Psilocybin as a New Approach to Treat Depression and Anxiety in the Context of Life-Threatening Diseases—A Systematic Review and Meta-Analysis of Clinical Trials


 ,
, 
 and
and
Abstract
1. Introduction
2. Methods
2.1. Search Strategy, Study Selection, Inclusion and Exclusion Criteria
2.2. Risk of Bias Assessment
2.3. Data Extraction and Summary
2.4. Statistical Analyses
3. Results
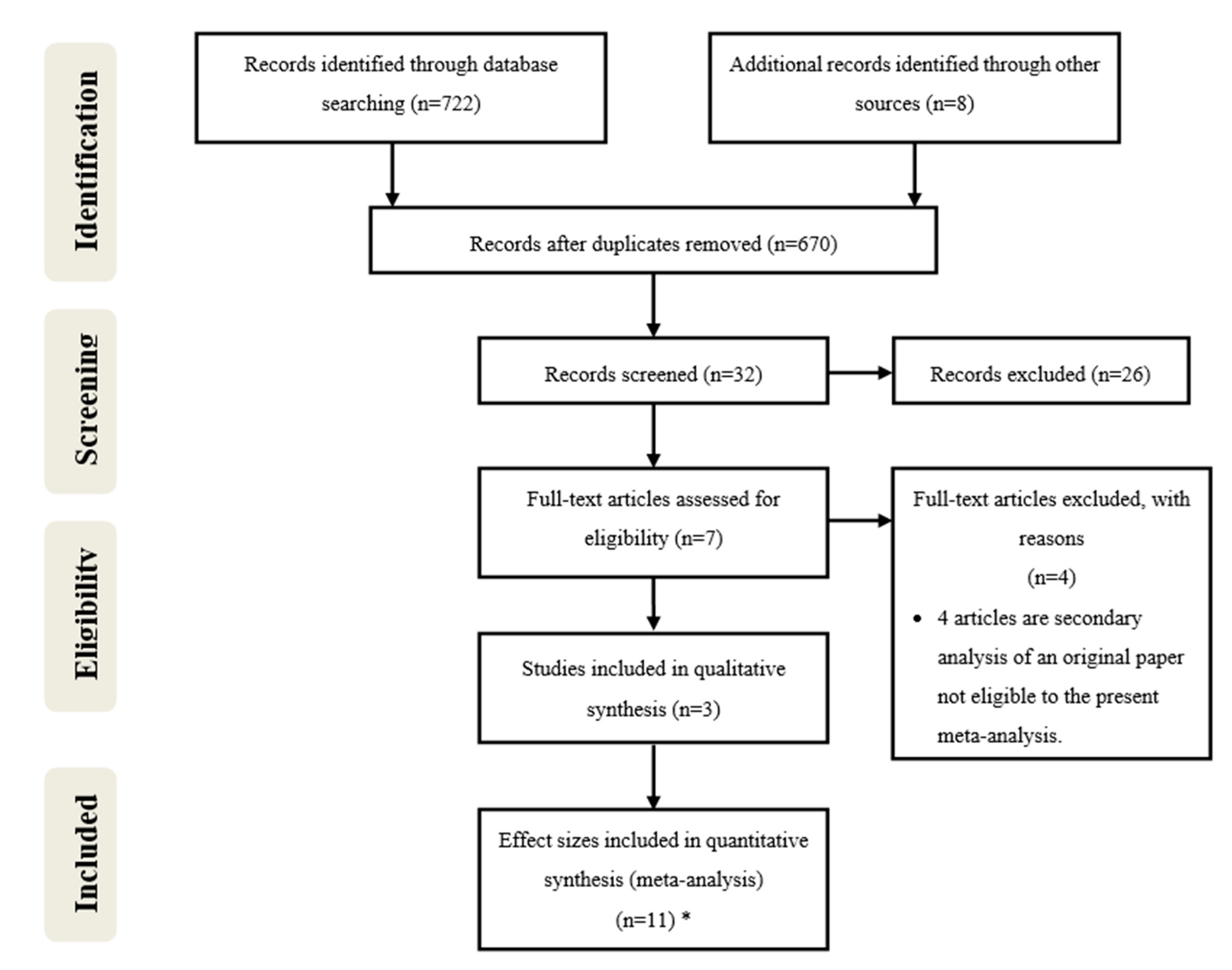
3.1. Search and Selection of Studies
3.2. Included Studies and Trials Characteristics
3.3. Risk of Publication Bias
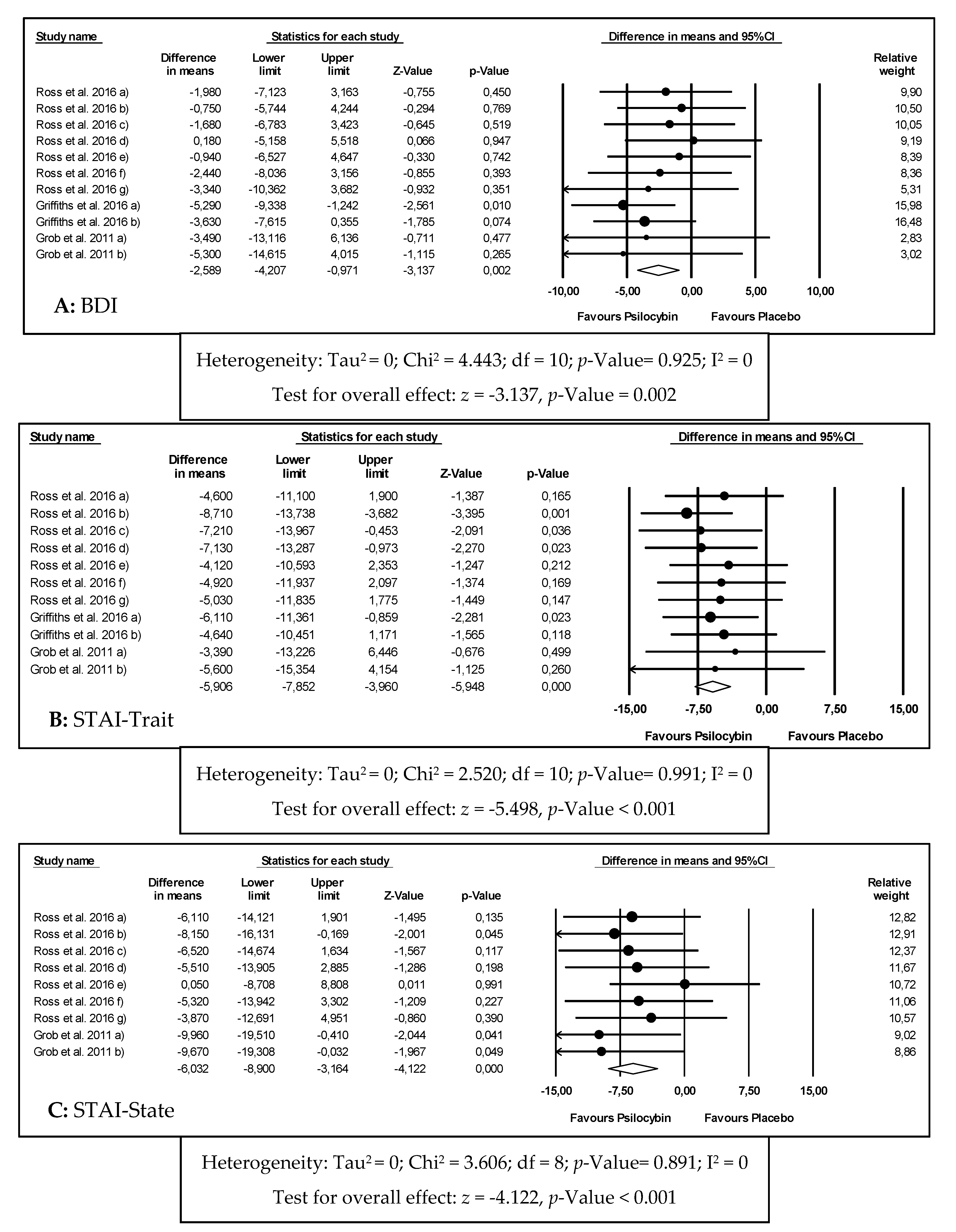
3.4. Primary Outcomes: Effects of Psilocybin on Depression and Anxiety
3.5. Subgroup and Sensitivity Analyses
3.6. Publication Bias
3.7. Secondary Outcomes: Effects of Psilocybin on Systolic Blood Pressure, Diastolic Blood Pressure and Heart Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Akil, H.; Gordon, J.; Hen, R.; Javitch, J.; Mayberg, H.; McEwen, B.; Meaney, M.J.; Nestler, E.J. Treatment resistant depression: A multi-scale, systems biology approach. Neurosci. Biobehav. Rev. 2018, 84, 272–288. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Filteau, M.; Martin, L.; Patry, S.; Carvalho, A.; Cha, D.S.; Barakat, M.; Miguelez, M. Treatment-resistant depression: Definitions, review of the evidence, and algorithmic approach. J. Affect. Disord. 2014, 156, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Passik, S.D.; Kirsh, K.L.; Rosenfield, B.; McDonald, M.V.; Theobald, D.E. The changeable nature of patients’ fears regarding chemotherapy: Implications for palliative care. J. Pain Symptom Manag. 2001, 21, 113–120. [Google Scholar] [CrossRef]
- Groenvold, M.; Petersen, M.A.; Idler, E.; Bjorner, J.B.; Fayers, P.M.; Mouridsen, H.T. Psychological distress and fatigue predicted recurrence and survival in primary breast cancer patients. Breast Cancer Res. Treat. 2007, 105, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Duberstein, P.R. Depression and cancer mortality: A meta-analysis. Psychol. Med. 2010, 40, 1797–1810. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J. Psychopharmacol. 2016, 30, 1181–1197. [Google Scholar] [CrossRef] [PubMed]
- Grassi, L.; Spiegel, D.; Riba, M. Advancing psychosocial care in cancer patients. F1000Research 2017, 6, 2083. [Google Scholar] [CrossRef] [PubMed]
- Freedman, R.A.; Kouri, E.M.; West, D.W.; Lii, J.; Keating, N.L. Association of Breast Cancer Knowledge With Receipt of Guideline-Recommended Breast Cancer Treatment. J. Oncol. Pract. 2016, 12, e613–e625. [Google Scholar] [CrossRef][Green Version]
