
Three-Month Durability of Bilateral Two-Level Stellate Ganglion Blocks for Traumatic Brain Injury: A Retrospective Analysis

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TBI | Traumatic Brain Injury |
| NSI | Neurobehavioral Symptom Inventory |
| 2LCSB | Two-level cervical sympathetic chain block |
| SGB | Stellate ganglion block |
| BBB | Blood–brain barrier |
| RCT | Randomized controlled trial |
| PTSD | Posttraumatic stress disorder |
| GCS | Glasgow Coma Scale |
| HBOT | Hyperbaric Oxygen Therapy |
| IQR | Interquartile Range |
| BL | Baseline |
| 1W | 1-week |
| 1M | 1-month |
| 2M | 2-month |
| 3M | 3-month |
References
- Brain Trauma Foundation Brain Trauma Foundation—Frequently Asked Questions (FAQ). Available online: https://braintrauma.org/info/faq (accessed on 13 March 2025).
- CDC Multiple Cause of Death Data on CDC WONDER. Available online: https://wonder.cdc.gov/mcd.html (accessed on 13 March 2025).
- Karamian, A.; Lucke-Wold, B.; Seifi, A. Prevalence of Traumatic Brain Injury in the General Adult Population of the USA: A Meta-Analysis. Neuroepidemiology 2024, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Schiller, J.S.; Lucas, J.W.; Ward, B.W.; Peregoy, J.A. Summary health statistics for U.S. adults: National Health Interview Survey, 2010. Vital Health Stat. 2012, 10, 1–207. [Google Scholar]
- Coronado, V.G.; McGuire, L.C.; Sarmiento, K.; Bell, J.; Lionbarger, M.R.; Jones, C.D.; Geller, A.I.; Khoury, N.; Xu, L. Trends in Traumatic Brain Injury in the U.S. And the Public Health Response: 1995–2009. J. Saf. Res. 2012, 43, 299–307. [Google Scholar] [CrossRef]
- Bhattrai, A.; Irimia, A.; Van Horn, J.D. Neuroimaging of Traumatic Brain Injury in Military Personnel: An Overview. J. Clin. Neurosci. 2019, 70, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Reger, M.A.; Brenner, L.A.; du Pont, A. Traumatic Brain Injury and Veteran Mortality after the War in Afghanistan. JAMA Netw. Open 2022, 5, e2148158. [Google Scholar] [CrossRef] [PubMed]
- Selassie, A.W.; Wilson, D.A.; Pickelsimer, E.E.; Voronca, D.C.; Williams, N.R.; Edwards, J.C. Incidence of Sport-Related Traumatic Brain Injury and Risk Factors of Severity: A Population-Based Epidemiologic Study. Ann. Epidemiol. 2013, 23, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Covassin, T.; Moran, R.; Elbin, R.J. Sex Differences in Reported Concussion Injury Rates and Time Loss from Participation: An Update of the National Collegiate Athletic Association Injury Surveillance Program from 2004–2005 through 2008–2009. J. Athl. Train. 2016, 51, 189–194. [Google Scholar] [CrossRef]
- Brenner, L.A.; Forster, J.E.; Gradus, J.L.; Hostetter, T.A.; Hoffmire, C.A.; Walsh, C.G.; Larson, M.J.; Stearns-Yoder, K.A.; Adams, R.S. Associations of Military-Related Traumatic Brain Injury with New-Onset Mental Health Conditions and Suicide Risk. JAMA Netw. Open 2023, 6, e2326296. [Google Scholar] [CrossRef]
- Hoge, C.W.; McGurk, D.; Thomas, J.L.; Cox, A.L.; Engel, C.C.; Castro, C.A. Mild Traumatic Brain Injury in U.S. Soldiers Returning from Iraq. N. Engl. J. Med. 2008, 358, 453–463. [Google Scholar] [CrossRef]
- Haydel, M.J. Evaluation of Traumatic Brain Injury, Acute—Differential Diagnosis of Symptoms | BMJ Best Practice. Available online: https://bestpractice.bmj.com/topics/en-us/515 (accessed on 13 March 2025).
