
Organization of the Cytoskeleton in Ectopic Foci of the Endometrium with Rare Localization


Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
- -
- Group 1 (n = 6): a control group of women with confirmed menopause for at least 3 years prior to the study who had no anamnesis of endometriosis. Biomaterial: eutopic endometrium without pathology, obtained by separate diagnostic curettage for a polyp (however, polyp tissue was not included in the tissues for investigation for all groups).
- -
- Group 2 (n = 6): a control group of fertile women whose average age corresponded to the age of patients with endometriosis, but who had no anamnesis of endometriosis. Biomaterial: eutopic endometrium without pathology, obtained by separate diagnostic curettage for polyps.
- -
- Group 3 (n = 5): a group of patients with adenomyosis. Biomaterial: eutopic endometrium, obtained by separate diagnostic curettage for polyps or menorrhagia.
- -
- Group 4 (n = 4): a group of patients with external genital endometriosis. Biomaterial: ectopic endometrium (localization-ovaries and/or projection of the posterior surface of the cervix), obtained laparoscopically.
- -
- Group 5 (n = 4): a group of patients with extragenital endometriosis. Biomaterial: ectopic endometrium (localization-pelvic peritoneum).
- -
- Group 6 (n = 2): two patients with histologically confirmed umbilical endometriosis.
2.2. Protein Extraction and Western Blotting
2.3. Evaluation of the Relative mRNA Level by Quantitative PCR
2.4. Determination of 5-hydroxymethylcytosine (5hmC) Content in DNA by the Dot Blot Method
2.5. Statistical Analysis
3. Results
3.1. Clinical Observation
3.2. Cytoskeletal Proteins ant Its mRNA Content
3.3. Acetylase/Deacetylase Relative Content
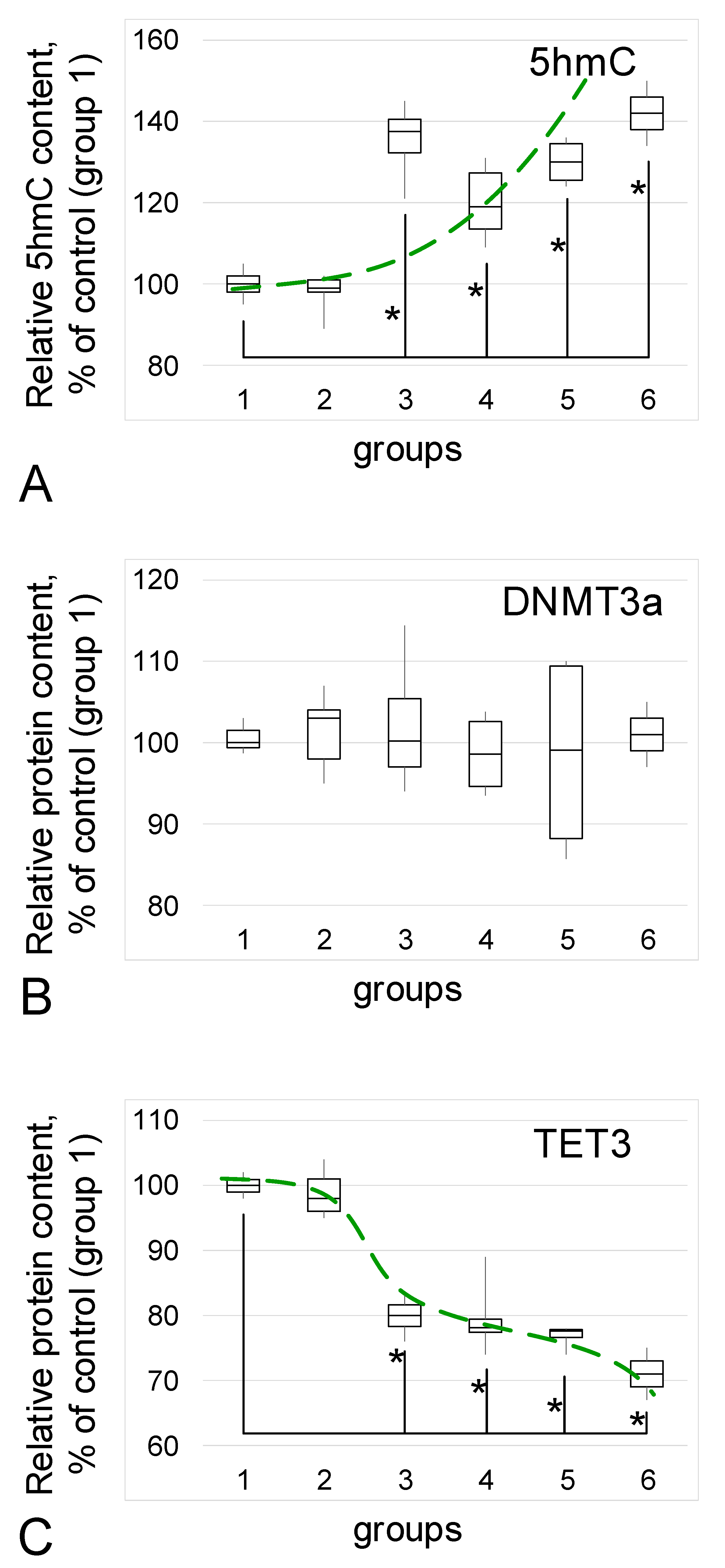
3.4. 5hmC Content and Methylase/Demethylase Relative Content
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Albertsen, H.M.; Ward, K. Genes Linked to Endometriosis by GWAS Are Integral to Cytoskeleton Regulation and Suggests That Mesothelial Barrier Homeostasis Is a Factor in the Pathogenesis of Endometriosis. Reprod. Sci. 2016, 24, 803–811. [Google Scholar] [CrossRef]
- Proestling, K.; Birner, P.; Gamperl, S.; Nirtl, N.; Marton, E.; Yerlikaya, G.; Wenzl, R.; Streubel, B.; Husslein, H. Enhanced epi-thelial to mesenchymal transition (EMT) and upregulated MYC in ectopic lesions contribute independently to endometriosis. Reprod. Biol. Endocrinol. 2015, 13, 75. [Google Scholar] [CrossRef] [PubMed]