- Orhurhu, V.J.; Claus, L.E.; Cohen, S.P. Ketamine Toxicity; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Goldberg, S.B.; Pace, B.T.; Nicholas, C.R.; Raison, C.L.; Hutson, P.R. The experimental effects of psilocybin on symptoms of anxiety and depression: A meta-analysis. Psychiatry Res. 2020, 284, 112749. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011, 63, S467–S472. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.; Hill, S.; Prictor, M.; McKenzie, J. Cochrane Consumers & Communication Review Group Study Quality Guide Guide for Review Authors on Assessing Study Quality. 2013. Available online: https://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/public/uploads/StudyQualityGuide_May%202013.pdf (accessed on 8 February 2020).
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savocic, J.; Schilz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.; Higgins, J. Introduction to Meta-Analysis; John Wiley & Sons: Chichester, UK, 2009. [Google Scholar]
- Higgins, J.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Ross, S.; Bossis, A.; Guss, J.; Agin-Liebes, G.; Malone, T.; Cohen, B.; Mennenga, S.E.; Belser, A.; Kalliontzi, K.; Babb, J.; et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: A randomized controlled trial. J. Psychopharmacol. 2016, 30, 1165–1180. [Google Scholar] [CrossRef]
- Grob, C.S.; Danforth, A.L.; Chopra, G.S.; Hagerty, M.; McKay, C.R.; Halberstadt, A.L.; Greer, G.R. Pilot Study of Psilocybin Treatment for Anxiety in Patients With Advanced-Stage Cancer. Arch. Gen. Psychiatry 2011, 68, 71. [Google Scholar] [CrossRef]
- Stroud, J.B.; Freeman, T.P.; Leech, R.; Hindocha, C.; Lawn, W.; Nutt, D.J.; Curran, H.V.; Carhart-Harris, R.L. Psilocybin with psychological support improves emotional face recognition in treatment-resistant depression. Psychopharmacology 2018, 235, 459–466. [Google Scholar] [CrossRef]
- Lyons, T.; Carhart-Harris, R.L. More Realistic Forecasting of Future Life Events After Psilocybin for Treatment-Resistant Depression. Front. Psychol. 2018, 9, 1721. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Bolstridge, M.; Day, C.M.J.; Rucker, J.; Watts, R.; Erritzoe, D.E.; Kaelen, M.; Giribaldi, B.; Bloomfield, M.; Pillimg, S.; et al. Psilocybin with psychological support for treatment-resistant depression: Six-month follow-up. Psychopharmacology 2018, 235, 399–408. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Bolstridge, M.; Rucker, J.; Day, C.M.J.; Erritzoe, D.; Kaelen, M.; Bloomfield, M.; Rickard, J.A.; Forbes, B.; Feilding, A.; et al. Psilocybin with psychological support for treatment-resistant depression: An open-label feasibility study. Lancet 2016, 3, 619–627. [Google Scholar] [CrossRef]
