
Viability Assessment in Liver Transplantation—What Is the Impact of Dynamic Organ Preservation?


 ,
,  and
and
Abstract
1. Introduction
2. What Do We Expect from a Viability Test?
3. Why Is Viability Testing Clinically Relevant?
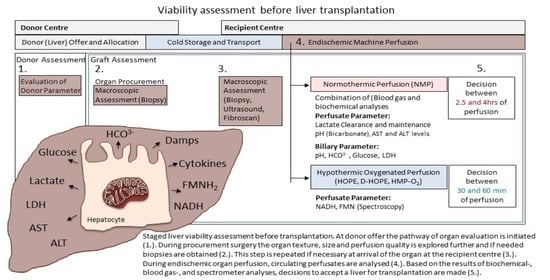
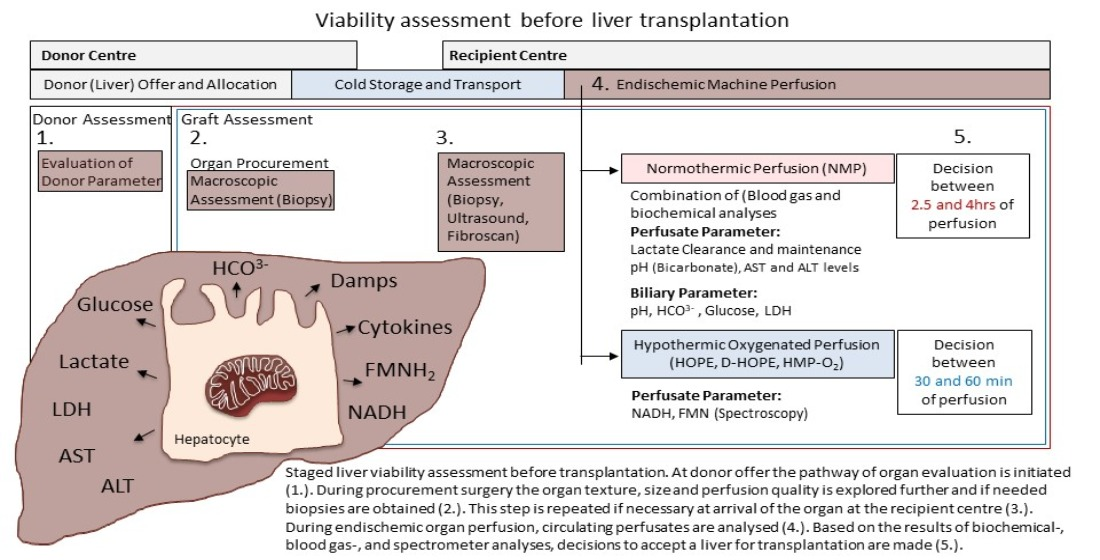
4. What Are Available Modalities to Test Viability?
5. What Is More Important: Liver Injury or Function?
6. How Do We Test Viability during Normothermic Machine Liver Perfusion?
6.1. Perfusion Quality and Hemodynamic Parameter
6.2. How Helpful Is the Quantification of Liver Transaminases?
6.3. What Is the Predictive Value of Lactate?
6.4. Perfusate Acid Balance and pH
6.5. Glucose Metabolism
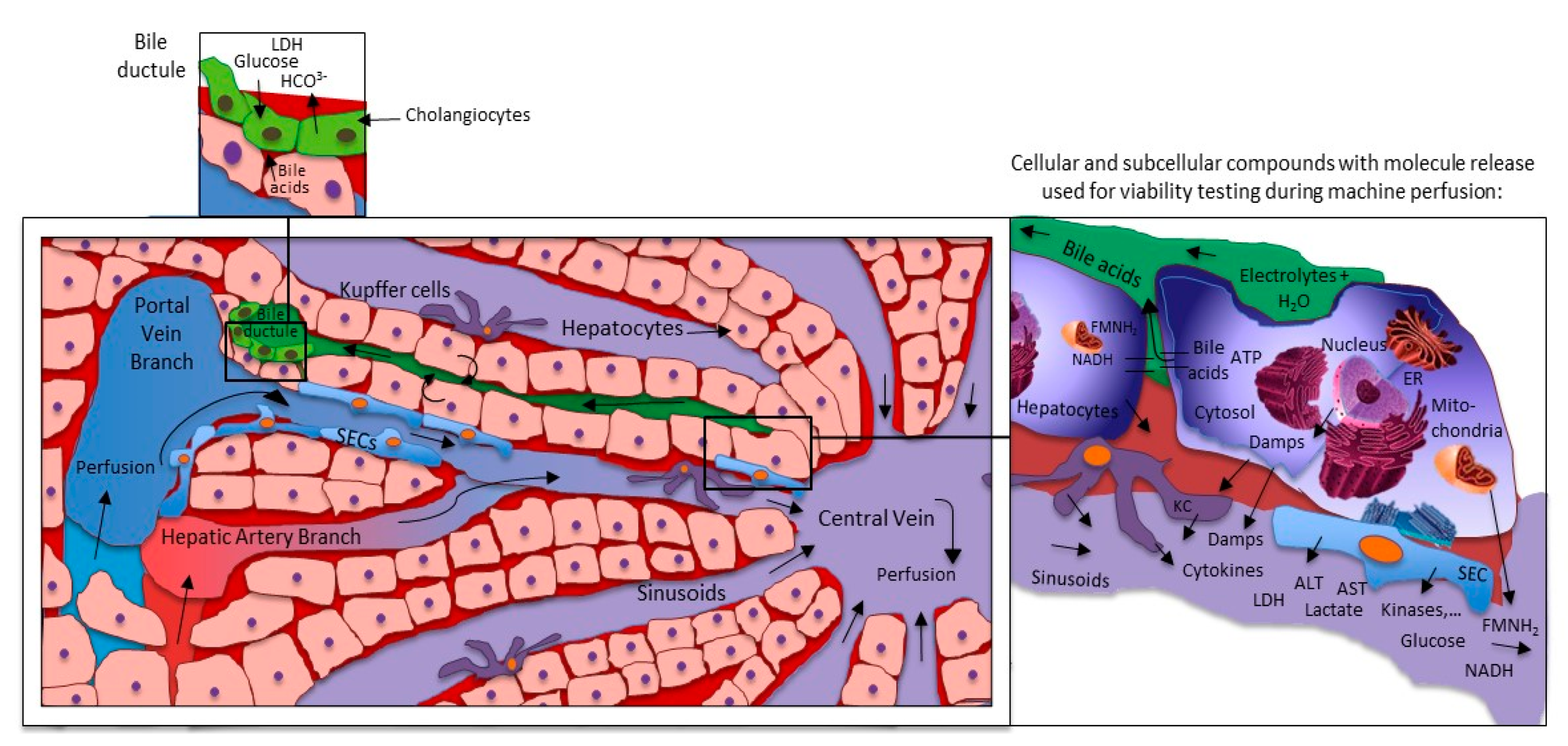
6.6. How to Assess the “Biliary Tree” during Machine Perfusion?
6.7. Clinical Decision Making Based on Viability Parameter
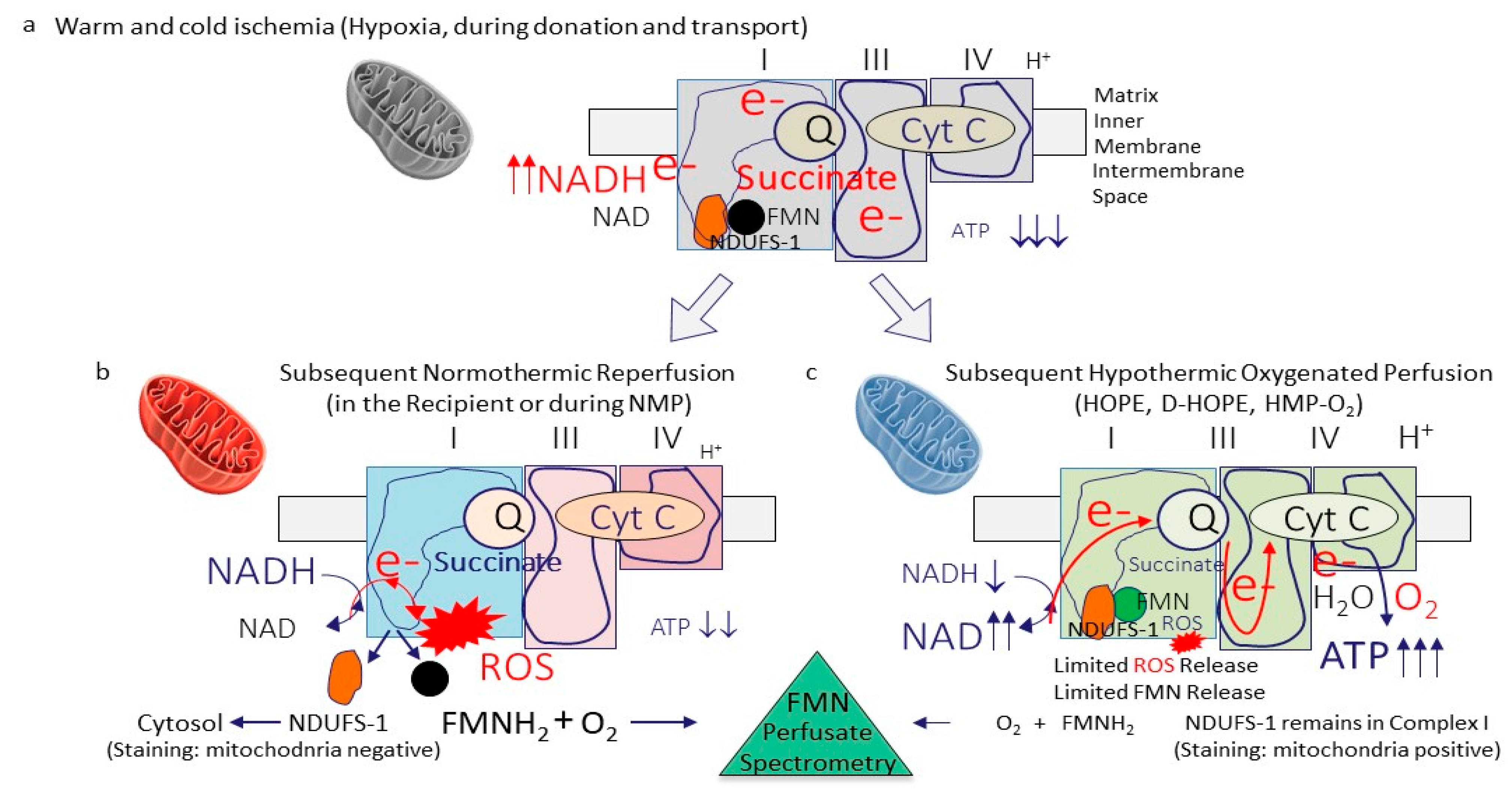
7. Viability Assessment during Hypothermic Oxygenated Perfusion
7.1. Can We Use the Same Parameters as in Normothermic Liver Perfusion?
7.2. How Can We Assess Mitochondrial Function and Injury?
8. Summary and Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schlegel, A.; Muller, X.; Dutkowski, P. Hypothermic Liver Perfusion. Curr. Opin. Organ. Transpl. 2017, 22, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Boteon, Y.; Afford, S.; Mergental, H. Pushing the Limits: Machine Preservation of the Liver as a Tool to Recondition High-Risk Grafts. Curr. Transpl. Rep. 2018, 5, 113–120. [Google Scholar] [CrossRef]
- Lindbergh, C.A. An apparatus for the culture of whole organs. J. Exp. Med. 1935, 62, 409. [Google Scholar] [CrossRef] [PubMed]
- Friend, P.J. Strategies in Organ Preservation—A New Golden Age. Transplantation 2020, 104, 1753–1755. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, A.; Oniscu, G. Challenges and advances in optimizing liver allografts from donation after circulatory death donors. J. Nat. Sci. Biol. Med. 2016, 7, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ceresa, C.D.L.; Nasralla, D.; Jassem, W. Normothermic Machine Preservation of the Liver: State of the Art. Curr. Transpl. Rep. 2018. [Google Scholar] [CrossRef]
- He, X.; Guo, Z.; Zhao, Q.; Ju, W.; Wang, D.; Wu, L.; Yang, L.; Ji, F.; Tang, Y.; Zhang, Z.; et al. The first case of ischemia-free organ transplantation in humans: A proof of concept. Am. J. Transpl. 2018, 18, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.A.; Guarrera, J.V. “resuscitation” of marginal liver allografts for transplantation with machine perfusion technology. J. Hepatol. 2014, 61, 418–431. [Google Scholar] [CrossRef]
- Mergental, H.; Laing, R.W.; Kirkham, A.J.; Perera, M.T.P.R.; Boteon, Y.L.; Attard, J.; Barton, D.; Curbishley, S.; Wilkhu, M.; Neil, D.A.H.; et al. Transplantation of discarded livers following viability testing with normothermic machine perfusion. Nat. Commun. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Nasralla, D.; Coussios, C.C.; Mergental, H.; Akhtar, M.Z.; Butler, A.J.; Ceresa, C.D.L.; Chiocchia, V.; Dutton, S.J.; Garcia-Valdecasas, J.C.; Heaton, N.; et al. A randomized trial of normothermic preservation in liver transplantation. Nature 2018, 557, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, R.; Van Den Berg, A.P.; Erdmann, J.I.; Heaton, N.; Van Hoek, B.; De Jonge, J. Study protocol for a multicenter randomized controlled trial to compare the efficacy of end-ischemic dual hypothermic oxygenated machine perfusion with static cold storage in preventing non-anastomotic biliary strictures after transplantation of liver gra. BMC Gastroenterol. 2019. [Google Scholar] [CrossRef]
- Eshmuminov, D.; Becker, D.; Bautista Borrego, L.; Hefti, M.; Schuler, M.J.; Hagedorn, C.; Muller, X.; Mueller, M.; Onder, C.; Graf, R.; et al. An integrated perfusion machine preserves injured human livers for 1 week. Nat. Biotechnol. 2020, 38, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Ciria, R.; Ayllon-Teran, M.D.; González-Rubio, S.; Gómez-Luque, I.; Ferrín, G.; Moreno, A.; Sanchez-Frias, M.; Alconchel, F.; Herrera, C.; Martin, V.; et al. Rescue of Discarded Grafts for Liver Transplantation by Ex Vivo Subnormothermic and Normothermic Oxygenated Machine Perfusion: First Experience in Spain. Transpl. Proc. 2019, 51, 20–24. [Google Scholar] [CrossRef]
- Mergental, H.; Stephenson, B.T.F.; Laing, R.W.; Kirkham, A.J.; Neil, D.A.H.; Wallace, L.L.; Boteon Yuri, L.; Widmer, J.e.a.n.n.e.t.t.e.; Bhogal Ricky, H.; Perera MThamara, P.R.; et al. Development of Clinical Criteria for Functional Assessment to Predict Primary Nonfunction of High-Risk Livers Using Normothermic Machine Perfusion. Liver Transpl. 2018, 24, 1453–1469. [Google Scholar] [CrossRef] [PubMed]
- Linares-Cervantes, I.; Echeverri, J.; Cleland, S.; Kaths, J.M.; Rosales, R.; Goto, T.; Kollmann, D.; Hamar, M.; Urbanellis, P.; Mazilescu, L.; et al. Predictor parameters of liver viability during porcine normothermic ex situ liver perfusion in a model of liver transplantation with marginal grafts. Am. J. Transpl. 2019, 19, 2991–3005. [Google Scholar] [CrossRef] [PubMed]