- Bartley, J.; Jülicher, A.; Hotz, B.; Mechsner, S.; Hotz, H. Epithelial to mesenchymal transition (EMT) seems to be regulated differently in endometriosis and the endometrium. Arch. Gynecol. Obstet. 2013, 289, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Bostanci Durmus, A.; Dincer Cengiz, S.; Yılmaz, H.; Candar, T.; Gursoy, A.Y.; Sinem Caglar, G. The levels of matrix metallo-proteinase-9 and neutrophil gelatinase-associated lipocalin in different stages of endometriosis. J. Obstet. Gynaecol. 2019, 39, 991–995. [Google Scholar] [CrossRef]
- Christodoulakos, G.; Augoulea, A.; Lambrinoudaki, I.; Sioulas, V.; Creatsas, G. Pathogenesis of endometriosis: The role of de-fective ‘immunosurveillance’. Eur. J. Contracept Reprod. Health Care 2007, 12, 194–202. [Google Scholar] [CrossRef]
- Ulukus, M.; Ulukus, E.C.; Goker, E.N.T.; Tavmergen, E.; Zheng, W.; Arici, A. Expression of interleukin-8 and mon-ocyte chemotactic protein 1 in women with endometriosis. Fertil. Steril. 2009, 91, 687–693. [Google Scholar] [CrossRef]
- Sikora, J.; Smycz-Kubańska, M.; Mielczarek-Palacz, A.; Kondera-Anasz, Z. Abnormal peritoneal regulation of chemokine activation-The role of IL-8 in pathogenesis of endometriosis. Am. J. Reprod. Immunol. 2017, 77, e12622. [Google Scholar] [CrossRef] [PubMed]
- McLaren, J. Vascular endothelial growth factor and endometriotic angiogenesis. Hum. Reprod. Updat. 2000, 6, 45–55. [Google Scholar] [CrossRef]
- Shifren, J.L.; Tseng, J.F.; Zaloudek, C.J.; Ryan, I.P.; Meng, Y.G.; Ferrara, N.; Jaffe, R.B.; Taylor, R.N. Ovarian steroid regulation of vascular endothelial growth factor in the human endometrium: Implications for angiogenesis during the menstrual cycle and in the pathogenesis of endometriosis. J. Clin. Endocrinol. Metab. 1996, 81, 3112–3118. [Google Scholar] [CrossRef][Green Version]
- Hortu, I.; Ozceltik, G.; Karadadas, E.; Erbas, O.; Yigitturk, G.; Ulukus, M. The Role of Ankaferd Blood Stopper and Oxytocin as Potential Therapeutic Agents in Endometriosis: A Rat Model. Curr. Med. Sci. 2020, 40, 556–562. [Google Scholar] [CrossRef]
- Zhang, T.; De Carolis, C.; Man, C.W.; Wang, C.C. The link between immunity, autoimmunity and endometriosis: A literature update. Autoimmun. Rev. 2018, 17, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Akoum, A.; Kong, J.; Metz, C.; Beaumont, M.C. Spontaneous and stimulated secretion of monocyte chemotactic protein-1 and macrophage migration inhibitory factor by peritoneal macrophages in women with and without endometriosis. Fertil. Steril. 2002, 77, 989–994. [Google Scholar] [CrossRef]
- Wu, J.; Xie, H.; Yao, S.; Liang, Y. Macrophage and nerve interaction in endometriosis. J. Neuroinflamm. 2017, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Sikora, J.; Wróblewska-Czech, A.; Smycz-Kubańska, M.; Mielczarek-Palacz, A.; Cygal, A.; Witek, A.; Kondera-Anasz, Z. The role of complement components C1q, MBL and C1 inhibitor in pathogenesis of endometriosis. Arch. Gynecol. Obstet. 2018, 297, 1495–1501. [Google Scholar] [CrossRef]
