
Early Chronic Kidney Disease (G1-G3a) in Combination with Steatosis as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study in Non-Diabetic Koreans



Abstract
:1. Introduction
2. Materials and Methods
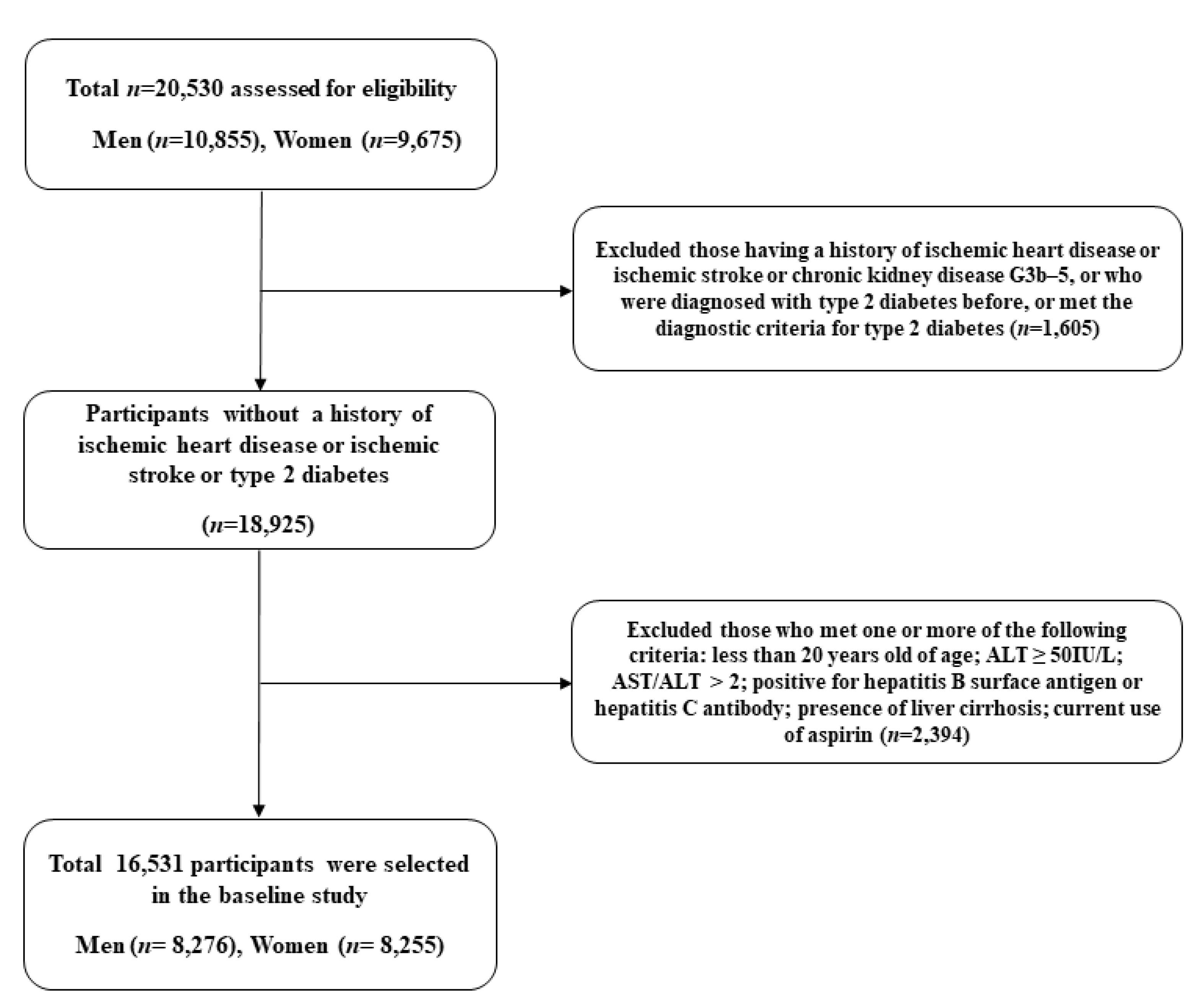
2.1. Study Population
2.2. Anthropometric and Laboratory Measurements
2.3. Definition of CKD and Hepatic Steatosis
2.4. Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.R. Global prevalence of chronic kidney disease—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.-y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple, L.S.; Katz, R.; Kestenbaum, B.; Shlipak, M.G.; Sarnak, M.J.; Stehman-Breen, C.; Seliger, S.; Siscovick, D.; Newman, A.B.; Fried, L. Chronic kidney disease and the risk of end-stage renal disease versus death. J. Gen. Intern. Med. 2011, 26, 379–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peter, W.S. Introduction: Chronic kidney disease: A burgeoning health epidemic. J. Manag. Care Pharm. 2007, 13, 2–5. [Google Scholar] [CrossRef] [Green Version]
- Coresh, J.; Byrd-Holt, D.; Astor, B.C.; Briggs, J.P.; Eggers, P.W.; Lacher, D.A.; Hostetter, T.H. Chronic kidney disease awareness, prevalence, and trends among us adults, 1999 to 2000. J. Am. Soc. Nephrol. 2005, 16, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Marchesini, G.; Bugianesi, E.; Forlani, G.; Cerrelli, F.; Lenzi, M.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; Melchionda, N. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003, 37, 917–923. [Google Scholar] [CrossRef]
- Vernon, G.; Baranova, A.; Younossi, Z. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef]
- Nasrallah, S.M.; Wills, C.E.; Galambos, J.T. Hepatic morphology in obesity. Dig. Dis. Sci. 1981, 26, 325–327. [Google Scholar] [CrossRef]
- Marchesini, G.; Brizi, M.; Morselli-Labate, A.M.; Bianchi, G.; Bugianesi, E.; McCullough, A.J.; Forlani, G.; Melchionda, N. Association of nonalcoholic fatty liver disease with insulin resistance. Am. J. Med. 1999, 107, 450–455. [Google Scholar] [CrossRef]
