
Analysis of KRAS Mutation Subtype in Tissue DNA and Cell-Free DNA Using Droplet Digital PCR and the Function of Cell-Free DNA as a Recurrence Predictive Marker in Pancreatic Cancer

 , ,
, ,  , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical Information
2.3. DNA Preparation and ddPCR Assay
2.4. Statistical Analysis
3. Results
3.1. Clinicopathological Features of Enrolled Patients
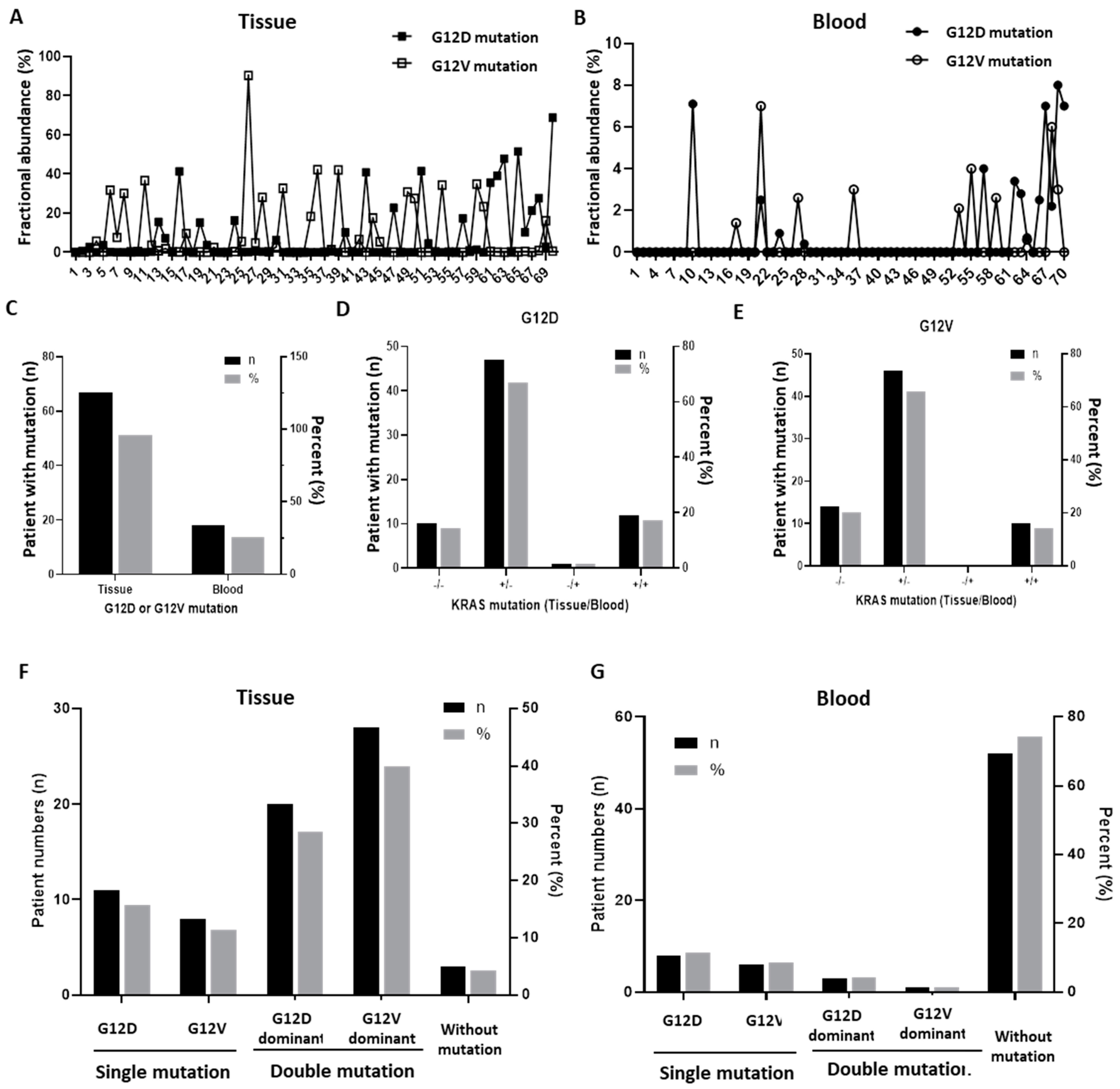
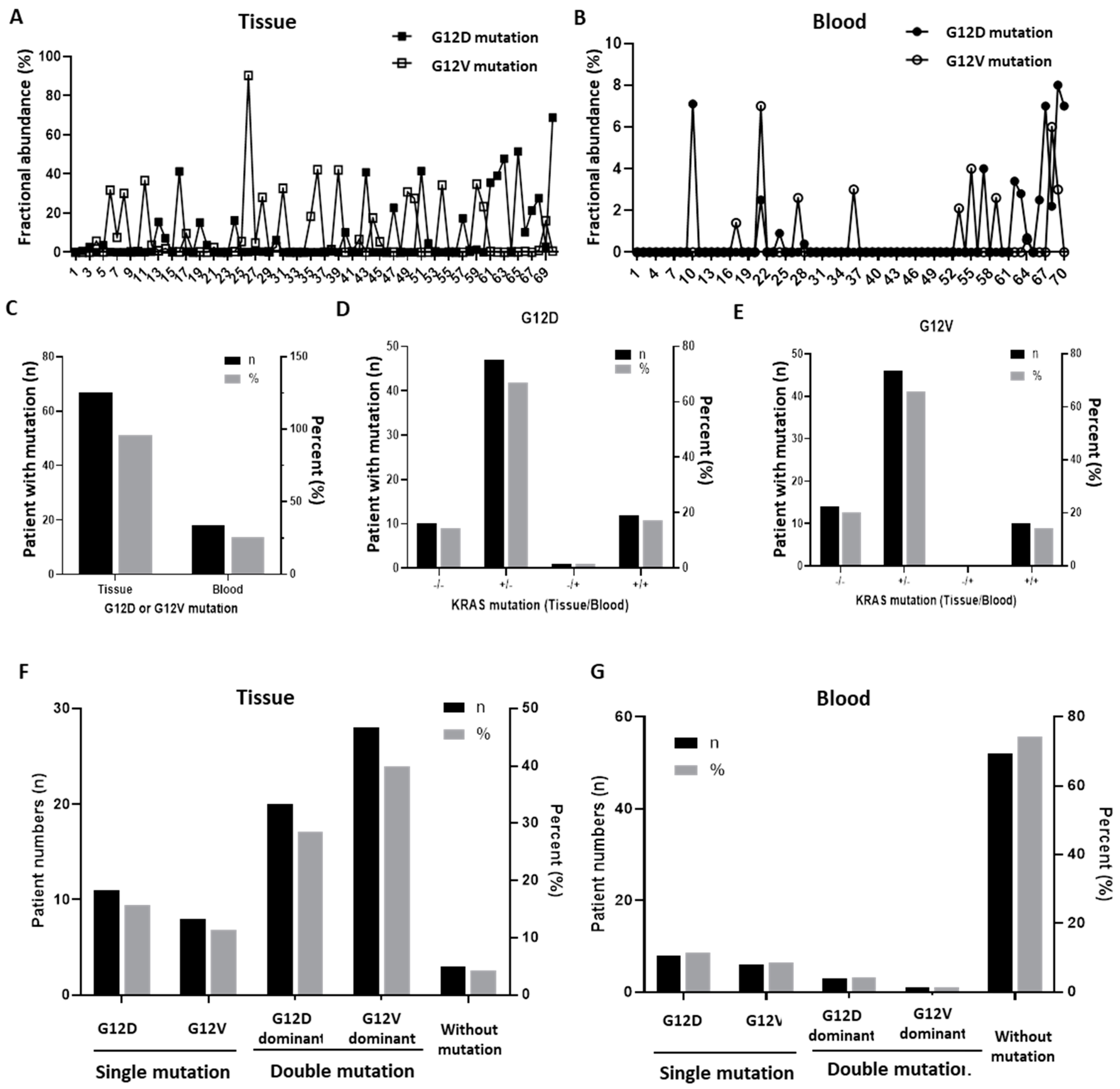
3.2. Presence of KRAS Mutation in Paired Tissue DNA of Tumor and cfDNA in Blood
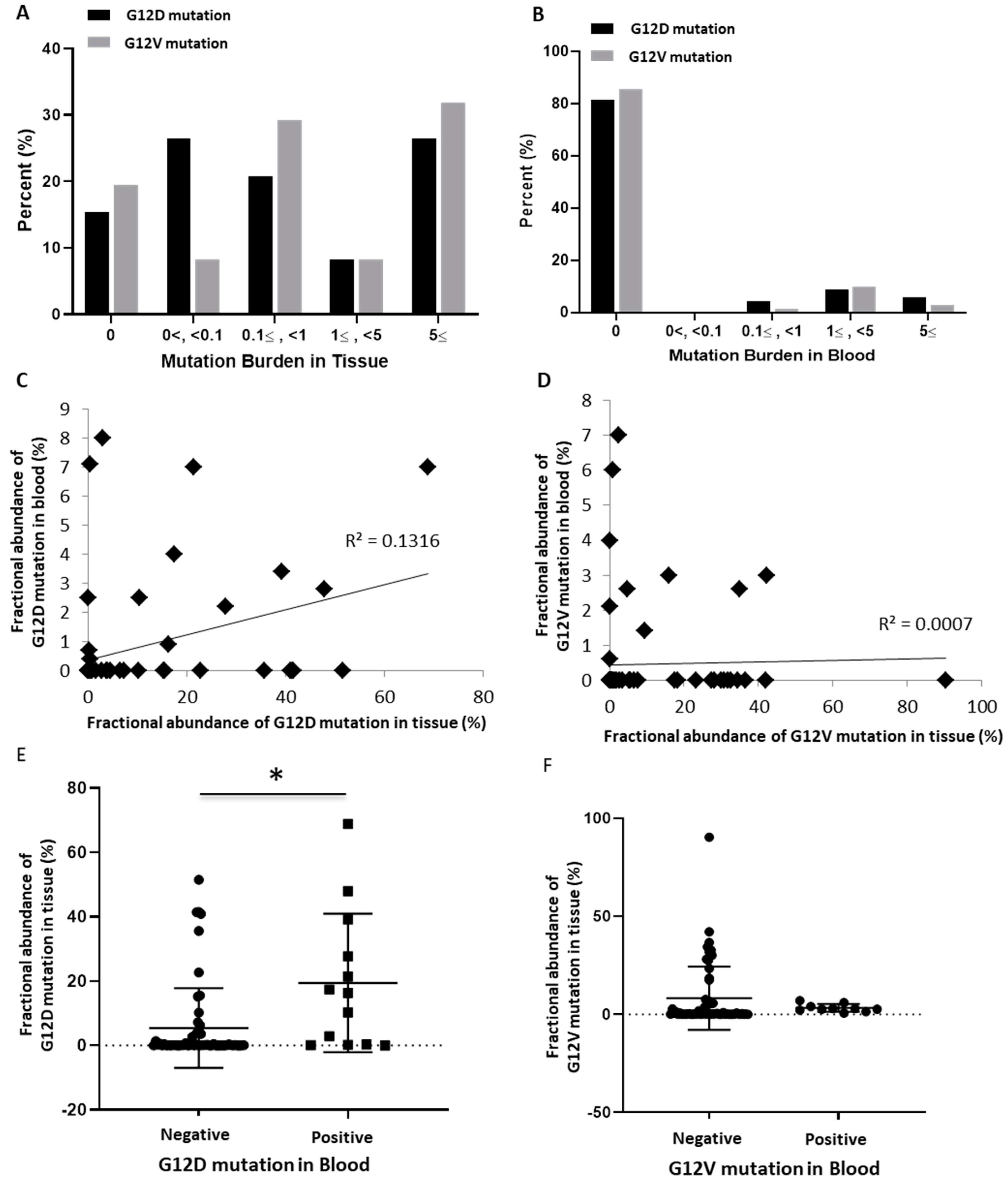
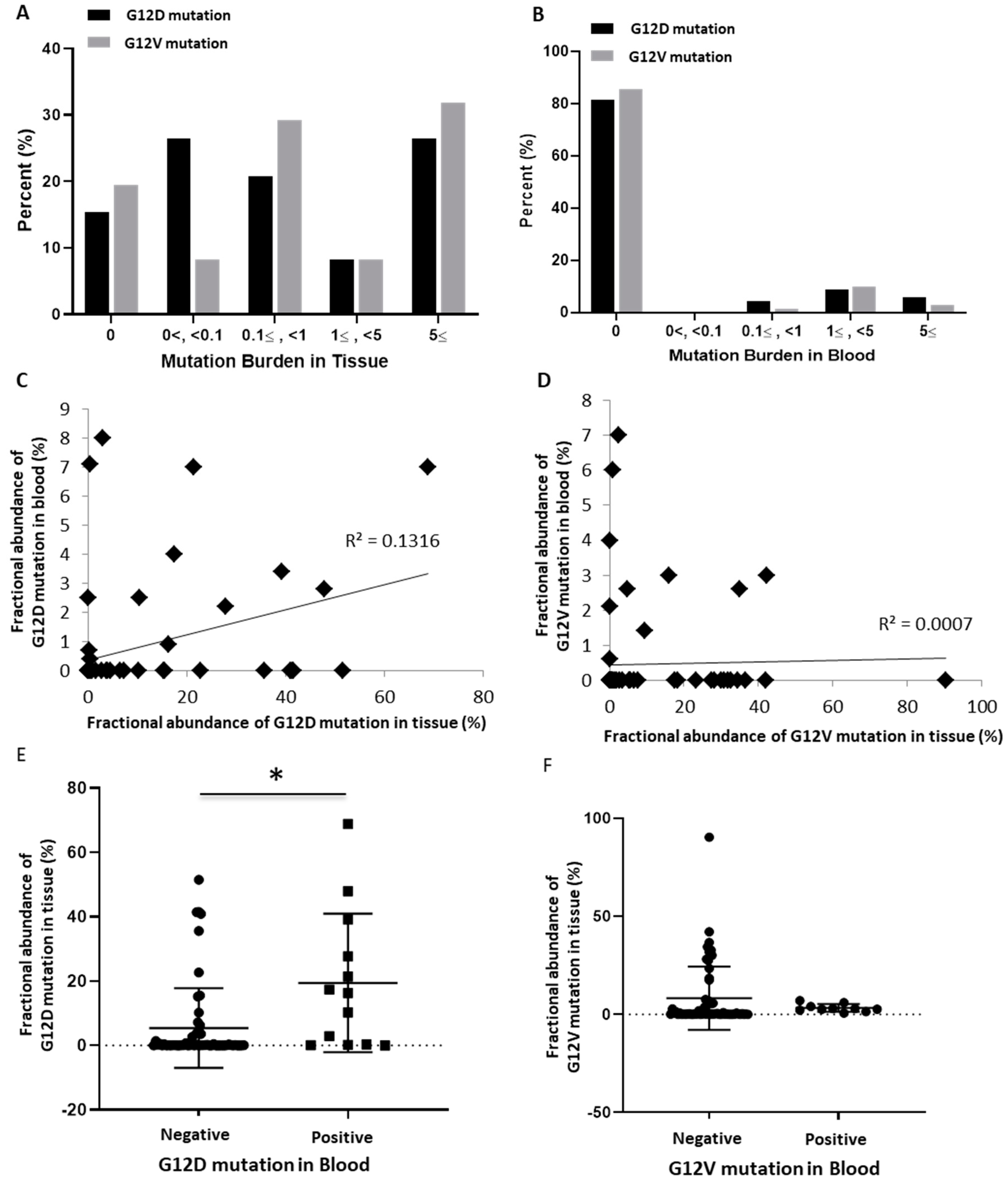
3.3. Correlation of KRAS Mutation Burden with Clinicopathological Status
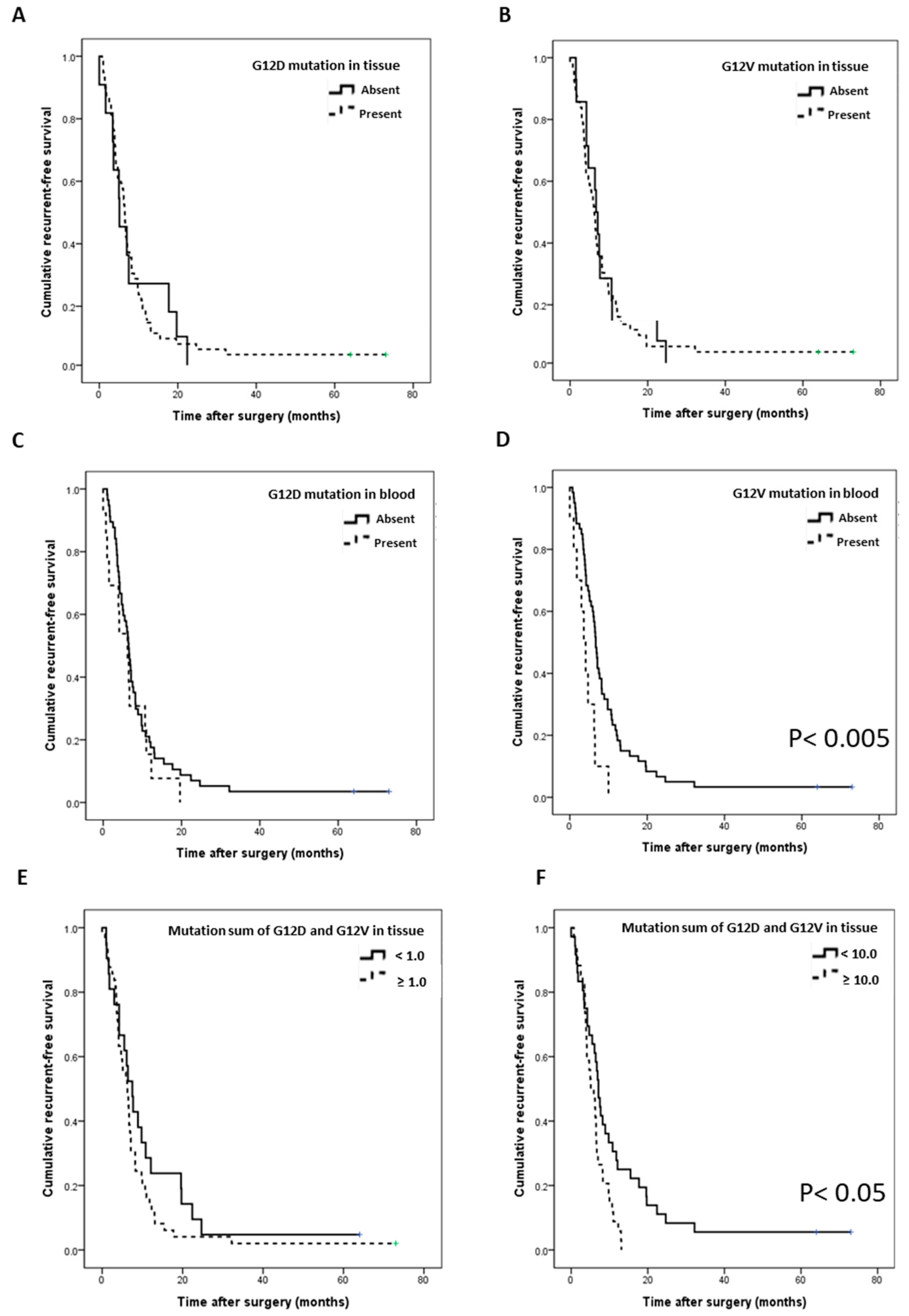
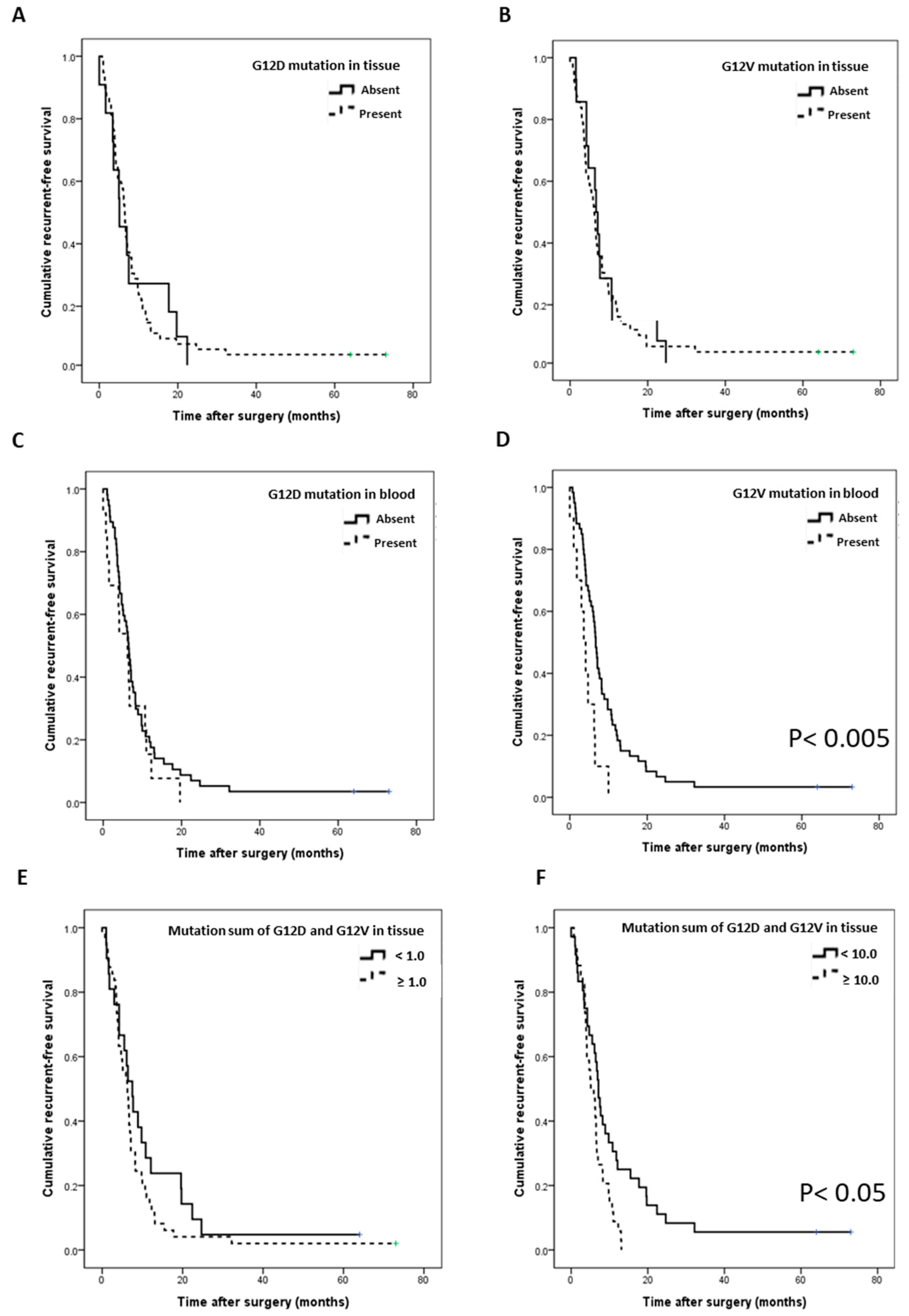
3.4. Survival Analysis According to the Site and Subtype of KRAS Mutation
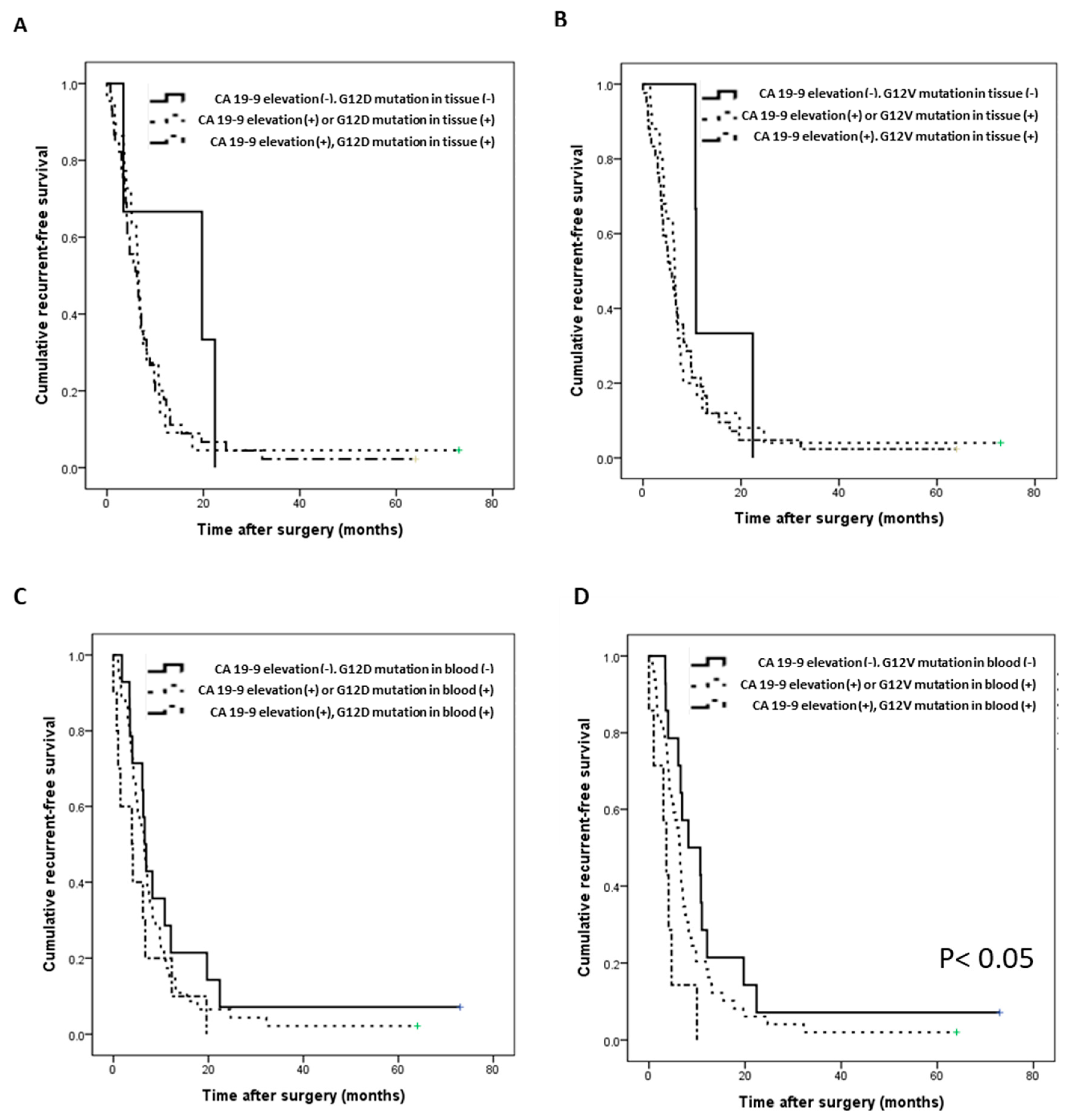
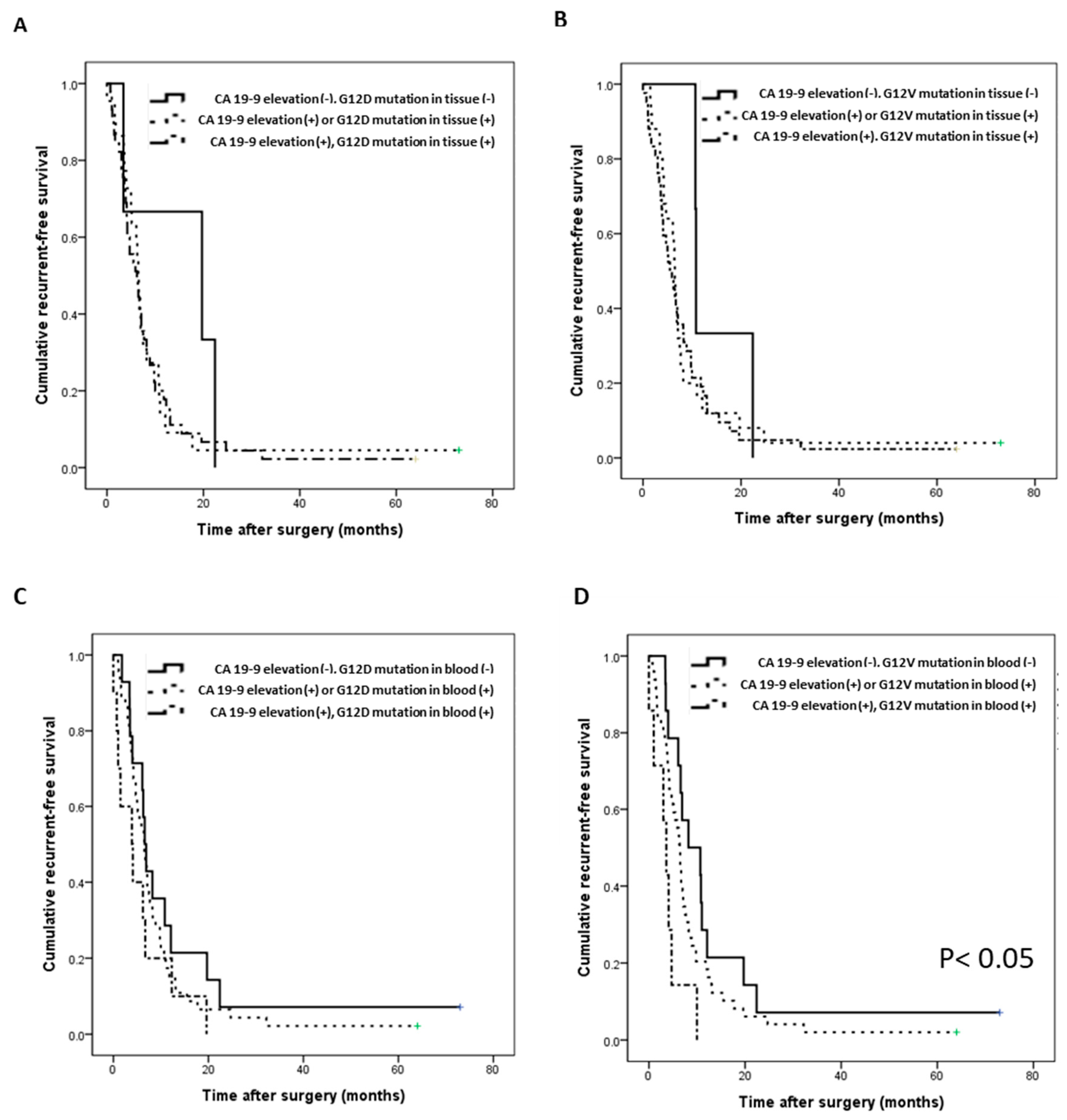
3.5. Survival Prediction with the Combination of KRAS Mutation and CA 19-9
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillen, S.; Schustser, T.; Büschenfelde, C.M.Z.; Friess, H.; Kleeff, J. Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [Green Version]
- Hidalgo, M. Pancreatic Cancer. N. Engl. J. Med. 2010, 362, 1605–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavros, M.N.; Moris, D.; Karanicolas, P.J.; Katz, M.H.G.; O’Reilly, E.M.; Pawlik, T.M. Clinical Trials of Systemic Chemotherapy for Resectable Pancreatic Cancer: A Review. JAMA Surg. 2021, 156, 663–672. [Google Scholar] [CrossRef]