- Nichols, D.E. Psychedelics. Pharmacol. Rev. 2016, 68, 264–355. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R.L.; Erritzoe, D.; Williams, T.; Stone, J.M.; Reed, L.J.; Colasanti, A.; Tyacke, R.J.; Leech, R.; Malizia, A.L.; Murphy, K.; et al. Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc. Natl. Acad. Sci. USA 2012, 109, 2138–2143. [Google Scholar] [CrossRef] [PubMed]
- Kraehenmann, R.; Preller, K.H.; Scheidegger, M.; Pokorny, T.; Bosch, O.G.; Seifritz, E.; Vollenweider, F.X. Psilocybin-Induced Decrease in Amygdala Reactivity Correlates with Enhanced Positive Mood in Healthy Volunteers. Biol. Psychiatry 2015, 78, 572–581. [Google Scholar] [CrossRef] [PubMed]
- DeRubeis, R.J.; Siegle, G.J.; Hollon, S.D. Cognitive therapy versus medication for depression: Treatment outcomes and neural mechanisms. Nat. Rev. Neurosci. 2008, 9, 788–796. [Google Scholar] [CrossRef]
- Pandey, G.N.; Dwivedi, Y.; Rizavi, H.S.; Ren, X.; Pandey, S.C.; Pesold, C.; Roberts, R.C.; Conley, R.R.; Tamminga, C.A. Higher expression of serotonin 5-HT(2A) receptors in the postmortem brains of teenage suicide victims. Am. J. Psychiatry 2002, 159, 419–429. [Google Scholar] [CrossRef]
- Breitbart, W.; Rosenfeld, B.; Pessin, H.; Kaim, M.; Funesti-Esch, J.; Galietta, M.; Nelson, C.J.; Brescia, R. Depression, Hopelessness, and Desire for Hastened Death in Terminally Ill Patients With Cancer. JAMA 2000, 284, 2907. [Google Scholar] [CrossRef]
- Hasler, F.; Grimberg, U.; Benz, M.A.; Huber, T.; Vollenweider, F.X. Acute psychological and physiological affects of psilocybin in healthy humans: A double-blind, placebo-controlled dose-effect study. Psychopharmacology 2004, 172, 145–156. [Google Scholar] [CrossRef]
- Swift, T.C.; Belser, A.B.; Agin-Liebes, G.; Devenot, N.; Terrana, S.; Friedman, H.L.; Guss, J.; Bossis, A.P.; Ross, S. Cancer at the Dinner Table: Experiences of Psilocybin-Assisted Psychotherapy for the Treatment of Cancer-Related Distress. J. Humanist. Psychol. 2017, 57, 488–519. [Google Scholar] [CrossRef]
- Studerus, E.; Kometer, M.; Hasler, F.; Vollenweider, F.X. Acute, subacute and long-term subjective effects of psilocybin in healthy humans: A pooled analysis of experimental studies. J. Psychopharmacol. 2011, 25, 1434–1452. [Google Scholar] [CrossRef]
