
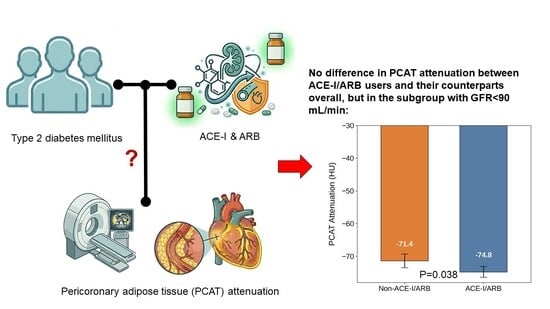
Analysis of Pericoronary Adipose Tissue Attenuation in Patients with Type 2 Diabetes Mellitus on Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers: A Propensity-Score-Matched Observational Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Screening and Clinical Data Collection
2.2. CT Imaging Acquisition and PCAT Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shih, C.J.; Chu, H.; Ou, S.M.; Chen, Y.T. Comparative effectiveness of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on major adverse cardiac events in patients with newly diagnosed type 2 diabetes: A nationwide study. Int. J. Cardiol. 2015, 199, 283–289. [Google Scholar] [CrossRef]
- Lv, X.; Zhang, Y.; Niu, Y.; Song, Q.; Zhao, Q. Comparison of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular outcomes in hypertensive patients with type 2 diabetes mellitus: A PRISMA-compliant systematic review and meta-analysis. Medicine 2018, 97, e0256. [Google Scholar] [CrossRef]
- Griendling, K.K.; Ushio-Fukai, M.; Lassègue, B.; Alexander, R.W. Angiotensin II signaling in vascular smooth muscle. New concepts. Hypertension 1997, 29, 366–373. [Google Scholar] [CrossRef]
- Brasier, A.R.; Recinos, A.; Eledrisi, M.S. Vascular inflammation and the renin-angiotensin system. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, J.; Hao, P.; Chen, W.; Meng, X.; Li, H.; Zhang, Y.; Zhang, C.; Yang, J. Imbalance between angiotensin II and angiotensin-(1-7) in human coronary atherosclerosis. J. Renin-Angiotensin-Aldosterone Syst. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Awad, K.; Zaki, M.M.; Mohammed, M.; Lewek, J.; Lavie, C.J.; Banach, M.; Lipid and Blood Pressure Meta-analysis Collaboration Group. Effect of the Renin-Angiotensin System Inhibitors on Inflammatory Markers: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Mayo Clin. Proc. 2022, 97, 1808–1823. [Google Scholar] [CrossRef]
- Tan, N.; Dey, D.; Marwick, T.H.; Nerlekar, N. Pericoronary Adipose Tissue as a Marker of Cardiovascular Risk: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2023, 81, 913–923. [Google Scholar] [CrossRef]
- Tzolos, E.; Williams, M.C.; McElhinney, P.; Lin, A.; Grodecki, K.; Flores Tomasino, G.; Cadet, S.; Kwiecinski, J.; Doris, M.; Adamson, P.D.; et al. Pericoronary Adipose Tissue Attenuation, Low-Attenuation Plaque Burden, and 5-Year Risk of Myocardial Infarction. JACC Cardiovasc. Imaging 2022, 15, 1078–1088. [Google Scholar] [CrossRef]
- Nedosugova, L.V.; Markina, Y.V.; Bochkareva, L.A.; Kuzina, I.A.; Petunina, N.A.; Yudina, I.Y.; Kirichenko, T.V. Inflammatory Mechanisms of Diabetes and Its Vascular Complications. Biomedicines 2022, 10, 1168. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulos, A.S.; Angelopoulos, A.; Papanikolaou, P.; Simantiris, S.; Oikonomou, E.K.; Vamvakaris, K.; Koumpoura, A.; Farmaki, M.; Trivella, M.; Vlachopoulos, C.; et al. Biomarkers of Vascular Inflammation for Cardiovascular Risk Prognostication: A Meta-Analysis. JACC Cardiovasc. Imaging 2022, 15, 460–471. [Google Scholar] [CrossRef]