- Karadadas, E.; Hortu, I.; Ak, H.; Ergenoglu, A.M.; Karadadas, N.; Aydin, H.H. Evaluation of complement system proteins C3a, C5a and C6 in patients of endometriosis. Clin. Biochem. 2020, 81, 15–19. [Google Scholar] [CrossRef]
- Schulke, L.; Berbic, M.; Manconi, F.; Tokushige, N.; Markham, R.; Fraser, I.S. Dendritic cellpopulations in the eutopic and ectopic endometrium of women with endometriosis. Hum. Reprod. 2009, 24, 1695–1703. [Google Scholar] [CrossRef]
- Emmanuel, I.; Ochigbo, A.; Philip, A.; Nyam, E.Y. Adenomyosis:A Clinico-pathological Study. W. Afr. J. Med. 2019, 36, 88–92. [Google Scholar]
- Sampson, J.A. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am. J. Obstet. Gynecol. 1927, 14, 422–469. [Google Scholar] [CrossRef]
- Nahar, K.; Ferdous, B.; Akhter, N.; Shamsunnahar, P.A.; Khatun, K.; Begum, S.A.; Aziz, M.A. Ovarian Endometrioid Ade-nocarcinoma Arising in Endometriosis: A Case Report. Mymensingh Med. J. 2018, 27, 420–423. [Google Scholar]
- Tsai, C.; Huang, S.-H.; Huang, C.-Y. Polypoid endometriosis-A rare entity of endometriosis mimicking ovarian cancer. Taiwan. J. Obstet. Gynecol. 2019, 58, 328–329. [Google Scholar] [CrossRef]
- Saliba, C.; Jaafoury, H.; El Hajj, M.; Nicolas, G.; Ahmad, H.H. Abdominal Wall Endometriosis: A Case Report. Cureus 2019, 11, e4061. [Google Scholar] [CrossRef]
- Flieder, D.B.; Moran, C.A.; Travis, W.D.; Koss, M.N.; Mark, E.J. Pleuro-pulmonary endometriosis and pulmonary ectopic de-ciduosis: A clinicopathologic and immunohistochemical study of 10 cases with emphasis on diagnostic pitfalls. Hum. Pathol. 1998, 29, 1495–1503. [Google Scholar] [CrossRef]
- Ping, S.; Ma, C.; Liu, P.; Yang, L.; Yang, X.; Wu, Q.; Zhao, X.; Gong, B. Molecular mechanisms underlying endometriosis pathogenesis revealed by bioinformatics analysis of microarray data. Arch. Gynecol. Obstet. 2015, 293, 797–804. [Google Scholar] [CrossRef]
- Flamini, M.; Sánchez, A.; Goglia, L.; Tosi, V.; Genazzani, A.; Simoncini, T. Differential actions of estrogen and SERMs in regulation of the actin cytoskeleton of endometrial cells. Mol. Hum. Reprod. 2009, 15, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Gentilini, D.; Vigano, P.; Somigliana, E.; Vicentini, L.M.; Vignali, M.; Busacca, M.; Di Blasio, A.M. Endometrial stromal cells from women with endometriosis reveal peculiar migratory behavior in response to ovarian steroids. Fertil. Steril. 2010, 93, 706–715. [Google Scholar] [CrossRef]
- Giudice, L.C.; Kao, L.C. Endometriosis. Lancet 2004, 364, 1789–1799. [Google Scholar] [CrossRef]
- Bulun, S.E. Endometriosis. N. Engl. J. Med. 2009, 360, 268–279. [Google Scholar] [CrossRef]