- Sutton, M.E.; Op Den Dries, S.; Karimian, N.; Weeder, P.D.; De Boer, M.T.; Wiersema-Buist, J.; Gouw, A.S.H.; Leuvenink, H.G.D.; Lisman, T.; Porte, R.J. Criteria for Viability Assessment of Discarded Human Donor Livers during Ex Vivo Normothermic Machine Perfusion. PLoS ONE 2014, 9, e0110642. [Google Scholar] [CrossRef]
- Raigani, S.; De Vries, R.J.; Carroll, C.; Chen, Y.W.; Chang, D.C.; Shroff, S.G.; Uygun, K.; Yeh, H. Viability testing of discarded livers with normothermic machine perfusion: Alleviating the organ shortage outweighs the cost. Clin. Transpl. 2020, 34, e14069. [Google Scholar] [CrossRef] [PubMed]
- Patrono, D.; Catalano, G.; Rizza, G.; Lavorato, N.; Berchialla, P.; Gambella, A.; Caropreso, P.; Mengozzi, G.; Romagnoli, R. Perfusate Analysis during Dual Hypothermic Oxygenated Machine Perfusion of Liver Grafts: Correlations with Donor Factors and Early Outcomes. Transplantation 2020, 104, 1929–1942. [Google Scholar] [CrossRef]
- Matton, A.P.M.; de Vries, Y.; Burlage, L.C.; van Rijn, R.; Fujiyoshi, M.; de Meijer, V.E.; de Boer, M.T.; de Kleine, R.H.J.; Verkade, H.J.; Gouw, A.S.H.; et al. Biliary Bicarbonate, pH, and Glucose Are Suitable Biomarkers of Biliary Viability During Ex Situ Normothermic Machine Perfusion of Human Donor Livers. Transplantation 2019, 103, 1405. [Google Scholar] [CrossRef]
- de Vries, Y.; Matton, A.; Nijsten, M.; Werner, M.; van den Berg, A.; de Boer, M.; Buis, C.I.; Fujiyoshi, M.; de Kleine, R.H.J.; van Leeuwen, O.B.; et al. Pretransplant Sequential Hypo- and Normothermic Machine Perfusion of Suboptimal Livers Donated after Circulatory Death Using a Hemoglobin-based Oxygen Carrier Perfusion Solution. Am. J. Transpl. 2018, 19, 1202–1211. [Google Scholar] [CrossRef]
- Ceresa, C.D.L.; Nasralla, D.; Watson, C.J.E.; Butler, A.J.; Coussios, C.C.; Crick, K.; Hodson, L.; Imber, C.; Jassem, W.; Knight, S.R.; et al. Transient Cold Storage Prior to Normothermic Liver Perfusion May Facilitate Adoption of a Novel Technology. Liver Transpl. 2019. [Google Scholar] [CrossRef]
- Bral, M.; Gala-Lopez, B.; Bigam, D.; Kneteman, N.; Malcolm, A.; Livingstone, S.; Andres, A.; Emamaullee, J.; Russell, L.; Coussios, C.; et al. Preliminary Single-Center Canadian Experience of Human Normothermic Ex Vivo Liver Perfusion: Results of a Clinical Trial. Am. J. Transpl. 2017, 17, 1071–1080. [Google Scholar] [CrossRef]
- Muller, X.; Schlegel, A.; Kron, P.; Eshmuminov, D.; Würdinger, M.; Meierhofer, D.; Clavien, P.; Dutkowski, P. Novel real time prediction of liver graft function during hypothermic oxygenated machine perfusion prior to liver transplantation. Ann. Surg. 2019, 270, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Moldenhauer, J. Use of a viability test method: Does it mean what you think? Am. Pharm. Rev. 2010, 13, 22. [Google Scholar]
- Attard, J.A.; Dunn, W.B.; Mergental, H.; Mirza, D.F.; Afford, S.C.; Perera, M.T.P.R. Systematic Review: Clinical Metabolomics to Forecast Outcomes in Liver Transplantation Surgery. Omi. A J. Integr. Biol. 2019, 23, 463–476. [Google Scholar] [CrossRef]
- Marcon, F.; Schlegel, A.; Bartlett, D.; Bishop, D.; Mergental, H.; Roberts, K.; Mirza, D.F.; Isaac, J.; Muiesan, P. Utilisation of declined liver grafts yields comparable transplant outcomes and previous decline should not be a deterrent to graft use. Transplantation 2018, 102, e211–e218. [Google Scholar] [CrossRef]
- Goldberg, D.S.; French, B.; Lewis, J.D.; Scott, F.I.; Mamtani, R.; Gilroy, R.; Halpern, S.D.; Abt, P.L. Liver transplant center variability in accepting organ offers and its impact on patient survival. J. Hepatol. 2016, 64, 843–851. [Google Scholar] [CrossRef]
- Schlegel, A.; Scalera, I.; Perera, M.T.P.R.; Kalisvaart, M.; Mergental, H.; Mirza, D.F.; Isaac, J.; Muiesan, P. Impact of donor age in donation after circulatory death liver transplantation: Is the cutoff “60” still of relevance? Liver Transpl. 2018, 24, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Croome, K.P.; Lee, D.D.; Keaveny, A.P.; Burcin Taner, C. Improving National Results in Liver Transplantation Using Grafts from Donation after Cardiac Death Donors. Transplantation 2016, 100, 2640–2647. [Google Scholar] [CrossRef]
- Kalisvaart, M.; Muiesan, P.; Schlegel, A. The UK-DCD-Risk-Score—practical and new guidance for allocation of a specific organ to a recipient? Expert Rev. Gastroenterol. Hepatol. 2019, 13, 771–783. [Google Scholar] [CrossRef] [PubMed]
- De Vries, Y.; Berendsen, T.A.; Fujiyoshi, M.; Van Den Berg, A.P.; Blokzijl, H.; De Boer, M.T. Transplantation of high-risk donor livers after resuscitation and viability assessment using a combined protocol of oxygenated hypothermic, rewarming and normothermic machine perfusion: Study protocol for a prospective, single-arm study (DHOPE-COR-NMP tri. BMJ Open 2019, 9, e028596. [Google Scholar] [CrossRef] [PubMed]
