Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective ‘Genetic’ Matched Analysis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Location
2.2. Study Population
2.3. Data Acquisition
2.4. Statistics
3. Results
3.1. Baseline Characteristics
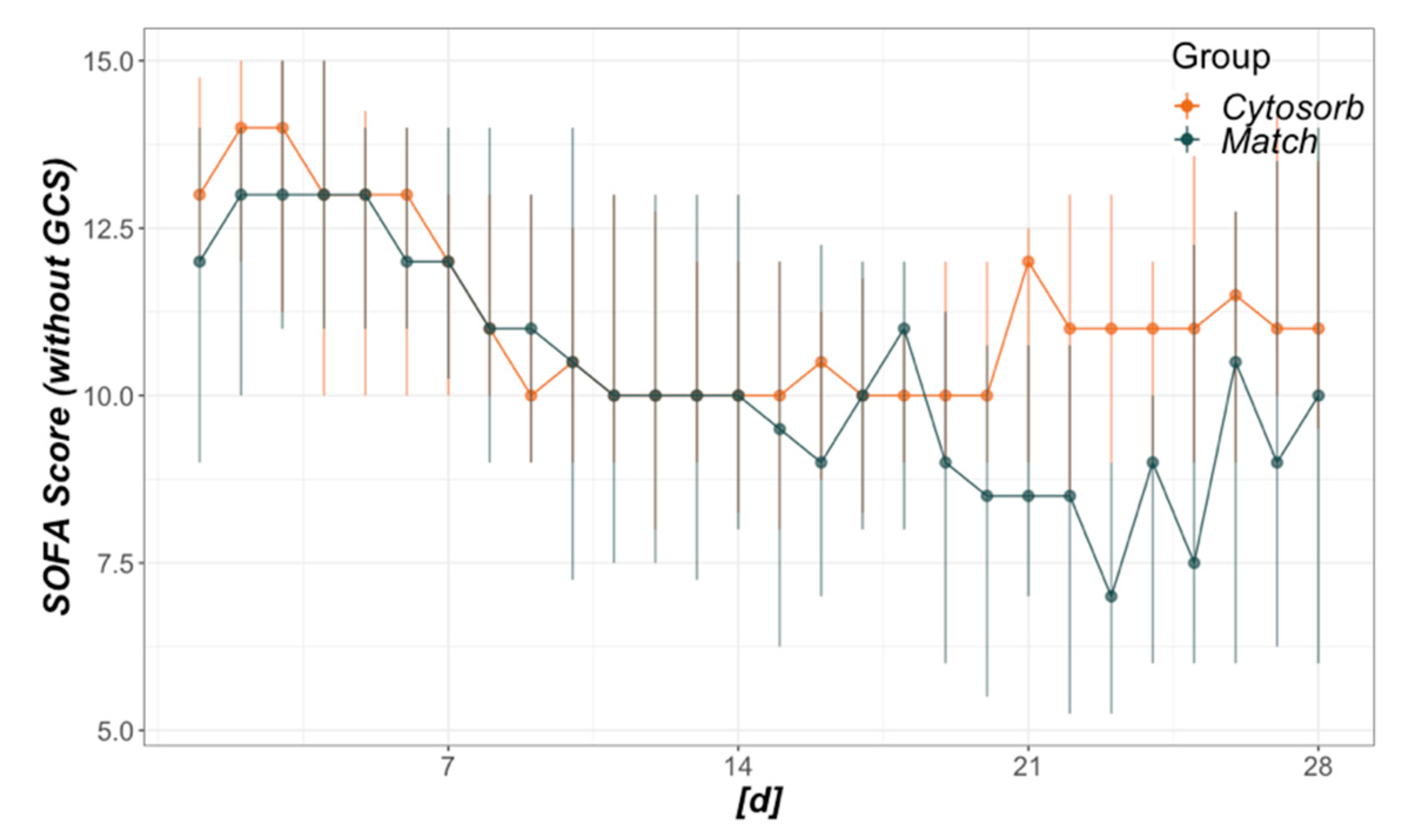
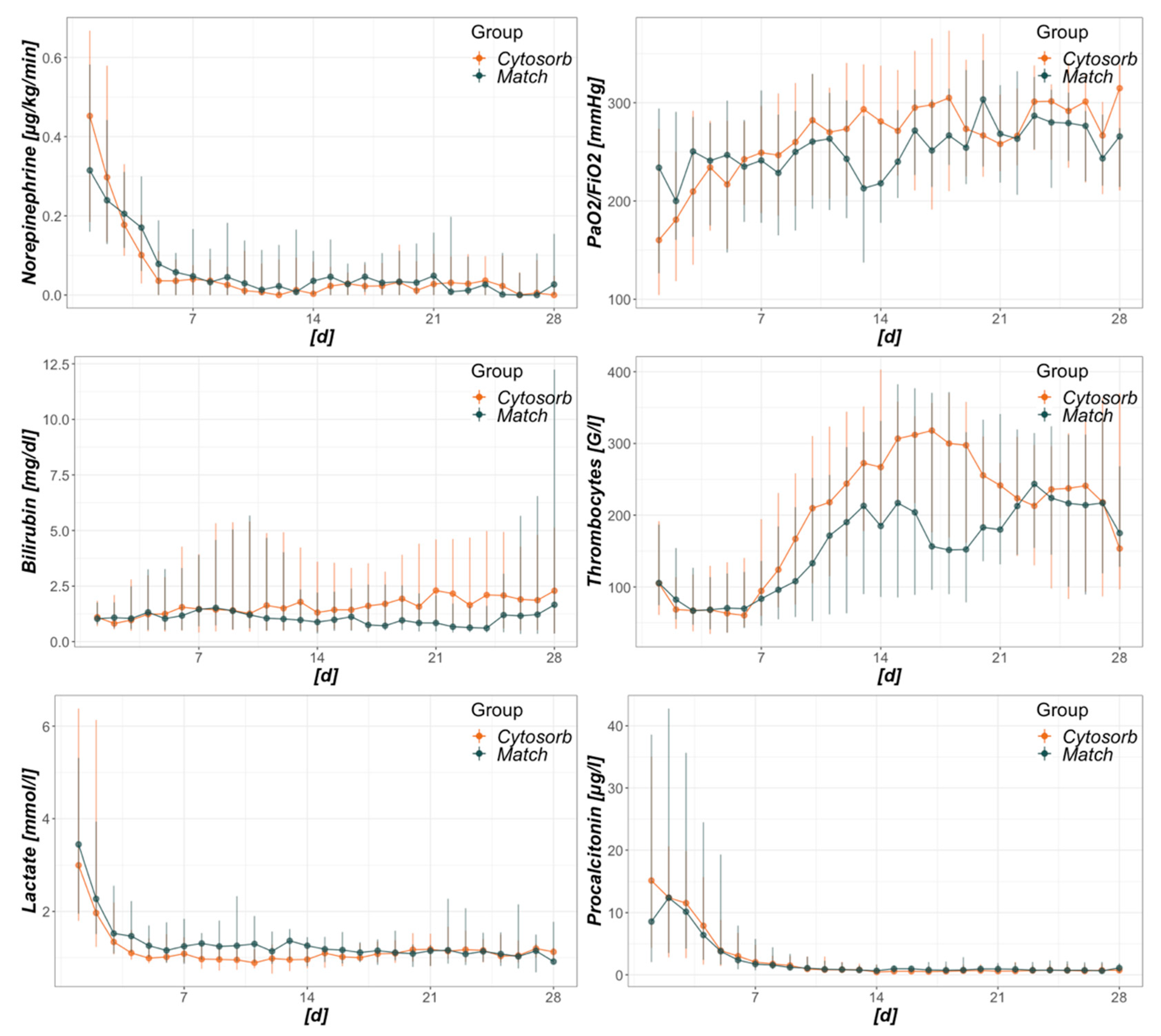
3.2. Development of Catecholamine Requirements and Organ Failure
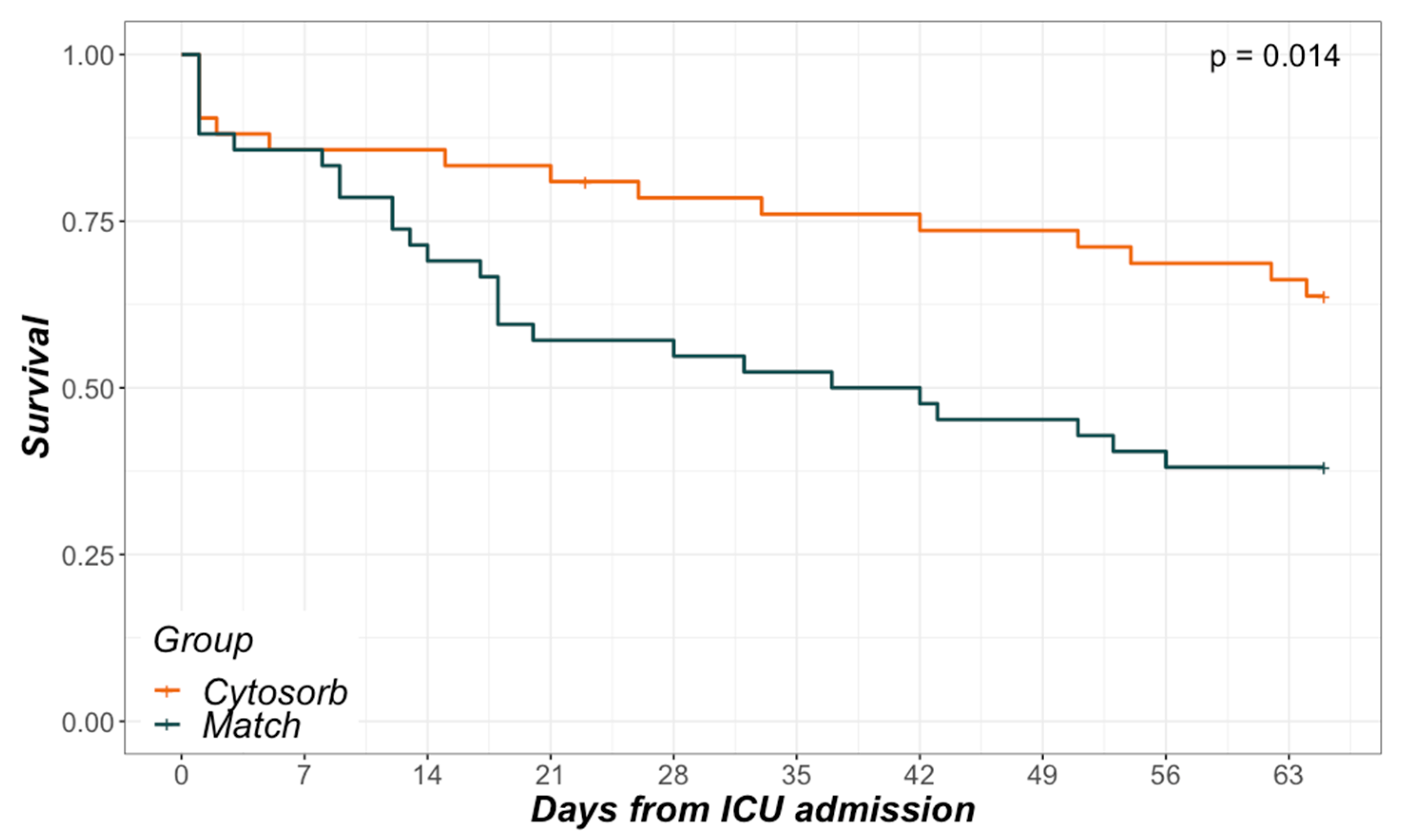
3.3. Mortality
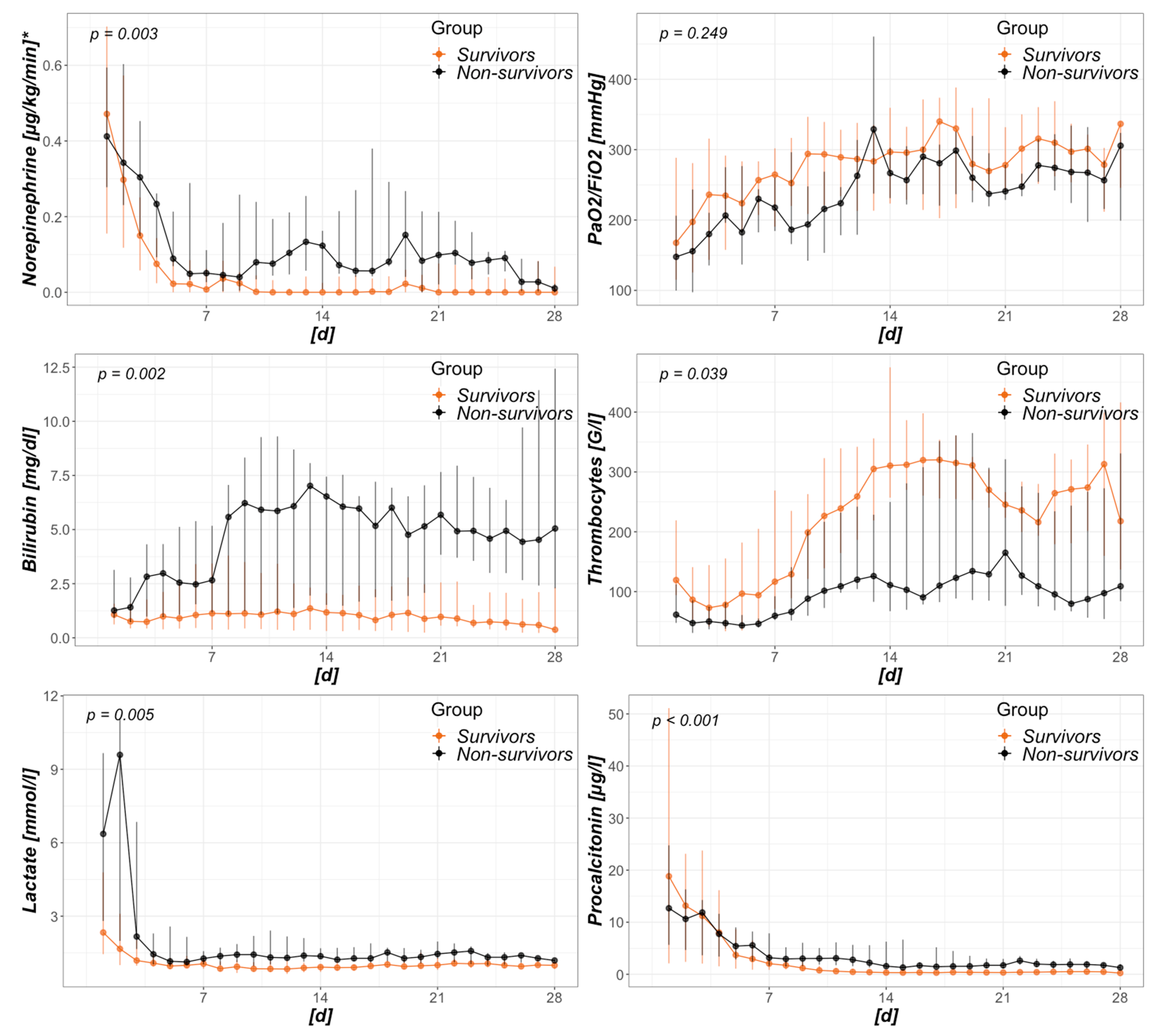
3.4. Risk Factors for Mortality within the CytoSorb Group
4. Discussion
4.1. Baseline Characteristics
4.2. Development of Catecholamine Requirements and Organ Failure
4.3. Mortality
4.4. Risk Factors for Mortality within the CytoSorb Group
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| RRT | renal replacement therapy |
| SOFA | sequential organ failure assessment score |
| ICU | intensive care unit |
| LOS | length of stay |
| GCS | Glasgow coma scale |
| OR | odds ratio |
| CI | confidence interval |
| ROC | receiver operating characteristics |
| IQR | interquartile range |
| CRP | c-reactive protein |
| PCT | procalcitonin |
| FiO2 | fraction of inspired oxygen |
| PaO2 | arterial oxygen partial pressure |
| COPD | chronic obstructive pulmonary disease |
| IL | interleukin |
| ARDS | acute respiratory distress syndrome |
Appendix A



References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Dantes, R.; Epstein, L.; Murphy, D.J.; Seymour, C.W.; Iwashyna, T.J.; Kadri, S.S.; Angus, D.C.; Danner, R.L.; Fiore, A.E.; et al. Incidence and Trends of Sepsis in US Hospitals Using Clinical vs. Claims Data, 2009–2014. JAMA 2017, 318, 1241. [Google Scholar] [CrossRef]
- Bauer, M.; Gerlach, H.; Vogelmann, T.; Preissing, F.; Stiefel, J.; Adam, D. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019—Results from a systematic review and meta-analysis. Crit. Care 2020, 24, 239. [Google Scholar] [CrossRef]
- van der Poll, T.; van de Veerdonk, F.L.; Scicluna, B.P.; Netea, M.G. The immunopathology of sepsis and potential therapeutic targets. Nat. Rev. Immunol. 2017, 17, 407–420. [Google Scholar] [CrossRef]
- Dinarello, C.A. Historical insights into cytokines. Eur. J. Immunol. 2007, 37, S34–S45. [Google Scholar] [CrossRef]
- Chousterman, B.G.; Swirski, F.K.; Weber, G.F. Cytokine storm and sepsis disease pathogenesis. Semin. Immunopathol. 2017, 39, 517–528. [Google Scholar] [CrossRef]
