
Case Study of a Broken Instrument in a Primary Tooth and Literature Review

Abstract
1. Introduction
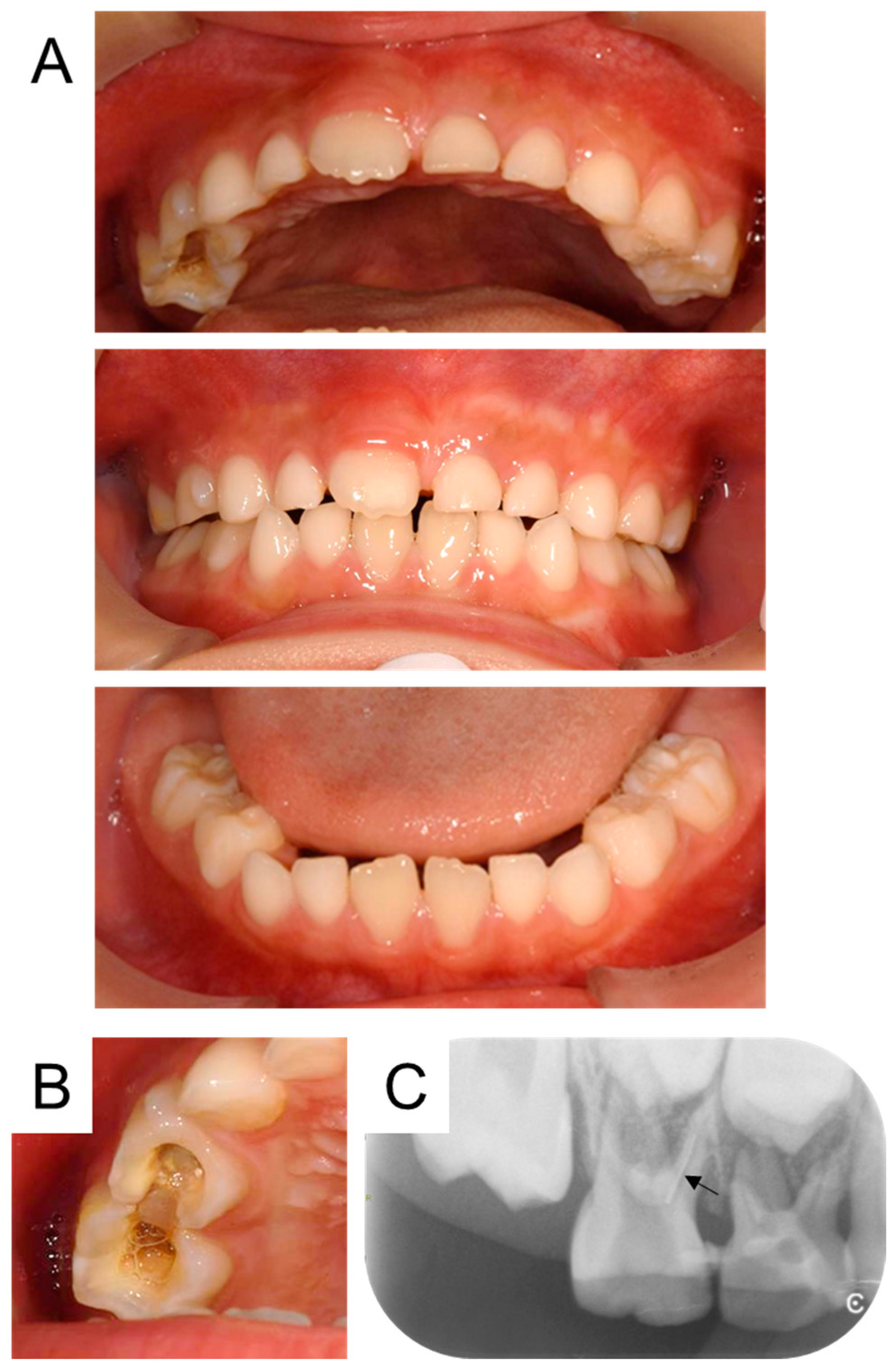
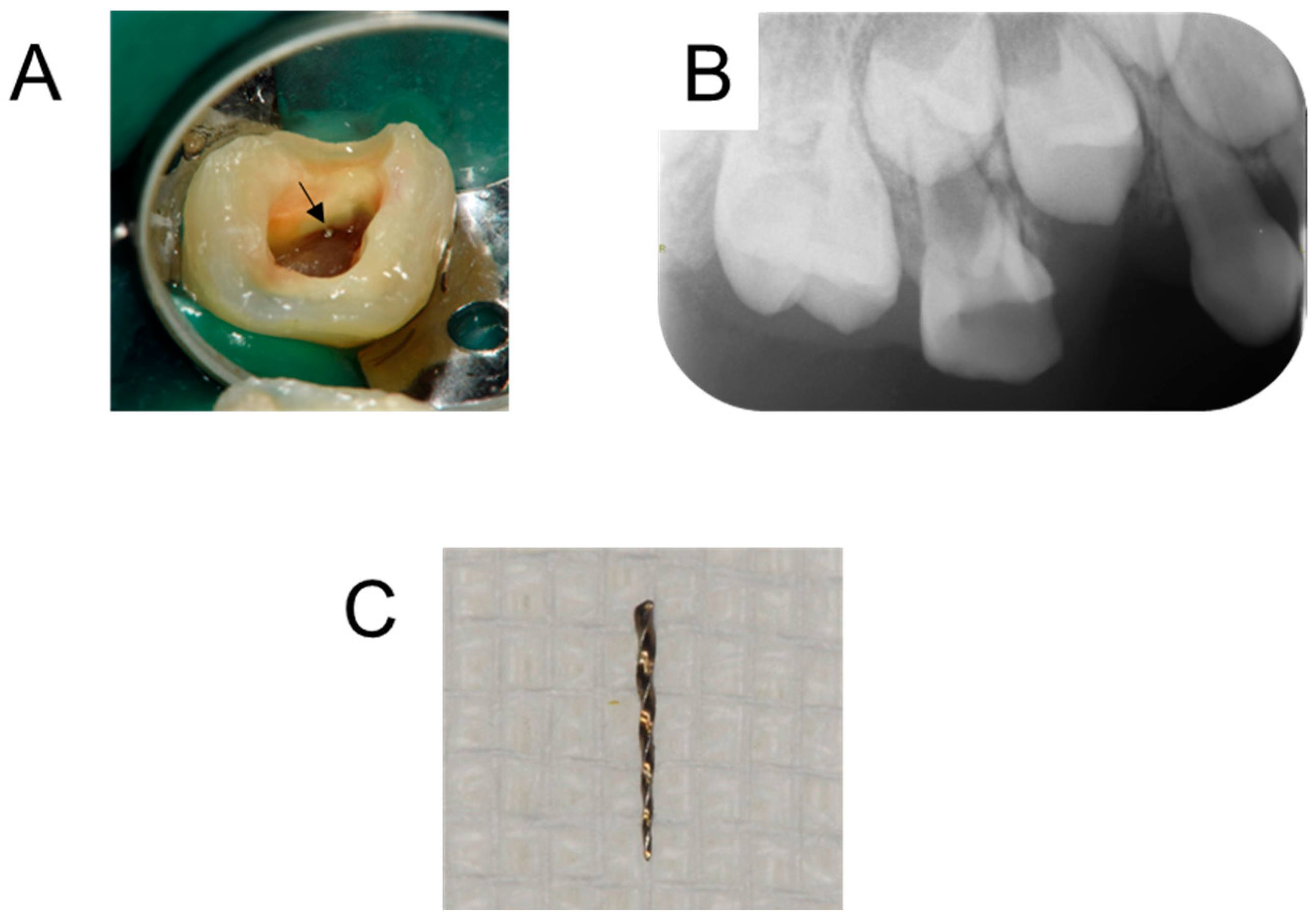
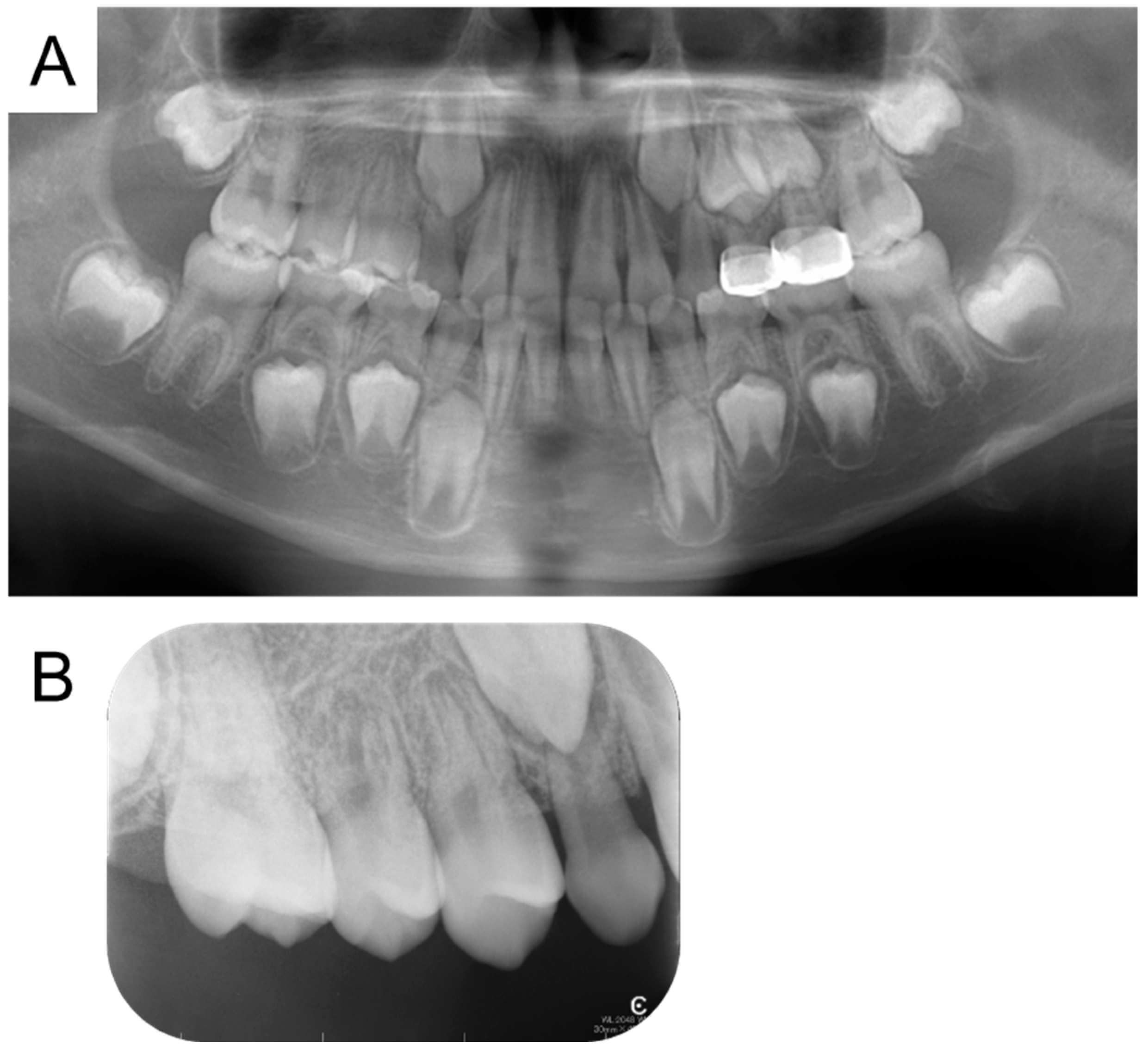
2. Detailed Case Description
3. Methods
3.1. Search Strategy
3.2. Inclusion Criteria
- -
- Articles that could be viewed in their entirety.