- Yilmaz, B.D.; E Bulun, S. Endometriosis and nuclear receptors. Hum. Reprod. Updat. 2019, 25, 473–485. [Google Scholar] [CrossRef]
- Bulun, S.E.; Cheng, Y.-H.; Pavone, M.E.; Xue, Q.; Attar, E.; Trukhacheva, E.; Tokunaga, H.; Utsunomiya, H.; Yin, P.; Luo, X.; et al. Estrogen Receptor-β, Estrogen Receptor-α, and Progesterone Resistance in Endometriosis. Semin. Reprod. Med. 2010, 28, 036–043. [Google Scholar] [CrossRef]
- Monsivais, D.; Dyson, M.T.; Yin, P.; Navarro, A.; Coon, J.S.; Pavone, M.E.; Bulun, S.E. Estrogen receptor β regulates en-dometriotic cell survival through serum and glucocorticoid-regulated kinase activation. Fertil. Steril. 2016, 105, 1266–1273. [Google Scholar] [CrossRef]
- Takayama, K.; Zeitoun, K.; Gunby, R.T.; Sasano, H.; Carr, B.R.; Bulun, S.E. Treatment of severe postmenopausal endometriosis with an aromatase inhibitor. Fertil. Steril. 1998, 69, 709–713. [Google Scholar] [CrossRef]
- Soysal, S.; Soysal, M.E.; Ozer, S.; Gul, N.; Gezgin, T. The effects of post-surgical administration of goserelin plus anastrozole compared to goserelin alone in patients with severe endometriosis: A prospective randomized trial. Hum. Reprod. 2004, 19, 160–167. [Google Scholar] [CrossRef]
- Ecker, A.M.; Donnellan, N.M.; Shepherd, J.P.; Lee, T.T. Abdominal wall endometriosis: 12 years of experience at a large aca-demic institution. Am. J. Obstet. Gynecol. 2014, 211, 363.e1–363.e5. [Google Scholar] [CrossRef]
- Jaime, T.J.; Jaime, T.J.; Ormiga, P.; Leal, F.; Nogueira, O.M.; Rodrigues, N. Umbilical endometriosis: Report of a case and its dermoscopic features*. An. Bras. de Dermatol. 2013, 88, 121–124. [Google Scholar] [CrossRef]
- Loh, S.-H.; Lew, B.-L.; Sim, W.-Y. Primary Cutaneous Endometriosis of Umbilicus. Ann. Dermatol. 2017, 29, 621–625. [Google Scholar] [CrossRef]
- Wan, C.; Chen, L. Primary cutaneous endometriosis of the umbilicus. Indian J. Dermatol. Venereol. Leprol. 2021, 87, 146–146. [Google Scholar] [CrossRef]
- Tentler, D.; Lomert, E.; Novitskaya, K.; Barlev, N.A. Role of ACTN4 in Tumorigenesis, Metastasis, and EMT. Cells 2019, 8, 1427. [Google Scholar] [CrossRef]
- Xu, J.; Lv, H.; Zhang, B.; Xu, F.; Zhu, H.; Chen, B.; Zhu, C.; Shen, J. miR-30b-5p acts as a tumor suppressor microRNA in esophageal squamous cell carcinoma. J. Thorac. Dis. 2019, 11, 3015–3029. [Google Scholar] [CrossRef]
- Kovac, B.; Mäkelä, T.P.; Vallenius, T. Increased α-actinin-1 destabilizes E-cadherin-based adhesions and associates with poor prognosis in basal-like breast cancer. PLoS ONE 2018, 13, e0196986. [Google Scholar] [CrossRef]
- Li, C.F.; Wang, J.M.; Kang, H.Y.; Huang, C.K.; Wang, J.W.; Fang, F.M.; Wang, Y.H.; Wu, W.R.; Li, S.H.; Yu, S.C.; et al. Characterization of gene amplification-driven SKP2 overexpression in myxofibrosar-coma: Potential implications in tumor progression and therapeutics. Clin. Cancer Res. 2012, 18, 1598–1610. [Google Scholar] [CrossRef] [PubMed]