- Honore, P.M.; Hoste, E.; Molnár, Z.; Jacobs, R.; Joannes-Boyau, O.; Malbrain, M.L.N.G.; Forni, L.G. Cytokine removal in human septic shock: Where are we and where are we going? Ann. Intensive Care 2019, 9, 56. [Google Scholar] [CrossRef]
- Angus, D.C.; Poll, T. van der Severe Sepsis and Septic Shock. N. Engl. J. Med. 2013, 369, 840–851. [Google Scholar] [CrossRef]
- Kellum, J.A.; Kong, L.; Fink, M.P.; Weissfeld, L.A.; Yealy, D.M.; Pinsky, M.R.; Fine, J.; Krichevsky, A.; Delude, R.L.; Angus, D.C. Understanding the Inflammatory Cytokine Response in Pneumonia and Sepsis: Results of the Genetic and Inflammatory Markers of Sepsis (GenIMS) Study. Arch. Intern. Med. 2007, 167, 1655–1663. [Google Scholar] [CrossRef]
- Gogos, C.A.; Drosou, E.; Bassaris, H.P.; Skoutelis, A. Pro- versus Anti-inflammatory Cytokine Profile in Patients with Severe Sepsis: A Marker for Prognosis and Future Therapeutic Options. J. Infect. Dis. 2000, 181, 176–180. [Google Scholar] [CrossRef]
- Monneret, G.; Finck, M.-E.; Venet, F.; Debard, A.-L.; Bohé, J.; Bienvenu, J.; Lepape, A. The anti-inflammatory response dominates after septic shock: Association of low monocyte HLA-DR expression and high interleukin-10 concentration. Immunol. Lett. 2004, 95, 193–198. [Google Scholar] [CrossRef]
- Frencken, J.F.; van Vught, L.A.; Peelen, L.M.; Ong, D.S.Y.; Klouwenberg, P.M.C.K.; Horn, J.; Bonten, M.J.M.; van der Poll, T.; Cremer, O.L.; Consortium, M. An Unbalanced Inflammatory Cytokine Response Is Not Associated With Mortality Following Sepsis. Crit. Care Med. 2017, 45, e493–e499. [Google Scholar] [CrossRef]
- Ronco, C.; Tetta, C.; Mariano, F.; Wratten, M.L.; Bonello, M.; Bordoni, V.; Cardona, X.; Inguaggiato, P.; Pilotto, L.; D’Intini, V.; et al. Interpreting the Mechanisms of Continuous Renal Replacement Therapy in Sepsis: The Peak Concentration Hypothesis. Artif. Organs 2003, 27, 792–801. [Google Scholar] [CrossRef]
- Ankawi, G.; Neri, M.; Zhang, J.; Breglia, A.; Ricci, Z.; Ronco, C. Extracorporeal techniques for the treatment of critically ill patients with sepsis beyond conventional blood purification therapy: The promises and the pitfalls. Crit. Care 2018, 22, 262. [Google Scholar] [CrossRef]
- Zhou, F.; Peng, Z.; Murugan, R.; Kellum, J.A. Blood Purification and Mortality in Sepsis. Crit. Care Med. 2013, 41, 2209–2220. [Google Scholar] [CrossRef]
