

Pediatric Non-Alcoholic Fatty Liver Disease (NAFLD): Trends, Mortality, and Socioeconomic Disparities in the U.S., 1998–2020

 , and
, and 
Abstract
1. Introduction
- -
- Non-alcoholic fatty liver disease (NAFLD) is linked to obesity and type 2 diabetes.
- -
- The prevalence of NAFLD has been increasing in children due to rising obesity rates.
- -
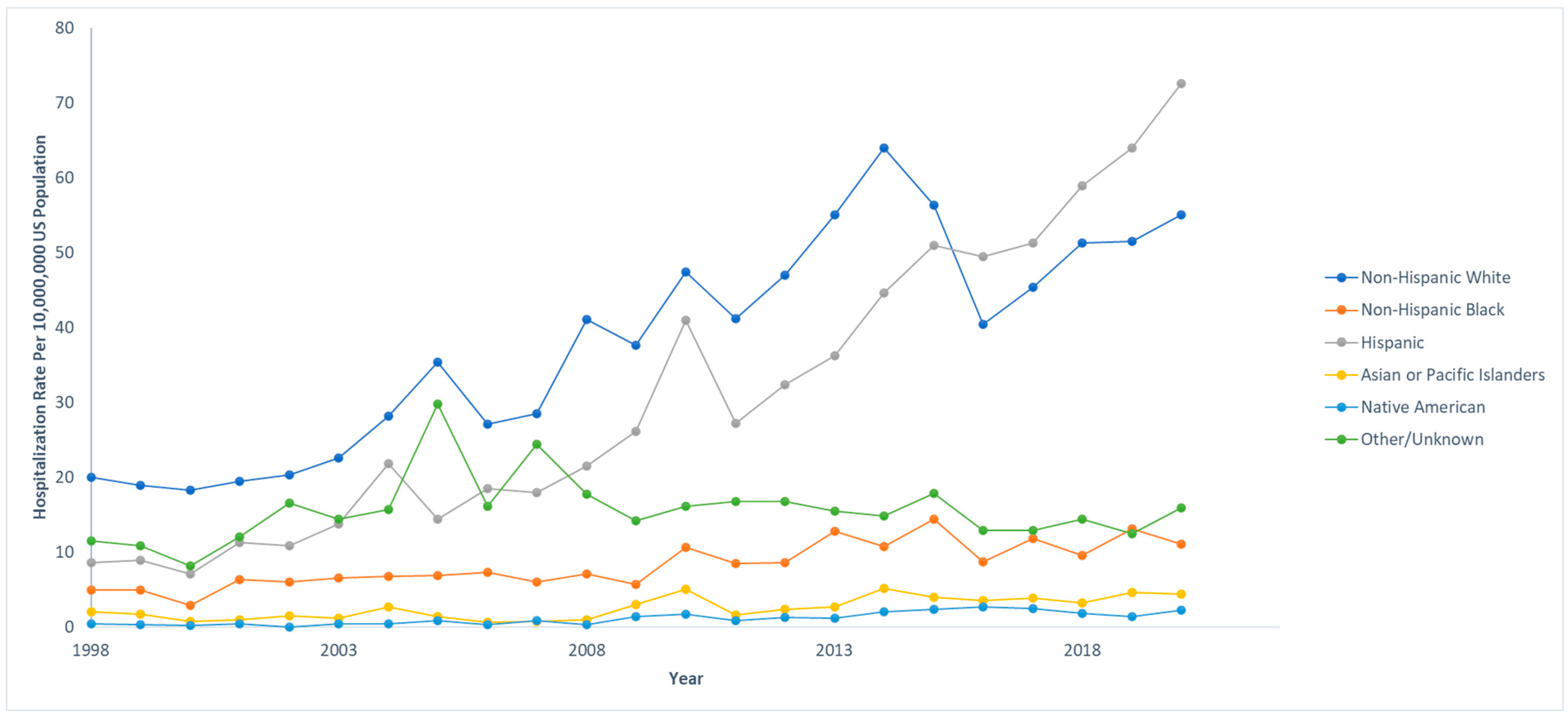
- NAFLD hospitalizations are more common among certain demographics, particularly Hispanic people.