- Van Golen, R.F.; Van Gulik, T.M.; Heger, M. Mechanistic overview of reactive species-induced degradation of the endothelial glycocalyx during hepatic ischemia/reperfusion injury. Free Radic. Biol. Med. 2012, 52, 1382–1402. [Google Scholar] [CrossRef] [PubMed]
- Land, W.G. Emerging role of innate immunity in organ transplantation. Part I: Evolution of innate immunity and oxidative allograft injury. Transpl. Rev. 2012, 26, 60–72. [Google Scholar] [CrossRef]
- Chouchani, E.T.; Pell, V.R.; James, A.M.; Work, L.M.; Saeb-Parsy, K.; Frezza, C.; Krieg, T.; Murphy, M.P. A unifying mechanism for mitochondrial superoxide production during ischemia-reperfusion injury. Cell Metab. 2016, 23, 254–263. [Google Scholar] [CrossRef]
- Hofmann, J.; Otarashvili, G.; Meszaros, A.; Ebner, S.; Weissenbacher, A.; Cardini, B.; Oberhuber, R.; Resch, T.; Ofner, D.; Schneeberger, S.; et al. Restoring mitochondrial function while avoiding redox stress: The key to preventing ischemia/reperfusion injury in machine perfused liver grafts? Int. J. Mol. Sci. 2020, 21, 3132. [Google Scholar] [CrossRef]
- Mills, E.L.; Kelly, B.; O’neill, L.A.J. Mitochondria are the powerhouses of immunity. Nat. Immunol. 2017, 18, 488–498. [Google Scholar] [CrossRef] [PubMed]
- Stegemann, J.; Minor, T. Energy charge restoration, mitochondrial protection and reversal of preservation induced liver injury by hypothermic oxygenation prior to reperfusion. Cryobiology 2009, 58, 331–336. [Google Scholar] [CrossRef]
- Schlegel, A.; Muller, X.; Mueller, M.; Stepanova, A.; Kron, P.; de Rougemont, O.; Muiesan, P.; Clavien, P.; Galkin, A.; Meierhofer, D.; et al. Hypothermic oxygenated perfusion protects from mitochondrial injury before liver transplantation. EBioMedicine 2020, 60, 103014. [Google Scholar] [CrossRef] [PubMed]
- Westerkamp, A.; Karimian, N.; Matton, A.; Mahboub, P.; van Rijn, R.; Wiersema-Buist, J.; de Boer, M.T.; Leuvenink, H.G.D.; Gouw, A.S.H.; Lisman, T.; et al. Oxygenated Hypothermic Machine Perfusion After Static Cold Storage Improves Hepatobiliary Function of Extended Criteria Donor Livers. Transplantation 2016, 100, 825–835. [Google Scholar] [CrossRef]
- Murphy, M.P. How mitochondria produce reactive oxygen species. Biochem. J. 2009, 417, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chouchani, E.T.; Pell, V.R.; Gaude, E.; Aksentijević, D.; Sundier, S.Y.; Robb, E.L.; Logan, A.; Nadtochiy, S.M.; Ord, E.N.J.; Smith, A.C.; et al. Ischaemic accumulation of succinate controls reperfusion injury through mitochondrial ROS. Nature 2014, 515, 431–435. [Google Scholar] [CrossRef]
- Granger, D.N.; Kvietys, P.R. Reperfusion injury and reactive oxygen species: The evolution of a concept. Redox Biol. 2015, 6, 524–551. [Google Scholar] [CrossRef]
- Kron, P.; Schlegel, A.; Mancina, L.; Clavien, P.A.; Dutkowski, P. Hypothermic oxygenated perfusion (HOPE) for fatty liver grafts in rats and humans. J. Hepatol. 2018, 68, 82–91. [Google Scholar] [CrossRef]
- Kim, M.; Stepanova, A.; Niatsetskaya, Z.; Sosunov, S.; Arndt, S.; Murphy, M.P.; Galkin, A.; Ten, V.S. Attenuation of oxidative damage by targeting mitochondrial complex I in neonatal hypoxic-ischemic brain injury. Free Radic. Biol. Med. 2018. [CrossRef]
- Mills, E.L.; Kelly, B.; Logan, A.; Costa, A.S.H.; Varma, M.; Bryant, C.E.; Tourlomousis, P.; Dabritz, J.H.M.; Gottlieb, E.; Latorre, I.; et al. Succinate Dehydrogenase Supports Metabolic Repurposing of Mitochondria to Drive Inflammatory Macrophages. Cell 2016, 167, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Boudjema, K.; D’Alessandro, A.; Southard, J.H. Machine perfusion of the liver: Maintenance of mitochondrial function after 48-h preservation. Transpl. Proc. 1997, 29, 3452–3454. [Google Scholar] [CrossRef]
- Westerkamp, A.C.; Mahboub, P.; Meyer, S.L.; Hottenrott, M.; Ottens, P.J.; Wiersema-Buist, J.; Gouw, A.S.H.; Lisman, T.; Leuvenink, H.G.D.; Porte, R.J. End-ischemic machine perfusion reduces bile duct injury in donation after circulatory death rat donor livers independent of the machine perfusion temperature. Liver Transpl. 2015, 21, 1300–1311. [Google Scholar] [CrossRef]
- Van Rijn, R.; Karimian, N.; Matton, A.; Burlage, L.; Wetserkamp, A.; van den Berg, A.; de Kleine, R.H.J.; de Boer, M.T.; Lisman, T.; Porte, R.J. Dual hypothermic oxygenated machine perfusion in liver transplants donated after circulatory death. Br. J. Surg. 2017, 104, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Todd, J.L.; Palmer, S.M. Danger signals in regulating the immune response to solid organ transplantation. J. Clin. Investig. 2017, 127, 2464–2472. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Kron, P.; Graf, R.; Dutkowski, P.; Clavien, P.A. Warm vs. cold perfusion techniques to rescue rodent liver grafts. J. Hepatol. 2014, 61, 1267–1275. [Google Scholar] [CrossRef]