- Pan, L.; Fang, J.; Tong, C.; Chen, M.; Zhang, B.; Juengpanich, S.; Wang, Y.; Cai, X. Survival benefits of neoadjuvant chemo(radio)therapy versus surgery first in patients with resectable or borderline resectable pancreatic cancer: A systematic review and meta-analysis. World J. Surg. Oncol. 2019, 18, 1–13. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Naffouje, S.A.; Salti, G.I.; Dahdaleh, F.S. Neoadjuvant Chemotherapy for Pancreatic Ductal Adenocarcinoma is Associated with Lower Post-Pancreatectomy Readmission Rates: A Population-Based Cohort Study. Ann. Surg. Oncol. 2021, 28, 1896–1905. [Google Scholar] [CrossRef]
- Hamarsheh, S.; Groß, O.; Brummer, T.; Zeiser, R. Immune modulatory effects of oncogenic KRAS in cancer. Nat. Commun. 2020, 11, 5439. [Google Scholar] [CrossRef] [PubMed]
- Waters, A.; Der, C.J. KRAS: The Critical Driver and Therapeutic Target for Pancreatic Cancer. Cold Spring Harb. Perspect. Med. 2018, 8, a031435. [Google Scholar] [CrossRef]
- Morris, J.P., IV; Wang, S.C.; Hebrok, M. KRAS, Hedgehog, Wnt and the twisted developmental biology of pancreatic ductal adenocarcinoma. Nat. Rev. Cancer 2010, 10, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Viciana, P.; Tetsu, O.; Oda, K.; Okada, J.; Rauen, K.; McCormick, F. Cancer Targets in the Ras Pathway. Cold Spring Harb. Symp. Quant. Biol. 2005, 70, 461–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grippo, P.J.; Nowlin, P.S.; Demeure, M.J.; Longnecker, D.S.; Sandgren, E.P. Preinvasive pancreatic neoplasia of ductal phenotype induced by acinar cell targeting of mutant Kras in transgenic mice. Cancer Res. 2003, 63, 2016–2019. [Google Scholar]