- Teasdale, G.; Jennett, B. Assessment of Coma and Impaired Consciousness. Lancet 1974, 304, 81–84. [Google Scholar] [CrossRef]
- Foulkes, M.A.; Eisenberg, H.M.; Jane, J.A.; Marmarou, A.; Marshall, L.F. The Traumatic Coma Data Bank: Design, Methods, and Baseline Characteristics. J. Neurosurg. 1991, 75, S8–S13. [Google Scholar] [CrossRef]
- Malec, J.F.; Brown, A.W.; Leibson, C.L.; Flaada, J.T.; Mandrekar, J.N.; Diehl, N.N.; Perkins, P.K. The Mayo Classification System for Traumatic Brain Injury Severity. J. Neurotrauma 2007, 24, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Bodien, Y.G.; Barra, A.; Temkin, N.R.; Barber, J.; Foreman, B.; Vassar, M.; Robertson, C.; Taylor, S.R.; Markowitz, A.J.; Manley, G.T.; et al. Diagnosing Level of Consciousness: The Limits of the Glasgow Coma Scale Total Score. J. Neurotrauma 2021, 38, 3295–3305. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.Y.; Lee, A.Y.W. Traumatic Brain Injuries: Pathophysiology and Potential Therapeutic Targets. Front. Cell. Neurosci. 2019, 13, 528. [Google Scholar] [CrossRef]
- Laskowitz, D.; Grant, G. Translational Research in Traumatic Brain Injury; CRC Press: Boca Raton, FL, USA, 2016; Chapter 3; ISBN 9781466584914. [Google Scholar]
- Tang-Schomer, M.D.; Patel, A.R.; Baas, P.W.; Smith, D.H. Mechanical Breaking of Microtubules in Axons during Dynamic Stretch Injury Underlies Delayed Elasticity, Microtubule Disassembly, and Axon Degeneration. FASEB J. 2010, 24, 1401–1410. [Google Scholar] [CrossRef]
- Smith, D.H.; Stewart, W. Tackling Concussion, beyond Hollywood. Lancet Neurol. 2016, 15, 662–663. [Google Scholar] [CrossRef]
- Barbier, P.; Zejneli, O.; Martinho, M.; Lasorsa, A.; Belle, V.; Smet-Nocca, C.; Tsvetkov, P.O.; Devred, F.; Landrieu, I. Role of Tau as a Microtubule-Associated Protein: Structural and Functional Aspects. Front. Aging Neurosci. 2019, 11, 204. [Google Scholar] [CrossRef]
- Mudher, A.; Colin, M.; Dujardin, S.; Medina, M.; Dewachter, I.; Alavi Naini, S.M.; Mandelkow, E.-M.; Mandelkow, E.; Buée, L.; Goedert, M.; et al. What Is the Evidence That Tau Pathology Spreads through Prion-like Propagation? Acta Neuropathol. Commun. 2017, 5, 99. [Google Scholar] [CrossRef]
- Marklund, N.; Vedung, F.; Lubberink, M.; Tegner, Y.; Johansson, J.; Blennow, K.; Zetterberg, H.; Fahlström, M.; Haller, S.; Stenson, S.; et al. Tau Aggregation and Increased Neuroinflammation in Athletes after Sports-Related Concussions and in Traumatic Brain Injury Patients—A PET/MR Study. NeuroImage Clin. 2021, 30, 102665. [Google Scholar] [CrossRef]