- Nichols, D.E.; Johnson, M.W.; Nichols, C.D. Psychedelics as Medicines: An Emerging New Paradigm. Clin. Pharmacol. Ther. 2017, 101, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Raichle, M.E. The neural correlates of consciousness: An analysis of cognitive skill learning. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 1998, 353, 1889–1901. [Google Scholar]
- Passie, T.; Seifert, J.; Schneider, U.; Emrick, H.M. The pharmacology of psilocybin. Addict. Biol. 2002, 7, 357–364. [Google Scholar] [CrossRef]
- Isbell, H. Comparison of the reactions induced by psilocybin and LSD-25 in man. Psychopharmacologia 1959, 1, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Hermle, L.; Simon, M.; Ruchsow, M.; Geppert, M. Hallucinogen-persisting perception disorder. Ther. Adv. Psychopharmacol. 2012, 2, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Studerus, E.; Gamma, A.; Kometer, M.; Vollenweider, F.X. Prediction of psilocybin response in healthy volunteers. PLoS ONE 2012, 7, e30800. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.; Richards, W.; Griffiths, R. Human hallucinogen research: Guidelines for safety. J. Psychopharmacol. 2008, 22, 603–620. [Google Scholar] [CrossRef]
- Tylš, F.; Páleníček, T.; Horáček, J. Psilocybin—Summary of knowledge and new perspectives. Eur. Neuropsychopharmacol. 2014, 24, 342–356. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.W.M.; Griffiths, R.R.; Hendricks, P.S.; Henningfield, J.E. The abuse potential of medical psilocybin according to the 8 factors of the Controlled Substances Act. Neropharmacology 2018, 142, 143–166. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study/Year | Sample Size | Study Design | Medical Condition | Mean/Range Age (Years) | Gender (F/M) | Intervention Drug | Control Group | Duration 1 | Primary Outcomes | Secondary Outcomes | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ross et al., 2016 [19] | 29 | Double-blind, randomized | Depression and anxiety associated with a life-threatening disease (cancer) | 56.28 | 18/11 | Psilocybin, 0.3 mg/kg | Niacin, 250 mg | (a) | 1 day post-dose 1 | BDI, STAI-State, STAI-Trait | - |
| (b) | 14 days post-dose 1 | ||||||||||
| (c) | 42 days post-dose 1 | ||||||||||
| (d) | 49 days post-dose 1 | ||||||||||
| (e) | 1 day post-dose 2 | ||||||||||
| (f) | 42 days post-dose 2 | ||||||||||
| (g) | 189 days post-dose 2 | ||||||||||
