
Characteristics and Outcomes in Primary Aldosteronism Patients Harboring Glucocorticoid-Remediable Aldosteronism

 , , and
, , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Ethical Approval
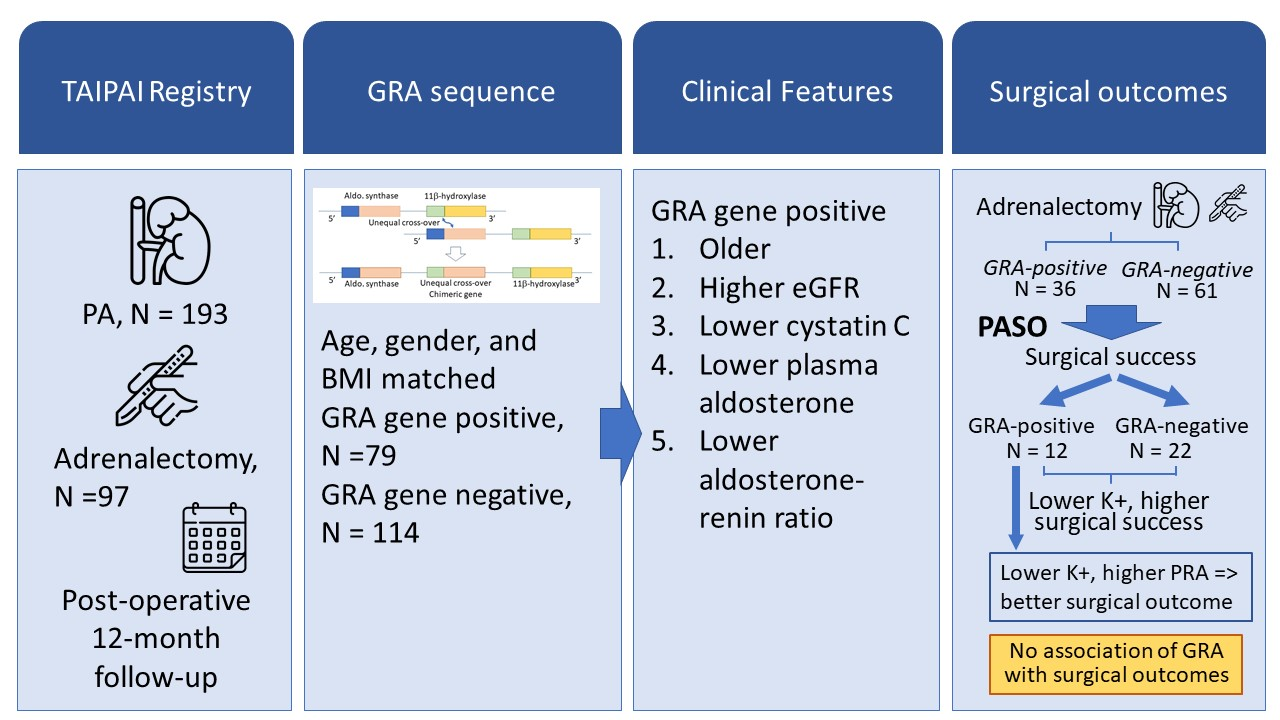
2.2. Study Design and Participants
2.3. Diagnosis of GRA Using Long-Range PCR
2.4. Outcomes of Interest
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of uPA Patients
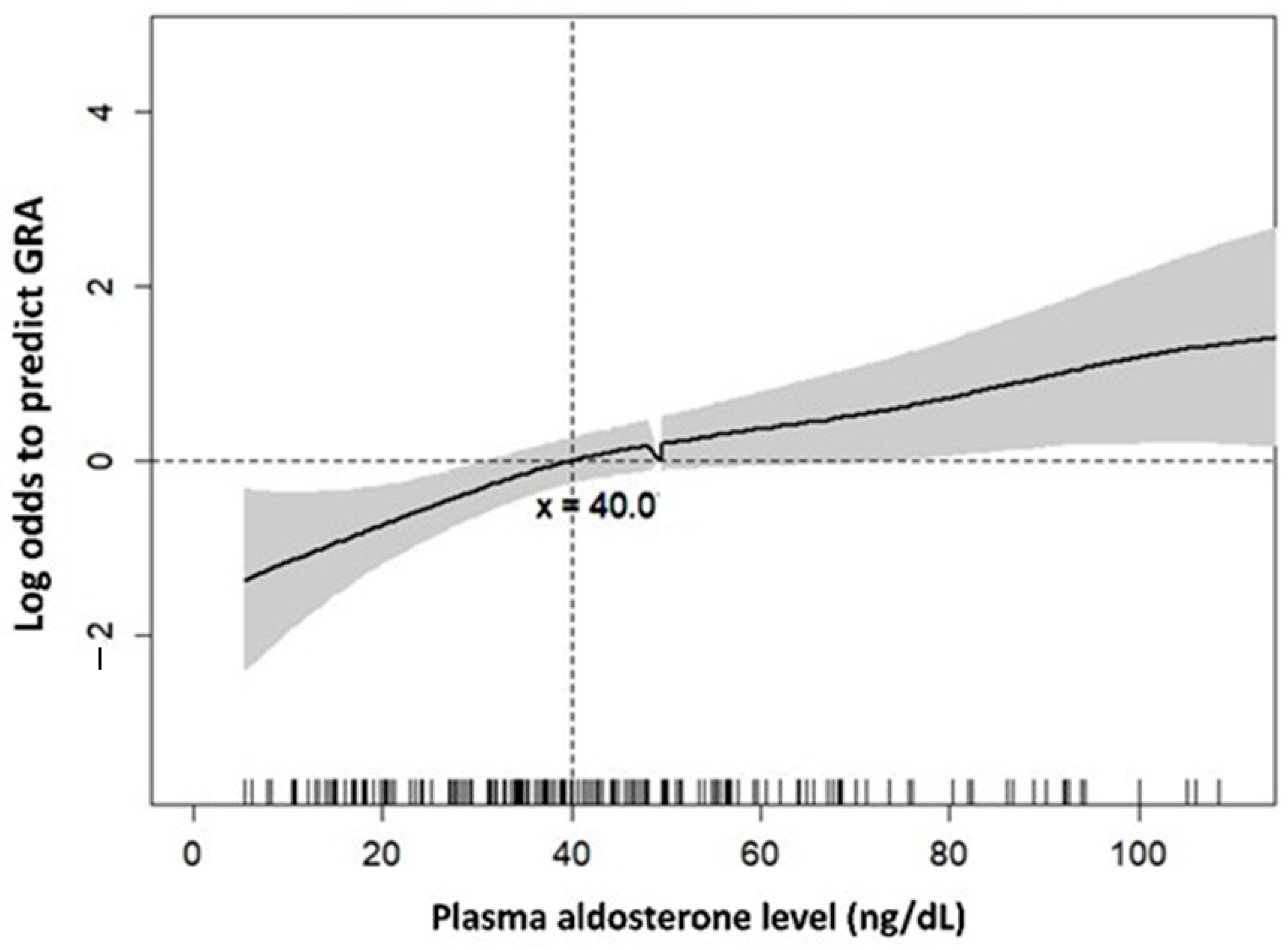
3.2. Factors Associated with GRA
3.3. Lower Potassium Associated with Better Surgical Outcomes in All PA Patients
3.4. Lower Potassium and High PRA Associated with Better Surgical Outcomes in GRA Patients
4. Discussion
4.1. PA Patients Harboring GRA and Clinical Outcome
4.2. Factors Related to Hypertension-Remission of GRA Patients after Adrenalectomy
4.3. Limitation and Strength of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martinez-Aguayo, A.; Fardella, C. Genetics of hypertensive syndrome. Horm. Res. Paediatr. 2009, 71, 253–259. [Google Scholar] [CrossRef]
- Prada, E.T.A.; Burrello, J.; Reincke, M.; Williams, T.A. Old and New Concepts in the Molecular Pathogenesis of Primary Aldosteronism. Hypertension 2017, 70, 875–881. [Google Scholar] [CrossRef]
- Lifton, R.P.; Dluhy, R.G.; Powers, M.; Rich, G.M.; Cook, S.; Ulick, S.; Lalouel, J.M. A chimaeric 11 beta-hydroxylase/aldosterone synthase gene causes glucocorticoid-remediable aldosteronism and human hypertension. Nature 1992, 355, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, D.J.; Ruse, J.L.; Laidlaw, J.C. Hypertension, increased aldosterone secretion and low plasma renin activity relieved by dexamethasone. Can. Med. Assoc. J. 1966, 95, 1109–1119. [Google Scholar]
- Aglony, M.; Martinez-Aguayo, A.; Carvajal, C.A.; Campino, C.; Garcia, H.; Bancalari, R.; Bolte, L.; Avalos, C.; Loureiro, C.; Trejo, P.; et al. Frequency of familial hyperaldosteronism type 1 in a hypertensive pediatric population: Clinical and biochemical presentation. Hypertension 2011, 57, 1117–1121. [Google Scholar] [CrossRef]