- McKee, A.C.; Cairns, N.J.; Dickson, D.W.; Folkerth, R.D.; Dirk Keene, C.; Litvan, I.; Perl, D.P.; Stein, T.D.; Vonsattel, J.-P.; Stewart, W.; et al. The First NINDS/NIBIB Consensus Meeting to Define Neuropathological Criteria for the Diagnosis of Chronic Traumatic Encephalopathy. Acta Neuropathol. 2015, 131, 75–86. [Google Scholar] [CrossRef]
- Leibson, C.L.; Brown, A.W.; Ransom, J.E.; Diehl, N.N.; Perkins, P.K.; Mandrekar, J.; Malec, J.F. Incidence of Traumatic Brain Injury across the Full Disease Spectrum. Epidemiology 2011, 22, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Permenter, C.M.; Fernández-de Thomas, R.J.; Sherman, A.L. Postconcussive Syndrome. Available online: https://www.ncbi.nlm.nih.gov/books/NBK534786/ (accessed on 13 March 2025).
- Rabinowitz, A.R.; Watanabe, T.K. Pharmacotherapy for Treatment of Cognitive and Neuropsychiatric Symptoms after MTBI. J. Head Trauma Rehabil. 2020, 35, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Min, J.H.; Shin, Y.-I. Treatment and Rehabilitation for Traumatic Brain Injury: Current Update. Brain Neurorehabilit. 2022, 15, e14. [Google Scholar] [CrossRef]
- Sergeyenko, Y.; Andreae, M.E.; Segal, M. Diagnosis and Management of Mild Traumatic Brain Injury (MTBI): A Comprehensive, Patient-Centered Approach. Curr. Pain Headache Rep. 2025, 29, 19. [Google Scholar] [CrossRef] [PubMed]
- Daly, S.; Thorpe, M.; Rockswold, S.; Hubbard, M.; Bergman, T.; Samadani, U.; Rockswold, G. Hyperbaric Oxygen Therapy in the Treatment of Acute Severe Traumatic Brain Injury: A Systematic Review. J. Neurotrauma 2018, 35, 623–629. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, X.; Wu, Z.; Yin, G.; Chu, H.; Zhao, P. HBOT Has a Better Cognitive Outcome than NBH for Patients with Mild Traumatic Brain Injury: A Randomized Controlled Clinical Trial. Medicine 2023, 102, e35215. [Google Scholar] [CrossRef]
- Hadanny, A.; Maroon, J.C.; Efrati, S. The Efficacy of Hyperbaric Oxygen Therapy in Traumatic Brain Injury Patients: Literature Review and Clinical Guidelines. Med. Res. Arch. 2023, 11, 1–33. [Google Scholar] [CrossRef]
- Fann, J.R.; Quinn, D.K.; Hart, T. Treatment of Psychiatric Problems after Traumatic Brain Injury. Biol. Psychiatry 2021, 91, 508–521. [Google Scholar] [CrossRef]
- Galimberti, A.; Tik, M.; Pellegrino, G.; Schuler, A.-L. Effectiveness of RTMS and TDCS Treatment for Chronic TBI Symptoms: A Systematic Review and Meta-Analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2024, 128, 110863. [Google Scholar] [CrossRef]
- Heslot, C.; Azouvi, P.; Perdrieau, V.; Granger, A.; Lefèvre-Dognin, C.; Cogné, M. A Systematic Review of Treatments of Post-Concussion Symptoms. J. Clin. Med. 2022, 11, 6224. [Google Scholar] [CrossRef]