- Honoré, P.M.; Matson, J.R. Extracorporeal removal for sepsis: Acting at the tissue level—The beginning of a new era for this treatment modality in septic shock &ast. Crit. Care Med. 2004, 32, 896–897. [Google Scholar] [CrossRef]
- Carlo, J.V.D.; Alexander, S.R. Hemofiltration for Cytokine-Driven Illnesses: The Mediator Delivery Hypothesis. Int. J. Artif. Organs 2005, 28, 777–786. [Google Scholar] [CrossRef]
- Peng, Z.-Y.; Bishop, J.V.; Wen, X.-Y.; Elder, M.M.; Zhou, F.; Chuasuwan, A.; Carter, M.J.; Devlin, J.E.; Kaynar, A.M.; Singbartl, K.; et al. Modulation of chemokine gradients by apheresis redirects leukocyte trafficking to different compartments during sepsis, studies in a rat model. Crit. Care 2014, 18, R141. [Google Scholar] [CrossRef]
- Rimmelé, T.; Kellum, J.A. Clinical review: Blood purification for sepsis. Crit. Care 2011, 15, 205. [Google Scholar] [CrossRef]
- Vriese, A.S.D.; Vanholder, R.C.; Pascual, M.; Lameire, N.H.; Colardyn, F.A. Can inflammatory cytokines be removed efficiently by continuous renal replacement therapies? Intensive Care Med. 1999, 25, 903–910. [Google Scholar] [CrossRef]
- Gruda, M.C.; Ruggeberg, K.-G.; O’Sullivan, P.; Guliashvili, T.; Scheirer, A.R.; Golobish, T.D.; Capponi, V.J.; Chan, P.P. Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb® sorbent porous polymer beads. PLoS ONE 2018, 13, e0191676. [Google Scholar] [CrossRef]
- Malard, B.; Lambert, C.; Kellum, J.A. In vitro comparison of the adsorption of inflammatory mediators by blood purification devices. Intensive Care Med. Exp. 2018, 6, 12. [Google Scholar] [CrossRef]
- Song, M.; Winchester, J.; Albright, R.L.; Capponi, V.J.; Choquette, M.D.; Kellum, J.A. Cytokine Removal with a Novel Adsorbent Polymer. Blood Purif. 2004, 22, 428–434. [Google Scholar] [CrossRef]
- Namas, R.A.; Namas, R.; Lagoa, C.; Barclay, D.; Mi, Q.; Zamora, R.; Peng, Z.; Wen, X.; Fedorchak, M.V.; Valenti, I.E.; et al. Hemoadsorption Reprograms Inflammation in Experimental Gram-negative Septic Peritonitis: Insights from In Vivo and In Silico Studies. Mol. Med. 2012, 18, 1366–1374. [Google Scholar] [CrossRef]
- Peng, Z.-Y.; Carter, M.J.; Kellum, J.A. Effects of hemoadsorption on cytokine removal and short-term survival in septic rats. Crit. Care Med. 2008, 36, 1573–1577. [Google Scholar] [CrossRef]
- Schädler, D.; Pausch, C.; Heise, D.; Meier-Hellmann, A.; Brederlau, J.; Weiler, N.; Marx, G.; Putensen, C.; Spies, C.; Jörres, A.; et al. The effect of a novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic patients: A randomized controlled trial. PLoS ONE 2017, 12, e0187015. [Google Scholar] [CrossRef]