- Dluhy, R.G.; Anderson, B.; Harlin, B.; Ingelfinger, J.; Lifton, R. Glucocorticoid-remediable aldosteronism is associated with severe hypertension in early childhood. J. Pediatr. 2001, 138, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Rich, G.M.; Ulick, S.; Cook, S.; Wang, J.Z.; Lifton, R.P.; Dluhy, R.G. Glucocorticoid-remediable aldosteronism in a large kindred: Clinical spectrum and diagnosis using a characteristic biochemical phenotype. Ann. Intern. Med. 1992, 116, 813–820. [Google Scholar] [CrossRef]
- Litchfield, W.R.; Anderson, B.F.; Weiss, R.J.; Lifton, R.P.; Dluhy, R.G. Intracranial aneurysm and hemorrhagic stroke in glucocorticoid-remediable aldosteronism. Hypertension 1998, 31, 445–450. [Google Scholar] [CrossRef]
- Wyckoff, J.A.; Seely, E.W.; Hurwitz, S.; Anderson, B.F.; Lifton, R.P.; Dluhy, R.G. Glucocorticoid-remediable aldosteronism and pregnancy. Hypertension 2000, 35, 668–672. [Google Scholar] [CrossRef][Green Version]
- Stowasser, M.; Bachmann, A.W.; Huggard, P.R.; Rossetti, T.R.; Gordon, R.D. Severity of hypertension in familial hyperaldosteronism type I: Relationship to gender and degree of biochemical disturbance. J. Clin. Endocrinol. Metab. 2000, 85, 2160–2166. [Google Scholar] [CrossRef] [PubMed]
- Dluhy, R.G.; Lifton, R.P. Glucocorticoid-remediable aldosteronism. J. Clin. Endocrinol. Metab. 1999, 84, 4341–4344. [Google Scholar] [CrossRef]
- Wu, V.C.; Chueh, J.S.; Hsieh, M.Y.; Hu, Y.H.; Huang, K.H.; Lin, Y.H.; Yang, S.Y.; Chu, T.S.; Kuo, C.F. Familial Aggregation and Heritability of Aldosteronism with Cardiovascular Events. J. Clin. Endocrinol. Metab. 2020, 105, e2176–e2184. [Google Scholar] [CrossRef]
- Funder, J.W.; Carey, R.M.; Fardella, C.; Gomez-Sanchez, C.E.; Mantero, F.; Stowasser, M.; Young, W.F., Jr.; Montori, V.M.; Endocrine, S. Case detection, diagnosis, and treatment of patients with primary aldosteronism: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2008, 93, 3266–3281. [Google Scholar] [CrossRef]
- MacConnachie, A.A.; Kelly, K.F.; McNamara, A.; Loughlin, S.; Gates, L.J.; Inglis, G.C.; Jamieson, A.; Connell, J.M.; Haites, N.E. Rapid diagnosis and identification of cross-over sites in patients with glucocorticoid remediable aldosteronism. J. Clin. Endocrinol. Metab. 1998, 83, 4328–4331. [Google Scholar] [CrossRef]
- Carvajal, C.A.; Stehr, C.B.; Gonzalez, P.A.; Riquelme, E.M.; Montero, T.; Santos, M.J.; Kalergis, A.M.; Fardella, C.E. A de novo unequal cross-over mutation between CYP11B1 and CYP11B2 genes causes familial hyperaldosteronism type I. J. Endocrinol. Investig. 2011, 34, 140–144. [Google Scholar] [CrossRef]