- Yu, Y.; Ding, X.; Yu, L.; Dai, X.; Wang, Y.; Zhang, J. Increased coronary pericoronary adipose tissue attenuation in diabetic patients compared to non-diabetic controls: A propensity score matching analysis. J. Cardiovasc. Comput. Tomogr. 2022, 16, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Mátyás, B.B.; Benedek, I.; Raț, N.; Blîndu, E.; Parajkó, Z.; Mihăilă, T.; Benedek, T. Assessing the Impact of Long-Term High-Dose Statin Treatment on Pericoronary Inflammation and Plaque Distribution-A Comprehensive Coronary CTA Follow-Up Study. Int. J. Mol. Sci. 2024, 25, 1700. [Google Scholar] [CrossRef]
- Li, Y.; Yao, W.; Wang, T.; Yang, Q.; Song, K.; Zhang, F.; Wang, F.; Dang, Y. Association of semaglutide treatment with coronary artery inflammation in type 2 diabetes mellitus patients: A retrospective study based on pericoronary adipose tissue attenuation. Cardiovasc. Diabetol. 2024, 23, 348. [Google Scholar] [CrossRef]
- Wu, B.; Nieman, K.; Sandoval, R. High-intensity statin therapy is associated with reduced coronary inflammation on CT in patients with type 2 diabetes mellitus. Diabetes Obes. Metab. 2025, 27, 6395–6402. [Google Scholar] [CrossRef]
- Zhang, Y.; Ding, X.; Hua, B.; Liu, Q.; Chen, H.; Zhao, X.Q.; Li, W.; Li, H. Real-world use of ACEI/ARB in diabetic hypertensive patients before the initial diagnosis of obstructive coronary artery disease: Patient characteristics and long-term follow-up outcome. J. Transl. Med. 2020, 18, 150. [Google Scholar] [CrossRef]
- Pitt, B.; O’Neill, B.; Feldman, R.; Ferrari, R.; Schwartz, L.; Mudra, H.; Bass, T.; Pepine, C.; Texter, M.; Haber, H.; et al. The QUinapril Ischemic Event Trial (QUIET): Evaluation of chronic ACE inhibitor therapy in patients with ischemic heart disease and preserved left ventricular function. Am. J. Cardiol. 2001, 87, 1058–1063. [Google Scholar] [CrossRef]
- Hirohata, A.; Yamamoto, K.; Miyoshi, T.; Hatanaka, K.; Hirohata, S.; Yamawaki, H.; Komatsubara, I.; Murakami, M.; Hirose, E.; Sato, S.; et al. Impact of olmesartan on progression of coronary atherosclerosis a serial volumetric intravascular ultrasound analysis from the OLIVUS (impact of OLmesarten on progression of coronary atherosclerosis: Evaluation by intravascular ultrasound) trial. J. Am. Coll. Cardiol. 2010, 55, 976–982. [Google Scholar] [CrossRef]
- Williams, C.; Han, D.; Takagi, H.; Fordyce, C.B.; Sellers, S.; Blanke, P.; Lin, F.Y.; Shaw, L.J.; Lee, S.E.; Andreini, D.; et al. Effects of renin-angiotensin-aldosterone-system inhibitors on coronary atherosclerotic plaques: The PARADIGM registry. Atherosclerosis 2023, 383, 117301. [Google Scholar] [CrossRef] [PubMed]
- Olechnowicz-Tietz, S.; Gluba, A.; Paradowska, A.; Banach, M.; Rysz, J. The risk of atherosclerosis in patients with chronic kidney disease. Int. Urol. Nephrol. 2013, 45, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.; Gao, W.; Xu, H.; Liang, W.; Ma, G. Role and Mechanism of the Renin-Angiotensin-Aldosterone System in the Onset and Development of Cardiorenal Syndrome. J. Renin-Angiotensin-Aldosterone Syst. 2022, 2022, 3239057. [Google Scholar] [CrossRef] [PubMed]