- Lipov, E.; Kelzenberg, B. Sympathetic System Modulation to Treat Post-Traumatic Stress Disorder (PTSD): A Review of Clinical Evidence and Neurobiology. J. Affect. Disord. 2012, 142, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lebovits, A.H.; Yarmush, J.; Lefkowitz, M. Reflex Sympathetic Dystrophy and Posttraumatic Stress Disorder. Clin. J. Pain 1990, 6, 153–157. [Google Scholar] [CrossRef]
- Mulvaney, S.; Mahadevan, S.; Dineen, K.; Desronvilles, R.; Rae Olmsted, K.L. Long-Term Durability of Bilateral Two-Level Stellate Ganglion Blocks in Posttraumatic Stress Disorder: A Six-Month Retrospective Analysis. Clin. Transl. Neurosci. 2025, 9, 7. [Google Scholar] [CrossRef]
- Blakey, S.M.; Rae Olmsted, K.L.; Hirsch, S.; Asman, K.; Wallace, D.; Olmsted, M.G.; Vandermaas-Peeler, R.; Karg, R.S.; Walters, B.B. Differential Posttraumatic Stress Disorder Symptom Cluster Response to Stellate Ganglion Block: Secondary Analysis of a Randomized Controlled Trial. Transl. Psychiatry 2024, 14, 1–8. [Google Scholar] [CrossRef]
- Prasad, S.; Jain, N.; Umar, T.P.; Radenkov, I.; Ahmed, S.K.; Sakagianni, V.; Kollia, S.; Hingora, M.J.; Kumari, N.; Akbari, A.R.; et al. Sympathetic Nerve Blocks for Posttraumatic Stress Disorder: An Evidentiary Review for Future Clinical Trials. Front. Psychiatry 2023, 14, 1309986. [Google Scholar] [CrossRef]
- Peterson, A.L.; Straud, C.L.; Young-McCaughan, S.; McCallin, J.P.; Hoch, M.; Roux, N.P.; Koch, L.; Lara-Ruiz, J.; Roache, J.D.; Hein, J.M.; et al. Combining a Stellate Ganglion Block with Prolonged Exposure Therapy for Posttraumatic Stress Disorder: A Nonrandomized Clinical Trial. J. Trauma. Stress 2022, 35, 1801–1809. [Google Scholar] [CrossRef]
- Rae Olmsted, K.L.; Bartoszek, M.; Mulvaney, S.; McLean, B.; Turabi, A.; Young, R.; Kim, E.; Vandermaas-Peeler, R.; Morgan, J.K.; Constantinescu, O.; et al. Effect of Stellate Ganglion Block Treatment on Posttraumatic Stress Disorder Symptoms. JAMA Psychiatry 2020, 77, 130. [Google Scholar] [CrossRef]
- McLean, B. Safety and Patient Acceptability of Stellate Ganglion Blockade as a Treatment Adjunct for Combat-Related Post-Traumatic Stress Disorder: A Quality Assurance Initiative. Cureus 2015, 7, e320. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, M.; Reddy, V.; Singh, P. Neuroanatomy, Stellate Ganglion; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Moore, D.C. Stellate Ganglion Block: Techniques, Indications, Uses; Thomas: Seoul, Republic of Korea, 1954. [Google Scholar]
- Baek, J.H. Characteristics of the Middle Cervical Sympathetic Ganglion: A Systematic Review and Meta-Analysis. Pain Physician 2018, 1, 9–18. [Google Scholar] [CrossRef]