- -
- Articles with their full text in English.
- -
- Case reports about broken instruments in primary teeth.
3.3. Exclusion Criteria
- -
- Articles that were not suitable for the objective of this review.
- -
- Articles that used the wrong study design.
- -
- Not being a case report, such as review.
3.4. Study Selection
3.5. Data Extraction
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frencken, J.E.; Sharma, P.; Stenhouse, L.; Green, D.; Laverty, D.; Dietrich, T. Global epidemiology of dental caries and severe periodontitis—A comprehensive review. J. Clin. Periodontol. 2017, 44 (Suppl. 18), S94–S105. [Google Scholar] [CrossRef] [PubMed]
- Usuda, M.; Kametani, M.; Hamada, M.; Suehiro, Y.; Matayoshi, S.; Okawa, R.; Naka, S.; Matsumoto-Nakano, M.; Akitomo, T.; Mitsuhata, C.; et al. Inhibitory Effect of Adsorption of Streptococcus mutans onto Scallop-Derived Hydroxyapatite. Int. J. Mol. Sci. 2023, 24, 11371. [Google Scholar] [CrossRef]
- Yasuda, J.; Yasuda, H.; Nomura, R.; Matayoshi, S.; Inaba, H.; Gongora, E.; Iwashita, N.; Shirahata, S.; Kaji, N.; Akitomo, T.; et al. Investigation of periodontal disease development and Porphyromonas gulae FimA genotype distribution in small dogs. Sci. Rep. 2024, 14, 5360. [Google Scholar] [CrossRef] [PubMed]
- Tinanoff, N. Dental caries risk assessment and prevention. Dent. Clin. N. Am. 1995, 39, 709–719. [Google Scholar] [CrossRef] [PubMed]
- Pessan, J.P.; Al-Ibrahim, N.S.; Buzalaf, M.A.; Toumba, K.J. Slow-release fluoride devices: A literature review. J. Appl. Oral Sci. 2008, 16, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Bashir, N.Z. Trends in the prevalence of dental caries in the US pediatric population 2011–2020. J. Clin. Pediatr. Dent. 2022, 46, 51–57. [Google Scholar] [PubMed]
- Yawaka, Y.; Iwabuchi, H.; Ito, S.; Kaga, M. A Seven-year Survey at the Pediatric Dentistry Clinic of a University Hospital of Patients with Systemic Diseases. Jpn. J. Ped. Dent. 2007, 45, 623–631. (In Japanese) [Google Scholar]
- Tominaga, S.; Tanaka, A.; Nemoto, K.; Hamaguchi, S.; Tamura, R.; Tanase, T.; Sakurai, A.; Tsujino, K.; Shintani, S. A Survey of the Actual Condition of New Patients at the Pediatric Dentistry Department of College Hospitals and Dental Caries Status in Deciduous Dentition: A Comparison Study between Tokyo and Chiba. Jpn. J. Ped. Dent. 2020, 58, 49–54. (In Japanese) [Google Scholar]
- Ng, L.; Malandris, M.; Cheung, W.; Rossi-Fedele, G. Traumatic dental injuries presenting to a paediatric emergency department in a tertiary children’s hospital, Adelaide, Australia. Dent. Traumatol. 2020, 36, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Akitomo, T.; Asao, Y.; Mitsuhata, C.; Kozai, K. A new supernumerary tooth occurring in the same region during follow-up after supernumerary tooth extraction: A case report. Pediatr. Dent. J. 2021, 31, 100–107. [Google Scholar] [CrossRef]
- Akitomo, T.; Kusaka, S.; Iwamoto, Y.; Usuda, M.; Kametani, M.; Asao, Y.; Nakano, M.; Tachikake, M.; Mitsuhata, C.; Nomura, R. Five-Year Follow-Up of a Child with Non-Syndromic Oligodontia from before the Primary Dentition Stage: A Case Report. Children 2023, 10, 717. [Google Scholar] [CrossRef]
- Akitomo, T.; Ogawa, M.; Kaneki, A.; Nishimura, T.; Usuda, M.; Kametani, M.; Kusaka, S.; Asao, Y.; Iwamoto, Y.; Tachikake, M.; et al. Dental Abnormalities in Pediatric Patients Receiving Chemotherapy. J. Clin. Med. 2024, 13, 2877. [Google Scholar] [CrossRef] [PubMed]
