

Interferon Gamma and Tumor Necrosis Factor Alpha Are Inflammatory Biomarkers for Major Adverse Cardiovascular Events in Patients with Peripheral Artery Disease
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
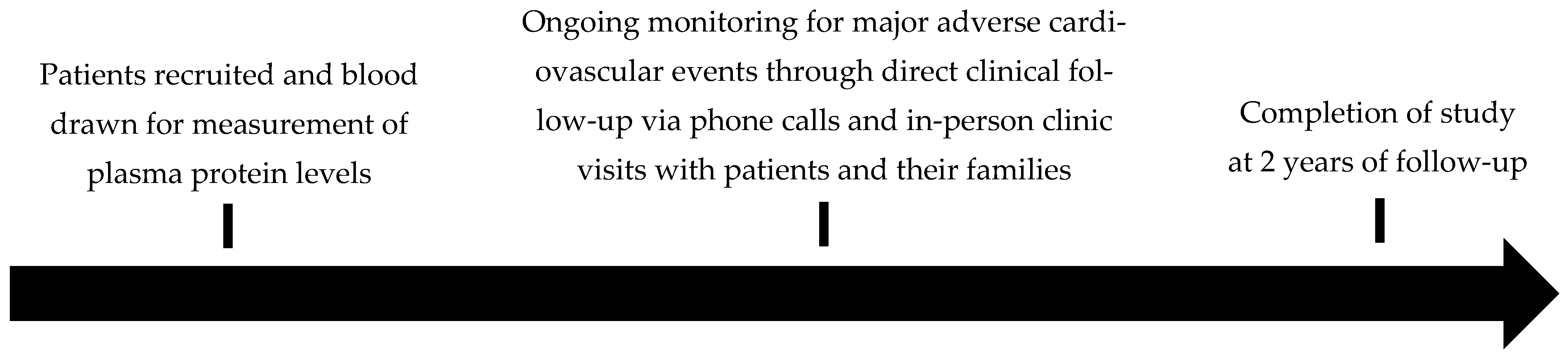
2.2. Design
2.3. Patient Recruitment
2.4. Baseline Characteristics
2.5. Quantification of Plasma Protein Concentrations
2.6. Follow-Up and Outcomes
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Outcomes
3.3. Plasma Concentrations of Inflammatory Proteins
3.4. Associations Between Inflammatory Proteins and 2-Year MACE in Patients with PAD
4. Discussion
4.1. Summary of Study Findings
4.2. Comparison to Existing Literature
4.3. Explanation of Findings
4.4. Implications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olin, J.W.; Sealove, B.A. Peripheral Artery Disease: Current Insight Into the Disease and Its Diagnosis and Management. Mayo Clin. Proc. 2010, 85, 678–692. [Google Scholar] [CrossRef] [PubMed]
- Horváth, L.; Németh, N.; Fehér, G.; Kívés, Z.; Endrei, D.; Boncz, I. Epidemiology of Peripheral Artery Disease: Narrative Review. Life 2022, 12, 1041. [Google Scholar] [CrossRef] [PubMed]
- Grenon, S.M.; Vittinghoff, E.; Owens, C.D.; Conte, M.S.; Whooley, M.; Cohen, B.E. Peripheral Artery Disease and Risk of Cardiovascular Events in Patients with Coronary Artery Disease: Insights from the Heart and Soul Study. Vasc. Med. 2013, 18, 176–184. [Google Scholar] [CrossRef]
- Adhikary, D.; Barman, S.; Ranjan, R.; Stone, H. A Systematic Review of Major Cardiovascular Risk Factors: A Growing Global Health Concern. Cureus 2022, 14, e30119. [Google Scholar] [CrossRef]
- Jennings, C.; Astin, F. A Multidisciplinary Approach to Prevention. Eur. J. Prev. Cardiol. 2017, 24, 77–87. [Google Scholar] [CrossRef]
- Li, B.; Shaikh, F.; Zamzam, A.; Syed, M.H.; Abdin, R.; Qadura, M. The Identification and Evaluation of Interleukin-7 as a Myokine Biomarker for Peripheral Artery Disease Prognosis. J. Clin. Med. 2024, 13, 3583. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Khan, H.; Shaikh, F.; Zamzam, A.; Abdin, R.; Qadura, M. Prediction of Major Adverse Limb Events in Females with Peripheral Artery Disease Using Blood-Based Biomarkers and Clinical Features. J. Cardiovasc. Transl. Res. 2024, 18, 316–330. [Google Scholar] [CrossRef]
- Li, B.; Shaikh, F.; Zamzam, A.; Raphael, R.; Syed, M.H.; Younes, H.K.; Abdin, R.; Qadura, M. Prediction of Peripheral Artery Disease Prognosis Using Clinical and Inflammatory Biomarker Data. J. Inflamm. Res. 2024, 17, 4865–4879. [Google Scholar] [CrossRef]
- Li, B.; Shaikh, F.; Zamzam, A.; Syed, M.H.; Abdin, R.; Qadura, M. A Machine Learning Algorithm for Peripheral Artery Disease Prognosis Using Biomarker Data. iScience 2024, 27, 109081. [Google Scholar] [CrossRef]
- Li, B.; Djahanpour, N.; Zamzam, A.; Syed, M.H.; Jain, S.; Arfan, S.; Abdin, R.; Qadura, M. The Prognostic Capability of Inflammatory Proteins in Predicting Peripheral Artery Disease Related Adverse Events. Front. Cardiovasc. Med. 2022, 9, 1073751. [Google Scholar] [CrossRef]