- Carvalho, P.D.; Guimarães, C.; Cardoso, A.; Mendonça, S.; Costa, A.; Oliveira, M.J.; Velho, S. KRAS Oncogenic Signaling Extends beyond Cancer Cells to Orchestrate the Microenvironment. Cancer Res. 2018, 78, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Ji, S.; Liang, C.; Qin, Y.; Jin, K.; Liang, D.; Xu, W.; Shi, S.; Zhang, B.; Liu, L.; et al. Critical role of oncogenic KRAS in pancreatic cancer (Review). Mol. Med. Rep. 2016, 13, 4943–4949. [Google Scholar] [CrossRef] [Green Version]
- Merz, V.; Gaule, M.; Zecchetto, C.; Cavaliere, A.; Casalino, S.; Pesoni, C.; Contarelli, S.; Sabbadini, F.; Bertolini, M.; Mangiameli, D.; et al. Targeting KRAS: The Elephant in the Room of Epithelial Cancers. Front. Oncol. 2021, 11, 638360. [Google Scholar] [CrossRef] [PubMed]
- Haigis, K.M. KRAS Alleles: The Devil Is in the Detail. Trends Cancer 2017, 3, 686–697. [Google Scholar] [CrossRef]
- Muñoz-Maldonado, C.; Zimmer, Y.; Medová, M. A Comparative Analysis of Individual RAS Mutations in Cancer Biology. Front. Oncol. 2019, 9, 1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Windon, A.L.; Loaiza-Bonilla, A.; Jensen, C.; Randall, M.P.; Morrissette, J.J.D.; Shroff, S.G. A KRAS wild type mutational status confers a survival advantage in pancreatic ductal adenocarcinoma. J. Gastrointest. Oncol. 2018, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bournet, B.; Muscari, F.; Buscail, C.; Assenat, E.; Barthet, M.; Hammel, P.; Selves, J.; Guimbaud, R.; Cordelier, P.; Buscail, L. KRAS G12D Mutation Subtype Is A Prognostic Factor for Advanced Pancreatic Adenocarcinoma. Clin. Transl. Gastroenterol. 2016, 7, e157. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Löhr, M.; Nilsson, M.; Segersvärd, R.; Matsson, H.; Verbeke, C.; Heuchel, R.; Kere, J.; Iafrate, A.J.; Zheng, Z.; et al. Variant Profiling of Candidate Genes in Pancreatic Ductal Adenocarcinoma. Clin. Chem. 2015, 61, 1408–1416. [Google Scholar] [CrossRef] [Green Version]
