
Ten-Second Cold Water Stress Test Differentiates Parkinson’s Disease from Multiple System Atrophy: A Cross-Sectional Pilot Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ten-Second Cold Water Stress Test (10sec-CWST)
2.3. Statistical Analysis
3. Results
3.1. Patients’ Background Data
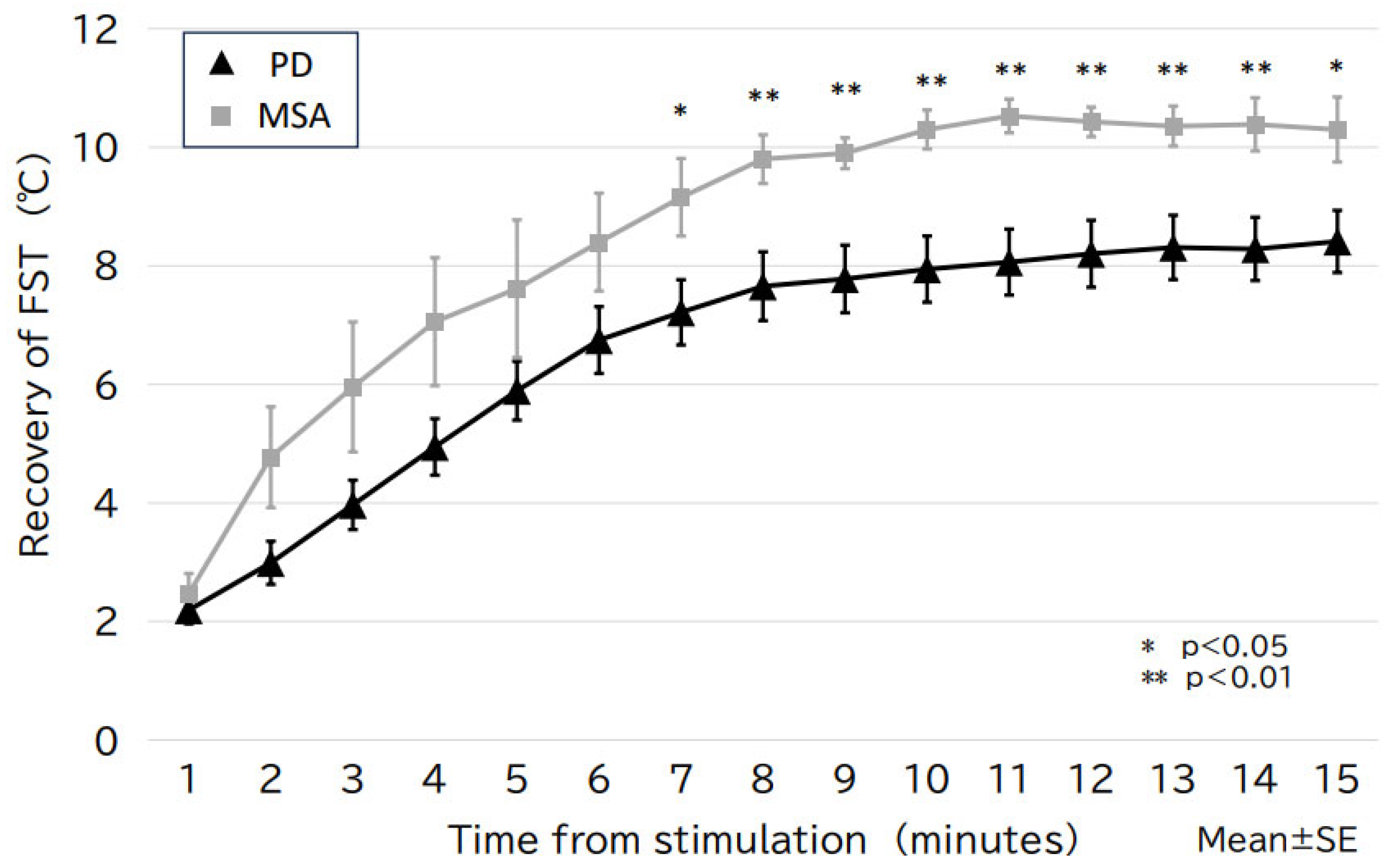
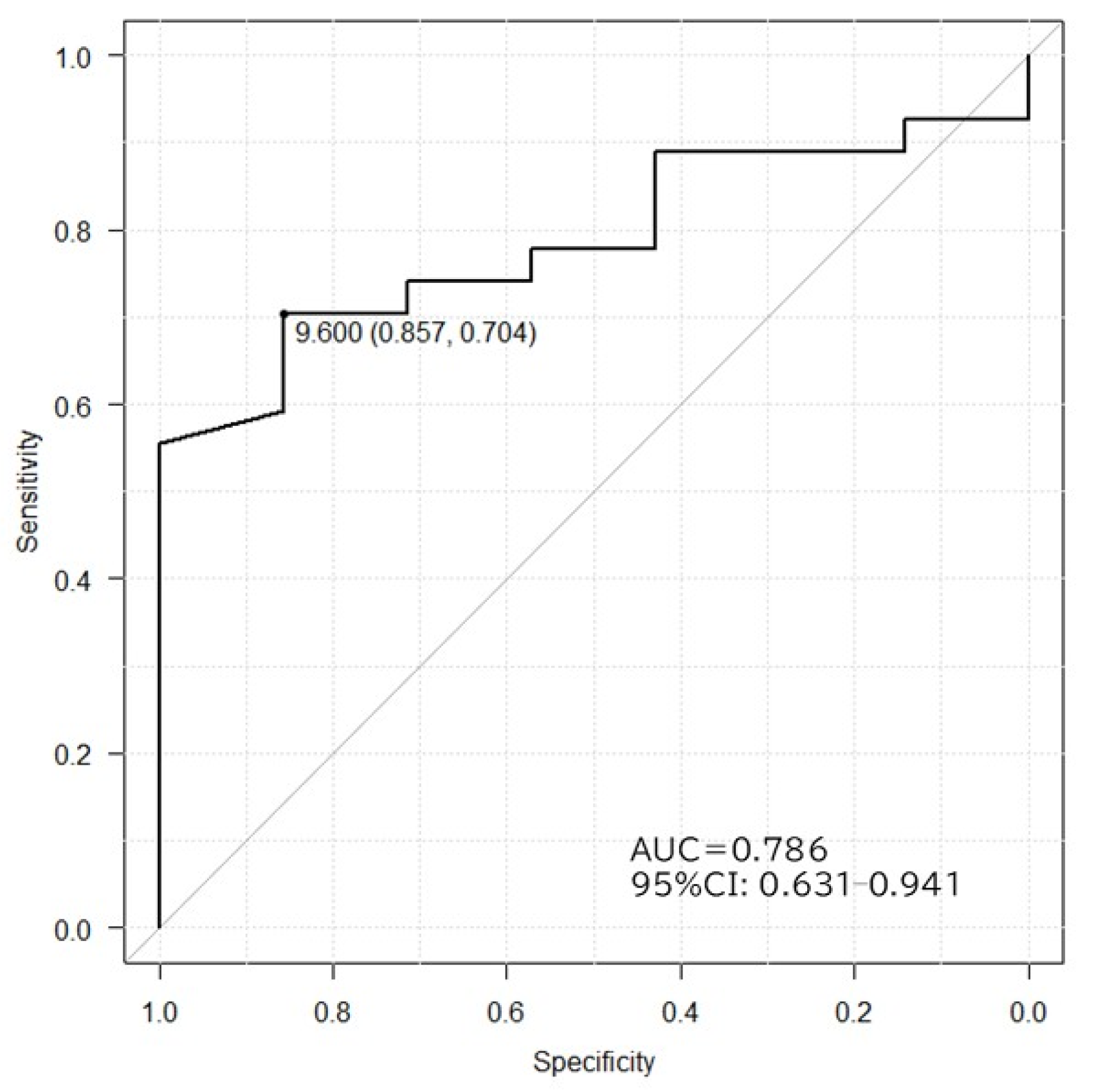
3.2. Change in FST After 10sec-CWST
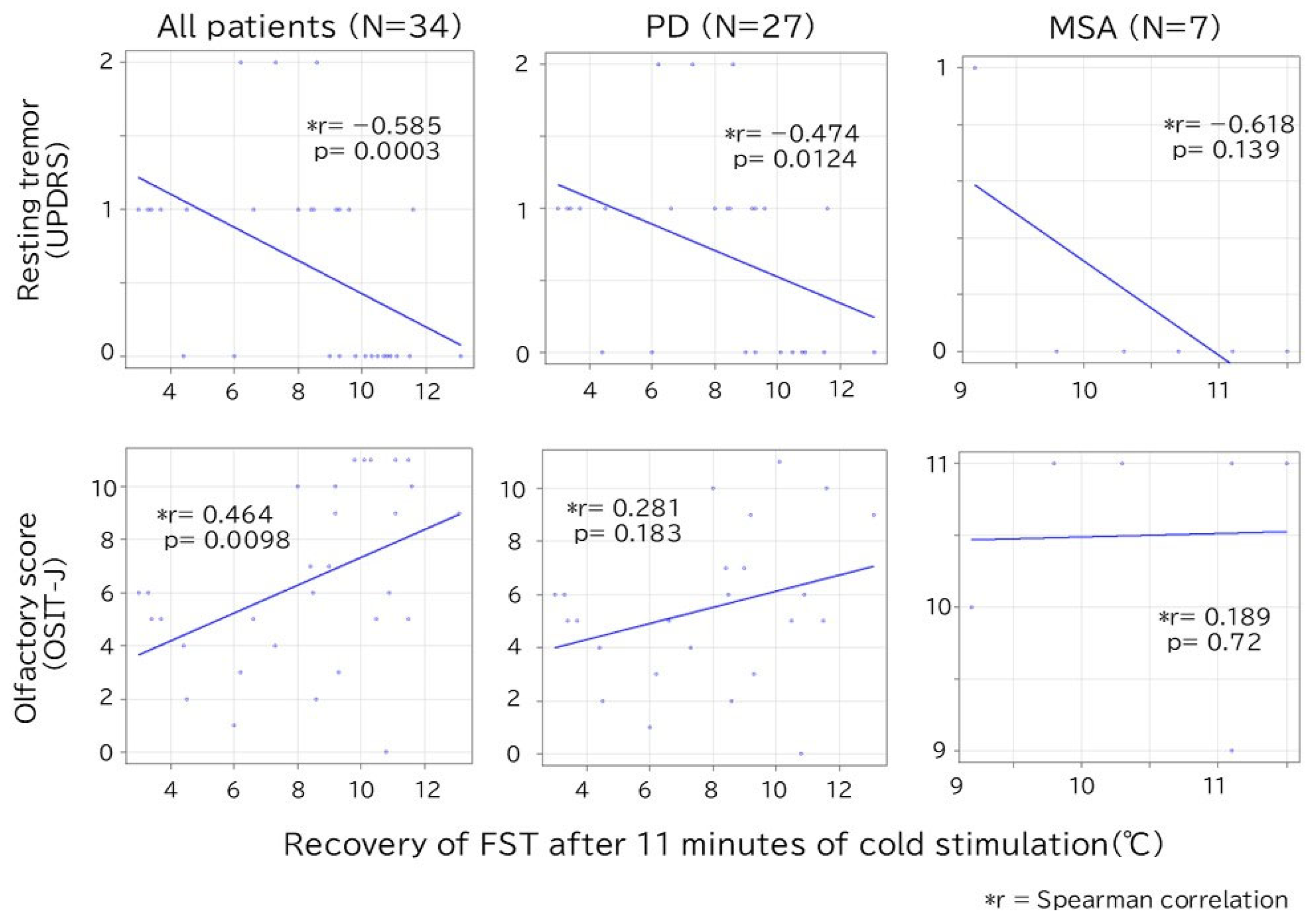
3.3. Factors Related to the Change in FST
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PD | Parkinson’s disease |
| MSA | Multiple system atrophy |
| FST | Finger surface temperature |
| 10sec-CWST | 10 s cold water stress test |
| ANS | Autonomic nervous system |
| MIBG | Metaiodobenzylguanidine |
| OSIT-J | Odor stick identification test for the Japanese |
| LEDD | Levodopa equivalent daily dose |
| RBD | REM sleep behavior disorder |
| OH | Orthostatic hypotension |
| L-dopa | Levodopa |
| DRT | Dopamine replacement therapy |
References
- Kalia, L.V.; Lang, A.E. Parkinson’s disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef] [PubMed]
- Morris, H.R.; Spillantini, M.G.; Sue, C.M.; Williams-Gray, C.H. The pathogenesis of Parkinson’s disease. Lancet 2024, 403, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Erro, M.E.; Arrondo, P.; Gaston, I.; Clavero, P.; Sanchez Rulz de Grodoa, J.; Marti Andres, G.; Valenti, R.; Delfrade, J.; Vincente, E. Epidemiologic and clinical features of multisystem atrophy: A population-based study in Navarre, Spain. J. Neurol. 2024, 271, 6647–6654. [Google Scholar] [CrossRef]