- Longatto Boteon, Y.; Schlegel, A.; Laing, R.; Attard, J.; Bhogal, R.; Wallace, L.; Reynolds, G.; Mirza, D.; Mergental, H.; Afford, S. Combination of hypothermic oxygenated machine perfusion followed by normothermic machine perfusion optimises the reconditioning of marginal human donor livers. HPB 2018, 20, S823. [Google Scholar] [CrossRef][Green Version]
- Brüggenwirth, I.M.A.; de Meijer, V.E.; Porte, R.J.; Martins, P.N. Viability criteria assessment during liver machine perfusion. Nat. Biotechnol. 2020, 38, 1260–1262. [Google Scholar] [CrossRef] [PubMed]
- Dröse, S.; Brandt, U.; Wittig, I. Mitochondrial respiratory chain complexes as sources and targets of thiol-based redox-regulation. Biochim. Biophys. Acta Proteins Proteomics 2014, 1844, 1344–1354. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, A.; Kahl, A.; Konrad, C.; Ten, V.; Starkov, A.S.; Galkin, A. Reverse electron transfer results in a loss of flavin from mitochondrial complex I: Potential mechanism for brain ischemia reperfusion injury. J. Cereb. Blood Flow Metab. 2017, 37, 3649–3658. [Google Scholar] [CrossRef]
- Iwasaki, M.; Takada, Y.; Hayashi, M.; Minamiguchi, S.; Haga, H.; Maetani, Y.; Fujii, K.; Kiuchi, T.; Tanaka, K. Noninvasive evaluation of graft steatosis in living donor liver transplantation. Transplantation 2004, 78, 1501–1505. [Google Scholar] [CrossRef]
- El-Badry, A.M.; Breitenstein, S.; Jochum, W.; Washington, K.; Paradis, V.; Rubbia-Brandt, L.; Puhan, M.A.; Slankamenac, K.; Graf, R.; Clavien, P. Assessment of hepatic steatosis by expert pathologists: The end of a gold standard. Ann. Surg. 2009, 250, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Ravikumar, R.; Jassem, W.; Mergental, H.; Heaton, N.; Mirza, D.; Perera, M.T.P.R.; Quaglia, A.; Holroyd, D.; Vogel, T.; Coussios, C.C.; et al. Liver Transplantation After Ex Vivo Normothermic Machine Preservation: A Phase 1 (First-in-Man) Clinical Trial. Am. J. Transpl. 2016, 16, 1779–1787. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.J.E.; Kosmoliaptsis, V.; Randle, L.V.; Gimson, A.E.; Brais, R.; Klinck, J.R.; Hamed, M.; Tsyben, A.; Butler, A.J. Normothermic perfusion in the assessment and preservation of declined livers before transplantation: Hyperoxia and vasoplegia-important lessons from the first 12 cases. Transplantation 2017, 101, 1084. [Google Scholar] [CrossRef] [PubMed]
- Reiling, J.; Butler, N.; Simpson, A.; Hodgkinson, P.; Campbell, C.; Lockwood, D.; Bridle, K.; Santrampurwala, N.; Britton, L.; Crawford, D.; et al. Assessment and Transplantation of Orphan Donor Livers: A Back-to-Base Approach to Normothermic Machine Perfusion. Liver Transpl. 2020, 26, 1618–1628. [Google Scholar] [CrossRef]
- Watson, C.; Kosmoliaptsis, V.; Pley, C.; Randle, L.; Fear, C.; Crick, K.; Gimson, A.E.; Allison, M.; Upponi, S.; Brais, R.; et al. Observations on the ex situ perfusion of livers for transplantation. Am. J. Transpl. 2018, 18, 2005–2020. [Google Scholar] [CrossRef]
- Matton, A.P.M.; Selten, J.W.; Roest, H.P.; de Jonge, J.; IJzermans, J.N.M.; de Meijer, V.E.; Porte, R.J.; van der Laan, L.J.W. Cell-free microRNAs as early predictors of graft viability during ex vivo normothermic machine perfusion of human donor livers. Clin. Transpl. 2020, 34, e13790. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Raoof, M.; Chen, Y.; Sumi, Y.; Sursal, T.; Junger, W.; Brohi, K.; Itagaki, K.; Hauser, C.J. Circulating mitochondrial DAMPs cause inflammatory responses to injury. Nature 2010, 464, 104–107. [Google Scholar] [CrossRef]
- Jara, M.; Malinowski, M.; Lüttgert, K.; Schott, E.; Neuhaus, P.; Stockmann, M. Prognostic value of enzymatic liver function for the estimation of short-term survival of liver transplant candidates: A prospective study with the LiMAx test. Transpl. Int. 2015, 28, 52–58. [Google Scholar] [CrossRef]
- Dutkowski, P.; Mueller, M.; Eshmuminov, D.; Bautista Borrego, L.; Becker, D.; Hefti, M.; Schuler, M.J.; von Rohr, P.R.; Clavien, P. Reply to: Lactate measurements in an integrated perfusion machine for human livers. Nat. Biotechnol. 2020, 38, 1263–1264. [Google Scholar] [CrossRef] [PubMed]
- Guarrera, J.V.; Henry, S.D.; Chen, S.W.C.; Brown, T.; Nachber, E.; Arrington, B.; Boykin, J.; Samstein, B.; Brown, R.S., Jr.; Emond, J.C.; et al. Hypothermic machine preservation attenuates ischemia/reperfusion markers after liver transplantation: Preliminary results. J. Surg. Res. 2011, 167, e365–e373. [Google Scholar] [CrossRef] [PubMed]
- Okaya, T.; Blanchard, J.; Schuster, R.; Kuboki, S.; Husted, T.; Caldwell, C.C.; Zingarelli, B.; Wong, H.; Solomkin, J.S.; Lentsch, A.B. Age-dependent responses to hepatic ischemia/reperfusion injury. Shock 2005, 24, 421–427. [Google Scholar] [CrossRef]
- Hosgood, S.A.; Patel, M.; Nicholson, M.L. The conditioning effect of ex vivo normothermic perfusion in an experimental kidney model. J. Surg. Res. 2013, 182, 153–160. [Google Scholar] [CrossRef]