- -
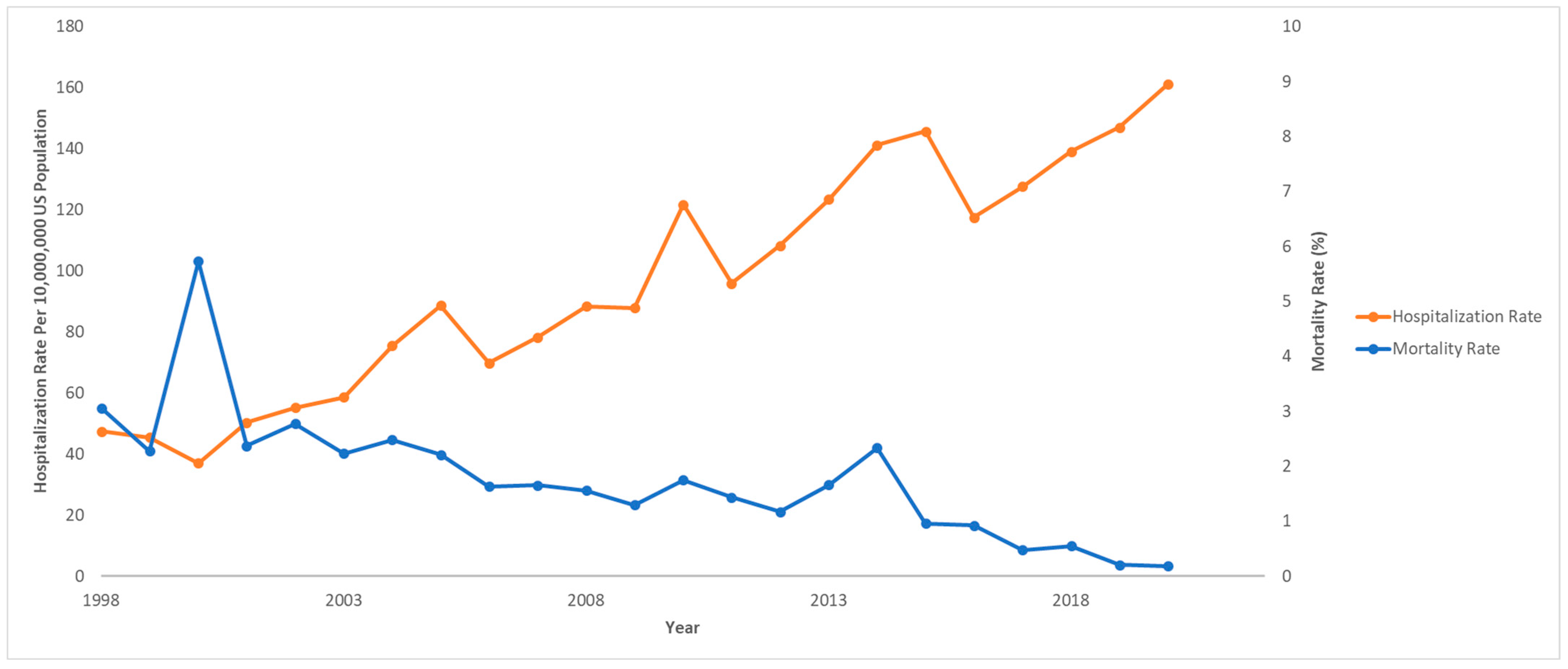
- Mortality rates in pediatric NAFLD decreased from 1998 to 2020, despite increasing hospitalization rates.
- -
- Risk factors associated with decreased mortality include older age (≥12 years), diabetes, and obesity, while coagulopathies significantly increase the risk of mortality.
- -
- Non-Hispanic Black children have the highest mortality rate from NAFLD, although they have lower hospitalization rates than Hispanic and non-Hispanic White children.