- Wenning, G.K.; Stankovic, I.; Vignatelli, L.; Fanciulli, A.; Calandra-Buonaura, G.; Seppi, K.; Palma, J.A.; Meissner, W.G.; Krismer, F.; Berg, D.; et al. The Movement Disorder Society criteria for the diagnosis of multiple system atrophy. Mov. Disord. 2022, 37, 1131–1148. [Google Scholar] [CrossRef]
- Miki, Y.; Tsushima, E.; Foti, S.C.; Strand, K.M.; Asi, Y.T.; Yamamoto, A.K.; Bettencourt, C.; Oliveira, M.C.B.; De Pablo-Fernández, E.; Jaunmuktane, Z.; et al. Identification of multiple system atrophy mimicking Parkinson’s disease or progressive supranuclear palsy. Brain 2021, 144, 1138–1151. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Hashimoto, M.; Yoshioka, M.; Murakami, M.; Kawasaki, K.; Urashima, M. The odor stick identification test for Japanese differentiates Parkinson’s disease from multiple system atrophy and progressive supra nuclear palsy. BMC Neurol. 2011, 11, 157. [Google Scholar] [CrossRef]
- Coon, E.A.; Cutsforth-Gregory, J.K.; Benarroch, E.E. Neuropathology of autonomic dysfunction in synucleinopathies. Mov. Disord. 2018, 33, 349–358. [Google Scholar] [CrossRef]
- Takahashi, M.; Ikemura, M.; Oka, T.; Uchihara, T.; Wakabayashi, K.; Kakita, A.; Takahashi, H.; Yoshida, M.; Toru, S.; Kobayashi, T.; et al. Quantitative correlation between cardiac MIBG uptake and remaining axons in the cardiac sympathetic nerve in lewy body disease. J. Neurol. Neurosurg. Psychiatry 2015, 86, 939–944. [Google Scholar] [CrossRef]
