrospective Monocentric Study. Nutrients 2023, 15, 484. [Google Scholar] [CrossRef]
- Chan, B.; Woodbury, A.; Hazelwood, L.; Singh, Y. Feeding Approach to Optimizing Nutrition in Infants with Congenital Heart Disease. J. Cardiovasc. Dev. Dis. 2025, 12, 38. [Google Scholar] [CrossRef]
- Mignot, M.; Huguet, H.; Cambonie, G.; Guillaumont, S.; Vincenti, M.; Blanc, J.; Ovaert, C.; Picot, M.-C.; Karsenty, C.; Amedro, P.; et al. Risk factors for early occurrence of malnutrition in infants with severe congenital heart disease. Eur. J. Pediatr. 2023, 182, 1261–1269. [Google Scholar] [CrossRef]
- Anderson, J.B.; Kalkwarf, H.J.; Kehl, J.E.; Eghtesady, P.; Marino, B.S. Low Weight-for-Age Z-Score and Infection Risk After the Fontan Procedure. Ann. Thorac. Surg. 2011, 91, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.B.; Shi, B.X.; Zhou, S.H.; Li, S.L.; Lin, Y.J. Preoperative Nutritional Status of Infants with Non-Restricted Ventricular Septal Defect and Its Influence on Postoperative Recovery. Heart Surg. Forum 2023, 26, E560–E565. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz Ferhatoglu, S.; Yurdakok, O.; Yurtseven, N. Malnutrition on admission to the paediatric cardiac intensive care unit increases the risk of mortality and adverse outcomes following paediatric congenital heart surgery: A prospective cohort study. Aust. Crit. Care 2022, 35, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.C.; Jaggers, J.; Li, J.S.; Jacobs, M.L.; Jacobs, J.P.; Benjamin, D.K.; O’Brien, S.M.; Peterson, E.D.; Smith, P.B.; Pasquali, S.K. Center variation in patient age and weight at Fontan operation and impact on postoperative outcomes. Ann. Thorac. Surg. 2011, 91, 1445–1452. [Google Scholar] [CrossRef]
- WHO. Malnutrition in Children. Available online: https://www.who.int/data/nutrition/nlis/info/malnutrition-in-children (accessed on 20 February 2025).
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- WHO. Malnutrition in Women. Available online: https://www.who.int/data/nutrition/nlis/info/malnutrition-in-women (accessed on 3 March 2025).
- Thourani, V.H.; Keeling, W.B.; Kilgo, P.D.; Puskas, J.D.; Lattouf, O.M.; Chen, E.P.; Guyton, R.A. The impact of body mass index on morbidity and short- and long-term mortality in cardiac valvular surgery. J. Thorac. Cardiovasc. Surg. 2011, 142, 1052–1061. [Google Scholar] [CrossRef]
- Engelman, D.T.; Adams, D.H.; Byrne, J.G.; Aranki, S.F.; Collins, J.J., Jr.; Couper, G.S.; Allred, E.N.; Cohn, L.H.; Rizzo, R.J. Impact of body mass index and albumin on morbidity and mortality after cardiac surgery. J. Thorac. Cardiovasc. Surg. 1999, 118, 866–873. [Google Scholar] [CrossRef]
- Ri, M.; Miyata, H.; Aikou, S.; Seto, Y.; Akazawa, K.; Takeuchi, M.; Matsui, Y.; Konno, H.; Gotoh, M.; Mori, M.; et al. Effects of body mass index (BMI) on surgical outcomes: A nationwide survey using a Japanese web-based database. Surg. Today 2015, 45, 1271–1279. [Google Scholar] [CrossRef]
- Bechard, L.J.; Duggan, C.; Touger-Decker, R.; Parrott, J.S.; Rothpletz-Puglia, P.; Byham-Gray, L.; Heyland, D.; Mehta, N.M. Nutritional Status Based on Body Mass Index Is Associated With Morbidity and Mortality in Mechanically Ventilated Critically Ill Children in the PICU. Crit. Care Med. 2016, 44, 1530–1537. [Google Scholar] [CrossRef]
- Marino, L.V.; Harris, A.; Johnstone, C.; Friend, A.; Newell, C.; Miles, E.A.; Lucas, J.S.; Calder, P.C.; Walker, W.T. Characterising the nutritional status of children with primary ciliary dyskinesia. Clin. Nutr. 2019, 38, 2127–2135. [Google Scholar] [CrossRef]