- Lipov, E.G.; Jacobs, R.; Springer, S.; Candido, K.D.; Knezevic, N.N. Utility of Cervical Sympathetic Block in Treating Post-Traumatic Stress Disorder in Multiple Cohorts: A Retrospective Analysis. PubMed 2022, 25, 77–85. [Google Scholar]
- Mulvaney, S.W.; Lynch, J.H.; Kotwal, R.S. Clinical Guidelines for Stellate Ganglion Block to Treat Anxiety Associated with Posttraumatic Stress Disorder. J. Spec. Oper. Med. 2015, 15, 79. [Google Scholar] [CrossRef] [PubMed]
- Mulvaney, S.W.; Lynch, J.H.; Curtis, K.E.; Ibrahim, T.S. The Successful Use of Left-Sided Stellate Ganglion Block in Patients That Fail to Respond to Right-Sided Stellate Ganglion Block for the Treatment of Post-Traumatic Stress Disorder Symptoms: A Retrospective Analysis of 205 Patients. Mil. Med. 2021, 187, e826–e829. [Google Scholar] [CrossRef] [PubMed]
- Mulvaney, S.W.; Dineen, K.J.; Mahadevan, S.; Desronvilles, R.; Rae Olmsted, K.L. Three-Month Durability of Bilateral Two-Level Stellate Ganglion Blocks in Patients with Generalized Anxiety Disorder: A Retrospective Analysis. Brain Sci. 2025, 15, 188. [Google Scholar] [CrossRef]
- Mulvaney, S.W.; Lynch, J.H.; Rae, K.L.; Mahadevan, S.; Dineen, K.J. The Successful Use of Bilateral 2-Level Ultrasound-Guided Stellate Ganglion Block to Improve Traumatic Brain Injury Symptoms: A Retrospective Analysis of 23 Patients. Mil. Med. 2024, 10, e2573–e2577. [Google Scholar] [CrossRef]
- Meyers, J.E.; English, J.; Miller, R.M.; Lee, A.J. Normative Data for the Neurobehavioral Symptom Inventory. Appl. Neuropsychol. Adult 2015, 22, 427–434. [Google Scholar] [CrossRef]
- Mulvaney, S.W.; Lynch, J.H.; Mahadevan, S.; Dineen, K.J.; Rae, K.L. The Effect of Bilateral, Two-Level Cervical Sympathetic Chain Blocks on Specific Symptom Clusters for Traumatic Brain Injury, Independent of Concomitant PTSD Symptoms. Brain Sci. 2024, 14, 1193. [Google Scholar] [CrossRef]
- Andrews, R.J.; Fonda, J.R.; Levin, L.K.; McGlinchey, R.E.; Milberg, W.P. Comprehensive Analysis of the Predictors of Neurobehavioral Symptom Reporting in Veterans. Neurology 2018, 91, e732–e745. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.A. Review of the Neurobehavioral Symptom Inventory. Rehabil. Psychol. 2020, 66, 170. [Google Scholar] [CrossRef]
- Weaver, L.K.; Ziemnik, R.; Deru, K.; Russo, A.A. A Double-Blind Randomized Trial of Hyperbaric Oxygen for Persistent Symptoms after Brain Injury. Sci. Rep. 2025, 15, 6885. [Google Scholar] [CrossRef]
- Yang, X.; Shi, Z.; Li, X.; Li, J. Impacts of Stellate Ganglion Block on Plasma NF-ΚB and Inflammatory Factors of TBI Patients. PubMed 2015, 8, 15630–15638. [Google Scholar]