- Torrino, S.; Grasset, E.M.; Audebert, S.; Belhadj, I.; Lacoux, C.; Haynes, M.; Pisano, S.; Abélanet, S.; Brau, F.; Chan, S.Y.; et al. Mechano-induced cell metabolism promotes microtubule glutamylation to force metastasis. Cell Metab. 2021, 33, 1342–1357.e10. [Google Scholar] [CrossRef]
- Wattanathamsan, O.; Thararattanobon, R.; Rodsiri, R.; Chanvorachote, P.; Vinayanuwattikun, C.; Pongrakhananon, V. Tu-bulin acetylation enhances lung cancer resistance to paclitaxel-induced cell death through Mcl-1 stabilization. Cell Death Discov. 2021, 7, 67. [Google Scholar] [CrossRef]
- Zhu, H.; Li, W.; Shuai, W.; Liu, Y.; Yang, L.; Tan, Y.; Zheng, T.; Yao, H.; Xu, J.; Zhu, Z.; et al. Discovery of novel N-benzylbenzamide derivatives as tubulin polymerization inhibitors with potent antitumor activities. Eur. J. Med. Chem. 2021, 216, 113316. [Google Scholar] [CrossRef]
- Vicari, H.P.; Lima, K.; Gomes, R.D.C.; Fernandes, D.C.; da Silva, J.C.L.; Junior, M.T.R.; de Oliveira, A.S.B.; dos Santos, R.N.; Andricopulo, A.D.; Coelho, F.; et al. Synthetic cyclopenta[b]indoles exhibit antineoplastic activity by targeting microtubule dynamics in acute myeloid leukemia cells. Eur. J. Pharmacol. 2021, 894, 173853. [Google Scholar] [CrossRef]
- Araujo-Silva, C.A.; De Souza, W.; Martins-Duarte, E.S.; Vommaro, R.C. HDAC inhibitors Tubastatin A and SAHA affect parasite cell division and are potential anti-Toxoplasma gondii chemotherapeutics. Int. J. Parasitol. Drugs Drug Resist. 2020, 15, 25–35. [Google Scholar] [CrossRef]
- Colón-Díaz, M.; Báez-Vega, P.; García, M.; Ruiz, A.; Monteiro, J.B.; Fourquet, J.; Bayona, M.; Alvarez-Garriga, C.; Achille, A.; Seto, E.; et al. HDAC1 and HDAC2 are Differentially Expressed in Endometriosis. Reprod. Sci. 2012, 19, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Xia, M.; Zhao, M.; Ma, J.; Fang, X. Aberrant histone acetylation and methylation levels in woman with endometriosis. Arch. Gynecol. Obstet. 2013, 287, 487–494. [Google Scholar]
- Samartzis, E.P.; Noske, A.; Samartzis, N.; Fink, D.; Imesch, P. The Expression of Histone Deacetylase 1, But Not Other Class I Histone Deacetylases, Is Significantly Increased in Endometriosis. Reprod. Sci. 2013, 20, 1416–1422. [Google Scholar] [CrossRef]
- Szwagierczak, A.; Bultmann, S.; Schmidt, C.S.; Spada, F.; Leonhardt, H. Sensitive enzymatic quantification of 5-hydroxymethylcytosine in genomic DNA. Nucleic Acids Res. 2010, 38, e181–e181. [Google Scholar] [CrossRef] [PubMed]
- Bochtler, M.; Kolano, A.; Xu, G.-L. DNA demethylation pathways: Additional players and regulators. BioEssays 2016, 39, 1–13. [Google Scholar] [CrossRef]