- Friesecke, S.; Stecher, S.-S.; Gross, S.; Felix, S.B.; Nierhaus, A. Extracorporeal cytokine elimination as rescue therapy in refractory septic shock: A prospective single-center study. J. Artif. Organs 2017, 20, 252–259. [Google Scholar] [CrossRef]
- Zuccari, S.; Damiani, E.; Domizi, R.; Scorcella, C.; D’Arezzo, M.; Carsetti, A.; Pantanetti, S.; Vannicola, S.; Casarotta, E.; Ranghino, A.; et al. Changes in Cytokines, Haemodynamics and Microcirculation in Patients with Sepsis/Septic Shock Undergoing Continuous Renal Replacement Therapy and Blood Purification with CytoSorb. Blood Purif. 2020, 49, 107–113. [Google Scholar] [CrossRef]
- Linden, K.; Scaravilli, V.; Kreyer, S.F.X.; Belenkiy, S.M.; Stewart, I.J.; Chung, K.K.; Cancio, L.C.; Batchinsky, A.I. Evaluation of the CytosorbTM Hemoadsorptive Column in a PIG Model of Severe Smoke and Burn Injury. Shock Inj. Inflamm. Sepsis Lab. Clin. Approaches 2015, 44, 487–495. [Google Scholar] [CrossRef]
- Hinz, B.; Jauch, O.; Noky, T.; Friesecke, S.; Abel, P.; Kaiser, R. CytoSorb, a Novel Therapeutic Approach for Patients with Septic Shock: A Case Report. Int. J. Artif. Organs 2015, 38, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Pathak, S.; Goyal, J.; Chaudhry, R.; Goel, R.B.; Barwal, A. Use of a novel hemoadsorption device for cytokine removal as adjuvant therapy in a patient with septic shock with multi-organ dysfunction: A case study. Indian J. Crit. Care Med. 2014, 18, 822–824. [Google Scholar] [CrossRef]
- Hetz, H.; Berger, R.; Recknagel, P.; Steltzer, H. Septic Shock Secondary to β-hemolytic Streptococcus-induced Necrotizing Fasciitis treated with a Novel Cytokine Adsorption Therapy. Int. J. Artif. Organs 2013, 37, 422–426. [Google Scholar] [CrossRef]
- Träger, K.; Fritzler, D.; Fischer, G.; Schröder, J.; Skrabal, C.; Liebold, A.; Reinelt, H. Treatment of Post-Cardiopulmonary Bypass SIRS by Hemoadsorption: A Case Series. Int. J. Artif. Organs 2016, 39, 141–146. [Google Scholar] [CrossRef]
- Bottari, G.; Guzzo, I.; Marano, M.; Stoppa, F.; Ravà, L.; Nardo, M.D.; Cecchetti, C. Hemoperfusion with Cytosorb in pediatric patients with septic shock: A retrospective observational study. Int. J. Artif. Organs 2020, 43, 587–593. [Google Scholar] [CrossRef]