- Wolf, D.; Ley, K. Immunity and Inflammation in Atherosclerosis. Circ. Res. 2019, 124, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Elyasi, A.; Voloshyna, I.; Ahmed, S.; Kasselman, L.J.; Behbodikhah, J.; De Leon, J.; Reiss, A.B. The Role of Interferon-γ in Cardiovascular Disease: An Update. Inflamm. Res. 2020, 69, 975–988. [Google Scholar] [CrossRef]
- Yuan, S.; Carter, P.; Bruzelius, M.; Vithayathil, M.; Kar, S.; Mason, A.M.; Lin, A.; Burgess, S.; Larsson, S.C. Effects of Tumour Necrosis Factor on Cardiovascular Disease and Cancer: A Two-Sample Mendelian Randomization Study. EBioMedicine 2020, 59, 102956. [Google Scholar] [CrossRef]
- Dubois-Deruy, E.; Peugnet, V.; Turkieh, A.; Pinet, F. Oxidative Stress in Cardiovascular Diseases. Antioxidants 2020, 9, 864. [Google Scholar] [CrossRef]
- Frostegård, J. Immunity, Atherosclerosis and Cardiovascular Disease. BMC Med. 2013, 11, 117. [Google Scholar] [CrossRef] [PubMed]
- Booz, G.W.; Altara, R.; Zouein, F.A. Editorial: Immunomodulatory Approaches in Cardiovascular Diseases. Front. Cardiovasc. Med. 2022, 9, 873452. [Google Scholar] [CrossRef]
- Deroissart, J.; Porsch, F.; Koller, T.; Binder, C.J. Anti-Inflammatory and Immunomodulatory Therapies in Atherosclerosis. In Prevention and Treatment of Atherosclerosis: Improving State-of-the-Art Management and Search for Novel Targets; von Eckardstein, A., Binder, C.J., Eds.; Springer: Cham, Switzerland, 2022; ISBN 978-3-030-86075-2. [Google Scholar]
- Lutgens, E.; Atzler, D.; Döring, Y.; Duchene, J.; Steffens, S.; Weber, C. Immunotherapy for Cardiovascular Disease. Eur. Heart J. 2019, 40, 3937–3946. [Google Scholar] [CrossRef]
- Yamashita, T.; Sasaki, N.; Kasahara, K.; Hirata, K.-I. Anti-Inflammatory and Immune-Modulatory Therapies for Preventing Atherosclerotic Cardiovascular Disease. J. Cardiol. 2015, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Steven, S.; Frenis, K.; Oelze, M.; Kalinovic, S.; Kuntic, M.; Bayo Jimenez, M.T.; Vujacic-Mirski, K.; Helmstädter, J.; Kröller-Schön, S.; Münzel, T.; et al. Vascular Inflammation and Oxidative Stress: Major Triggers for Cardiovascular Disease. Oxid. Med. Cell Longev. 2019, 2019, 7092151. [Google Scholar] [CrossRef]
- Li, B.; Nassereldine, R.; Shaikh, F.; Younes, H.; AbuHalimeh, B.; Zamzam, A.; Abdin, R.; Qadura, M. Inflammatory Protein Panel: Exploring Diagnostic Insights for Peripheral Artery Disease Diagnosis in a Cross-Sectional Study. Diagnostics 2024, 14, 1847. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Collins, G.S.; Moons, K.G.M.; Dhiman, P.; Riley, R.D.; Beam, A.L.; Calster, B.V.; Ghassemi, M.; Liu, X.; Reitsma, J.B.; van Smeden, M.; et al. TRIPOD+AI Statement: Updated Guidance for Reporting Clinical Prediction Models That Use Regression or Machine Learning Methods. BMJ 2024, 385, e078378. [Google Scholar] [CrossRef]