- Matumoto, H.; Kakuta, H.; Natsubori, H.; Harada, R.; Tanaka, M. A Survey on the Present Situation of the First Visit Patients in a University Pediatric Dental Clinic. Jpn. J. Ped. Dent. 2007, 45, 405–411. (In Japanese) [Google Scholar]
- Kaneko, K.; Tsubokura, A.; Tsujino, K.; Mochizuki, K.; Ohtawa, Y.; Yakushiji, M. An Investigation of the Actual Conditions During the Initial Visit of Patients Under 3 years of Age at the Pedodontics of Dental College Hospital. Jpn. J. Ped. Dent. 2008, 46, 342–346. (In Japanese) [Google Scholar]
- Barrieshi-Nusair, K.; Al-Omari, M.; Al-Hiyasat, A. Radiographic technical quality of root canal treatment performed by dental students at the Dental Teaching Center in Jordan. J. Dent. 2004, 1132, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Er, O.; Sagsen, B.; Maden, M.; Cinar, S.; Kahraman, Y. Radiographic technical quality of root fillings performed by dental students in Turkey. Int. Endod. J. 2006, 39, 867–872. [Google Scholar] [CrossRef] [PubMed]
- AlRahabi, M.K. Evaluation of complications of root canal treatment performed by undergraduate dental students. Libyan J. Med. 2017, 12, 1345582. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.; Mor, C. The success of endodontic therapy—Healing and functionality. J. Calif. Dent. Assoc. 2004, 32, 493–503. [Google Scholar] [CrossRef]
- Imura, N.; Pinheiro, E.T.; Gomes, B.P.; Zaia, A.A.; Ferraz, C.C.; Souza-Filho, F.J. The outcome of endodontic treatment: A retrospective study of 2000 cases performed by a specialist. J. Endod. 2007, 33, 1278–1282. [Google Scholar] [CrossRef]
- Godiny, M.; Hatam, R.; Khavid, A.; Khanlari, S. Apical Microleakage in Root Canals Containing Broken Rotary Instruments. Iran. Endod. J. 2017, 12, 360–365. [Google Scholar] [PubMed]
- Shen, Y.; Zhou, H.-M.; Zheng, Y.-F.; Peng, B.; Haapasalo, M. Current Challenges and Concepts of the Thermomechanical Treatment of Nickel-Titanium Instruments. J. Endod. 2013, 39, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Faramarzi, F.; Fakhri, H.; Javaheri, H.H. Endodontic treatment of a mandibular first molar with three mesial canals and broken instrument removal. Aust. Endod. J. 2010, 36, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Shibata, A.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Sakaida, K.; Furuki, Y. Use of an intraoperative navigation system for retrieving a broken dental instrument in the mandible: A case report. J. Med. Case Rep. 2017, 11, 14. [Google Scholar] [CrossRef]
- Meidyawati, R.; Suprastiwi, E.; Setiati, H.D. Broken File Retrieval in the Lower Right First Molar Using an Ultrasonic Instrument and Endodontic Micro Forceps. Case Rep. Dent. 2019, 2019, 7940126. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Akitomo, T.; Kusaka, S.; Usuda, M.; Kametani, M.; Kaneki, A.; Nishimura, T.; Ogawa, M.; Mitsuhata, C.; Nomura, R. Fusion of a Tooth with a Supernumerary Tooth: A Case Report and Literature Review of 35 Cases. Children 2024, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Pk, M.; Sc, K.; As, S. Broken instrument retrieval with indirect ultrasonics in a primary molar. Eur. Arch. Paediatr. Dent. 2015, 17, 71–74. [Google Scholar] [CrossRef]