- Orimo, S.; Suzuki, M.; Inaba, A.; Mizusawa, H. 123I-MIBG myocardial scintigraphy for differentiating Parkinson’s disease from other neurodegenerative parkinsonism: A systematic review and meta-analysis. Park. Relat. Disord. 2012, 18, 494–500. [Google Scholar] [CrossRef]
- Orimo, S.; Kanazawa, T.; Nakamura, A.; Uchihara, T.; Mori, F.; Kakita, A.; Wakabayashi, K.; Takahashi, H. Degeneration of cardiac sympathetic nerve can occur in multiple system atrophy. Acta Neuropathol. 2007, 113, 81–86. [Google Scholar] [CrossRef]
- Zeng, J.; Xing, Y.; Mei, S.; Xu, B.; Xue, X.; Song, H.; Xu, E. The differences of orthostatic hypotension in patients with Parkinson’s disease and multiple system atrophy. Front. Neurol. 2023, 14, 1070943. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, R.; Hattori, T.; Uchiyama, T.; Yamanishi, T. Videourodynamic and sphincter motor unit potential analyses in Parkinson’s disease and multiple system atrophy. J. Neurol. Neurosurg. Psychiatry 2001, 71, 600–606. [Google Scholar] [CrossRef]
- Antonio-Rubio, I.; Madrid-Navarro, C.J.; Salazar-López, E.; Pérez-Navarro, M.J.; Sáez-Zea, C.; Gómez-Milán, E.; Mínguez-Castellanos, A.; Escamilla-Sevilla, F. Abnormal thermography in Parkinson’s disease. Park. Relat. Disord. 2015, 21, 852–857. [Google Scholar] [CrossRef]
- Sousa, E.; Vardasca, R.; Teixeira, S.; Seixas, A.; Mendes, J.; Costa-Ferreira, A. A review on the application of medical infrared thermal imaging in hands. Infrared Phys. 2017, 85, 315–323. [Google Scholar] [CrossRef]