- Kim, D.H. The Effect of Oxygen Administration on Regional Cerebral Oxygen Saturation after Stellate Ganglion Block on the Non-Blocked Side. Pain Physician 2013, 16, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Ter Laan, M.; van Dijk, J.M.C.; Elting, J.W.J.; Staal, M.J.; Absalom, A.R. Sympathetic Regulation of Cerebral Blood Flow in Humans: A Review. Br. J. Anaesth. 2013, 111, 361–367. [Google Scholar] [CrossRef]
- Loane, D.J.; Kumar, A. Microglia in the TBI Brain: The Good, the Bad, and the Dysregulated. Exp. Neurol. 2016, 275, 316–327. [Google Scholar] [CrossRef]
- Ziebell, J.M.; Morganti-Kossmann, M.C. Involvement of Pro- and Anti-Inflammatory Cytokines and Chemokines in the Pathophysiology of Traumatic Brain Injury. Neurotherapeutics 2010, 7, 22–30. [Google Scholar] [CrossRef]
- Muradashvili, N.; Lominadze, D. Role of Fibrinogen in Cerebrovascular Dysfunction after Traumatic Brain Injury. Brain Inj. 2013, 27, 1508–1515. [Google Scholar] [CrossRef]
- Sulhan, S.; Lyon, K.A.; Shapiro, L.A.; Huang, J.H. Neuroinflammation and Blood-Brain Barrier Disruption Following Traumatic Brain Injury: Pathophysiology and Potential Therapeutic Targets. J. Neurosci. Res. 2018, 98, 19–28. [Google Scholar] [CrossRef]
- Strogulski, N.R.; Portela, L.V.; Polster, B.M.; Loane, D.J. Fundamental Neurochemistry Review: Microglial Immunometabolism in Traumatic Brain Injury. J. Neurochem. 2023, 167, 129–153. [Google Scholar] [CrossRef] [PubMed]
- Giza, C.C.; Hovda, D.A. The New Neurometabolic Cascade of Concussion. Neurosurgery 2014, 75, S24–S33. [Google Scholar] [CrossRef]
- Shao, F.; Wang, X.; Wu, H.; Wu, Q.; Zhang, J. Microglia and Neuroinflammation: Crucial Pathological Mechanisms in Traumatic Brain Injury-Induced Neurodegeneration. Front. Aging Neurosci. 2022, 14, 825086. [Google Scholar] [CrossRef]
- Qin, P.; Sun, Y.; Li, L. Mitochondrial Dysfunction in Chronic Neuroinflammatory Diseases (Review). Int. J. Mol. Med. 2024, 53, 47. [Google Scholar] [CrossRef]
- Michinaga, S.; Koyama, Y. Pathophysiological Responses and Roles of Astrocytes in Traumatic Brain Injury. Int. J. Mol. Sci. 2021, 22, 6418. [Google Scholar] [CrossRef] [PubMed]
- Bramlett, H.M.; Dietrich, W.D.; Green, E.J.; Busto, R. Chronic Histopathological Consequences of Fluid-Percussion Brain Injury in Rats: Effects of Post-Traumatic Hypothermia. Acta Neuropathol. 1997, 93, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Alnaji, O.; Malik, M.; Gambale, T.; Farrokhyar, F.; Rathbone, M.P. Inflammatory Cytokines Associated with Mild Traumatic Brain Injury and Clinical Outcomes: A Systematic Review and Meta-Analysis. Front. Neurol. 2023, 14, 1123407. [Google Scholar] [CrossRef]