| Griffiths et al., 2016 [6] | 51 | Double-blind, randomized | Depression and anxiety associated with a life-threatening disease (cancer) | 56.3 | 25/26 | Psilocybin, 0.3 or 0.4 mg/kg | Psilocybin, 1 or 3 mg/70 kg | (a) | 28 days pre-crossover | BDI, STAI-Trait | SBP, DBP, HR |
| 35 days pre-crossover | |||||||||||
| (b) | 28 days pre-crossover | ||||||||||
| 35 days post-crossover | |||||||||||
| Grob et al., 2011 [20] | 12 | Pilot | Anxiety associated with a life-threatening disease (advanced-stage cancer) | From 36 to 58 | 11/1 | Psilocybin, 0.2 mg/kg | Niacin, 250 mg | (a) | 1 day | BDI, STAI-State, STAI-Trait | SBP, DBP, HR |
| (b) | 14 days | ||||||||||
| Outcome Analyzed | Number of Effect Sizes | WMD Observed (95% CI) | p-Value | I2 (%) | Model USED | WMD Adjusted |
|---|---|---|---|---|---|---|
| (95% CI) | ||||||
| BDI | 11 | −4.589 | 0.002 * | 0 | Fixed | −4.589 |
| (−4.207 to −0.971) | (−4.207 to −0.971) | |||||
| STAI-Trait | 11 | −5.906 | <0.001 * | 0 | Fixed | −6.389 |
| (−7.852 to −3.960) | (−8.151 to −4.626) | |||||
| STAI-State | 9 | −6.032 | <0.001 * | 0 | Fixed | −6.032 |
| (−8.900 to −3.164) | (−8.900 to −3.164) |
| Variable | BDI | STAI−Trait | ||||||
| Number of Effect Sizes | 95% CI | p−Value | I2 (%) | Number of Effect Sizes | 95% CI | p−Value | I2 (%) | |
| Total | 11 | − | - | - | 11 | − | − | − |
| WMD observed | - | −2.589 | 0.002 * | 0 | - | −5.906 | <0.001 * | 0 |
| (−4.207 to −0.971) | (−7.852 to −3.960) | |||||||
| WMD adjusted | - | −2.589 | - | - | - | −5.906 | - | - |
| (−4.207 to −0.971) | (−7.852 to −3.960) | |||||||
| Dose (mg/kg) | BDI | STAI−Trait | ||||||
| Number of Effect Sizes | 95% CI | p−Value | I2 (%) | Number of Effect Sizes | 95% CI | p−Value | I2 (%) | |
| 0.2 | 2 | −4.425 | 0.195 | 0 | 2 | −4.509 | 0.208 | 0 |
| (−11.118 to −2.269) | (−11.430 to 2.422) | |||||||
| 0.3 | 7 | −1.438 | 0.171 | 0 | 7 | −6.240 | <0.001 * | 0 |
| (−3.498 to 0.622) | (−8.615 to −3.865) | |||||||
| 0.4 | 2 | −4.447 | 0.002 * | 0 | 2 | −5.449 | 0.008 * | 0 |
| (−7.287 to −1.607) | (−9.345 to −1.553) | |||||||
| Time (days) after Psilocybin Administration | BDI | STAI−Trait | ||||||
| Number of Effect Sizes | 95% CI | p−Value | I2 (%) | Number of Effect Sizes | 95% CI | p−Value | I2 (%) | |
| 1 | 3 | −1.769 | 0.325 | 0 | 2 | −4.359 | 0.067 | 0 |
| (−5.290 to 1.752) | (−8.946 to 0.228) | |||||||
| 14 | 2 | −1.766 | 0.432 | 0 | 3 | −7.258 | 0.005 * | 39.340 |
| (−6.167 to 2.635) | (−11.330 to −3.184) | |||||||
| 35–189 | 6 | −3.024 | 0.003 * | 0 | 6 | −5.854 | <0.001 * | 0 |
| (−5.026 to −1.023) | (−8.385 to −3.322) | |||||||