- Lin, Y.F.; Peng, K.Y.; Chang, C.H.; Hu, Y.H.; Wu, V.C.; Chueh, J.S.; Wu, K.D. Adrenalectomy Completely Cured Hypertension in Patients With Familial Hyperaldosteronism Type I Who Had Somatic KCNJ5 Mutation. J. Clin. Endocrinol. Metab. 2019, 104, 5462–5466. [Google Scholar] [CrossRef]
- Peng, K.Y.; Liao, H.W.; Chan, C.K.; Lin, W.C.; Yang, S.Y.; Tsai, Y.C.; Huang, K.H.; Lin, Y.H.; Chueh, J.S.; Wu, V.C. Presence of Subclinical Hypercortisolism in Clinical Aldosterone-Producing Adenomas Predicts Lower Clinical Success. Hypertension 2020, 76, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.A.; Lenders, J.W.M.; Mulatero, P.; Burrello, J.; Rottenkolber, M.; Adolf, C.; Satoh, F.; Amar, L.; Quinkler, M.; Deinum, J.; et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: An international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017, 5, 689–699. [Google Scholar] [CrossRef]
- Wu, V.C.; Yang, S.Y.; Lin, J.W.; Cheng, B.W.; Kuo, C.C.; Tsai, C.T.; Chu, T.S.; Huang, K.H.; Wang, S.M.; Lin, Y.H.; et al. Kidney impairment in primary aldosteronism. Clin. Chim. Acta 2011, 412, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.K.; Yang, W.S.; Lin, Y.H.; Huang, K.H.; Lu, C.C.; Hu, Y.H.; Wu, V.C.; Chueh, J.S.; Chu, T.S.; Chen, Y.M. Arterial Stiffness Is Associated with Clinical Outcome and Cardiorenal Injury in Lateralized Primary Aldosteronism. J. Clin.Endocrinol. Metab. 2020, 105, e3950–e3960. [Google Scholar] [CrossRef]
- Morisaki, M.; Kurihara, I.; Itoh, H.; Naruse, M.; Takeda, Y.; Katabami, T.; Ichijo, T.; Wada, N.; Yoshimoto, T.; Ogawa, Y.; et al. Predictors of Clinical Success After Surgery for Primary Aldosteronism in the Japanese Nationwide Cohort. J. Endocr. Soc. 2019, 3, 2012–2022. [Google Scholar] [CrossRef]
- Vorselaars, W.; Nell, S.; Postma, E.L.; Zarnegar, R.; Drake, F.T.; Duh, Q.Y.; Talutis, S.D.; McAneny, D.B.; McManus, C.; Lee, J.A.; et al. Clinical Outcomes After Unilateral Adrenalectomy for Primary Aldosteronism. JAMA Surg. 2019, 154, e185842. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.P. Primary aldosteronism: A needle in a haystack or a yellow cab on Fifth Avenue? Curr. Hypertens. Rep. 2004, 6, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.P.; Pessina, A.C.; Heagerty, A.M. Primary aldosteronism: An update on screening, diagnosis and treatment. J. Hypertens. 