- Singh, Y.; Chhabra, S.; Lashkari, K.; Taneja, A.; Garg, A.; Chandra, A.; Chhabra, M.; Singh, G.; Jain, S. Hemoadsorption by extracorporeal cytokine adsorption therapy (CytoSorb®) in the management of septic shock: A retrospective observational study. Int. J. Artif. Organs 2019, 43, 372–378. [Google Scholar] [CrossRef]
- Kogelmann, K.; Jarczak, D.; Scheller, M.; Drüner, M. Hemoadsorption by CytoSorb in septic patients: A case series. Crit. Care 2017, 21, 74. [Google Scholar] [CrossRef]
- Kogelmann, K.; Scheller, M.; Drüner, M.; Jarczak, D. Use of hemoadsorption in sepsis-associated ECMO-dependent severe ARDS: A case series. J. Intensive Care Soc. 2020, 21, 183–190. [Google Scholar] [CrossRef]
- Brouwer, W.P.; Duran, S.; Kuijper, M.; Ince, C. Hemoadsorption with CytoSorb shows a decreased observed versus expected 28-day all-cause mortality in ICU patients with septic shock: A propensity-score-weighted retrospective study. Crit. Care 2019, 23, 317. [Google Scholar] [CrossRef]
- Nadeem, R.; Obaida, Z.A.; Kamat, S. Hemoadsorption of cytokines by CytoSorb filter: A simulation study without human factor—pilot is the difference. Crit. Care 2020, 24, 13. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score—Development, utility and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef]
- Sekhon, J.S. Multivariate and Propensity Score Matching Software with Automated Balance Optimization: The Matching Package for R. J. Stat. Softw. 2011, 42. [Google Scholar] [CrossRef]
- Diamond, A.; Sekhon, J.S. Genetic Matching for Estimating Causal Effects: A General Multivariate Matching Method for Achieving Balance in Observational Studies. Rev. Econ. Stat. 2013, 95, 932–945. [Google Scholar] [CrossRef]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. nparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Softw. 2012, 50. [Google Scholar] [CrossRef]
- Hawchar, F.; László, I.; Öveges, N.; Trásy, D.; Ondrik, Z.; Molnar, Z. Extracorporeal cytokine adsorption in septic shock: A proof of concept randomized, controlled pilot study. J. Crit. Care 2018, 49, 172–178. [Google Scholar] [CrossRef]
- Friesecke, S.; Träger, K.; Schittek, G.A.; Molnar, Z.; Bach, F.; Kogelmann, K.; Bogdanski, R.; Weyland, A.; Nierhaus, A.; Nestler, F.; et al. International registry on the use of the CytoSorb® adsorber in ICU patients. Med. Klin. Intensivmed. Notfallmedizin 2019, 114, 699–707. [Google Scholar] [CrossRef]