- Gul, F.; Janzer, S.F. Peripheral Vascular Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of Classification Systems in Peripheral Artery Disease. Semin. Interv. Radiol. 2014, 31, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; De Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; The Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF). Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.V.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An Updated Definition of Stroke for the 21st Century: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024, 105, S117–S314. [Google Scholar] [CrossRef]
- Paulino, E.T. Development of the Cardioprotective Drugs Class Based on Pathophysiology of Myocardial Infarction: A Comprehensive Review. Curr. Probl. Cardiol. 2024, 49, 102480. [Google Scholar] [CrossRef]
- Siti, H.N.; Kamisah, Y.; Kamsiah, J. The Role of Oxidative Stress, Antioxidants and Vascular Inflammation in Cardiovascular Disease (a Review). Vascul Pharmacol. 2015, 71, 40–56. [Google Scholar] [CrossRef]
- Luminex Assays, Multiplex Immunoassays. Available online: https://www.bio-techne.com/ (accessed on 6 May 2023).
- Luminex Assays-CA. Available online: https://www.thermofisher.com/ca/en/home/life-science/antibodies/immunoassays/procartaplex-assays-luminex.html (accessed on 18 December 2021).
- MAGPIX® System | xMAP Instrument | Luminex Corporation. Available online: https://www.luminexcorp.com/magpix-system/ (accessed on 18 December 2021).
- xPONENT® Software for xMAP® Instruments; Luminex Corporation: Austin, TX, USA, 2025.
- Rigatti, S.J. Random Forest. J. Insur. Med. 2017, 47, 31–39. [Google Scholar] [CrossRef] [PubMed]
- SPSS Software. Available online: https://www.ibm.com/analytics/spss-statistics-software (accessed on 18 December 2021).
- Libby, P.; Lichtman, A.H.; Hansson, G.K. Immune Effector Mechanisms Implicated in Atherosclerosis: From Mice to Humans. Immunity 2013, 38, 1092–1104. [Google Scholar] [CrossRef] [PubMed]
- Golia, E.; Limongelli, G.; Natale, F.; Fimiani, F.; Maddaloni, V.; Pariggiano, I.; Bianchi, R.; Crisci, M.; D’Acierno, L.; Giordano, R.; et al. Inflammation and Cardiovascular Disease: From Pathogenesis to Therapeutic Target. Curr. Atheroscler. Rep. 2014, 16, 435. [Google Scholar] [CrossRef]
- Zohlnhöfer, D.; Richter, T.; Neumann, F.-J.; Nührenberg, T.; Wessely, R.; Brandl, R.; Murr, A.; Klein, C.A.; Baeuerle, P.A. Transcriptome Analysis Reveals a Role of Interferon-γ in Human Neointima Formation. Mol. Cell 2001, 7, 1059–1069. [Google Scholar] [CrossRef]
- Ranjbaran, H.; Sokol, S.I.; Gallo, A.; Eid, R.E.; Iakimov, A.O.; D’Alessio, A.; Kapoor, J.R.; Akhtar, S.; Howes, C.J.; Aslan, M.; et al. An Inflammatory Pathway of IFN-γ Production in Coronary Atherosclerosis. J. Immunol. 2007, 178, 592–604. [Google Scholar] [CrossRef]
- Frostegård, J.; Ulfgren, A.-K.; Nyberg, P.; Hedin, U.; Swedenborg, J.; Andersson, U.; Hansson, G.K. Cytokine Expression in Advanced Human Atherosclerotic Plaques: Dominance of pro-Inflammatory (Th1) and Macrophage-Stimulating Cytokines. Atherosclerosis 1999, 145, 33–43. [Google Scholar] [CrossRef]