2008, 26, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Ogata, H.; Yamazaki, Y.; Tezuka, Y.; Gao, X.; Omata, K.; Ono, Y.; Kawasaki, Y.; Tanaka, T.; Nagano, H.; Wada, N.; et al. Renal Injuries in Primary Aldosteronism: Quantitative Histopathological Analysis of 19 Patients With Primary Adosteronism. Hypertension 2021, 78, 411–421. [Google Scholar] [CrossRef]
- Chan, Y.H.B.; Loh, L.M.; Foo, R.S.; Loh, W.J.; Lim, D.S.T.; Zhang, M.; Sultana, R.; Tan, Y.K.; Ng, K.S.; Tay, D.; et al. Re-evaluating absent clinical success after adrenalectomy in unilateral primary aldosteronism. Surgery 2021, 170, 1389–1396. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Sun, C.Y.; Lu, C.C.; Chang, Y.S.; Pan, H.C.; Lin, Y.H.; Wu, V.C.; Chueh, J.S. Urinary sodium potassium ratio is associated with clinical success after adrenalectomy in patients with unilateral primary aldosteronism. Ther. Adv.Chronic Dis. 2021, 12, 2040622321990274. [Google Scholar] [CrossRef]
- Neal, B.; Wu, Y.; Feng, X.; Zhang, R.; Zhang, Y.; Shi, J.; Zhang, J.; Tian, M.; Huang, L.; Li, Z.; et al. Effect of Salt Substitution on Cardiovascular Events and Death. N. Engl. J. Med. 2021, 385, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Vallotton, M.B.; Rossier, M.F.; Capponi, A.M. Potassium-angiotensin interplay in the regulation of aldosterone biosynthesis. Clin. Endocrinol. 1995, 42, 111–119. [Google Scholar] [CrossRef]
- Sawka, A.M.; Young, W.F.; Thompson, G.B.; Grant, C.S.; Farley, D.R.; Leibson, C.; van Heerden, J.A. Primary aldosteronism: Factors associated with normalization of blood pressure after surgery. Ann. Intern. Med. 2001, 135, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Letavernier, E.; Peyrard, S.; Amar, L.; Zinzindohoue, F.; Fiquet, B.; Plouin, P.F. Blood pressure outcome of adrenalectomy in patients with primary hyperaldosteronism with or without unilateral adenoma. J. Hypertens. 2008, 26, 1816–1823. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | GRA-Positive (N = 79) | GRA-Negative (N = 114) | p Value |
|---|---|---|---|
| Women/men (%) | 39/40 (49.4%/50.6%) | 65/49 (57.0%/43.0%) | 0.298 |
| Age (years) | 51.2 ± 13.8 | 48.1 ± 13.0 | 0.081 |
| Body weight (kg) | 72.5 ± 17.0 | 71.0 ± 13.7 | 0.442 |