- Peng, Z.-Y.; Wang, H.-Z.; Carter, M.J.; Dileo, M.V.; Bishop, J.V.; Zhou, F.-H.; Wen, X.-Y.; Rimmelé, T.; Singbartl, K.; Federspiel, W.J.; et al. Acute removal of common sepsis mediators does not explain the effects of extracorporeal blood purification in experimental sepsis. Kidney Int. 2012, 81, 363–369. [Google Scholar] [CrossRef]
- Hartmann, J.; Harm, S. Removal of bile acids by extracorporeal therapies: An in vitro study. Int. J. Artif. Organs 2017, 41, 52–57. [Google Scholar] [CrossRef]
- Damiani, E.; Adrario, E.; Luchetti, M.M.; Scorcella, C.; Carsetti, A.; Mininno, N.; Pierantozzi, S.; Principi, T.; Strovegli, D.; Bencivenga, R.; et al. Plasma Free Hemoglobin and Microcirculatory Response to Fresh or Old Blood Transfusions in Sepsis. PLoS ONE 2015, 10, e0122655. [Google Scholar] [CrossRef]
- Honoré, P.M.; Matson, J.R. Hemofiltration, adsorption, sieving and the challenge of sepsis therapy design. Crit. Care 2002, 6, 394. [Google Scholar] [CrossRef]
- Dünser, M.W.; Ruokonen, E.; Pettilä, V.; Ulmer, H.; Torgersen, C.; Schmittinger, C.A.; Jakob, S.; Takala, J. Association of arterial blood pressure and vasopressor load with septic shock mortality: A post hoc analysis of a multicenter trial. Crit. Care 2009, 13, R181. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Harrison, D.A.; Rubenfeld, G.D.; Rowan, K. Epidemiology of sepsis and septic shock in critical care units: Comparison between sepsis-2 and sepsis-3 populations using a national critical care database. Br. J. Anaesth. 2017, 119, 626–636. [Google Scholar] [CrossRef]
- Kaukonen, K.-M.; Bailey, M.; Suzuki, S.; Pilcher, D.; Bellomo, R. Mortality Related to Severe Sepsis and Septic Shock Among Critically Ill Patients in Australia and New Zealand, 2000–2012. JAMA 2014, 311, 1308–1316. [Google Scholar] [CrossRef]
- Gentile, L.F.; Cuenca, A.G.; Efron, P.A.; Ang, D.; Bihorac, A.; McKinley, B.A.; Moldawer, L.L.; Moore, F.A. Persistent inflammation and immunosuppression. J. Trauma Acute Care Surg. 2012, 72, 1491–1501. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CytoSorb (n = 42) | Match (n = 42) | p | |
|---|---|---|---|
| n (%) or Median (IQR) | n (%) or Median (IQR) | ||
| Sex | |||
| Male | 27 (64.3) | 25 (59.5) | |
| Female | 15 (35.7) | 17 (40.5) | 0.823 |
| Age | 64 (48–73) | 68 (55–74) | 0.400 |
| Sepsis source | |||
| Abdominal | 15 (35.7) | 15 (35.7) | 1.000 |
| Pulmonal | 15 (35.7) | 14 (33.3) | 0.820 |