- Ammirati, E.; Moroni, F.; Magnoni, M.; Camici, P.G. The Role of T and B Cells in Human Atherosclerosis and Atherothrombosis. Clin. Exp. Immunol. 2015, 179, 173–187. [Google Scholar] [CrossRef]
- Zhao, J.; Sun, B.; Huang, S.; Chen, Y.; Yan, J. Causal Association between Circulating Inflammatory Proteins and Peripheral Artery Disease: A Bidirectional Two-Sample Mendelian Randomization Study. Front. Immunol. 2024, 15, 1432041. [Google Scholar] [CrossRef] [PubMed]
- Botti, C.; Maione, C.; Dogliotti, G.; Russo, P.; Signoriello, G.; Molinari, A.M.; Corsi, M.M.; Sica, V.; Cobellis, G. Circulating Cytokines Present in the Serum of Peripheral Arterial Disease Patients Induce Endothelial Dysfunction. J. Biol. Regul. Homeost. Agents 2012, 26, 67–79. [Google Scholar]
- Rolski, F.; Błyszczuk, P. Complexity of TNF-α Signaling in Heart Disease. J. Clin. Med. 2020, 9, 3267. [Google Scholar] [CrossRef]
- Pande, R.L.; Brown, J.; Buck, S.; Redline, W.; Doyle, J.; Plutzky, J.; Creager, M.A. Association of Monocyte Tumor Necrosis Factor α Expression and Serum Inflammatory Biomarkers with Walking Impairment in Peripheral Artery Disease. J. Vasc. Surg. 2015, 61, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Rifai, N.; Pfeffer, M.; Sacks, F.; Lepage, S.; Braunwald, E. Elevation of Tumor Necrosis Factor-α and Increased Risk of Recurrent Coronary Events after Myocardial Infarction. Circulation 2000, 101, 2149–2153. [Google Scholar] [CrossRef]
- Kim, E.Y.; Moudgil, K.D. Immunomodulation of Autoimmune Arthritis by Pro-Inflammatory Cytokines. Cytokine 2017, 98, 87–96. [Google Scholar] [CrossRef]
- Razaghi, A.; Owens, L.; Heimann, K. Review of the Recombinant Human Interferon Gamma as an Immunotherapeutic: Impacts of Production Platforms and Glycosylation. J. Biotechnol. 2016, 240, 48–60. [Google Scholar] [CrossRef]
- Thiel, D.J.; le Du, M.-H.; Walter, R.L.; D’Arcy, A.; Chène, C.; Fountoulakis, M.; Garotta, G.; Winkler, F.K.; Ealick, S.E. Observation of an Unexpected Third Receptor Molecule in the Crystal Structure of Human Interferon-γ Receptor Complex. Structure 2000, 8, 927–936. [Google Scholar] [CrossRef]
- Ealick, S.E.; Cook, W.J.; Vijay-Kumar, S.; Carson, M.; Nagabhushan, T.L.; Trotta, P.P.; Bugg, C. Three-Dimensional Structure of Recombinant Human Interferon-γ. Science 1991, 252, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Manry, J.; Laval, G.; Patin, E.; Fornarino, S.; Tichit, M.; Bouchier, C.; Barreiro, L.B.; Quintana-Murci, L. Evolutionary Genetics Evidence of an Essential, Nonredundant Role of the IFN-γ Pathway in Protective Immunity. Human. Mutation 2011, 32, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Sikorski, K.; Chmielewski, S.; Przybyl, L.; Heemann, U.; Wesoly, J.; Baumann, M.; Bluyssen, H.A.R. STAT1-Mediated Signal Integration between IFNγ and LPS Leads to Increased EC and SMC Activation and Monocyte Adhesion. Am. J. Physiol.-Cell Physiol. 2011, 300, C1337–C1344. [Google Scholar] [CrossRef]