- Nan, X.; Ng, H.H.; Johnson, C.A.; Laherty, C.D.; Turner, B.M.; Eisenman, R.N.; Bird, A. Transcriptional repression by the methyl-CpG-binding protein MeCP2 involves a histone deacetylase complex. Nature 1998, 393, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, T.-H. Effects of DNA Methylation on the Structure of Nucleosomes. J. Am. Chem. Soc. 2011, 134, 173–175. [Google Scholar] [CrossRef]
- Das, P.M.; Singal, R. DNA Methylation and Cancer. J. Clin. Oncol. 2004, 22, 4632–4642. [Google Scholar] [CrossRef] [PubMed]
- Loktev, S.S.; Ogneva, I.V. DNA Methylation of Mouse Testes, Cardiac and Lung Tissue During Long-Term Microgravity Simulation. Sci. Rep. 2019, 9, 7974. [Google Scholar] [CrossRef] [PubMed]
- Pappalardo, X.G.; Barra, V. Losing DNA methylation at repetitive elements and breaking bad. Epigenetics Chromatin 2021, 14, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Calaway, J.D.; Domínguez, J.I.; Hanson, M.E.; Cambranis, E.C.; de Villena, F.P.-M.; de la Casa-Esperon, E. Intronic parent-of-origin dependent differential methylation at the Actn1 gene is conserved in rodents but is not associated with im-printed expression. PLoS ONE 2012, 7, e48936. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.-W. Endometriosis and ovarian cancer: Potential benefits and harms of screening and risk-reducing surgery. Fertil. Steril. 2015, 104, 813–830. [Google Scholar] [CrossRef]
- Vercellini, P.; Scarfone, G.; Bolis, G.; Stellato, G.; Carinelli, S.; Crosignani, P.G. Site of origin of epithelial ovarian cancer: The endometriosis connection. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 1155–1157. [Google Scholar] [CrossRef]
- Matalliotakis, M.; Matalliotaki, C.; Goulielmos, G.N.; Patelarou, E.; Tzardi, M.; Spandidos, D.; Arici, A.; Matalliotakis, I. Association between ovarian cancer and advanced endometriosis. Oncol. Lett. 2018, 15, 7689–7692. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protein | Manufacturer with Catalog Number, Dilution |
|---|---|
| ACTB (beta-actin, 42 kDa) | Santa Cruz Biotechnology, Inc., Paso Robles, CA, USA, #sc-81178, 1:300 |
| ACTG1 (gamma-actin, 42 kDa) | Santa Cruz Biotechnology, Inc., Paso Robles, CA, USA, #sc-65638, 1:100 |
| ACTN1 (alpha-actinin1, 103 kDa) | Santa Cruz Biotechnology, Inc., Paso Robles, CA, USA, #sc-17829, 1:500 |
| ACTN4 (alpha-actinin4, 102 kDa) | Santa Cruz Biotechnology, Inc., Paso Robles, CA, USA, #sc-393495, 1:100 |
| TUBA1C (alpha-tubulin, 50 kDa) | Abcam, Cambridge, UK, #ab52866, 1:1000–1:50,000 |
| TUBB4B (beta-tubulin, 50 kDa) | Abcam, Cambridge, UK, #ab179513, 1:1000 |
| TET3 (tet methylcytosine dioxygenase 2, 179 kDa) | Abcam, Cambridge, UK, #ab139805, 2 mkg/mL |