| Urogenital | 2 (4.8) | 4 (9.5) | 0.6760 |
| Soft tissue | 8 (19.0) | 8 (19.0) | 1.000 |
| Other | 9 (21.4) | 6 (14.3) | 0.569 |
| Suspected pathogen | 0.887 | ||
| Gram negative bacteria | 19 (45.2) | 18 (42.9) | |
| Gram positive bacteria | 17 (40.5) | 15 (35.7) | |
| Influenza | 2 (4.8) | 1 (2.4) | |
| Candida spp. | 1 (2.4) | 2 (4.8) | |
| Aspergillus spp. | 0 (0.0) | 1 (2.4) | |
| Unknown | 3 (7.1) | 6 (14.3) | |
| Comorbidities | 35 (83.3) | 37 (88.1) | 0.757 |
| Arterial hypertension | 32 (76.2) | 30 (71.4) | 0.804 |
| Cerebrovascular disease | 8 (19.0) | 10 (23.8) | 0.791 |
| COPD + | 4 (9.5) | 8 (19.0) | 0.350 |
| Coronary artery disease | 15 (35.7) | 16 (38.1) | 1.000 |
| Diabetes mellitus type 2 | 19 (45.2) | 14 (33.3) | 0.372 |
| Heart failure | 7 (16.7) | 7 (16.7) | 1.000 |
| Chronic kidney disease | 16 (38.1) | 14 (33.3) | 0.820 |
| Peripheral artery disease | 2 (4.8) | 7 (16.7) | 0.1560 |
| Total number of comorbidities | |||
| All | 2.5 (1.0–4.0) | 2.0 (0.3–4.0) | 0.9280 |
| Survivors | 1.0 (0.0–3.0) | 1.0 (0.0–3.3) | 0.9790 |
| Non-survivors | 4.0 (2.0–5.0) | 3.0 (2.0–4.8) | 0.5270 |
| Baseline values | |||
| SOFA score | 13.0 (12.0–14.75) | 12.0 (9.0–14.0) | 0.023 |
| PaO2/FiO2 [mmHg] | 160 (104–287) | 234 (126–294) | 0.095 |
| Norepinephrine [µg/kg/min] * | 0.52 (0.25–0.81) | 0.25 (0.05–0.54) | 0.014 |
| Bilirubin [mg/dL] | 1.18 (0.72–2.02) | 1.03 (0.78–1.76) | 0.747 |
| Thrombocytes [G/L] | 111 (70–172) | 106 (75–187) | 0.964 |
| Creatinine [mg/dL] | 1.84 (1.17–2.74) | 1.80 (1.29–2.69) | 0.758 |
| Leukocytes [G/L] | 13.95 (6.60–20.88) | 9.93 (6.11–15.26) | 0.304 |
| CRP [g/dl] | 13.64 (7.95–19.57) | 14.47 (10.40–24.25) | 0.508 |
| PCT [µg/L] | 15.53 (2.35–33.24) | 8.56 (2.05–38.60) | 0.567 |
| Lactate [mmol/L] | 3.5 (1.8–7.3) | 3.4 (2.0–5.3) | 0.687 |
| ICU LOS [d] | 21 (12–33) | 15 (8–26) | 0.121 |
| Hospital LOS [d] | 30 (17–49) | 30 (13–48) | 0.505 |
| 28d—mortality | |||
| Dead | 9 (21.4) | 20 (47.6) | 0.029 |
| alive | 33 (78.6) | 22 (52.4) | |
| In hospital mortality | |||
| Dead | 15 (35.7) | 26 (61.9) | |
| alive | 27 (64.3) | 16 (38.1) | 0.015 |
| Crude Odds Ratio (95% CI) | p | Adjusted Odds Ratio (95% CI) | p | |
|---|---|---|---|---|
| Age (per year) | 1.08 (1.02–1.15) | 0.009 | 1.09 (0.97–1.22) | 0.164 |
| Female Gender | 0.85 (0.23–3.21) | 0.81 | ||
| Sepsis source | 7.86 (0.94–65.59) | 0.057 | ||
| Abdominal | 11.00 (2.42–49.91) | 0.002 | ||