- Sikorski, K.; Chmielewski, S.; Olejnik, A.; Wesoly, J.Z.; Heemann, U.; Baumann, M.; Bluyssen, H. STAT1 as a Central Mediator of IFNγ and TLR4 Signal Integration in Vascular Dysfunction. JAK-STAT 2012, 1, 241–249. [Google Scholar] [CrossRef]
- Yu, X.-H.; Zhang, J.; Zheng, X.-L.; Yang, Y.-H.; Tang, C.-K. Interferon-γ in Foam Cell Formation and Progression of Atherosclerosis. Clin. Chim. Acta 2015, 441, 33–43. [Google Scholar] [CrossRef]
- Reiss, A.B.; Carsons, S.E.; Anwar, K.; Rao, S.; Edelman, S.D.; Zhang, H.; Fernandez, P.; Cronstein, B.N.; Chan, E.S.L. Atheroprotective Effects of Methotrexate on Reverse Cholesterol Transport Proteins and Foam Cell Transformation in Human THP-1 Monocyte/Macrophages. Arthritis Rheum. 2008, 58, 3675–3683. [Google Scholar] [CrossRef] [PubMed]
- Falvo, J.V.; Tsytsykova, A.V.; Goldfeld, A.E. Transcriptional Control of the TNF Gene. Curr. Dir. Autoimmun. 2010, 11, 27–60. [Google Scholar] [CrossRef] [PubMed]
- Grell, M.; Douni, E.; Wajant, H.; Löhden, M.; Clauss, M.; Maxeiner, B.; Georgopoulos, S.; Lesslauer, W.; Kollias, G.; Pfizenmaier, K.; et al. The Transmembrane Form of Tumor Necrosis Factor Is the Prime Activating Ligand of the 80 kDa Tumor Necrosis Factor Receptor. Cell 1995, 83, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Duerrschmid, C.; Crawford, J.R.; Reineke, E.; Taffet, G.E.; Trial, J.; Entman, M.L.; Haudek, S.B. TNF Receptor 1 Signaling Is Critically Involved in Mediating Angiotensin-II-Induced Cardiac Fibrosis. J. Mol. Cell. Cardiol. 2013, 57, 59–67. [Google Scholar] [CrossRef]
- Porter, K.E.; Turner, N.A.; O’Regan, D.J.; Ball, S.G. Tumor Necrosis Factor α Induces Human Atrial Myofibroblast Proliferation, Invasion and MMP-9 Secretion: Inhibition by Simvastatin. Cardiovasc. Res. 2004, 64, 507–515. [Google Scholar] [CrossRef]
- Brånén, L.; Hovgaard, L.; Nitulescu, M.; Bengtsson, E.; Nilsson, J.; Jovinge, S. Inhibition of Tumor Necrosis Factor-α Reduces Atherosclerosis in Apolipoprotein E Knockout Mice. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 2137–2142. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, X.; Bian, F.; Wu, P.; Xing, S.; Xu, G.; Li, W.; Chi, J.; Ouyang, C.; Zheng, T.; et al. TNF-α Promotes Early Atherosclerosis by Increasing Transcytosis of LDL across Endothelial Cells: Crosstalk between NF-κB and PPAR-γ. J. Mol. Cell. Cardiol. 2014, 72, 85–94. [Google Scholar] [CrossRef]
- Bakhet, M.; Ul-Haq, Z.; Kamalati, T.; Lucas, A.; Majeed, A.; El-Osta, A. Blood Tests in General Practice: The Use of Routine Data to Characterise Venous Blood Testing in North West London, 2016–2018. Br. J. Gen. Pract. 2020, 70, bjgp20X711605. [Google Scholar] [CrossRef]
- Cameron, S.J. Vascular Medicine. J. Am. Coll. Cardiol. 2015, 65, 2760–2763. [Google Scholar] [CrossRef]