| BMI (kg/m2) | 26.5 ± 4.4 | 26.1 ± 4.2 | 0.448 |
| eGFR (MDRD) (ml/min/1.73 m2) | 92.6 ± 36.7 | 88.7 ± 29.8 | 0.338 |
| Na (mmol/L) | 140.5 ± 2.9 | 140.0 ± 3.6 | 0.450 |
| K (mmol/L) | 3.82 ± 0.64 | 3.79 ± 0.62 | 0.399 |
| Cholesterol (mg/dL) | 180.4 ± 38.8 | 183.9 ± 34.5 | 0.562 |
| Triglyceride (mg/dL) | 136.7 ± 76.9 | 133.9 ± 81.1 | 0.820 |
| LDL-C (mg/dL) | 111.6 ± 29.7 | 108.7 ± 27.4 | 0.542 |
| TTKG | 5.43 ± 2.1 | 5.49 ± 2.7 | 0.880 |
| pH | 7.41 ± 0.04 | 7.40 ± 0.03 | 0.226 |
| HCO3 | 26.3 ± 3.1 | 25.8 ± 3.6 | 0.601 |
| Cortisol (μg/dL) | 11.8 ± 6.0 | 11.4 ± 4.7 | 0.740 |
| SBP (mmHg) | 156 ± 20 | 152 ± 22 | 0.215 |
| DBP (mmHg) | 94 ± 15 | 92 ± 15 | 0.591 |
| Intact PTH (pg/mL) | 67.01 ± 34.23 | 61.48 ± 31.54 | 0.122 |
| Cystatin C (mg/L) | 0.75 ± 0.13 | 0.85 ± 0.31 | 0.112 |
| CRP (mg/dL) | 0.27 ± 0.47 | 0.42 ± 0.92 | 0.329 |
| PAC (ng/dL) | 41.8 ± 30.9 | 55.1 ± 37.6 | 0.008 ** |
| PRA (ng/mL per hour) | 0.86 ± 1.46 | 0.80 ± 1.32 | 0.469 |
| ARR (ng/dL per ng/mL-h) | 364.6 ± 720.4 | 872.0 ± 1968.0 | 0.013 * |
| Urine Aldo | 19.1 ± 14.7 | 15.8 ± 18.4 | 0.271 |
| ACR (μg/mg) | 0.13 ± 0.43 | 0.19 ± 0.92 | 0.622 |
| Diabetes | 15 (19.0%) | 18 (15.8%) | 0.552 |
| MACE | 12 (15.2%) | 8 (7.0%) | 0.119 |
| Number of Anti-HTN drugs | 3 (0–8) | 3 (0–8) | 0.900 |
| Family member of HTN | 2 (1–3) | 1 (1–3) | 0.831 |
| Variables | Univariable | Multivariable | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Age (years) | 1.02 (1.00–1.04) | 0.075 | 1.02 (1.00–1.04) | 0.005 ** |
| eGFR (MDRD) (mL/min/1.73 m2) | 1.01 (0.98–1.02) | 0.347 | 1.01 (1.00–1.02) | 0.001 ** |
| Number of Anti-HTN drugs | 1.02 (0.87–1.20) | 0.822 | ||
| SBP (mmHg) | 0.99 (0.98–1.01) | 0.221 | 0.99 (0.97–1.00) | 0.079 |
| Intact PTH (pg/mL) | 0.99 (0.97–1.01) | 0.138 | ||
| Cystatin-C (mg/L) | 0.17 (0.02–1.71) | 0.133 | ||
| LnAldo | 0.14 (0.05–0.45) | 0.001 ** | 0.16 (0.05–0.51) | 0.006 ** |
| PRA | 1.03 (0.84–1.27) | 0.572 | ||
| ARR | 1.00 (0.98–1.01) | 0.049 * | ||
| ACR | 0.89 (0.54–1.47) | 0.654 | ||
| MACE | 2.05 (0.85–4.90) | 0.109 | ||
| Variable | Estimate | SE. | p Value | OR | Lower CI | Upper CI |
|---|---|---|---|---|---|---|
| Age (years) | −0.017 | 0.025 | 0.485 | 0.983 | 0.936 | 1.032 |
| Cr | 0.521 | 0.577 | 0.366 | 1.684 | 0.544 | 5.213 |