- Pacurari, M.; Kafoury, R.; Tchounwou, P.B.; Ndebele, K. The Renin-Angiotensin-aldosterone system in vascular inflammation and remodeling. Int. J. Inflam. 2014, 2014, 689360. [Google Scholar] [CrossRef]
- Didion, S.P. Cellular and Oxidative Mechanisms Associated with Interleukin-6 Signaling in the Vasculature. Int. J. Mol. Sci. 2017, 18, 2563. [Google Scholar] [CrossRef]
- Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; Johnson, H.M.; et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2023, 82, 833–955. [Google Scholar] [CrossRef]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S.; et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N. Engl. J. Med. 2001, 345, 861–869. [Google Scholar] [CrossRef]
- Evans, M.; Carrero, J.J.; Szummer, K.; Åkerblom, A.; Edfors, R.; Spaak, J.; Jacobson, S.H.; Andell, P.; Lindhagen, L.; Jernberg, T. Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers in Myocardial Infarction Patients with Renal Dysfunction. J. Am. Coll. Cardiol. 2016, 67, 1687–1697. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 10. Cardiovascular Disease and Risk Management: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47, S179–S218. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef] [PubMed]
- Hoshida, S.; Kato, J.; Nishino, M.; Egami, Y.; Takeda, T.; Kawabata, M.; Tanouchi, J.; Yamada, Y.; Kamada, T. Increased angiotensin-converting enzyme activity in coronary artery specimens from patients with acute coronary syndrome. Circulation 2001, 103, 630–633. [Google Scholar] [CrossRef]
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl. J. Med. 2000, 342, 145–153. [Google Scholar] [CrossRef]
- Mancini, G.B.; Henry, G.C.; Macaya, C.; O’Neill, B.J.; Pucillo, A.L.; Carere, R.G.; Wargovich, T.J.; Mudra, H.; Lüscher, T.F.; Klibaner, M.I.; et al. Angiotensin-converting enzyme inhibition with quinapril improves endothelial vasomotor dysfunction in patients with coronary artery disease. The TREND (Trial on Reversing ENdothelial Dysfunction) Study. Circulation 1996, 94, 258–265. [Google Scholar] [CrossRef]
- Gomes, R.A.F.; Furtado, L.C.C.; Montenegro, M.V.; Filho, D.C.S. Beta-blockers in post-myocardial infarction with preserved ejection fraction: Systematic review and meta-analysis. Cardiovasc. Diagn. Ther. 2025, 15, 398–413. [Google Scholar] [CrossRef] [PubMed]
- Jeffers, B.W.; Robbins, J.; Bhambri, R. Efficacy of Calcium Channel Blockers Versus Other Classes of Antihypertensive Medication in the Treatment of Hypertensive Patients With Previous Stroke and/or Coronary Artery Disease: A Systematic Review and Meta-Analysis. Am. J. Ther. 2017, 24, e68–e80. [Google Scholar] [CrossRef]
- Reinhart, M.; Puil, L.; Salzwedel, D.M.; Wright, J.M. First-line diuretics versus other classes of antihypertensive drugs for hypertension. Cochrane Database Syst. Rev. 2023, 7, CD008161. [Google Scholar] [CrossRef]
- Feldman, B.S.; Cohen-Stavi, C.J.; Leibowitz, M.; Hoshen, M.B.; Singer, S.R.; Bitterman, H.; Lieberman, N.; Balicer, R.D. Defining the role of medication adherence in poor glycemic control among a general adult population with diabetes. PLoS ONE 2014, 9, e108145. [Google Scholar] [CrossRef] [PubMed]