2. Materials and Methods
2.1. Study Population
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations and Acronyms
References
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef] [PubMed]
- Bessone, F.; Razori, M.V.; Roma, M.G. Molecular pathways of nonalcoholic fatty liver disease development and progression. Cell. Mol. Life Sci. 2019, 76, 99–128. [Google Scholar] [CrossRef] [PubMed]
- Arab, J.P.; Arrese, M.; Trauner, M. Recent Insights into the Pathogenesis of Nonalcoholic Fatty Liver Disease. Annu. Rev. Pathol. 2018, 13, 321–350. [Google Scholar] [CrossRef]
- Chen, Z.; Tian, R.; She, Z.; Cai, J.; Li, H. Role of oxidative stress in the pathogenesis of nonalcoholic fatty liver disease. Free Radic. Biol. Med. 2020, 152, 116–141. [Google Scholar] [CrossRef] [PubMed]
- Lebeaupin, C.; Vallée, D.; Hazari, Y.; Hetz, C.; Chevet, E.; Bailly-Maitre, B. Endoplasmic reticulum stress signalling and the pathogenesis of non-alcoholic fatty liver disease. J. Hepatol. 2018, 69, 927–947. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Baker, R.D.; Bhatia, T.; Zhu, L.; Baker, S.S. Pathogenesis of nonalcoholic steatohepatitis. Cell. Mol. Life Sci. 2016, 73, 1969–1987. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012, 142, 1592–1609. [Google Scholar] [CrossRef] [PubMed]
- Guan, H.; Shao, G.; Cheng, F.; Ni, P.; Wu, M. Risk factors of nonalcoholic fatty liver disease in healthy women. Medicine 2023, 102, e34437. [Google Scholar] [CrossRef] [PubMed]
- Muzurović, E.; Peng, C.C.; Belanger, M.J.; Sanoudou, D.; Mikhailidis, D.P.; Mantzoros, C.S. Nonalcoholic Fatty Liver Disease and Cardiovascular Disease: A Review of Shared Cardiometabolic Risk Factors. Hypertension 2022, 79, 1319–1326. [Google Scholar] [CrossRef]
- Seko, Y.; Yamaguchi, K.; Yano, K.; Takahashi, Y.; Takeuchi, K.; Kataoka, S.; Moriguchi, M.; Itoh, Y. The additive effect of genetic and metabolic factors in the pathogenesis of nonalcoholic fatty liver disease. Sci Rep. 2022, 12, 17608. [Google Scholar] [CrossRef]
- Ueno, M.; Takeda, H.; Takai, A.; Seno, H. Risk factors and diagnostic biomarkers for nonalcoholic fatty liver disease-associated hepatocellular carcinoma: Current evidence and future perspectives. World J. Gastroenterol. 2022, 28, 3410–3421. [Google Scholar] [CrossRef] [PubMed]
- Mosca, A.; De Cosmi, V.; Parazzini, F.; Raponi, M.; Alisi, A.; Agostoni, C.; Nobili, V. The Role of Genetic Predisposition, Programing During Fetal Life, Family Conditions, and Post-natal Diet in the Development of Pediatric Fatty Liver Disease. J. Pediatr. 2019, 211, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K.; Isaacs, S.; Barb, D.; Basu, R.; Caprio, S.; Garvey, W.T.; Kashyap, S.; Mechanick, J.I.; Mouzaki, M.; Nadolsky, K.; et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr. Pract. 2022, 28, 528–562. [Google Scholar]
- Powell, E.E.; Wong, V.W.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef] [PubMed]
- Kage, M.; Aishima, S.; Kusano, H.; Yano, H. Histopathological findings of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. J. Med. Ultrason. 2020, 47, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridi, M.; Cholongitas, E. Diagnosis of Non-alcoholic Fatty Liver Disease (NAFLD): Current Concepts. Curr Pharm Des. 2018, 24, 4574–4586. [Google Scholar] [CrossRef]
- Anderson, E.L.; Howe, L.D.; Jones, H.E.; Higgins, J.P.T.; Lawlor, D.A.; Fraser, A. The Prevalence of Non-Alcoholic Fatty Liver Disease in Children and Adolescents: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0140908. [Google Scholar] [CrossRef]