- Kaul, R.; Gupta, R.; Chhabra, S.; Koul, R. Dental Operating Microscope-guided Retrieval of Broken Instrument from a Deciduous Molar Using Ultrasonics. Int. J. Clin. Pediatr. Dent. 2022, 15 (Suppl. 1), S114–S118. [Google Scholar]
- Iqbal, M.K.; Kohli, M.R.; Kim, J.S. A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: A PennEndo database study. J. Endod. 2006, 32, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- Cheung, G.S.; Bian, Z.; Shen, Y.; Peng, B.; Darvell, B.W. Comparison of defects in ProTaper hand-operated and engine-driven instruments after clinical use. Int. Endod. J. 2007, 40, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Tzanetakis, G.N.; Kontakiotis, E.G.; Maurikou, D.V.; Marzelou, M.P. Prevalence and management of instrument fracture in the postgraduate endodontic program at the Dental School of Athens: A five-year retrospective clinical study. J. Endod. 2008, 34, 675–678. [Google Scholar] [CrossRef] [PubMed]
- Abu-Tahun, I.; Al-Rabab’ah, M.A.; Hammad, M.; Khraisat, A. Technical quality of root canal treatment of posterior teeth after rotary or hand preparation by fifth year undergraduate students, The University of Jordan. Aust. Endod. J. 2014, 40, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, A.; Gökyay, S.S.; Dağlaroğlu, R.; Küçükay, I.K. Evaluation of deformation and fracture rates for nickel-titanium rotary instruments according to the frequency of clinical use. Eur. Oral Res. 2018, 52, 89–93. [Google Scholar] [PubMed]
- Eskibağlar, M.; Özata, M.Y.; Ocak, M.S.; Öztekin, F. Investigation of fracture prevalence of instruments used in root canal treatments at a faculty of dentistry: A prospective study. Restor. Dent. Endod. 2023, 48, e38. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, A.; Neuman, H. Iatrogenic damages caused by dental procedures. Foreign bodies in the oral cavity. Quintessence Int. 1983, 14, 361–366. [Google Scholar] [PubMed]
- Lin, L.M.; Rosenberg, P.A.; Lin, J. Do procedural errors cause endodontic treatment failure. J. Am. Dent. Assoc. 2005, 136, 187–193. [Google Scholar] [CrossRef]
- Madarati, A.A.; Watts, D.C.; Qualtrough, A.J. Factors contributing to the separation of endodontic files. Br. Dent. J. 2008, 204, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Heydari, A.; Rahmani, M.; Heydari, M. Removal of a Broken Instrument from a Tooth with Apical Periodontitis Using a Novel Approach. Iran. Endod. J. 2016, 11, 237–240. [Google Scholar] [PubMed]
- Hosey, M. Managing anxious children: The use of conscious sedation in paediatric dentistry. Int. J. Paediatr. Dent. 2002, 12, 359–372. [Google Scholar] [CrossRef] [PubMed]
- Shetty, V.; Suresh, L.R.; Hegde, A.M. Effect of Virtual Reality Distraction on Pain and Anxiety During Dental Treatment in 5 to 8 Year Old Children. J. Clin. Pediatr. Dent. 2019, 43, 97–102. [Google Scholar] [CrossRef]
- Lin, C.S.; Lee, C.Y.; Chen, L.L.; Wu, L.T.; Yang, S.F.; Wang, T.F. Magnification of fear and intention of avoidance in non-experienced versus experienced dental treatment in adults. BMC Oral Health 2021, 21, 328. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, B.; Erwood, K.; Ncomanzi, S.; Fischer, V.; O’Brien, D.; Lee, A. Management strategies for adult patients with dental anxiety in the dental clinic: A systematic review. Aust. Dent. J. 2022, 67 (Suppl. 1), S3–S13. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhu, L.; Mei, Y.; Cao, L.; Ma, H. Investigation of children’s dental fear. BJ Stomatol. 2007, 25, 225–227. [Google Scholar]