- Siman, R.; Giovannone, N.; Hanten, G.; Wilde, E.A.; McCauley, S.R.; Hunter, J.V.; Li, X.; Levin, H.S.; Smith, D.H. Evidence That the Blood Biomarker SNTF Predicts Brain Imaging Changes and Persistent Cognitive Dysfunction in Mild TBI Patients. Front. Neurol. 2013, 4, 190. [Google Scholar] [CrossRef] [PubMed]
- Cooksley, R.; Maguire, E.; Lannin, N.A.; Unsworth, C.A.; Farquhar, M.; Galea, C.; Mitra, B.; Schmidt, J. Persistent Symptoms and Activity Changes Three Months after Mild Traumatic Brain Injury. Aust. Occup. Ther. J. 2018, 65, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Madhok, D.Y.; Yue, J.K.; Sun, X.; Suen, C.G.; Coss, N.A.; Jain, S.; Manley, G.T.; The TRACK-TBI Investigators. Clinical Predictors of 3- and 6-Month Outcome for Mild Traumatic Brain Injury Patients with a Negative Head CT Scan in the Emergency Department: A TRACK-TBI Pilot Study. Brain Sci. 2020, 10, 269. [Google Scholar] [CrossRef]
- Dash, H.; Jain, V.; Rath, G.; Bithal, P.; Chouhan, R.; Suri, A. Stellate Ganglion Block for Treatment of Cerebral Vasospasm in Patients with Aneurysmal Subarachnoid Hemorrhage—A Preliminary Study. J. Anaesthesiol. Clin. Pharmacol. 2011, 27, 516. [Google Scholar] [CrossRef]
- Samagh, N.; Panda, N.; Gupta, V.K.; Bharti, N.; Tripathi, M.; Bhagat, H.; Chhabra, R.; Jangra, K.; Luthra, A. Impact of Stellate Ganglion Block in the Management of Cerebral Vasospasm: A Prospective Interventional Study. Neurol. India 2022, 70, 289–295. [Google Scholar] [CrossRef]
- Jing, L.; Wu, Y.; Liang, F.; Jian, M.; Bai, Y.; Wang, Y.; Liu, H.; Wang, A.; Chen, X.; Han, R. Effect of Early Stellate Ganglion Block in Cerebral Vasospasm after Aneurysmal Subarachnoid Hemorrhage (BLOCK-CVS): Study Protocol for a Randomized Controlled Trial. Trials 2022, 23, 922. [Google Scholar] [CrossRef]
- Gupta, M.M.; Bithal, P.K.; Dash, H.H.; Chaturvedi, A.; Mahajan, R.P. Effects of Stellate Ganglion Block on Cerebral Haemodynamics as Assessed by Transcranial Doppler Ultrasonography. Br. J. Anaesth. 2005, 95, 669–673. [Google Scholar] [CrossRef]
- Bardt, T.F.; Unterberg, A.W.; Härtl, R.; Kiening, K.L.; Schneider, G.H.; Lanksch, W.R. Monitoring of Brain Tissue PO2 in Traumatic Brain Injury: Effect of Cerebral Hypoxia on Outcome. Intracranial Press. Neuromonitoring Brain Inj. 1998, 71, 153–156. [Google Scholar] [CrossRef]
- Vespa, P.M. Brain Hypoxia and Ischemia after Traumatic Brain Injury. JAMA Neurol. 2016, 73, 504. [Google Scholar] [CrossRef] [PubMed]
- Mautes, A.E.M.; Müller, M.; Cortbus, F.; Schwerdtfeger, K.; Maier, B.; Holanda, M.; Nacimiento, A.; Marzi, I.; Steudel, W.-I. Alterations of Norepinephrine Levels in Plasma and CSF of Patients after Traumatic Brain Injury in Relation to Disruption of the Blood-Brain Barrier. Acta Neurochir. 2001, 143, 51–58. [Google Scholar] [CrossRef]