- Thirunavayakalathil, M.; Varghese, C.; Bharathan, V.; Chandran, B.; Nair, K.; Mallick, S.; Mathew, J.S.; Amma, B.S.P.T.; Menon, R.N.; Gopalakrishnan, U.; et al. Double-blind placebo-controlled randomized trial of N-acetylcysteine infusion following live donor liver transplantation. Hepatol. Int. 2020, 1–8. [Google Scholar] [CrossRef]
- Lindell, S.L.; Klahn, S.L.; Piazza, T.M.; Mangino, M.J.; Torrealba, J.R.; Southard, J.H.; Carey, H.V. Natural resistance to liver cold ischemia-reperfusion injury associated with the hibernation phenotype. Am. J. Physiol. Gastrointest Liver Physiol. 2005, 288, G473–G480. [Google Scholar] [CrossRef]
- Jani, A.; Epperson, E.; Martin, J.; Pacic, A.; Ljubanovic, D.; Martin, S.L.; Edelstein, C.L. Renal protection from prolonged cold ischemia and warm reperfusion in hibernating squirrels. Transplantation 2011, 92, 1215–1221. [Google Scholar] [CrossRef]
- Abele, D. Toxic oxygen: The radical life-giver. Nature 2002, 420, 27. [Google Scholar] [CrossRef]
- Sumimoto, K.; Inagaki, K.; Yamada, K.; Kawasaki, T.; Dohi, K. Reliable indices for the determination of viability of grafted liver immediately after orthotopic transplantation: Bile flow rate and cellular adenosine triphosphate level. Transplantation 1988, 46, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Boteon, Y.L.; Afford, S.C. Machine perfusion of the liver: Which is the best technique to mitigate ischaemia-reperfusion injury? World J. Transpl. 2019. [CrossRef]
- Zhang, Z.; Ju, A.W.; Tang, Y.; Wang, L.; Zhu, C.; Gao, N.; Zhao, Q.; Huang, S.; Wang, D.; Yang, L.; et al. First preliminary experience with preservation of liver grafts from extended-criteria donors by normothermic machine perfusion in Asia. Ann. Transpl. 2020, 25, e921529. [Google Scholar] [CrossRef]
- Monbaliu, D.; Liu, Q.; Libbrecht, L.; De Vos, R.; Vekemans, K.; Debbaut, C.; Detry, O.; Roskams, T.; van Pelt, J.; Pirenne, J. Preserving the morphology and evaluating the quality of liver grafts by hypothermic machine perfusion: A proof-of-concept study using discarded human livers. Liver Transpl. 2012, 18, 1495–1507. [Google Scholar] [CrossRef]
- Fukumori, T.; Ohkohchi, N.; Tsukamoto, S.; Satomi, S. Why is fatty liver unsuitable for transplantation? Deterioration of mitochondrial ATP synthesis and sinusoidal structure during cold preservation of a liver with steatosis. Transpl. Proc. 1997, 29, 412–415. [Google Scholar] [CrossRef]
- Laing, R.W.; Scalera, I.; Isaac, J.; Mergental, H.; Mirza, D.F.; Hodson, J.; Wilkin, R.J.W.; Perera, M.T.P.R.; Muiesan, P. Liver transplantation using grafts from donors after circulatory death: A propensity-matched study from a single centre. Am. J. Transpl. 2016, 16, 1795–1804. [Google Scholar] [CrossRef]
- Cardini, B.; Oberhuber, R.; Fodor, M.; Hautz, T.; Margreiter, C.; Resch, T.; Scheidl, S.; Maglione, M.; Bosmuller, C.; Mair, H.; et al. Clinical Implementation of Prolonged Liver Preservation and Monitoring through Normothermic Machine Perfusion in Liver Transplantation. Transplantation 2020, 104, 1917–1928. [Google Scholar] [CrossRef] [PubMed]
- Dutkowski, P.; Southard, J.H.; Junginger, T. Liver metabolism during cold ischemic incubation in UW solution in the rat model. Langenbecks Arch. Chir. 1997, 382, 343–348. [Google Scholar] [PubMed]
- Mergental, H.; Perera, M.T.P.R.; Laing, R.W.; Muiesan, P.; Isaac, J.R.; Smith, A.; Stephenson, B.T.F.; Cilliers, H.; Neil, D.A.H.; Hubscher, S.G.; et al. Transplantation of Declined Liver Allografts Following Normothermic Ex-Situ Evaluation. Am. J. Transpl. 2016, 16, 3235–3245. [Google Scholar] [CrossRef]
- Van Leeuwen, O.B.; De Vries, Y.; Fujiyoshi, M.; Nijsten, M.W.N.; Ubbink, R.; Pelgrim, G.J.; Werner, M.J.M.; Reyntjens, K.M.E.M.; van den Berg, A.P.; de Boer, M.T.; et al. Transplantation of high-risk donor livers after ex situ resuscitation and assessment using combined hypo- A nd normothermic machine perfusion: A prospective clinical trial. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Schroeder, T.H.; Hansen, M. Effects of fresh versus old stored blood in the priming solution on whole blood lactate levels during paediatric cardiac surgery. Perfusion 2005, 20, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Op Den Dries, S.; Sutton, M.E.; Lisman, T.; Porte, R.J. Protection of bile ducts in liver transplantation: Looking beyond ischemia. Transplantation 2011, 92, 373–379. [Google Scholar] [CrossRef]
- Tabibian, J.H.; Masyuk, A.I.; Masyuk, T.V.; O’hara, S.P.; LaRusso, N.F. Physiology of cholangiocytes. Compr. Physiol. 2013, 3, 541–565. [Google Scholar] [CrossRef]
- Guzelian, P.; Boyer, J.L. Glucose reabsorption from bile. Evidence for a biliohepatic circulation. J. Clin. Investig. 1974, 53, 526–535. [Google Scholar] [CrossRef]