- Asahina, M.; Low, D.A.; Mathias, C.J.; Fujinuma, Y.; Katagiri, A.; Yamanaka, Y.; Shimada, J.; Poudel, A.; Kuwabara, S. Skin temperature of the hand in multiple system atrophy and Parkinson’s disease. Park. Relat. Disord. 2013, 19, 560–562. [Google Scholar] [CrossRef] [PubMed]
- Augustis, S.; Saferis, V.; Jost, W.H. Autonomic disturbances including impaired hand thermoregulation in multiple system atrophy and Parkinson’s disease. J. Neural Transm. 2017, 124, 965–972. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Gilman, S.; Wenning, G.K.; Low, P.A.; Brooks, D.J.; Mathias, C.J.; Trojanowski, J.Q.; Wood, N.W.; Colosimo, C.; Dürr, A.; Fowler, C.J.; et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology 2008, 71, 670–676. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Roy, S.; Srivastava, A.K.; Jaryal, A.K.; Deepak, K.K. Cardiovascular responses during cold pressor test are different in Parkinson disease and multiple system atrophy with parkinsonism. Clin. Auton. Res. 2015, 25, 219–224. [Google Scholar] [CrossRef]
- Shindo, K.; Kobayashi, F.; Miwa, M.; Nagasaka, T.; Takiyama, Y.; Shiozawa, Z. Temporal prolongation of decreased skin blood flow causes cold limbs in Parkinson’s disease. J. Neural Transm. 2013, 120, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Shindo, K.; Tsuchiya, M.; Ichinose, Y.; Koh, K.; Hata, T.; Yamashiro, N.; Kobayashi, F.; Nagasaka, T.; Takiyama, Y. Vasomotor regulation in patients with multiple system atrophy. J. Neural Transm. 2017, 124, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; McDermott, M.; Carter, J.; Gauthier, S.; Goetz, C.; Golbe, L.; Huber, S.; Koller, W.; Olanow, C.; Shoulson, I. Variable expression of Parkinson’s disease: A baseline analysis of the DATATOP cohort. The Parkinson Study Group. Neurology 1990, 40, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