- Karst, M.; Winterhalter, M.; Münte, S.; Francki, B.; Hondronikos, A.; Eckardt, A.; Hoy, L.; Buhck, H.; Bernateck, M.; Fink, M. Auricular acupuncture for dental anxiety: A randomized controlled trial. Anesth. Analg. 2007, 104, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.H.; Song, Y.R. Usage of a Reward System for Dealing with Pediatric Dental Fear. Chin. Med. J. 2016, 129, 1935–1938. [Google Scholar] [CrossRef] [PubMed]
- Bangash, M.; Mustafa, L.; Irshad, M.; Omer, Q.; Alam, M.K. Short Term Effects of Inhalation Sedation on Child Dental Fear and Anxiety. Curr. Pediatr. Rev. 2024, 20, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Terauchi, Y.; Ali, W.T.; Abielhassan, M.M. Present status and future directions: Removal of fractured instruments. Int. Endod. J. 2022, 55 (Suppl. 3), 685–709. [Google Scholar] [CrossRef] [PubMed]
- Pedir, S.S.; Mahran, A.H.; Beshr, K.; Baroudi, K. Evaluation of the Factors and Treatment Options of Separated Endodontic Files Among Dentists and Undergraduate Students in Riyadh Area. J. Clin. Diagn. Res. 2016, 10, ZC18–ZC23. [Google Scholar] [CrossRef] [PubMed]
- Cunha, R.S.; Junaid, A.; Ensinas, P.; Nudera, W.; da Silveira Bueno, C.E. Assessment of the separation incidence of reciprocating WaveOne files: A prospective clinical study. J. Endod. 2014, 40, 922–924. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.Y.; Kim, H.C.; Kim, E. Kinematic effects of nickel-titanium instruments with reciprocating or continuous rotation motion: A systematic review of in vitro studies. J. Endod. 2016, 42, 1009–1017. [Google Scholar] [CrossRef]
- Bueno, C.S.P.; de Oliveira, D.P.; Pelegrine, R.A.; Fontana, C.E.; Rocha, D.G.P.; da Silveira Bueno, C.E. Fracture incidence of WaveOne and Reciproc Files during root canal preparation of up to 3 posterior teeth: A prospective clinical study. J. Endod. 2017, 43, 705–708. [Google Scholar] [CrossRef]
- Pedersen, J.; Stensgaard, K.; Melsen, B. Prevalence of malocclusion in relation to premature loss of primary teeth. Community Dent. Oral Epidemiol. 1978, 6, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Ahamed, S.S.; Reddy, V.N.; Krishnakumar, R.; Mohan, M.G.; Sugumaran, D.K.; Rao, A.P. Prevalence of early loss of primary teeth in 5-10-year-old school children in Chidambaram town. Contemp. Clin. Dent. 2012, 3, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Law, C.S. Management of premature primary tooth loss in the child patient. J. Calif. Dent. Assoc. 2013, 41, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Monte-Santo, A.S.; Viana, S.V.C.; Moreira, K.M.S.; Imparato, J.C.P.; Mendes, F.M.; Bonini, G.A.V.C. Prevalence of early loss of primary molar and its impact in schoolchildren’s quality of life. Int. J. Paediatr. Dent. 2018, 28, 595–601. [Google Scholar] [CrossRef]