- Bridgwood, B.M.; Sayers, R.D. Peripheral Artery Disease (PAD) in Primary Care-Educational Experiences for PAD Primary Care in England-a Mixed-Method Study. Fam. Pract. 2023, 40, 820–826. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Doenst, T.; Haverich, A.; Serruys, P.; Bonow, R.O.; Kappetein, P.; Falk, V.; Velazquez, E.; Diegeler, A.; Sigusch, H. PCI and CABG for Treating Stable Coronary Artery Disease: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 964–976. [Google Scholar] [CrossRef] [PubMed]
- Rockley, M.; Kobewka, D.; Kunkel, E.; Nagpal, S.; McIsaac, D.I.; Thavorn, K.; Forster, A. Characteristics of High-Cost Inpatients with Peripheral Artery Disease. J. Vasc. Surg. 2020, 72, 250–258.e8. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Buckley, L.; Sun, C.; Al Rifai, M.; Yu, B.; Nambi, V.; Virani, S.S.; Selvin, E.; Matsushita, K.; Hoogeveen, R.C.; et al. Association of Interleukin-6 and Interleukin-18 with Cardiovascular Disease in Older Adults: Atherosclerosis Risk in Communities Study. Eur. J. Prev. Cardiol. 2023, 30, 1731–1740. [Google Scholar] [CrossRef]
- Denegri, A.; Boriani, G. High Sensitivity C-Reactive Protein (hsCRP) and Its Implications in Cardiovascular Outcomes. Curr. Pharm. Des. 2021, 27, 263–275. [Google Scholar] [CrossRef]
- Jiang, W.; Huang, G.; Du, J.; Yang, H.; Zhou, S.; Dai, D.; Tang, K.; Fang, L.; Wang, X.; Deng, X. White Blood Cell Counts Can Predict 4-Year Cardiovascular Disease Risk in Patients with Stable Coronary Heart Disease: A Prospective Cohort Study. Front. Cardiovasc. Med. 2024, 11, 1358378. [Google Scholar] [CrossRef]

{kind=link}
| Patients with PAD (n = 465) | |
|---|---|
| Age, mean (SD) | 71 (10) |
| Female sex | 145 (31.1) |
| Hypertension | 394 (84.6) |
| Dyslipidemia | 383 (82.3) |
| Diabetes | 220 (47.2) |
| Chronic kidney disease | 216 (46.5) |
| Past smoking | 269 (57.9) |
| Current smoking | 110 (23.6) |
| Congestive heart failure | 22 (4.7) |
| Coronary artery disease | 181 (39.0) |
| Previous stroke | 92 (19.7) |
| Acetylsalicylic acid | 350 (75.3) |
| Statin | 322 (69.2) |
| ACE-I/ARB | 290 (62.4) |
| Patients with PAD (n = 465) | 1 Year of Follow-Up | 2 Years of Follow-Up |
|---|---|---|
| Major adverse cardiovascular event | 52 (11.2) | 84 (18.1) |
| Myocardial infarction | 45 (9.7) | 70 (15.0) |
| Stroke | 13 (2.8) | 22 (4.7) |
| Death | 3 (0.6) | 5 (1.2) |
| No MACE (n = 381) | MACE (n = 84) | p-Value | |
|---|---|---|---|
| IFN-γ | 33.85 (SD 12.46) pg/mL | 42.55 (SD 15.11) pg/mL | <0.001 |
| TNF-α | 4.65 (SD 4.29) pg/mL | 9.00 (SD 5.00) pg/mL | <0.001 |
| CXCL9 | 5.38 (SD 64.18) pg/mL | 75.99 (SD 65.14) pg/mL | 0.002 |
| MIP-1β | 15.67 (SD 16.93) pg/mL | 20.88 (SD 18.10) pg/mL | 0.009 |
| MIP-1δ | 17.98 (SD 4.01) pg/mL | 25.29 (SD 4.22) pg/mL | 0.026 |
| IL-6 | 6.72 (SD 38.98) pg/mL | 12.50 (SD 40.00) pg/mL | 0.035 |
| TARC | 298.95 (SD 426.3) pg/mL | 273.06 (SD 263.81) pg/mL | 0.562 |
| MIP-1a | 2.85 (SD 2.21) pg/mL | 2.96 (SD 2.11) pg/mL | 0.640 |
| MCP-1 | 652.15 (SD 1051.28) pg/mL | 606.93 (SD 849.17) pg/mL | 0.694 |
| CCL1 | 2.84 (SD 3.05) pg/mL | 2.74 (SD 1.4) pg/mL | 0.763 |
| CXCL16 | 12.21 (SD 11.51) pg/mL | 12.03 (SD 10.71) pg/mL | 0.897 |
| Eotaxin | 122.91 (SD 179.21) pg/mL | 125.44 (SD 59.97) pg/mL | 0.893 |