- Adamek, K.E.; Ramadurai, D.; Gunzburger, E.; Plomondon, M.E.; Ho, P.M.; Raghavan, S. Association of Diabetes Mellitus Status and Glycemic Control With Secondary Prevention Medication Adherence After Acute Myocardial Infarction. J. Am. Heart Assoc. 2019, 8, e011448. [Google Scholar] [CrossRef]
- Tzolos, E.; McElhinney, P.; Williams, M.C.; Cadet, S.; Dweck, M.R.; Berman, D.S.; Slomka, P.J.; Newby, D.E.; Dey, D. Repeatability of quantitative pericoronary adipose tissue attenuation and coronary plaque burden from coronary CT angiography. J. Cardiovasc. Comput. Tomogr. 2021, 15, 81–84. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Non-ACE-I/ARB (n = 101) | ACE-I/ARB (n = 122) | p-Value |
|---|---|---|---|
| Age (years) | 64.0 ± 8.9 | 65.6 ± 8.7 | 0.164 |
| BMI (kg/m2) | 27.7 ± 4.0 | 28.5 ± 4.1 | 0.136 |
| CAC score | 518.8 ± 781.3 | 759.5 ± 1026.1 | 0.057 |
| HbA1C (%) | 6.7 ± 0.9 | 6.8 ± 0.8 | 0.519 |
| Glomerular filtration rate (mL/min) | 87.9 ± 19.0 | 84.3 ± 17.4 | 0.148 |
| Creatinine (mg/dL) | 0.90 ± 0.28 | 0.91 ± 0.24 | 0.803 |
| Sex (male) | 74.3% | 64.8% | 0.146 |
| Race | |||
| Caucasians | 35.6% | 32.0% | 0.572 |
| East Asians | 20.8% | 22.1% | 0.871 |
| African Americans | 4.0% | 5.7% | 0.758 |
| Hispanics | 15.8% | 22.1% | 0.306 |
| South Asians | 15.8% | 13.1% | 0.571 |
| Pacific Islanders | 4.0% | 3.3% | 1 |
| Others | 4.0% | 1.6% | 0.414 |
| Hypertension | 75.2% | 97.5% | <0.001 |
| Hyperlipidemia | 82.2% | 92.6% | 0.023 |
| Current smoker | 5.0% | 5.7% | 1 |
| Microvascular complications | 40.6% | 47.5% | 0.344 |
| Coronary interventions required | 14.9% | 17.2% | 0.716 |
| Indications for CT | |||
| Chest pain or anginal equivalent | 57.4% | 67.2% | 0.164 |
| Preoperative evaluation | 21.8% | 9.8% | 0.015 |
| Abnormal cardiac testing | 13.9% | 13.1% | 1 |
| Cardiomyopathy evaluation | 6.9% | 4.1% | 0.385 |
| Other | 0.0% | 5.7% | 0.017 |
| Medications | |||
| Metformin | 89.1% | 95.1% | 0.128 |
| GLP-1 receptor agonist | 13.9% | 26.2% | 0.204 |
| SGLT-2 inhibitors | 18.8% | 18.9% | 0.368 |
| Insulin | 22.0% | 15.6% | 0.228 |
| Aspirin | 36.6% | 44.3% | 0.275 |
| High-intensity statins | 23.8% | 44.3% | 0.001 |
| PCAT attenuation (HU) | −71.6 ± 8.0 | −73.5 ± 7.3 | 0.073 |
| 95% Confidence Interval | ||||
|---|---|---|---|---|
| Variables | Beta Coefficient | Lower Bound | Upper Bound | p-Value |
| Age | −0.081 | −0.196 | 0.035 | 0.304 |
| Male sex | 2.655 | 0.443 | 4.867 | 0.019 |
| Statin intensity | −1.708 | −0.312 | −0.297 | 0.018 |
| Hyperlipidemia | 0.302 | −2.927 | 3.531 | 0.854 |
| Hypertension | −1.265 | −4.329 | 1.798 | 0.416 |
| Presence of obstructive stenoses | 1.659 | −1.119 | 4.437 | 0.240 |
| CAC score * | −0.369 | −0.933 | 0.195 | 0.198 |
| Current smoking status | −1.845 | −6.268 | 2.578 | 0.412 |
| Variables | Non-ACE-I/ARB (n = 73) | ACE-I/ARB (n = 73) | p-Value |
|---|---|---|---|
| Age (years) | 64.3 ± 9.4 | 64.7 ± 8.9 | 0.767 |
| BMI (kg/m2) | 27.8 ± 3.8 | 27.8 ± 4.0 | 0.983 |