- Al-Mulla, F.; Milner-White, E.J.; Going, J.J.; Birnie, G.D. Structural differences between valine-12 and aspartate-12 Ras proteins may modify carcinoma aggression. J. Pathol. 1999, 187, 433–438. [Google Scholar] [CrossRef]
- Stolze, B.; Reinhart, S.; Bulllinger, L.; Fröhling, S.; Scholl, C. Comparative analysis of KRAS codon 12, 13, 18, 61 and 117 mutations using human MCF10A isogenic cell lines. Sci. Rep. 2015, 5, 8535. [Google Scholar] [CrossRef]
- Garassino, M.C.; Marabese, M.; Rusconi, P.; Rulli, E.; Martelli, O.; Farina, G.; Scanni, A.; Broggini, M. Different types of K-Ras mutations could affect drug sensitivity and tumour behaviour in non-small-cell lung cancer. Ann. Oncol. 2011, 22, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Lee, T.H.; Choi, M.K.; Kwon, I.S.; Bae, G.E.; Yeo, M.-K. Identification of a Clinical Cutoff Value for Multiplex KRASG12/G13 Mutation Detection in Colorectal Adenocarcinoma Patients Using Digital Droplet PCR, and Comparison with Sanger Sequencing and PNA Clamping Assay. J. Clin. Med. 2020, 9, 2283. [Google Scholar] [CrossRef]
- Demuth, C.; Spindler, K.-L.G.; Johansen, J.S.; Pallisgaard, N.; Nielsen, D.; Høgdall, E.; Vittrup, B.; Sorensen, B.S. Measuring KRAS Mutations in Circulating Tumor DNA by Droplet Digital PCR and Next-Generation Sequencing. Transl. Oncol. 2018, 11, 1220–1224. [Google Scholar] [CrossRef]
- Allen, P.J.; Kuk, D.; Castillo, C.F.-D.; Basturk, O.; Wolfgang, C.L.; Cameron, J.L.; Lillemoe, K.D.; Ferrone, C.R.; Morales-Oyarvide, V.; He, J.; et al. Multi-institutional Validation Study of the American Joint Commission on Cancer (8th Edition) Changes for T and N Staging in Patients With Pancreatic Adenocarcinoma. Ann. Surg. 2017, 265, 185–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, B.; Jun, E.; Liu, H.; Kim, E.J.; Park, Y.