| Pulmonal | 0.34 (0.08–1.51) | 0.156 | ||
| Urogenital | 2.00 (0.12–34.6) | 0.634 | ||
| Soft tissue | 1.20 (0.24–5.97) | 0.824 | ||
| Suspected pathogen | ||||
| Gram negative bacteria | reference | |||
| Gram positive bacteria | 0.53 (0.12–2.27) | 0.390 | ||
| Comorbidities (any) | 4.00 (0.43–36.92) | 0.221 | ||
| Arterial hypertension | 7.00 (0.79–61.97) | 0.080 | ||
| Cerebrovascular disease | 1.10 (0.22–5.42) | 0.907 | ||
| COPD | 6.50 (0.61–69.14) | 0.121 | ||
| Coronary artery disease | 3.27 (0.86–12.35) | 0.081 | ||
| Diabetes mellitus type 2 | 1.09 (0.31–3.88) | 0.890 | ||
| Heart failure | 1.44 (0.28–7.5) | 0.667 | ||
| Chronic kidney disease | 4.29 (1.12–16.44) | 0.034 | ||
| Peripheral artery disease | >99 (0–∞) | 0.992 | 1.46 (0.16–13.52) | 0.741 |
| Baseline characteristics | ||||
| SOFA Score (per point) | 1.57 (1.07–2.3) | 0.02 | ||
| PaO2/FiO2 (per mmHg) | 1.00 (0.99–1.00) | 0.757 | ||
| Norepinephrine (per µg/kg/min) * | 0.70 (0.09–5.59) | 0.737 | ||
| Bilirubin (per mg/dL) | 1.15 (0.87–1.51) | 0.334 | ||
| Thrombocytes (per G/L) | 0.98 (0.97–1.00) | 0.015 | 0.98 (0.96–1.00) | 0.049 |
| Procalcitonin (per µg/L) | 1.00 (0.99–1.00) | 0.287 | ||
| Lactate (per mmol/L) | 1.21 (1.03–1.43) | 0.019 | 1.27 (1.00–1.60) | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rugg, C.; Klose, R.; Hornung, R.; Innerhofer, N.; Bachler, M.; Schmid, S.; Fries, D.; Ströhle, M. Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective ‘Genetic’ Matched Analysis. Biomedicines 2020, 8, 539. https://doi.org/10.3390/biomedicines8120539
Rugg C, Klose R, Hornung R, Innerhofer N, Bachler M, Schmid S, Fries D, Ströhle M. Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective ‘Genetic’ Matched Analysis. Biomedicines. 2020; 8(12):539. https://doi.org/10.3390/biomedicines8120539
Chicago/Turabian StyleRugg, Christopher, Riko Klose, Rouven Hornung, Nicole Innerhofer, Mirjam Bachler, Stefan Schmid, Dietmar Fries, and Mathias Ströhle. 2020. "Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective ‘Genetic’ Matched Analysis" Biomedicines 8, no. 12: 539. https://doi.org/10.3390/biomedicines8120539
APA StyleRugg, C., Klose, R., Hornung, R., Innerhofer, N., Bachler, M., Schmid, S., Fries, D., & Ströhle, M. (2020). Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective ‘Genetic’ Matched Analysis. Biomedicines, 8(12), 539. https://doi.org/10.3390/biomedicines8120539