- Meurisse, N.; Vanden Bussche, S.; Jochmans, I.; Francois, J.; Desschans, B.; Laleman, W.; Van der Merwe, S.; van Steenbergen, W.; Cassiman, D.; Verslype, C.; et al. Outcomes of liver transplantations using donations after circulatory death: A single-center experience. Transpl. Proc. 2012, 44, 2868–2873. [Google Scholar] [CrossRef] [PubMed]
- DeOliveira, M.L.; Jassem, W.; Valente, R.; Khorsandi, S.E.; Santori, G.; Prachalias, A.; Srinivasan, P.; Rela, M.; Heaton, N. Biliary complications after liver transplantation using grafts from donors after cardiac death: Results from a matched control study in a single large volume center. Ann. Surg. 2011, 254, 716–722. [Google Scholar] [CrossRef]
- Kollmann, D.; Sapisochin, G.; Goldaracena, N.; Hansen, B.E.; Rajakumar, R.; Selzner, N.; Bhat, M.; McCluskey, S.; Cattral, M.S.; Greig, P.D.; et al. Expanding the donor pool: Donation after circulatory death and living liver donation do not compromise the results of liver transplantation. Liver Transpl. 2018, 24, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Karangwa, S.; Panayotova, G.; Dutkowski, P.; Porte, R.J.; Guarrera, J.V.; Schlegel, A. Hypothermic Machine Perfusion in Liver Transplantation. Int. J. Surg. 2020, 82, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Henry, S.D.; Nachber, E.; Tulipan, J.; Stone, J.; Bae, C.; Reznik, L.; Kato, T.; Samstein, B.; Emond, J.C.; Guarrera, J.V. Hypothermic machine preservation reduces molecular markers of ischemia/reperfusion injury in human liver transplantation. Am. J. Transpl. 2012. [CrossRef]
- Tulipan, J.E.; Stone, J.; Samstein, B.; Kato, T.; Emond, J.C.; Henry, S.D.; Guarrera, J.V. Molecular expression of acute phase mediators is attenuated by machine preservation in human liver transplantation: Preliminary analysis of effluent, serum, and liver biopsies. Surgery 2011, 150, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Kron, P.; De Oliveira, M.L.; Clavien, P.A.; Dutkowski, P. Reply to “Is single portal vein perfusion the best approach for machine preservation of liver grafts?”. J. Hepatol. 2016, 64, 1195–1196. [Google Scholar] [CrossRef][Green Version]
- Schlegel, A.; Kron, P.; De Oliveira, M.L.; Clavien, P.A.; Dutkowski, P. Is single portal vein approach sufficient for hypothermic machine perfusion of DCD liver grafts? J. Hepatol. 2016, 64, 239–241. [Google Scholar] [CrossRef]
- Mitchell, S.J.; Churchill, T.A.; Winslet, M.C.; Fuller, B.J. Effects of different cold preservation solutions on restoration of hepatic energy metabolism during cold reperfusion. Cryobiology 1996, 33, 413–422. [Google Scholar] [CrossRef]
- Dutkowski, P.; Furrer, K.; Tian, Y.; Graf, R.; Clavien, P.-A. Novel short-term hypothermic oxygenated perfusion (HOPE) system prevents injury in rat liver graft from non-heart beating donor. Ann. Surg. 2006, 244, 968–976. [Google Scholar] [CrossRef]
- Jain, S.; Lee, S.H.; Korneszczuk, K.; Culberson, C.R.; Southard, J.H.; Berthiaume, F.; Zhang, J.X.; Clemens, M.G.; Lee, C.Y. Improved preservation of warm ischemic livers by hypothermic machine perfusion with supplemented University of Wisconsin solution. J. Investig. Surg. 2008, 21, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Kahl, A.; Stepanova, A.; Konrad, C.; Anderson, C.; Manfredi, G.; Zhou, P.; Iadecola, C.; Galkin, A. Critical Role of Flavin and Glutathione in Complex I-Mediated Bioenergetic Failure in Brain Ischemia/Reperfusion Injury. Stroke 2018, 49, 1223–1231. [Google Scholar] [CrossRef]
- Stepanova, A.; Sosunov, S.; Niatsetskaya, Z.; Konrad, C.; Starkov, A.; Manfredi, G.; Wittig, I.; Ten, V.; Galkin, A. Redox-Dependent Loss of Flavin by Mitochondrial Complex I in Brain Ischemia/Reperfusion Injury. Antioxid. Redox Signal. 2019, 31, 608–622. [Google Scholar] [CrossRef]
- Holt, P.J.; Efremov, R.G.; Nakamaru-Ogiso, E.; Sazanov, L.A. Reversible FMN dissociation from Escherichia coli respiratory complex I. Biochim. Biophys. Acta Bioenerg. 2016, 1857, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Scholz, R.; Thurman, R.G.; Williamson, J.R.; Chance, B.; Bücher, T. Flavin and pyridine nucleotide oxidation-reduction changes in perfused rat liver. I. Anoxia and subcellular localization of fluorescent flavoproteins. J. Biol. Chem. 1969, 244, 2317–2324. [Google Scholar] [CrossRef]
- Panayotova, G.; Cutler, Q.; Paterno, F.; McCarty, M.; Bailey, A.; Dikdan, G.; Rosado, J.; Schlegel, A.; Dutkowski, P.; Shah, S.; et al. A Novel Biomarker to Predict Ischemia/Reperfusion Injury after Hypothermic Oxygenated Machine Preservation in Human Liver Transplants. ASTS 2019, 20, 78. [Google Scholar]
- Wang, L.; Thompson, E.; Bates, L.; Pither, T.L.; Hosgood, S.A.; Nicholson, M.L.; Watson, C.J.E.; Wilson, C.; Fisher, A.J.; Ali, S.; et al. Flavin mononucleotide as a biomarker of organ quality—A pilot study. Transpl. Direct 2020, 6. [Google Scholar] [CrossRef]
- Schlegel, A.; Rougemont, O.D.E.; Graf, R.; Clavien, P.A.; Dutkowski, P. Protective mechanisms of end-ischemic cold machine perfusion in DCD liver grafts. J. Hepatol. 2013, 58, 278–286. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Detection Method | Material | Parameters in Clinical Use | Time Needed for Assessment | Advantages | Disadvantages |