-Y.; Lim, S.-B.; Kim, S.C.; Shin, Y. A biocomposite-based rapid sampling assay for circulating cell-free DNA in liquid biopsy samples from human cancers. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Buscail, L.; Bournet, B.; Cordelier, P. Role of oncogenic KRAS in the diagnosis, prognosis and treatment of pancreatic cancer. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 153–168. [Google Scholar] [CrossRef] [PubMed]
- Taly, V.; Pekin, D.; Benhaim, L.; Kotsopoulos, S.K.; Le Corre, D.; Li, X.; Atochin, I.; Link, D.R.; Griffiths, A.D.; Pallier, K.; et al. Multiplex Picodroplet Digital PCR to Detect KRAS Mutations in Circulating DNA from the Plasma of Colorectal Cancer Patients. Clin. Chem. 2013, 59, 1722–1731. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Wang, S.; Fu, B.; Wang, J. Evaluation of droplet digital PCR and next generation sequencing for characterizing DNA reference material for KRAS mutation detection. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hadano, N.; Murakami, Y.; Uemura, K.; Hashimoto, Y.; Kondo, N.; Nakagawa, N.; Sueda, T.; Hiyama, E. Prognostic value of circulating tumour DNA in patients undergoing curative resection for pancreatic cancer. Br. J. Cancer 2016, 115, 59–65. [Google Scholar] [CrossRef]
- Bernard, V.; Kim, D.U.; Lucas, F.A.S.; Castillo, J.; Allenson, K.; Mulu, F.C.; Stephens, B.M.; Huang, J.; Semaan, A.; Guerrero, P.A.; et al. Circulating Nucleic Acids Are Associated With Outcomes of Patients With Pancreatic Cancer. Gastroenterology 2019, 156, 108–118.