- Targher, G.; Arcaro, G. Non-alcoholic fatty liver disease and increased risk of cardiovascular disease. Atherosclerosis 2007, 191, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Nagy, J.; Kovacs, T. A brief review on the rising incidence of chronic kidney diseases and non-alcoholic fatty liver disease. Physiol. Int. 2019, 106, 305–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of nafld and nash: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Kendrick, J.; Chonchol, M.B. Nontraditional risk factors for cardiovascular disease in patients with chronic kidney disease. Nat. Clin. Pract. Nephrol. 2008, 4, 672–681. [Google Scholar] [CrossRef]
- Kronenberg, F. Emerging risk factors and markers of chronic kidney disease progression. Nat. Rev. Nephrol. 2009, 5, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Sanyal, A.J. The global nafld epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.-H.; Lee, Y.J.; Park, B. Joint effect of hepatic steatosis and alanine aminotransferase within the normal range on incident ischemic heart disease: A prospective study in koreans. Clin. Interv. Aging 2021, 16, 513. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.-S.; Lee, H.-R.; Shim, J.-Y.; Kang, H.-T.; Lee, Y.-J. Relationship between blood mercury concentrations and serum γ-glutamyltranspeptidase level in korean adults using data from the 2010 korean national health and nutrition examination survey. Clin. Chim. Acta 2014, 430, 160–163. [Google Scholar] [CrossRef]
- Cho, N.H.; Kim, K.M.; Choi, S.H.; Park, K.S.; Jang, H.C.; Kim, S.S.; Sattar, N.; Lim, S. High blood pressure and its association with incident diabetes over 10 years in the korean genome and epidemiology study (koges). Diabetes Care 2015, 38, 1333–1338. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.-T.; Kim, J.-K.; Shim, J.-Y.; Lee, H.-R.; Linton, J.A.; Lee, Y.-J. Low-grade inflammation, metabolic syndrome and the risk of chronic kidney disease: The 2005 korean national health and nutrition examination survey. J. Korean Med. Sci. 2012, 27, 630–635. [Google Scholar] [CrossRef] [Green Version]
- Jang, J.K.; Choi, S.H.; Lee, J.S.; Kim, S.Y.; Lee, S.S.; Kim, K.W. Accuracy of the ultrasound attenuation coefficient for the evaluation of hepatic steatosis: A systematic review and meta-analysis of prospective studies. Ultrasonography 2021. [Google Scholar] [CrossRef]