|---|---|---|---|---|---|
| Macroscopic assessment | Entire liver | Size, perfusion quality, steatosis, fibrosis, vessel quality, injuries | Minutes | Routine, rapid, non-invasive, cheap | No information on function, imprecise, assessor dependent |
| Ultrasound | Entire liver | Size, level of steatosis, lesions | 30 min | Easy, assessment of liver parenchyma, rapid, cheap | Assessor dependent, no information on function |
| Fibroscan | Entire Liver | Level of fibrosis | 30 min | Non-invasive, simple, rapid, reproducible, non-operator-dependent | No information on function, additional costs |
| Histology | Liver tissue | Level of macro and microsteatosis, fibrosis, inflammation | 1–2 h | Histological evidence of quality provides criteria to exclude organ transplantation (e.g., Fibrosis) | Invasive, variability in interpretation, biopsy covers only small part of organ, no information on function |
| Heamodyn-amics during Perfusion | Entire Liver | HA & PV perfusion flow (pressure) | continuous | Real-Time | Not specific for cell type |
| Blood gas analysis | Perfusate, Effluate, Bile | pO2, pCO2, Lactate, Na, K, pH, Glucose | 5–15 min | Non invasive, any type of perfusion, multiple parameters, indirect cholangiocyte assessment, different time points | Timing, different parameters, not specific for a certain cell type |
| Biochemical analysis | Perfusate, Effluate, Bile | AST, ALT, LDH, HCO3-, ALP | 5–15 min | Non-invasive, indirect cholangiocyte assessment, different time points | Not specific for a certain cell type, no functional assessment, no reliable prediction of outcomes after transplantation |
| Spectroscopy | Perfusate, Effluate | FMN, NADH | 5–15 min | Easy, quick, cheap, reliable prediction of graft function, covers entire organ, any type of machine perfusion | No discrimination between different cell types |
| Metabolomics/proteomics/genomics | Liver tisue, perfusate, effluate, bile | Various molecules from all cellular and sub-cellular compounds | Days/Weeks | Multiple parameters, can be performed in any material (tissue, perfusate, bile) | Requires long time, expensive, not specific for a certain cell type |
| Author & Year | Country | Number and Type of Livers | Timepoint’s and Modality | Viability Criteria and Threshold | Prospective Decision Making | Events below the Threshold (within Criteria) |
|---|---|---|---|---|---|---|
| Hypothermic Machine Perfusion (HOPE, D-HOPE) | ||||||
| Schlegel et al., 2020 | Switzer-land | 50 perfused and transplanted (32 DCD, 18 DBD, HOPE) | Serial measurements (perfusate and tissue) by mass spectometry and spectroscopy, at 15, 30, 60 and 90 min and end of HOPE | Perfusate, tissue and mitochondria: FMN at 30 min (<8800 A.U. or sharp incline), NADH (<10,000 A.U.) | Yes (n = 16/50) | 1 ITBL in retrospective, development cohort, none since prospective application of no PNF |
| Patrono et al., 2020 | Italy | 50 perfused and transplanted (ECD DBD, D-HOPE) | Every 30 min (3 h perfusion) | Perfusate Lactate, AST, ALT, LDH, glucose, and pH | No | No threshold applied, 3 months follow up |
| Muller et al., 2019 | Switzer-land | 100 perfused and transplanted (80 DCD, 20 DBD), 54 assessed, HOPE | Serial perfusate measurements by mass spectometry and spectroscopy, at 15, 30, and 60 min and end of HOPE | Perfusate FMN at 30 min (<8800 A.U.) | No | Threshold established retrospectively |
| Normothermic Machine Perfusion (NMP, NMP after COR) | ||||||
| Mergental et al., 2020 | UK | 31 perfused, 22 transplanted (12 DBD, 10 DCD) | Serial measurements every 30 min Assessment at 2.5 and 4 h | Within 4 h of NMP: lactate < 2.5 mmol/L and ≥2 of the following criteria: 1. Evidence of bile production; 2. pH > 7.30; 3. Metabolism of glucose; 4. HA flow > 150 mL/min and PV flow > 500 mL/min; 5. Homogenous perfusion | Yes | 2 anastomotic strictures 4 ITBL with retransplantation 6 months follow up |
| Cardini et al., 2020 | Austria | 34 perfused, 25 transplanted (21 DBD, 4 DCD) | Serial measurements every hour until 6 h NMP, afterwards every 2 h | 1. Rapid decrease and maintenance of lactate levels (first 2 h of NMP); 2. Bile output and biliary pH; 3. Maintenance of physiological perfusate pH without sodium bicarbonate; 4. Exceptionally high OR sharp incline of AST, ALT, LDH | Yes | No PNF 7 anastomotic strictures 3 bile leaks 1 left hemihepatectomy (ascending cholangitis after stricture) 20 months follow up |
| Zhang et al., 2020 | China | 4 perfused and transplanted (1 DBD, 3 DCD) | Serial measurements perfusate BGA every 10 min for the first 40 min, and then every 20 min. Bile collected every hour | Within 4 h of NMP: Perfusate lactate ≤ 2.5 mmol/L; 2. Bile production; 3. Perfusate pH ≥ 7.30; 4. Stable HA flow > 150 mL/min and PV flow > 500 mL/min | Yes | 1 anastomotic stricture 6 months follow up |