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.K.; Woo, S.M.; Park, B.; Yoon, K.-A.; Kim, Y.-H.; Joo, J.; Lee, W.J.; Han, S.-S.; Park, S.-J.; Kong, S.-Y. Prognostic Implications of Multiplex Detection of KRAS Mutations in Cell-Free DNA from Patients with Pancreatic Ductal Adenocarcinoma. Clin. Chem. 2018, 64, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Goonetilleke, K.; Siriwardena, A. Systematic review of carbohydrate antigen (CA 19-9) as a biochemical marker in the diagnosis of pancreatic cancer. Eur. J. Surg. Oncol. (EJSO) 2007, 33, 266–270. [Google Scholar] [CrossRef]
- Singh, S.; Tang, S.-J.; Sreenarasimhaiah, J.; Lara, L.F.; Siddiqui, A. The Clinical Utility and Limitations of Serum Carbohydrate Antigen (CA19-9) as a Diagnostic Tool for Pancreatic Cancer and Cholangiocarcinoma. Dig. Dis. Sci. 2011, 56, 2491–2496. [Google Scholar] [CrossRef]
- Salk, J.J.; Fox, E.J.; Loeb, L.A. Mutational Heterogeneity in Human Cancers: Origin and Consequences. Annu. Rev. Pathol. Mech. Dis. 2010, 5, 51–75. [Google Scholar] [CrossRef] [Green Version]
- Lai, E.; Puzzoni, M.; Ziranu, P.; Pretta, A.; Impera, V.; Mariani, S.; Liscia, N.; Soro, P.; Musio, F.; Persano, M.; et al. New therapeutic targets in pancreatic cancer. Cancer Treat. Rev. 2019, 81, 101926. [Google Scholar] [CrossRef]
- Reiter, J.G.; Baretti, M.; Gerold, J.M.; Makohon-Moore, A.P.; Daud, A.; Iacobuzio-Donahue, C.A.; Azad, N.S.; Kinzler, K.W.; Nowak, M.A.; Vogelstein, B. An analysis of genetic heterogeneity in untreated cancers. Nat. Rev. Cancer 2019, 19, 639–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.H.; Kim, S.C.; Hong, S.-M.; Kim, Y.H.; Song, K.-B.; Park, K.-M.; Lee, Y.-J. Genetic Alterations of K-ras, p53, c-erbB-2, and DPC4 in Pancreatic Ductal Adenocarcinoma and Their Correlation With Patient Survival. Pancreas 2013, 42, 216–222. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Values | |