| CAC score | 589.7 ± 881.1 | 568.4 ± 960.8 | 0.899 |
| HbA1C (%) | 6.7 ± 0.9 | 6.8 ± 0.8 | 0.787 |
| Glomerular filtration rate (mL/min) | 86.1 ± 19.5 | 84.8 ± 17.8 | 0.686 |
| Creatinine (mg/dL) | 0.92 ± 0.30 | 0.92 ± 0.25 | 0.992 |
| Sex (male) | 72.6% | 71.2% | 1 |
| Race | |||
| Caucasians | 35.6% | 26.0% | 0.282 |
| East Asians | 21.9% | 21.9% | 1 |
| African Americans | 2.7% | 6.8% | 0.442 |
| Hispanics | 15.1% | 28.8% | 0.071 |
| South Asians | 13.7% | 15.1% | 1 |
| Pacific Islanders | 5.5% | 0.0% | 0.120 |
| Others | 5.5% | 1.4% | 0.366 |
| Hypertension | 95.9% | 95.9% | 1 |
| Hyperlipidemia | 90.4% | 89.0% | 1 |
| Current smoker | 6.8% | 2.7% | 0.442 |
| Microvascular complications | 42.5% | 45.2% | 0.868 |
| Coronary interventions required | 16.4% | 17.8% | 1 |
| Indications for CT | |||
| Chest pain or anginal equivalent | 60.3% | 69.9% | 0.298 |
| Preoperative evaluation | 17.8% | 11.0% | 0.346 |
| Abnormal cardiac testing | 13.7% | 12.3% | 1 |
| Cardiomyopathy evaluation | 8.2% | 2.7% | 0.275 |
| Other | 0.0% | 4.1% | 0.245 |
| Medications | |||
| Metformin | 89.0% | 94.5% | 0.367 |
| GLP-1 receptor agonist | 15.1% | 17.8% | 0.824 |
| SGLT-2 inhibitors | 21.9% | 28.8% | 0.447 |
| Insulin | 24.7% | 15.1% | 0.213 |
| Aspirin | 42.5% | 49.3% | 0.507 |
| High-intensity statins | 26.0% | 37.0% | 0.212 |
| PCAT attenuation (HU) | −71.7 ± 8.1 | −72.1 ± 7.5 | 0.722 |
| Classes of Medications | Not on Medication | On Medication | p-Value |
|---|---|---|---|
| DH-CCB | −72.3 ± 7.8 (n = 179) | −74.0 ± 6.9 (n = 44) | 0.502 |
| Beta blockers | −72.0 ± 7.2 (n = 168) | −74.5 ± 8.6 (n = 55) | 0.104 |
| Thiazides | −72.4 ± 7.8 (n = 189) | −73.8 ± 6.8 (n = 34) | 0.728 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Wu, B.; Joh, H.; Nieman, K.; Sandoval, R. Analysis of Pericoronary Adipose Tissue Attenuation in Patients with Type 2 Diabetes Mellitus on Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers: A Propensity-Score-Matched Observational Study. Biomedicines 2026, 14, 1268. https://doi.org/10.3390/biomedicines14061268
Wu B, Joh H, Nieman K, Sandoval R. Analysis of Pericoronary Adipose Tissue Attenuation in Patients with Type 2 Diabetes Mellitus on Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers: A Propensity-Score-Matched Observational Study. Biomedicines. 2026; 14(6):1268. https://doi.org/10.3390/biomedicines14061268
Chicago/Turabian StyleWu, Bryan, Hanyi Joh, Koen Nieman, and Ryan Sandoval. 2026. "Analysis of Pericoronary Adipose Tissue Attenuation in Patients with Type 2 Diabetes Mellitus on Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers: A Propensity-Score-Matched Observational Study" Biomedicines 14, no. 6: 1268. https://doi.org/10.3390/biomedicines14061268
APA StyleWu, B., Joh, H., Nieman, K., & Sandoval, R. (2026). Analysis of Pericoronary Adipose Tissue Attenuation in Patients with Type 2 Diabetes Mellitus on Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers: A Propensity-Score-Matched Observational Study. Biomedicines, 14(6), 1268. https://doi.org/10.3390/biomedicines14061268