| Reiling et al., 2020 | Australia | 10 perfused, transplanted (5 DBD, 5 DCD) | Serial arterial perfusate samples Bile every hour Biopsies at the retrieval, at the end of SCS and at the end of NMP | Within 2 h (to 4 h) of NMP: 1. Lactate clearance to <2 mmol/L 2. Decreasing trend in perfusate glucose concentration by 4 h. 3. Physiological pH without the need for sodium bicarbonate. 4. Stable HA and PV flows. 5. Homogeneous graft perfusion with soft parenchyma consistency 6. Evidence of bile production | Yes | 1 Anastomotic leak 1 Anastomotic stricture 6 months follow up |
| Van Leeuwen et al., 2019 | The Netherlands | 16 perfused, 11 transplanted (DCD) * | BGA perfusate & Bile: Assessment at 2.5 h (Trial: D-HOPE-COR-NMP) | After 2.5 h of NMP: 1. Lactate clearance to ≤1.7 mmol/L; 2. Perfusate pH 7.35–7.45; 3. Bile production > 10 mL; 4. Biliary pH > 7.45 | Yes | 1 ITBL 3 Anastomotic strictures Median follow up 12 months |
| Matton et al., 2019 | The Netherlands | (1) 23 perfused to define markers; (2) 6 perfused, 4 transplanted (DCD) | BGA perfusate and Bile: Assessment at 2.5 h (Trial: D-HOPE-COR-NMP) | After 2.5 h of NMP: 1. Lactate clearance to ≤1.7 mmol/L; 2. Perfusate pH 7.35–7.45; 3. Bile production > 10 mL; 4. Biliary pH > 7.48 | Yes | No relevant graft-related complications Median follow up 8.3 months |
| Ceresa et al., 2019 | UK | 34 perfused, 31 transplanted (23 DBD, 8 DCD) | Perfusate BGA and Bio-chemistry at 15min and 1h of NMP, then every 4 h, and the end of NMP | Within 2.5 h and within 4 h: Lactate clearance and maintenance, glucose metabolism, pH maintenance, bile production, perfusate transaminase levels | Yes | 1 Anastomotic leak 1 Anastomotic stricture 12 months follow up |
| De Vries et al., 2019 | The Netherlands | 7 perfused, 5 transplanted (DCD) | BGA perfusate & Bile: Assessment at 2.5 h (Trial: D-HOPE-COR-NMP) | After 2.5 h of NMP: 1. Lactate clearance to ≤1.7 mmol/L; 2. Perfusate pH 7.35–7.45; 3. Bile production > 10 mL; 4. Biliary pH > 7.45 | Yes | No relevant graft-related complications Median follow up 6.5 months |
| Watson et al., 2018 | UK | 47 perfused, 22 transplanted (16 DCD, 6 DBD) # | BGA + Biochemistry: at 10 and 30 min, every 30 min thereafter | 1. Peak lactate fall ≥ 4.4 mmol/L/kg/h 2. ALT < 6000 iU/L at 2 h 3. Maximum bile pH > 7.5 4. Bile glucose ≤ 3 mmol/L or 10 mmol less than perfusate glucose 5. Maintain perfusate pH > 7.2 with ≤30 mmol bicarbonate supplementation 6. Falling glucose beyond 2 h OR perfusate glucose < 10 mmol/L with subsequent fall during challenge with 2.5 g glucose | Yes | 1 PNF 4 ITBL (3 with retransplantation or awaiting) Median follow up 20 months |
| Watson et al., 2017 | UK | 12 perfused and transplanted (9 DCD, 3 DBD) | At 10 and 30 min, every 30 min thereafter | 1. Lactate clearance, glucose and transaminase concentrations 2. Maintaining pH without supplemental bicarbonate | No | 1 PNF 3 ITBL Median follow up 20 months |
| Bral et al., 2017 | Canada | 9 perfused and transplanted 4 DCD, 6 DBD | At perfusion start and every 2 h | pH, Lactate, ALT, AST, bilirubin, perfusion vascular stability, hourly bile production | No | No PNF, one early HCV recurrence with graft loss, 6 months follow up |
| Mergental et al., 2016 | UK | 6 perfused 5 transplanted (4 DCD, 1 DBD) | Every 30 min and at 3 h | Within 3 h of NMP: Lactate clearance to <2.5 mmol/L or evidence of bile production combined with two of the following criteria: 1. Perfusate pH > 7.30 2. Hepatic artery flow > 150 mL/min and portal vein flow > 500 mL/min 3. Homogenous perfusion with soft parenchyma consistency | Yes | No relevant graft-related complications Median follow up 7months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panconesi, R.; Flores Carvalho, M.; Mueller, M.; Meierhofer, D.; Dutkowski, P.; Muiesan, P.; Schlegel, A. Viability Assessment in Liver Transplantation—What Is the Impact of Dynamic Organ Preservation? Biomedicines 2021, 9, 161. https://doi.org/10.3390/biomedicines9020161
Panconesi R, Flores Carvalho M, Mueller M, Meierhofer D, Dutkowski P, Muiesan P, Schlegel A. Viability Assessment in Liver Transplantation—What Is the Impact of Dynamic Organ Preservation? Biomedicines. 2021; 9(2):161. https://doi.org/10.3390/biomedicines9020161
Chicago/Turabian StylePanconesi, Rebecca, Mauricio Flores Carvalho, Matteo Mueller, David Meierhofer, Philipp Dutkowski, Paolo Muiesan, and Andrea Schlegel. 2021. "Viability Assessment in Liver Transplantation—What Is the Impact of Dynamic Organ Preservation?" Biomedicines 9, no. 2: 161. https://doi.org/10.3390/biomedicines9020161
APA StylePanconesi, R., Flores Carvalho, M., Mueller, M., Meierhofer, D., Dutkowski, P., Muiesan, P., & Schlegel, A. (2021). Viability Assessment in Liver Transplantation—What Is the Impact of Dynamic Organ Preservation? Biomedicines, 9(2), 161. https://doi.org/10.3390/biomedicines9020161