|---|---|---|
| Age (y) | Avg. ± SD (Range) | 61.4 ± 10.1 (30–88) |
| Sex (Female/Male) | N (%) | 19/51 (27.1%/72.9%) |
| BMI(Kg/m2) | Avg. ± SD (range) | 23.5 ± 3.6 (16.2–35.4) |
| Neoadjuvant Chemotherapy (Yes/No) | N (%) | 61/9 (87.1%/12.9%) |
| Preoperative Lab | ||
| Hb (g/dL) | Avg. ± SD (range) | 12.6 ± 1.8 (8.4–16.5) |
| WBC (×103 μL) | Avg. ± SD (range) | 6.5 ± 2.2 (3.6–16.9) |
| Neutrophil (%) | Avg. ± SD (range) | 59.4 ± 12.7 (27.4–95.4) |
| Lymphocyte (%) | Avg. ± SD (range) | 29.2 ± 10.3 (2.2–51.7) |
| Monocyte (%) | Avg. ± SD (range) | 7.0 ± 2.4 (2.3–13.2) |
| Platelet (×103 μL) | Avg. ± SD (range) | 239.7 ± 95.9 (93.0–624.0) |
| AST (IU/L) | Avg. ± SD (range) | 30.9 ± 23.9 (8.0–161.0) |
| ALT (IU/L) | Avg. ± SD (range) | 47.6 ± 62.2 (7.0–359.0) |
| Total Protein (g/dL) | Avg. ± SD (range) | 6.6 ± 0.7 (3.9–7.9) |
| Albumin (g/dL) | Avg. ± SD (range) | 3.5 ± 0.5 (1.5–4.6) |
| BUN (mg/dL) | Avg. ± SD (range) | 14.0 ± 5.6 (2.0–35.0) |
| Creatinine (mg/dL) | Avg. ± SD (range) | 0.8 ± 0.4 (0.3–3.7) |
| CA19-9 (U/mL) | Avg. ± SD (range) | 674.5 ± 1301.7 (1.1–7480.0) |
| CEA (ng/mL) | Avg. ± SD (range) | 5.8 ± 8.1 (0.6–57.2) |
| Operation and Pathologic findings | ||
| PD/DPS | N (%) | 48/22 (68.6%/31.4%) |
| Tumor size (cm) | Avg. ± SD (range) | 3.7 ± 1.3 (1.6–9.0) |
| Tumor differentiation (wel/mod/por) | N (%) | 3/51/16 (4.3%/72.9%/22.9%) |
| T stage (T1/T2/T3) | N (%) | 2/48/20 (2.9%.68.6%/28.6%) |
| LVI (absent/present) | N (%) | 32/38 (45.7%/54.3%) |