| SBP | 0.022 | 0.021 | 0.291 | 1.022 | 0.982 | 1.064 |
| DBP | −0.024 | 0.027 | 0.381 | 0.976 | 0.925 | 1.030 |
| GRA | −0.264 | 0.562 | 0.638 | 0.768 | 0.255 | 2.308 |
| Gender | −0.579 | 0.552 | 0.294 | 0.560 | 0.190 | 1.654 |
| K | −1.257 | 0.472 | 0.008 | 0.285 | 0.113 | 0.717 |
| PRA | 0.541 | 0.298 | 0.069 | 1.718 | 0.959 | 3.077 |
| PAC | −0.008 | 0.009 | 0.394 | 0.992 | 0.975 | 1.010 |
| Variable | Estimate | SE. | p Value | OR | Lower CI | Upper CI |
|---|---|---|---|---|---|---|
| Age (years) | 1.169 | 1.178 | 0.321 | 3.217 | 0.320 | 32.341 |
| Cr | 0.218 | 0.884 | 0.806 | 1.243 | 0.220 | 7.031 |
| SBP | −1.124 | 1.309 | 0.390 | 0.325 | 0.025 | 4.224 |
| DBP | 0.009 | 0.042 | 0.828 | 1.009 | 0.930 | 1.095 |
| Gender | −0.592 | 1.070 | 0.580 | 0.553 | 0.068 | 4.503 |
| K | −2.019 | 1.018 | 0.048 | 0.133 | 0.018 | 0.978 |
| PRA | 2.455 | 1.227 | 0.045 | 11.645 | 1.052 | 128.940 |
| PAC | −0.016 | 0.021 | 0.457 | 0.984 | 0.945 | 1.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, C.-Y.; Liao, H.-W.; Peng, K.-Y.; Chen, T.-H.; Lin, Y.-H.; Chueh, J.S.; Wu, V.-C.; on behalf of the TAIPAI Study Group. Characteristics and Outcomes in Primary Aldosteronism Patients Harboring Glucocorticoid-Remediable Aldosteronism. Biomedicines 2021, 9, 1816. https://doi.org/10.3390/biomedicines9121816
Cheng C-Y, Liao H-W, Peng K-Y, Chen T-H, Lin Y-H, Chueh JS, Wu V-C, on behalf of the TAIPAI Study Group. Characteristics and Outcomes in Primary Aldosteronism Patients Harboring Glucocorticoid-Remediable Aldosteronism. Biomedicines. 2021; 9(12):1816. https://doi.org/10.3390/biomedicines9121816
Chicago/Turabian StyleCheng, Chung-Yi, Hung-Wei Liao, Kang-Yung Peng, Tso-Hsiao Chen, Yen-Hung Lin, Jeff S. Chueh, Vin-Cent Wu, and on behalf of the TAIPAI Study Group. 2021. "Characteristics and Outcomes in Primary Aldosteronism Patients Harboring Glucocorticoid-Remediable Aldosteronism" Biomedicines 9, no. 12: 1816. https://doi.org/10.3390/biomedicines9121816
APA StyleCheng, C.-Y., Liao, H.-W., Peng, K.-Y., Chen, T.-H., Lin, Y.-H., Chueh, J. S., Wu, V.-C., & on behalf of the TAIPAI Study Group. (2021). Characteristics and Outcomes in Primary Aldosteronism Patients Harboring Glucocorticoid-Remediable Aldosteronism. Biomedicines, 9(12), 1816. https://doi.org/10.3390/biomedicines9121816