- Fernandes, D.M.; Pantangi, V.; Azam, M.; Salomao, M.; Iuga, A.C.; Lefkowitch, J.H.; Gill, J.; Morotti, R.; Lavine, J.E.; Mencin, A.A. Pediatric Nonalcoholic Fatty Liver Disease in New York City: An Autopsy Study. J. Pediatr. 2018, 200, 174–180. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Behling, C.; Newbury, R.; Deutsch, R.; Nievergelt, C.; Schork, N.J.; Lavine, J.E. Histopathology of pediatric nonalcoholic fatty liver disease. Hepatology 2005, 42, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Dybbro, E.; Dongarwar, D.; Salihu, H.M.; Ihekweazu, F.D. Trends and Disparities in Pediatric Nonalcoholic Fatty Liver Disease-Associated Hospitalizations in the United States. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Hilliard, M.E.; Powell, P.W.; Anderson, B.J. Evidence-based behavioral interventions to promote diabetes management in children, adolescents, and families. Am. Psychol. 2016, 71, 590–601. [Google Scholar] [CrossRef] [PubMed]
- Ispriantari, A.; Agustina, R.; Konlan, K.D.; Lee, H. Family-centered interventions for children and adolescents with type 1 diabetes mellitus: An integrative review. Child Health Nurs. Res. 2023, 29, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.M.; Rissel, C.; He, G. The Effect of Early Life Factors and Early Interventions on Childhood Overweight and Obesity 2016. J. Obes. 2017, 2017, 3642818. [Google Scholar] [CrossRef]
- Feldman, A.; Wernly, B.; Strebinger, G.; Eder, S.K.; Zandanell, S.; Niederseer, D.; Strasser, M.; Haufe, H.; Sotlar, K.; Paulweber, B.; et al. Liver-related Mortality is Increased in Lean Subjects with Non-alcoholic Fatty Liver Disease Compared to Overweight and Obese Subjects. J. Gastrointest. Liver Dis. 2021, 30, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Zou, B.; Hoang, J.; Jeong, D.; Bensen, R.; Nguyen, M.H. Racial and socioeconomic disparities in hospitalization of pediatrics with liver disease from 2005 to 2015. Dig. Dis. Sci. 2020, 66, 2240–2249. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.R.; Mathis, C.C.; Woods, A.K. African Americans and their distrust of the health care system: Healthcare for diverse populations. J. Cult. Divers. 2007, 14, 56–60. [Google Scholar] [PubMed]
- Becker, G.; Newsom, E. Socioeconomic status and dissatisfaction with health care among chronically ill African Americans. Am. J. Public Health 2003, 93, 742–748. [Google Scholar] [CrossRef]
- Wajsbrot, N.B.; Leite, N.C.; Salles, G.F.; Villela-Nogueira, C.A. Non-alcoholic fatty liver disease and the impact of genetic, epigenetic and environmental factors in the offspring. World J. Gastroenterol. 2022, 28, 2890–2899. [Google Scholar] [CrossRef]
- Dongiovanni, P.; Anstee, Q.M.; Valenti, L. Genetic predisposition in NAFLD and NASH: Impact on severity of liver disease and response to treatment. Curr. Pharm. Des. 2013, 19, 5219–5238. [Google Scholar] [CrossRef] [PubMed]
- Ogresta, D.; Mrzljak, A.; Cigrovski Berkovic, M.; Bilic-Curcic, I.; Stojsavljevic-Shapeski, S.; Virovic-Jukic, L. Coagulation and Endothelial Dysfunction Associated with NAFLD: Current Status and Therapeutic Implications. J. Clin. Transl. Hepatol. 2022, 10, 339–355. [Google Scholar] [CrossRef] [PubMed]
- Wattacheril, J.J.; Abdelmalek, M.F.; Lim, J.K.; Sanyal, A.J. AGA Clinical Practice Update on the Role of Noninvasive Biomarkers in the Evaluation and Management of Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology 2023, 165, 1080–1088. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Calzadilla-Bertot, L.; Wong, V.W.S.; Castellanos, M.; Aller-de la Fuente, R.; Metwally, M.; Eslam, M.; Gonzalez-Fabian, L.; Sanz, M.A.Q.; Conde-Martin, A.F.; et al. Fibrosis Severity as a Determinant of Cause-Specific Mortality in Patients with Advanced Nonalcoholic Fatty Liver Disease: A Multi-National Cohort Study. Gastroenterology 2018, 155, 443–457.e17. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | NAFLD Alive | NAFLD Died | p-Value |