| PNI (absent/present) | N (%) | 7/63 (10.0%/90.0%) |
| N stage (N0/N1/N2) | N (%) | 23/30/17 (32.9%/42.9%/24.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jun, E.; Koo, B.; Kim, E.J.; Hwang, D.W.; Lee, J.H.; Song, K.B.; Lee, W.; Park, Y.; Hong, S.; Shin, Y.; et al. Analysis of KRAS Mutation Subtype in Tissue DNA and Cell-Free DNA Using Droplet Digital PCR and the Function of Cell-Free DNA as a Recurrence Predictive Marker in Pancreatic Cancer. Biomedicines 2021, 9, 1599. https://doi.org/10.3390/biomedicines9111599
Jun E, Koo B, Kim EJ, Hwang DW, Lee JH, Song KB, Lee W, Park Y, Hong S, Shin Y, et al. Analysis of KRAS Mutation Subtype in Tissue DNA and Cell-Free DNA Using Droplet Digital PCR and the Function of Cell-Free DNA as a Recurrence Predictive Marker in Pancreatic Cancer. Biomedicines. 2021; 9(11):1599. https://doi.org/10.3390/biomedicines9111599
Chicago/Turabian StyleJun, Eunsung, Bonhan Koo, Eo Jin Kim, Dae Wook Hwang, Jae Hoon Lee, Ki Byung Song, Woohyung Lee, Yejong Park, Sarang Hong, Yong Shin, and et al. 2021. "Analysis of KRAS Mutation Subtype in Tissue DNA and Cell-Free DNA Using Droplet Digital PCR and the Function of Cell-Free DNA as a Recurrence Predictive Marker in Pancreatic Cancer" Biomedicines 9, no. 11: 1599. https://doi.org/10.3390/biomedicines9111599
APA StyleJun, E., Koo, B., Kim, E. J., Hwang, D. W., Lee, J. H., Song, K. B., Lee, W., Park, Y., Hong, S., Shin, Y., & Kim, S. C. (2021). Analysis of KRAS Mutation Subtype in Tissue DNA and Cell-Free DNA Using Droplet Digital PCR and the Function of Cell-Free DNA as a Recurrence Predictive Marker in Pancreatic Cancer. Biomedicines, 9(11), 1599. https://doi.org/10.3390/biomedicines9111599