- Burn, D.J.; Rowan, E.N.; Allan, L.M.; Molloy, S.; O’Brien, J.T.; McKeith, I.G. Motor subtype and cognitive decline in Parkinson’s disease, Parkinson’s disease with dementia, and dementia with Lewy bodies. J. Neurol. Neurosurg. Psychiatry 2006, 77, 585–589. [Google Scholar] [CrossRef]
- Gu, S.C.; Shi, R.; Gao, C.; Yuan, X.L.; Wu, Y.; Liu, Z.G.; Wang, C.D.; Zhao, S.R.; Chen, X.; Yuan, C.X.; et al. Autonomic function and motor subtypes in Parkinson’s disease: A multicentre cross-sectional study. Sci. Rep. 2023, 13, 14548. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unit | PD (n = 27) | MSA (n = 7) | p | |
|---|---|---|---|---|
| MSA-C/P (5/2) | ||||
| Male–female | N | 10:17 | 02:05 | 1.000 |
| Age (mean) (range) | year | 69.4 (41–88) | 61.9 (52–78) | 0.088 |
| Disease duration (mean) (range) | year | 6.1 (1–17) | 3 (1–5) | 0.090 |
| Hohen–Yahr stage (mean) (range) | - | 2.8 (1–4) | 3 (2–4) | 0.604 |
| Resting tremor * (mean) (range) | - | 0.7 (0–2) | 0.1 (0–1) | 0.039 |
| Rigidity * (mean) (range) | - | 1.6 (1–2) | 1.0 (0–2) | 0.057 |
| RBD | N | 9 | 2 | 1.000 |
| OH | N | 6 | 4 | 0.157 |
| Constipation | N | 20 | 5 | 1.000 |
| Tachyuria | N | 15 | 2 | 0.398 |
| Dysuria | N | 0 | 4 | 0.157 |
| Dyshidrosis | N | 8 | 1 | 0.644 |
| Chilblains | N | 1 | 0 | 1.000 |
| OSIT-J (mean) (range) | - | 5.5 (1–11) | 10.5 (9–11) | 0.001 |
| MIBG early (mean) (range) | H/M | 1.92 (1.23–3.28) | 3.22 (3.07–3.52) | 0.009 |