- Ward, J.R.; Parashos, P.; Messer, H.H. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: Clinical cases. J. Endod. 2003, 29, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Suter, B.; Lussi, A.; Sequeira, P. Probability of removing fractured instruments from root canals. Int. Endod. J. 2005, 38, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Gencoglu, N.; Helvacioglu, D. Comparison of the different techniques to remove fractured endodontic instruments from root canal systems. Eur. J. Dent. 2009, 3, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Terauchi, Y.; Sexton, C.; Bakland, L.K.; Bogen, G. Factors Affecting the Removal Time of Separated Instruments. J. Endod. 2021, 47, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, S.P.; Cesario, F.E. Association Between Molar-Incisor Hypomineralization and Enamel Hypoplasia. J. Clin. Pediatr. Dent. 2022, 46, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Akitomo, T.; Asao, Y.; Iwamoto, Y.; Kusaka, S.; Usuda, M.; Kametani, M.; Ando, T.; Sakamoto, S.; Mitsuhata, C.; Kajiya, M.; et al. A Third Supernumerary Tooth Occurring in the Same Region: A Case Report. Dent. J. 2023, 11, 49. [Google Scholar] [CrossRef]
- Akitomo, T.; Tsuge, Y.; Mitsuhata, C.; Nomura, R. A Narrative Review of the Association between Dental Abnormalities and Chemotherapy. J. Clin. Med. 2024, 13, 4942. [Google Scholar] [CrossRef] [PubMed]
- Kebede, B.; Tare, D.; Bogale, B.; Alemseged, F. Odontogenic tumors in Ethiopia: Eight years retrospective study. BMC Oral Health 2017, 17, 54. [Google Scholar] [CrossRef]
- Usuda, M.; Akitomo, T.; Kametani, M.; Kusaka, S.; Mitsuhata, C.; Nomura, R. Dens invaginatus of fourteen teeth in a pediatric patient. Pediatr. Dent. J. 2023, 33, 240–245. [Google Scholar] [CrossRef]
- Kametani, M.; Akitomo, T.; Usuda, M.; Kusaka, S.; Asao, Y.; Nakano, M.; Iwamoto, Y.; Tachikake, M.; Ogawa, M.; Kaneki, A.; et al. Evaluation of Periodontal Status and Oral Health Habits with Continual Dental Support for Young Patients with Hemophilia. Appl. Sci. 2024, 14, 1349. [Google Scholar] [CrossRef]
- Saunders, J.L.; Eleazer, P.D.; Zhang, P.; Michalek, S. Effect of a Separated Instrument on Bacterial Penetration of Obturated Root Canals. J. Endod. 2004, 30, 177–179. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Tooth | Root Canal | Type of Instrument | X-Ray Follow-Up | Influence on Successive Teeth |
|---|---|---|---|---|---|
| Pk M, 2016 [27] | #84 | Mesio-lingual canal | H file | 15 months | Not listed |
| Kaul R, 2022 [28] | #85 | Disto-buccal canal | K file | 6 months | Not listed |
| Present case | #55 | Mesio-buccal canal | Reamer | 17 months | Enamel hypoplasia |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, M.; Akitomo, T.; Ogawa, M.; Kametani, M.; Usuda, M.; Kusaka, S.; Mitsuhata, C.; Nomura, R. Case Study of a Broken Instrument in a Primary Tooth and Literature Review. Children 2025, 12, 149. https://doi.org/10.3390/children12020149
Nakano M, Akitomo T, Ogawa M, Kametani M, Usuda M, Kusaka S, Mitsuhata C, Nomura R. Case Study of a Broken Instrument in a Primary Tooth and Literature Review. Children. 2025; 12(2):149. https://doi.org/10.3390/children12020149
Chicago/Turabian StyleNakano, Masashi, Tatsuya Akitomo, Masashi Ogawa, Mariko Kametani, Momoko Usuda, Satoru Kusaka, Chieko Mitsuhata, and Ryota Nomura. 2025. "Case Study of a Broken Instrument in a Primary Tooth and Literature Review" Children 12, no. 2: 149. https://doi.org/10.3390/children12020149
APA StyleNakano, M., Akitomo, T., Ogawa, M., Kametani, M., Usuda, M., Kusaka, S., Mitsuhata, C., & Nomura, R. (2025). Case Study of a Broken Instrument in a Primary Tooth and Literature Review. Children, 12(2), 149. https://doi.org/10.3390/children12020149