| Time (Hours) after Psilocybin Administration | WMD (95% CI) | p-Value | I2 (%) |
|---|---|---|---|
| Systolic blood pressure (SBP) | |||
| 1 | 13.824 (9.433 to 18.216) | <0.001 * | 0 |
| 2 | 22.601 (18.075 to 27.128) | <0.001 * | 0 |
| 3 | 18.939 (14.893 to 22.986) | <0.001 * | 49.577 |
| 4 | 15.252 (10.998 to 19.505) | <0.001 * | 0 |
| 5 | 7.978 (4.184 to 11.773) | <0.001 * | 0 |
| 6 | 4.222 (0.792 to 7.652) | 0.016 * | 0 |
| Overall | 12.741 (11.100 to 14.382) | <0.001 * | 82.280 |
| Diastolic blood pressure (DBP) | |||
| 1 | 11.242 (8.843 to 13.640) | <0.001 * | 0 |
| 2 | 11.020 (8.598 to 13.441) | <0.001 * | 61.227 |
| 3 | 11.381 (9.020 13.743) | <0.001 * | 52.635 |
| 4 | 8.625 (6.080 to 11.170) | <0.001 * | 0 |
| 5 | 4.912 (2.374 to 7.450) | <0.001 * | 0 |
| 6 | 1.194 (-0.883 to 3.271) | 0.260 | 0 |
| Overall | 7.741 (6.722 to 8.710) | <0.001 * | 86.350 |
| Heart Rate | |||
| 1 | 5.056 (0.787 to 9.325) | 0.020 * | 0 |
| 2 | 8.268 (4.115 to 12.421) | <0.001 * | 0 |
| 3 | 8.281 (4.288 to 12.275) | <0.001 * | 44.279 |
| 4 | 8.520 (4.495 to 12.546) | <0.001 * | 64.899 |
| 5 | 5.599 (1.495 to 9.703) | 0.008 * | 0 |
| 6 | 3.363 (-0.716 to 7.441) | 0.106 | 13.130 |
| Overall | 6.549 (4.875 to 8.223) | <0.001 * | 24.596 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas, A.S.; Luís, Â.; Barroso, M.; Gallardo, E.; Pereira, L. Psilocybin as a New Approach to Treat Depression and Anxiety in the Context of Life-Threatening Diseases—A Systematic Review and Meta-Analysis of Clinical Trials. Biomedicines 2020, 8, 331. https://doi.org/10.3390/biomedicines8090331
Vargas AS, Luís Â, Barroso M, Gallardo E, Pereira L. Psilocybin as a New Approach to Treat Depression and Anxiety in the Context of Life-Threatening Diseases—A Systematic Review and Meta-Analysis of Clinical Trials. Biomedicines. 2020; 8(9):331. https://doi.org/10.3390/biomedicines8090331
Chicago/Turabian StyleVargas, Ana Sofia, Ângelo Luís, Mário Barroso, Eugenia Gallardo, and Luísa Pereira. 2020. "Psilocybin as a New Approach to Treat Depression and Anxiety in the Context of Life-Threatening Diseases—A Systematic Review and Meta-Analysis of Clinical Trials" Biomedicines 8, no. 9: 331. https://doi.org/10.3390/biomedicines8090331
APA StyleVargas, A. S., Luís, Â., Barroso, M., Gallardo, E., & Pereira, L. (2020). Psilocybin as a New Approach to Treat Depression and Anxiety in the Context of Life-Threatening Diseases—A Systematic Review and Meta-Analysis of Clinical Trials. Biomedicines, 8(9), 331. https://doi.org/10.3390/biomedicines8090331