- Di Lullo, L.; House, A.; Gorini, A.; Santoboni, A.; Russo, D.; Ronco, C. Chronic kidney disease and cardiovascular complications. Heart Fail. Rev. 2015, 20, 259–272. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the american heart association councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef]
- Wang, C.C.; Lin, S.K.; Tseng, Y.F.; Hsu, C.S.; Tseng, T.C.; Lin, H.H.; Wang, L.Y.; Kao, J.H. Elevation of serum aminotransferase activity increases risk of carotid atherosclerosis in patients with non-alcoholic fatty liver disease. J. Gastroenterol. Hepatol. 2009, 24, 1411–1416. [Google Scholar] [CrossRef]
- Van Den Berghe, G.; Bronfman, M.; Vanneste, R.; Hers, H. The mechanism of adenosine triphosphate depletion in the liver after a load of fructose. A kinetic study of liver adenylate deaminase. Biochem. J. 1977, 162, 601–609. [Google Scholar] [CrossRef]
- Fan, C.-Y.; Wang, M.-X.; Ge, C.-X.; Wang, X.; Li, J.-M.; Kong, L.-D. Betaine supplementation protects against high-fructose-induced renal injury in rats. J. Nutr. Biochem. 2014, 25, 353–362. [Google Scholar] [CrossRef]
- Barchetta, I.; Carotti, S.; Labbadia, G.; Gentilucci, U.V.; Muda, A.O.; Angelico, F.; Silecchia, G.; Leonetti, F.; Fraioli, A.; Picardi, A. Liver vitamin d receptor, cyp2r1, and cyp27a1 expression: Relationship with liver histology and vitamin d3 levels in patients with nonalcoholic steatohepatitis or hepatitis c virus. Hepatology 2012, 56, 2180–2187. [Google Scholar] [CrossRef]
- Wang, X.X.; Jiang, T.; Shen, Y.; Santamaria, H.; Solis, N.; Arbeeny, C.; Levi, M. Vitamin d receptor agonist doxercalciferol modulates dietary fat-induced renal disease and renal lipid metabolism. Am. J. Physiol. -Ren. Physiol. 2011, 300, F801–F810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barchetta, I.; Angelico, F.; Del Ben, M.; Baroni, M.G.; Pozzilli, P.; Morini, S.; Cavallo, M.G. Strong association between non alcoholic fatty liver disease (nafld) and low 25 (oh) vitamin d levels in an adult population with normal serum liver enzymes. BMC Med. 2011, 9, 85. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, J.; Wang, X.; Ketteler, M.; Qureshi, A.R.; Heimbürger, O.; Bárány, P.; Lindholm, B.; Nordfors, L.; Stenvinkel, P. Is fetuin-a/α2-heremans-schmid glycoprotein associated with the metabolic syndrome in patients with chronic kidney disease? Am. J. Nephrol. 