| MIBG delay (mean) (range) | H/M | 1.63 (1.02–2.85) | 2.76 (2.63–2.93) | 0.009 |
| L-dopa (mean) (range) | mg/day | 321.3 (0–800) | 78.57 (0–450) | 0.029 |
| LEDD (mean) (range) | mg/day | 472.35 (0–1440) | 90 (0–450) | 0.018 |
| FST (mean) (range) | °C | 32.9 (26.4–36.7) | 34.8(34.4–35.4) | 0.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, M.; Hagiwara, W.; Itaya, S.; Abe, K.; Maeda, T.; Inaba, A.; Orimo, S. Ten-Second Cold Water Stress Test Differentiates Parkinson’s Disease from Multiple System Atrophy: A Cross-Sectional Pilot Study. Biomedicines 2025, 13, 1585. https://doi.org/10.3390/biomedicines13071585
Takahashi M, Hagiwara W, Itaya S, Abe K, Maeda T, Inaba A, Orimo S. Ten-Second Cold Water Stress Test Differentiates Parkinson’s Disease from Multiple System Atrophy: A Cross-Sectional Pilot Study. Biomedicines. 2025; 13(7):1585. https://doi.org/10.3390/biomedicines13071585
Chicago/Turabian StyleTakahashi, Makoto, Wataru Hagiwara, Sakiko Itaya, Keisuke Abe, Tetsuya Maeda, Akira Inaba, and Satoshi Orimo. 2025. "Ten-Second Cold Water Stress Test Differentiates Parkinson’s Disease from Multiple System Atrophy: A Cross-Sectional Pilot Study" Biomedicines 13, no. 7: 1585. https://doi.org/10.3390/biomedicines13071585
APA StyleTakahashi, M., Hagiwara, W., Itaya, S., Abe, K., Maeda, T., Inaba, A., & Orimo, S. (2025). Ten-Second Cold Water Stress Test Differentiates Parkinson’s Disease from Multiple System Atrophy: A Cross-Sectional Pilot Study. Biomedicines, 13(7), 1585. https://doi.org/10.3390/biomedicines13071585