| DNMT3A (120 kDa) | Abcam, Cambridge, UK, #ab2850, 2 mkg/mL |
| HAT1 (histone acetylase, 45 kDa) | Abcam, Cambridge, UK, #ab194296, 1:1000 |
| HDAC1 (histone deacetylase, 55 kDa) | Abcam, Cambridge, UK, #ab109411, 1:1000 |
| Gene | Primer Sequence, Forward/Reverse (5′… 3′) | Product Size, bp |
|---|---|---|
| ACTB | CTCGCCTTTGCCGATCC/TCTCCATGTCGTCCCAGTTG | 298 |
| ACTG1 | GTTTCTCTGCCGGTCGCAAT/CCGACGATGGAAGGAAACA | 126 |
| ACTN1 | GTGTCCGCCTAGTTCAGTGT/ATTGACCGCCAACACTTTGC | 251 |
| ACTN4 | AATCCAATGAGCACCTCCGC/TGGTGTGCTTGTTGTCGAAG | 243 |
| TUBA1C | CCGGCCACCCTTTCACTACT/CTCATCGTCTCCTTCAGCACT | 76 |
| TUBB4B | CCACCTCGGGGGCTAAAAAT/CCTCGGTGAACTCCATCTCG | 163 |
| Parameter | Group 1 (Control) | Group 2 (Control) | Group 3 (Adenomyosis) | Group 4 (Genital EM) | Group 5 (Extragenital EM) | Group 6 (Umbilical EM) |
|---|---|---|---|---|---|---|
| Hemoglobin, g/L | 139 ± 8 | 127 ± 5 | 123 ± 4 | 129 ± 7 | 136 ± 5 | 123 ± 0.5 |
| Leukocytes, 109/L | 6.4 ± 0.6 | 6.6 ± 0.9 | 6.9 ± 1.4 | 6.3 ± 0.3 | 7.0 ± 0.5 | 7.0 ± 0.9 |
| Cause of the surgery | Polyp in the uterus | Polyp in the uterus | Polyp in the uterus or menorrhagia | Ovarian cyst | Ectopic loci at the pelvic peritoneum | Ectopic loci in the umbilicus |
| Stage of the process (size of the neoplasm, mm) | 9.3 ± 1.3 | 8.5 ± 0.9 | 11 ± 2 | 39 ± 4 | 2–3 | 10 (YP), 0.8 (OP) |
| Endometrial thickness, mm (Seventh day of the menstrual cycle, for group 1—any day) | 5.0 ± 0.6 | 8.0 ± 0.7 | 13.3 ± 0.3 * | 7.3 ± 0.5 | 7.5 ± 1.1 | 7.7 ± 0.1 |
| Severity of the process (number of pathological loci) | 1 | 1–2 | 1 | 1 | 2–4 | 1 (YP), 5 (OP) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toniyan, K.A.; Povorova, V.V.; Gorbacheva, E.Y.; Boyarintsev, V.V.; Ogneva, I.V. Organization of the Cytoskeleton in Ectopic Foci of the Endometrium with Rare Localization. Biomedicines 2021, 9, 998. https://doi.org/10.3390/biomedicines9080998
Toniyan KA, Povorova VV, Gorbacheva EY, Boyarintsev VV, Ogneva IV. Organization of the Cytoskeleton in Ectopic Foci of the Endometrium with Rare Localization. Biomedicines. 2021; 9(8):998. https://doi.org/10.3390/biomedicines9080998
Chicago/Turabian StyleToniyan, Konstantin A., Victoria V. Povorova, Elena Yu. Gorbacheva, Valery V. Boyarintsev, and Irina V. Ogneva. 2021. "Organization of the Cytoskeleton in Ectopic Foci of the Endometrium with Rare Localization" Biomedicines 9, no. 8: 998. https://doi.org/10.3390/biomedicines9080998
APA StyleToniyan, K. A., Povorova, V. V., Gorbacheva, E. Y., Boyarintsev, V. V., & Ogneva, I. V. (2021). Organization of the Cytoskeleton in Ectopic Foci of the Endometrium with Rare Localization. Biomedicines, 9(8), 998. https://doi.org/10.3390/biomedicines9080998