2008, 28, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Sharma, K. Mechanisms linking obesity, chronic kidney disease, and fatty liver disease: The roles of fetuin-a, adiponectin, and ampk. J. Am. Soc. Nephrol. 2010, 21, 406–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musso, G.; De Michieli, F.; Bongiovanni, D.; Parente, R.; Framarin, L.; Leone, N.; Berrutti, M.; Gambino, R.; Cassader, M.; Cohney, S. New pharmacologic agents that target inflammation and fibrosis in nonalcoholic steatohepatitis–related kidney disease. Clin. Gastroenterol. Hepatol. 2017, 15, 972–985. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Cassader, M.; Cohney, S.; De Michieli, F.; Pinach, S.; Saba, F.; Gambino, R. Fatty liver and chronic kidney disease: Novel mechanistic insights and therapeutic opportunities. Diabetes Care 2016, 39, 1830–1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Controls (n = 10,922) | Early CKD Only (n = 627) | Hepatic Steatosis Only (n = 4646) | Hepatic Steatosis + Early CKD (n = 336) | P value 1 | Post Hoc 2 | |
|---|---|---|---|---|---|---|
| Age (years) | 44.0 ± 10.5 | 46.4 ± 12.3 | 47.1 ± 9.9 | 50.7 ± 11.0 | <0.001 | a,b,c,e,f |
| Male sex (%) | 41.6 | 49.6 | 68.5 | 71.7 | <0.001 | - |
| BMI (kg/m2) | 22.3 ± 2.6 | 22.3 ± 2.7 | 25.3 ± 2.7 | 25.0 ± 2.5 | <0.001 | b,c,d,e |
| Systolic BP (mmHg) | 118.8 ± 14.9 | 121.5 ± 16.0 | 127.1 ± 14.5 | 130.3 ± 15.9 | <0.001 | a,b,c,d,e,f |
| Diastolic BP (mmHg) | 74.0 ± 9.7 | 75.9 ± 10.2 | 79.6 ± 9.6 | 81.9 ± 9.9 | <0.001 | a,b,c,d,e,f |
| AST (IU/L) | 19.2 ± 5.0 | 20.7 ± 5.7 | 21.6 ± 5.9 | 23.1 ± 5.9 | <0.001 | a,b,c,d,e,f |
| ALT (IU/L) | 17.4 ± 7.5 | 19.1 ± 7.9 | 24.8 ± 9.5 | 26.4 ± 9.3 | <0.001 | a,b,c,d,e,f |
| GGT (IU/L) | 23.9 ± 22.9 | 30.1 ± 31.7 | 37.3 ± 31.3 | 40.3 ± 32.6 | <0.001 | a,b,c,d,e |
| FPG (mg/dL) | 89.3 ± 8.9 | 90.7 ± 10.6 | 95.0 ± 10.0 | 96.3 ± 10.9 | <0.001 | a,b,c,d,e |
| Total cholesterol (mg/dL) | 183.9 ± 31.8 | 191.1 ± 35.0 | 198.5 ± 34.1 | 205.1 ± 35.0 | <0.001 | a,b,c,d,e,f |
| Triglyceride (mg/dL) | 101.0 ± 56.4 | 105.3 ± 59.7 | 162.7 ± 110.2 | 176.7 ± 105.4 | <0.001 | b,c,d,e,f |