|---|---|---|---|---|
| Number of Hospitalizations, N | 68,869 | 67,899 | 970 | |
| Age, Year, Median (IQR) | 13 (6–16) | 13 (7–16) | 4 (0–12) | <0.001 |
| Sex | 0.193 | |||
| Male, N (%) | 36,101 (52.4) | 35,683 (52.6) | 418 (43.1) | |
| Female, N (%) | 32,768 (47.6) | 32,216 (47.4) | 552 (56.9) | |
| Race/Ethnicity | ||||
| Non-Hispanic White, N (%) | 27,080 (39.3) | 26,689 (39.3) | 391 (40.3) | 0.126 |
| Non-Hispanic Black, N (%) | 5918 (8.6) | 5796 (8.5) | 122 (12.6) | |
| Hispanic, N (%) | 22,329 (32.4) | 22,070 (32.5) | 259 (26.7) | |
| Asian or Pacific Islander, N (%) | 1793 (2.6) | 1754 (2.6) | 39 (4.0) | |
| Native American, N (%) | 811 (1.2) | 807 (1.2) | ≤10 | |
| Other/Unknown, N (%) | 10,938 (15.9) | 10,783 (15.9) | 155 (16.0) | |
| Region of Hospital | 0.839 | |||
| Northeast, N (%) | 10,023 (14.6) | 9871 (14.5) | 152 (15.7) | |
| Midwest, N (%) | 11,785 (17.1) | 11,640 (17.1) | 145 (14.9) | |
| South, N (%) | 25,142 (36.5) | 24,805 (36.5) | 337 (34.7) | |
| West, N (%) | 19,968 (29.0) | 19,680 (29.0) | 288 (29.7) | |
| Type of Hospital | 0.037 | |||
| Rural, N (%) | 2349 (3.4) | 2334 (3.4) | 15 (1.5) | |
| Urban Non-Teaching, N (%) | 8746 (12.7) | 8671 (12.8) | 75 (7.7) | |
| Urban Teaching, N (%) | 55,514 (80.6) | 54,686 (80.5) | 828 (85.4) |
| Risk Factors | Crude Odds Ratio (95% CI) | Crude p-Value | Adjusted Odds Ratio (95% CI) | Adjusted p-Value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age | ≥12 (vs. <12) | 0.25 (0.19–0.35) | <0.001 | 0.41 (0.30–0.57) | <0.001 |
| Sex | Female (vs. Male) | 0.83 (0.63–1.10) | 0.194 | 0.92 (0.69–1.23) | 0.577 |
| Race/Ethnicity | White (vs. Other) | 1.03 (0.77–1.39) | 0.839 | - | - |
| Metabolic Disorders | |||||
| Diabetes | Yes (vs. No) | 0.12 (0.05–0.33) | <0.001 | 0.30 (0.11–0.82) | 0.019 |
| Obesity | Yes (vs. No) | 0.10 (0.05–0.21) | <0.001 | 0.18 (0.08–0.37) | <0.001 |
| Co-Infections | |||||
| Hepatitis B | Yes (vs. No) | 5.97 (0.78–46.15) | 0.087 | 4.84 (0.70–33.47) | 0.110 |
| Hepatitis C | Yes (vs. No) | 3.03 (0.41–22.55) | 0.278 | - | - |
| HIV Positive | Yes (vs. No) | 4.03 (1.24–13.11) | 0.021 | 2.85 (0.85–9.52) | 0.089 |
| Social Factors | |||||
| Intravenous Drug Use | Yes (vs. No) | 2.73 (0.66–11.28) | 0.165 | 2.41 (0.48–12.15) | 0.288 |
| Other | |||||
| Coagulopathy | Yes (vs. No) | 6.12 (4.36–8.59) | <0.001 | 4.42 (3.10–6.29) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wasuwanich, P.; So, J.M.; Sadek, M.; Jarasvaraparn, C.; Rajborirug, S.; Quiros-Tejeira, R.E.; Karnsakul, W. Pediatric Non-Alcoholic Fatty Liver Disease (NAFLD): Trends, Mortality, and Socioeconomic Disparities in the U.S., 1998–2020. Children 2025, 12, 71. https://doi.org/10.3390/children12010071
Wasuwanich P, So JM, Sadek M, Jarasvaraparn C, Rajborirug S, Quiros-Tejeira RE, Karnsakul W. Pediatric Non-Alcoholic Fatty Liver Disease (NAFLD): Trends, Mortality, and Socioeconomic Disparities in the U.S., 1998–2020. Children. 2025; 12(1):71. https://doi.org/10.3390/children12010071
Chicago/Turabian StyleWasuwanich, Paul, Joshua M. So, Mustafa Sadek, Chaowapong Jarasvaraparn, Songyos Rajborirug, Ruben E. Quiros-Tejeira, and Wikrom Karnsakul. 2025. "Pediatric Non-Alcoholic Fatty Liver Disease (NAFLD): Trends, Mortality, and Socioeconomic Disparities in the U.S., 1998–2020" Children 12, no. 1: 71. https://doi.org/10.3390/children12010071
APA StyleWasuwanich, P., So, J. M., Sadek, M., Jarasvaraparn, C., Rajborirug, S., Quiros-Tejeira, R. E., & Karnsakul, W. (2025). Pediatric Non-Alcoholic Fatty Liver Disease (NAFLD): Trends, Mortality, and Socioeconomic Disparities in the U.S., 1998–2020. Children, 12(1), 71. https://doi.org/10.3390/children12010071