| Resistin | 4.27 (SD 5.35) pg/mL | 4.33 (SD 4.88) pg/mL | 0.912 |
| CD163 | 119.75 (SD 170.21) pg/mL | 121.24 (SD 163.75) pg/mL | 0.942 |
| Progranulin | 17.23 (SD 29.31) pg/mL | 171.13 (SD 19.90) pg/mL | 0.970 |
| Adjusted Hazard Ratio (95% CI) | p-Value | |
|---|---|---|
| TNF-α | 1.66 (1.28–2.33) | 0.001 |
| IFN-γ | 1.25 (1.12–2.29) | 0.033 |
| CXCL9 | 1.01 (0.93–1.07) | 0.367 |
| MCP-1 | 1.13 (0.91–1.20) | 0.408 |
| MIP-1a | 1.29 (0.64–1.38) | 0.423 |
| CCL1 | 1.19 (0.96–1.30) | 0.674 |
| MIP-1δ | 1.02 (0.86–1.19) | 0.680 |
| MIP-1β | 1.10 (0.83–1.19) | 0.687 |
| IL-6 | 1.18 (0.63–1.27) | 0.718 |
| Eotaxin | 0.92 (0.76–1.37) | 0.728 |
| CXCL16 | 1.19 (0.72–1.37) | 0.742 |
| Progranulin | 1.17 (0.83–1.30) | 0.797 |
| TARC | 1.12 (0.95–1.26) | 0.811 |
| CD163 | 1.18 (0.96–1.30) | 0.871 |
| Resistin | 0.94 (0.76–1.11) | 0.885 |
| Importance Score | 95% CI | p-Value | |
|---|---|---|---|
| IFN-γ | 0.19 | (0.17–0.21) | 0.001 |
| TNF-α | 0.15 | (0.13–0.18) | 0.002 |
| MIP-1δ | 0.15 | (0.13–0.17) | 0.231 |
| MIP-1β | 0.15 | (0.11–0.16) | 0.235 |
| CD163 | 0.14 | (0.12–0.18) | 0.244 |
| IL-6 | 0.14 | (0.10–0.19) | 0.002 |
| Resistin | 0.13 | (0.10–0.15) | 0.002 |
| CXCL9 | 0.13 | (0.11–0.15) | 0.270 |
| MCP-1 | 0.12 | (0.10–0.14) | 0.306 |
| Eotaxin | 0.10 | (0.08–0.12) | 0.370 |
| CCL1 | 0.09 | (0.07–0.11) | 0.391 |
| TARC | 0.08 | (0.06–0.10) | 0.447 |
| Progranulin | 0.08 | (0.06–0.10) | 0.468 |
| CXCL16 | 0.06 | (0.04–0.08) | 0.537 |
| MIP-1a | 0.06 | (0.04–0.08) | 0.550 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, B.; Lindner, E.; Abuhalimeh, R.; Shaikh, F.; Younes, H.; Abuhalimeh, B.; Zamzam, A.; Abdin, R.; Qadura, M. Interferon Gamma and Tumor Necrosis Factor Alpha Are Inflammatory Biomarkers for Major Adverse Cardiovascular Events in Patients with Peripheral Artery Disease. Biomedicines 2025, 13, 1586. https://doi.org/10.3390/biomedicines13071586
Li B, Lindner E, Abuhalimeh R, Shaikh F, Younes H, Abuhalimeh B, Zamzam A, Abdin R, Qadura M. Interferon Gamma and Tumor Necrosis Factor Alpha Are Inflammatory Biomarkers for Major Adverse Cardiovascular Events in Patients with Peripheral Artery Disease. Biomedicines. 2025; 13(7):1586. https://doi.org/10.3390/biomedicines13071586
Chicago/Turabian StyleLi, Ben, Eva Lindner, Raghad Abuhalimeh, Farah Shaikh, Houssam Younes, Batool Abuhalimeh, Abdelrahman Zamzam, Rawand Abdin, and Mohammad Qadura. 2025. "Interferon Gamma and Tumor Necrosis Factor Alpha Are Inflammatory Biomarkers for Major Adverse Cardiovascular Events in Patients with Peripheral Artery Disease" Biomedicines 13, no. 7: 1586. https://doi.org/10.3390/biomedicines13071586
APA StyleLi, B., Lindner, E., Abuhalimeh, R., Shaikh, F., Younes, H., Abuhalimeh, B., Zamzam, A., Abdin, R., & Qadura, M. (2025). Interferon Gamma and Tumor Necrosis Factor Alpha Are Inflammatory Biomarkers for Major Adverse Cardiovascular Events in Patients with Peripheral Artery Disease. Biomedicines, 13(7), 1586. https://doi.org/10.3390/biomedicines13071586