| HDL-C (mg/dL) | 56.3 ± 12.6 | 56.8 ± 14.6 | 47.8 ± 10.2 | 48.0 ± 11.1 | <0.001 | b,c,d,e |
| Hs-CRP (mg/L) | 1.1 ± 2.8 | 1.9 ± 5.2 | 1.7 ± 4.0 | 2.1 ± 6.0 | <0.001 | a,b,c |
| Current smoker (%) | 21.2 | 27.8 | 30.8 | 26.8 | <0.001 | - |
| Alcohol drinking (%) | 41.5 | 45.4 | 47.5 | 45.1 | <0.001 | - |
| Regular exercise (%) | 31.8 | 32.5 | 29.4 | 32.5 | 0.022 | - |
| Hypertension (%) | 14.3 | 24.2 | 30.1 | 41.4 | <0.001 | - |
| Hepatic steatosis severity 3 | 0.0 ± 0.0 | 0.0 ± 0.0 | 1.8 ± 1.2 | 1.9 ± 1.2 | <0.001 | b,c,d,e,f |
| eGFR | 85.0 ± 13.3 | 74.7 ± 16.4 | 82.7 ± 12.2 | 71.4 ± 14.5 | <0.001 | a,b,c,d,e,f |
| Controls (n = 10,922) | Early CKD Only (n = 627) | Hepatic Steatosis Only (n = 4646) | Hepatic Steatosis + Early CKD (n = 336) | ||
|---|---|---|---|---|---|
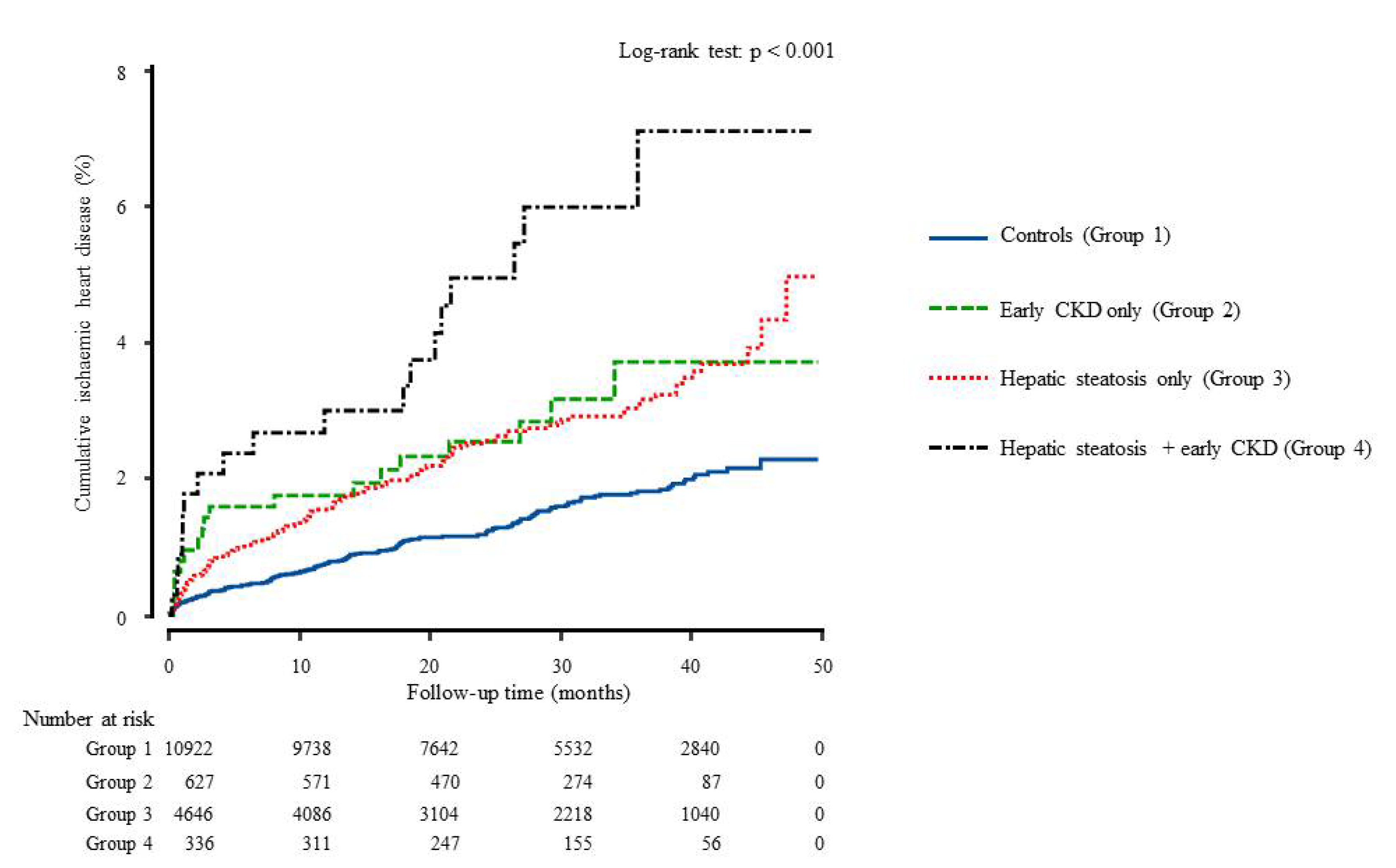
| New cases of ischemic heart disease, n | 164 | 18 | 126 | 18 | |
| Mean follow-up, years | 2.4 ± 1.1 | 2.3 ± 0.9 | 2.3 ± 1.1 | 2.3 ± 1.0 | |
| Pearson-years of follow-up | 26,023 | 1427 | 10,636 | 773 | |
| Incidence rate/1000 person–years | 6.3 | 12.6 | 11.8 | 23.3 | |
| Model 1 | HR (95% CI) | 1.00 (reference) | 1.51 (0.93–2.47) | 1.47 (1.16–1.86) | 2.16 (1.32–3.53) |
| p value | - | 0.097 | 0.001 | 0.002 | |
| Model 2 | HR (95% CI) | 1.00 (reference) | 1.34 (0.77–2.32) | 1.29 (0.98–1.69) | 1.95 (1.16–3.27) |
| p value | - | 0.299 | 0.068 | 0.011 | |
| Model 3 | HR (95% CI) | 1.00 (reference) | 1.26 (0.72–2.19) | 1.19 (0.90–1.57) | 1.76 (1.04–2.97) |
| p value | - | 0.425 | 0.230 | 0.033 | |
| Early CKD Only | Hepatic Steatosis Only | The Presence of Both | ||||
|---|---|---|---|---|---|---|
| HRs (95% CIs) | p value | HRs (95% CIs) | p value | HRs (95% CIs) | p value | |
| Age, years | 1.06 (1.05–1.07) | <0.001 | 1.06 (1.05–1.07) | <0.001 | 1.06 (1.05–1.07) | <0.001 |
| Male sex, yes vs. no | 1.34 (0.94–1.90) | 0.105 | 1.34 (0.94–1.91) | 0.106 | 1.34 (0.94–1.90) | 0.106 |
| Body mass index, kg/m2 | 1.04 (0.99–1.09) | 0.094 | 1.03 (0.98–1.08) | 0.276 | 1.03 (0.98–1.08) | 0.249 |
| Current smoking, yes vs. no | 1.22 (0.84–1.77) | 0.297 | 1.21 (0.84–1.76) | 0.307 | 1.22 (0.84–1.77) | 0.300 |
| Alcohol drinking, yes vs. no | 0.77 (0.59–0.99) | 0.047 | 0.77 (0.59–1.00) | 0.050 | 0.77 (0.59–1.00) | 0.052 |