- Leite, H.P.; Fisberg, M.; de Carvalho, W.B.; de Camargo Carvalho, A.C. Serum albumin and clinical outcome in pediatric cardiac surgery. Nutrition 2005, 21, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Radman, M.; Mack, R.; Barnoya, J.; Castañeda, A.; Rosales, M.; Azakie, A.; Mehta, N.; Keller, R.; Datar, S.; Oishi, P.; et al. The effect of preoperative nutritional status on postoperative outcomes in children undergoing surgery for congenital heart defects in San Francisco (UCSF) and Guatemala City (UNICAR). J. Thorac. Cardiovasc. Surg. 2014, 147, 442–450. [Google Scholar] [CrossRef]
- Keller, U. Nutritional Laboratory Markers in Malnutrition. J. Clin. Med. 2019, 8, 775. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, Y.; Ukil Isildak, F. Preoperative nutritional status effects postoperative outcome in patients undergoing surgery for congenital heart disease. Nutr. Clin. Et Métabolisme 2021, 35, 253–259. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal Nutritional Status, n (%) n = 92 | Malnourished, n (%) n = 47 | p-Value | |
|---|---|---|---|
| Age groups | 0.001 | ||
| <24 months | 52 (56.5) | 40 (85.1) | |
| ≥24 months | 40 (43.5) | 7 (14.9) | |
| Gender | 0.326 | ||
| Male | 55 (59.8) | 24 (51.1) | |
| Female | 37 (40.2) | 23 (48.9) | |
| Type of CHD | 0.218 | ||
| Acyanotic | 35 (38.0) | 23 (48.9) | |
| Cyanotic | 57 (62.0) | 24 (51.1) | |
| RACHS-1 categories | 0.536 | ||
| 1 to 3 | 81 (88.0) | 43 (91.5) | |
| 4 to 6 | 11 (12.0) | 4 (8.5) | |
| Pulmonary hypertension | 13 (14.1) | 11 (23.4) | 0.171 |
| Overall (n = 139) | |||
|---|---|---|---|
| Normal Nutritional Status (n = 92), n (%) | Malnourished (n = 47), n (%) | p-Value | |
| In-hospital mortality | 2 (2.2) | 0 (0.0) | 0.549 * |
| Infection | 29 (31.5) | 16 (32.7) | 0.764 |
| Length of hospital stay, median (IQR) | 9.0 (7.0-14.0) | 8.0 (7.0-15.0) | 0.725 |
| Length of hospital stay | 0.643 | ||
| ≤7 days | 24 (26.1) | 14 (29.8)) | |
| >7 days | 68 (73.9) | 33 (70.2) | |
| Length of PICU stay, median (IQR) | 2.0 (2.0-3.0) | 3.0 (2.0-7.0) | 0.004 |
| Duration of PICU stay | 0.008 | ||
| ≤3 days | 71 (77.2) | 28 (55.3) | |
| >3 days | 21 (22.8) | 21 (44.7) | |
| Inotropes use | 51 (55.4) | 25 (53.2) | 0.802 |
| Mechanical ventilation time | |||
| <48 h | 79 (85.9) | 37 (78.7) | 0.672 |
| ≥48 h | 13 (14.1) | 10 (21.3) | |
| Mechanical ventilation time, median (IQR) | 5.0 (3.0-16.5) | 9.0 (4.0-44.0) | 0.017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assy, J.; Yaacoub, C.; Khafaja, S.; Arabi, M.T.; El Rassi, I.; Bitar, F.; Yazbeck, N. The Association Between Preoperative Malnutrition and Early Postoperative Outcomes in Children with Congenital Heart Disease: A 2-Year Retrospective Study at a Lebanese Tertiary Medical Center. Children 2025, 12, 705. https://doi.org/10.3390/children12060705
Assy J, Yaacoub C, Khafaja S, Arabi MT, El Rassi I, Bitar F, Yazbeck N. The Association Between Preoperative Malnutrition and Early Postoperative Outcomes in Children with Congenital Heart Disease: A 2-Year Retrospective Study at a Lebanese Tertiary Medical Center. Children. 2025; 12(6):705. https://doi.org/10.3390/children12060705
Chicago/Turabian StyleAssy, Jana, Christelle Yaacoub, Sarah Khafaja, Mariam Toufic Arabi, Issam El Rassi, Fadi Bitar, and Nadine Yazbeck. 2025. "The Association Between Preoperative Malnutrition and Early Postoperative Outcomes in Children with Congenital Heart Disease: A 2-Year Retrospective Study at a Lebanese Tertiary Medical Center" Children 12, no. 6: 705. https://doi.org/10.3390/children12060705
APA StyleAssy, J., Yaacoub, C., Khafaja, S., Arabi, M. T., El Rassi, I., Bitar, F., & Yazbeck, N. (2025). The Association Between Preoperative Malnutrition and Early Postoperative Outcomes in Children with Congenital Heart Disease: A 2-Year Retrospective Study at a Lebanese Tertiary Medical Center. Children, 12(6), 705. https://doi.org/10.3390/children12060705