| Regular exercise, yes vs. no | 1.18 (0.93–1.50) | 0.170 | 1.19 (0.94–1.51) | 0.156 | 1.19 (0.94–1.51) | 0.158 |
| Mean arterial pressure, mmHg | 0.99 (0.98–1.01) | 0.334 | 0.99 (0.98–1.01) | 0.319 | 0.99 (0.98–1.01) | 0.298 |
| Fasting plasma glucose, mg/dL | 1.02 (1.00–1.03) | 0.011 | 1.02 (1.00–1.03) | 0.017 | 1.01 (1.00–1.03) | 0.020 |
| HDL-cholesterol, mg/dL | 0.99 (0.98–1.00) | 0.118 | 0.99 (0.98–1.00) | 0.183 | 0.99 (0.98–1.00) | 0.187 |
| γ-glutamyltransferase, IU | 1.00 (1.00–1.01) | 0.733 | 1.00 (1.00–1.01) | 0.797 | 1.00 (1.00–1.01) | 0.820 |
| High-sensitivity C-reactive protein, mg/L | 1.00 (0.96–1.03) | 0.748 | 1.00 (0.97–1.03) | 0.779 | 1.00 (0.96–1.03) | 0.752 |
| Hypertension medication, yes vs. no | 1.71 (1.26–2.32) | <0.001 | 1.73 (1.27–2.34) | <0.001 | 1.71 (1.26–2.32) | <0.001 |
| Early CKD, yes vs. no | 1.38 (0.95–2.02) | 0.093 | - | - | - | - |
| Hepatic steatosis, yes vs. no | - | - | 1.22 (0.93–1.59) | 0.150 | - | - |
| The presence of both, yes vs. controls | - | - | - | - | 1.76 (1.04–2.97) | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-B.; Park, B.-J.; Lee, Y.-J.; Jung, D.-H. Early Chronic Kidney Disease (G1-G3a) in Combination with Steatosis as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study in Non-Diabetic Koreans. Biomedicines 2021, 9, 1358. https://doi.org/10.3390/biomedicines9101358
Lee S-B, Park B-J, Lee Y-J, Jung D-H. Early Chronic Kidney Disease (G1-G3a) in Combination with Steatosis as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study in Non-Diabetic Koreans. Biomedicines. 2021; 9(10):1358. https://doi.org/10.3390/biomedicines9101358
Chicago/Turabian StyleLee, Sung-Bum, Byoung-Jin Park, Yong-Jae Lee, and Dong-Hyuk Jung. 2021. "Early Chronic Kidney Disease (G1-G3a) in Combination with Steatosis as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study in Non-Diabetic Koreans" Biomedicines 9, no. 10: 1358. https://doi.org/10.3390/biomedicines9101358
APA StyleLee, S.-B., Park, B.-J., Lee, Y.-J., & Jung, D.-H. (2021). Early Chronic Kidney Disease (G1-G3a) in Combination with Steatosis as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study in Non-Diabetic Koreans. Biomedicines, 9(10), 1358. https://doi.org/10.3390/biomedicines9101358