- Fernandez-Ortega, J.F.; Baguley, I.J.; Gates, T.A.; Garcia-Caballero, M.; Quesada-Garcia, J.G.; Prieto-Palomino, M.A. Catecholamines and Paroxysmal Sympathetic Hyperactivity after Traumatic Brain Injury. J. Neurotrauma 2017, 34, 109–114. [Google Scholar] [CrossRef]
- de Craen, A.J.M.; Tijssen, J.G.P.; de Gans, J.; Kleijnen, J. Placebo Effect in the Acute Treatment of Migraine: Subcutaneous Placebos Are Better than Oral Placebos. J. Neurol. 2000, 247, 183–188. [Google Scholar] [CrossRef]
- Holtedahl, R.; Brox, J.I.; Tjomsland, O. Placebo Effects in Trials Evaluating 12 Selected Minimally Invasive Interventions: A Systematic Review and Meta-Analysis. BMJ Open 2015, 5, e007331. [Google Scholar] [CrossRef]
- Edmed, S.L.; Sullivan, K.A.; Allan, A.C.; Smith, S.S. Assessment Method Influences the Severity and Type of Symptoms Reported after Self-Reported Mild Traumatic Brain Injury. J. Clin. Exp. Neuropsychol. 2015, 37, 641–652. [Google Scholar] [CrossRef] [PubMed]
- Port, A.; Willmott, C.; Charlton, J. Self-Awareness Following Traumatic Brain Injury and Implications for Rehabilitation. Brain Inj. 2002, 16, 277–289. [Google Scholar] [CrossRef]
- Daugherty, J.; Sarmiento, K.; Breiding, M. Comparison of Self-Reported Lifetime Concussions and Mild Traumatic Brain Injuries among Adults. Brain Inj. 2023, 37, 222–229. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
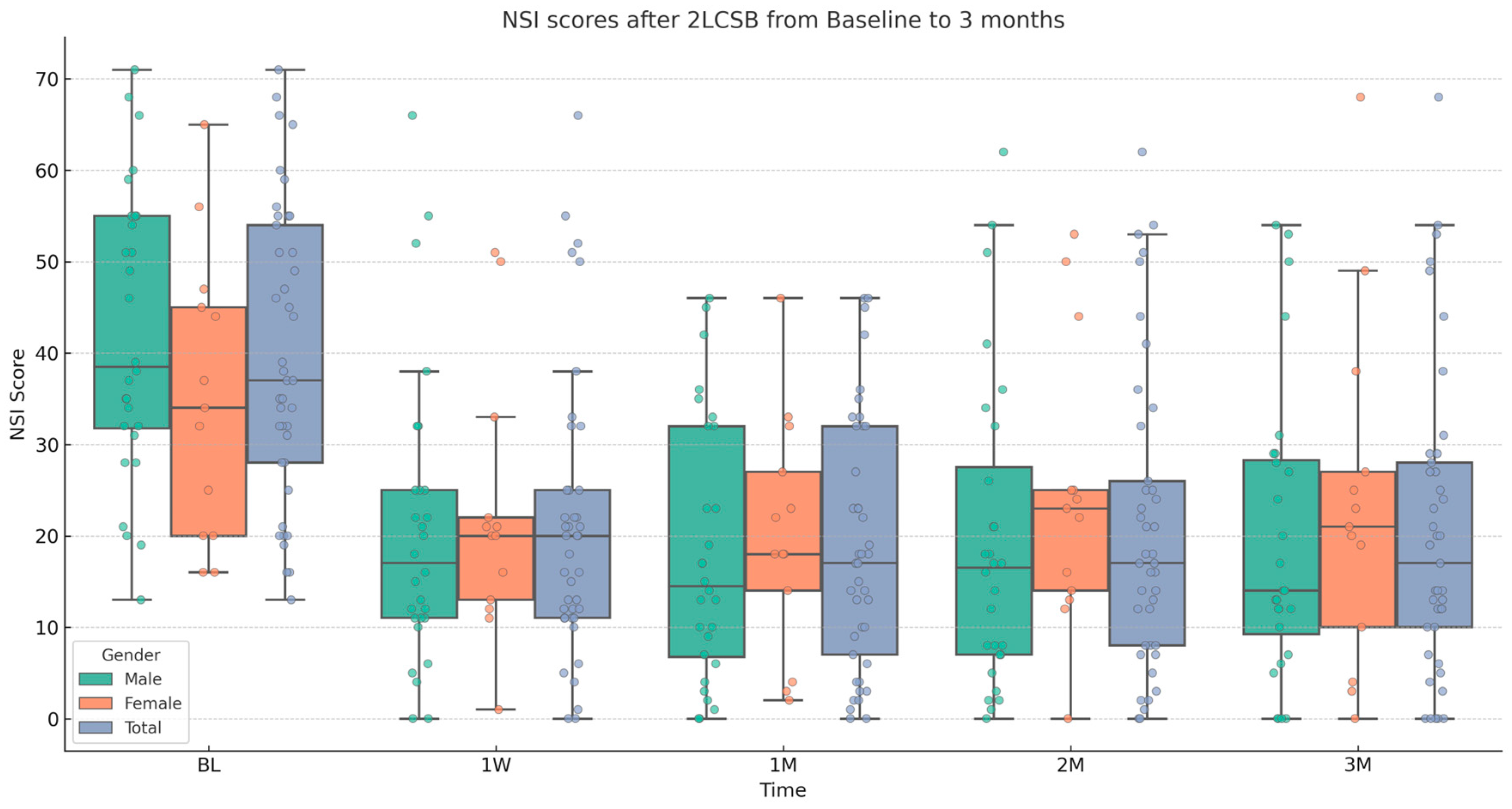
| Average NSI and NSI Sub-Scores | Male (SD) | Female (SD) | Total (SD) |
|---|---|---|---|
| Count | 28 | 13 | 41 |
| Baseline NSI scores | 42.21 (15.87) | 35.15 (15.68) | 39.92 (15.42) |
| Three-month NSI scores | 19.21 (15.88) | 23.62 (19.21) | 20.65 (16.3) |
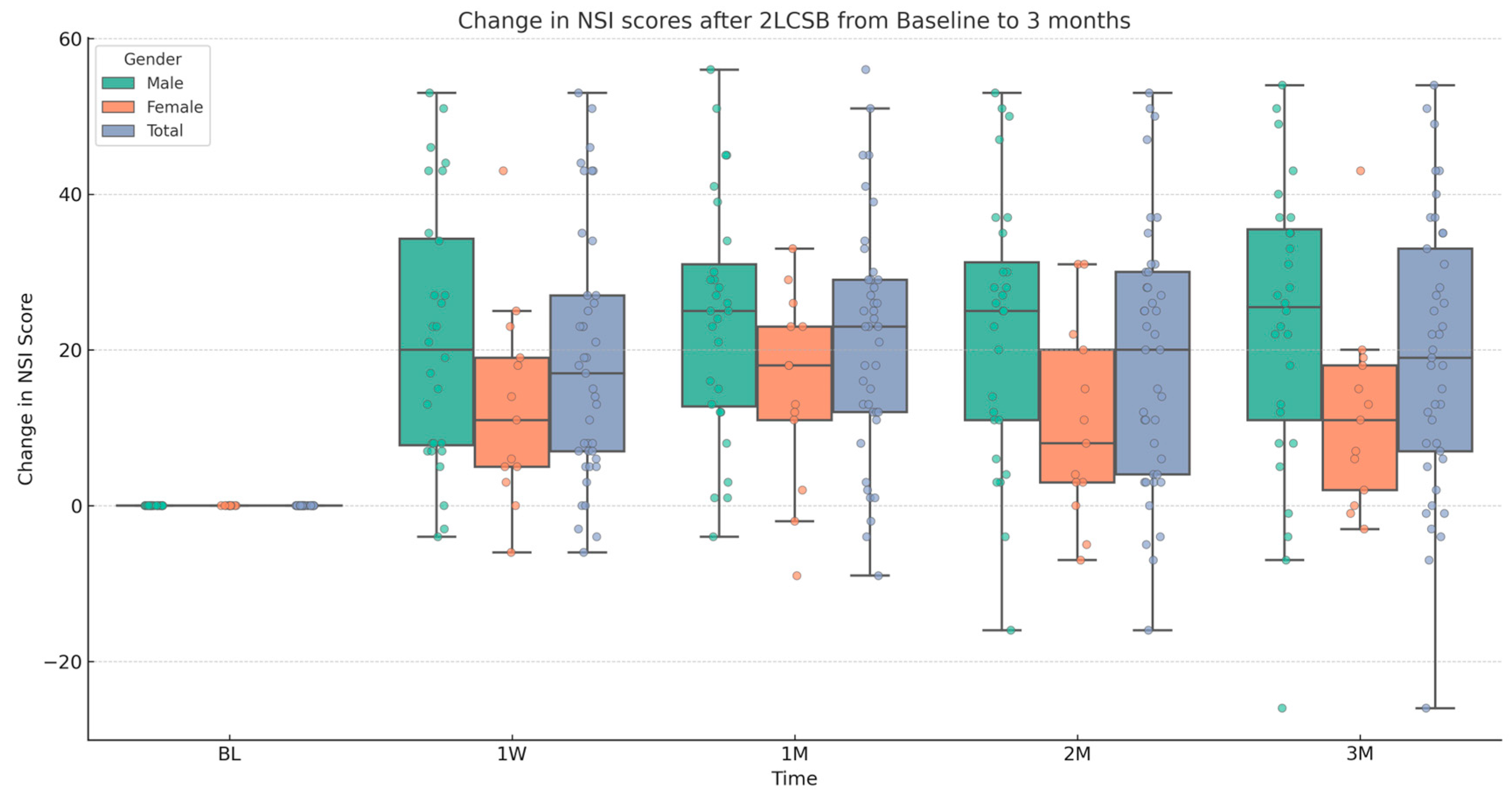
| Avg. Change in NSI Score (BL to 3M) | 22.93 (18.89) | 11.54 (12.31) | 19.37 (17.18) |
| Percent Decrease from Baseline | 54.16% | 32.82% | 48.44% |
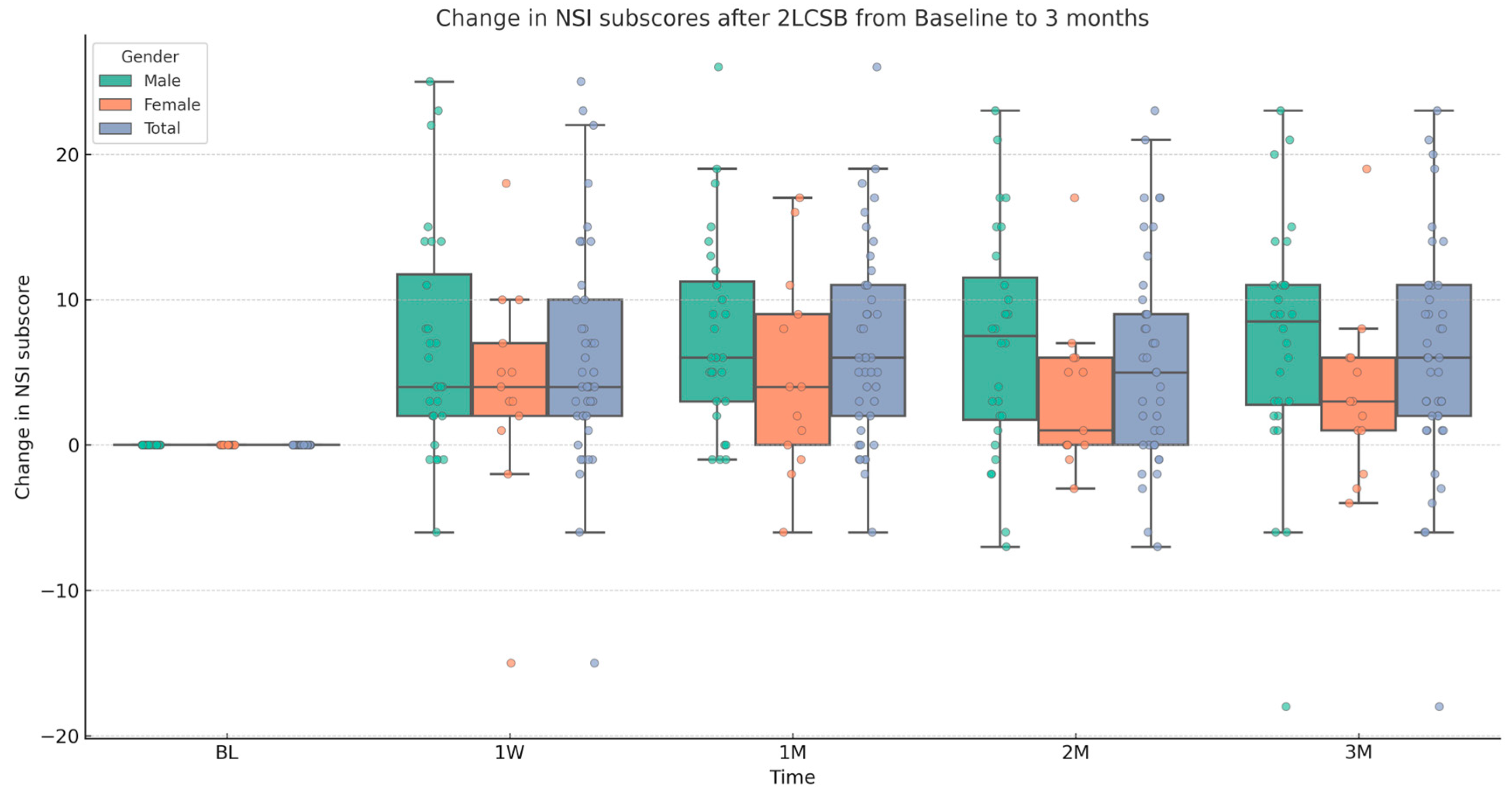
| Baseline NSI sub-scores | 14.65 (9.0) | 12.1 (6.79) | 13.78 (8.32) |
| Three-month NSI sub-scores | 7.58 (6.48) | 8.4 (7.4) | 7.86 (6.73) |
| Avg. Change in NSI sub-score (BL to 3M) | 7.07 (8.47) | 3.7 (5.55) | 5.92 (7.7) |
| Percent Decrease from Baseline | 48.22% | 29.03% | 43.11% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulvaney, S.W.; Mahadevan, S.; Desronvilles, R.J., Jr.; Dineen, K.J.; Rae Olmsted, K.L. Three-Month Durability of Bilateral Two-Level Stellate Ganglion Blocks for Traumatic Brain Injury: A Retrospective Analysis. Biomedicines 2025, 13, 1526. https://doi.org/10.3390/biomedicines13071526
Mulvaney SW, Mahadevan S, Desronvilles RJ Jr., Dineen KJ, Rae Olmsted KL. Three-Month Durability of Bilateral Two-Level Stellate Ganglion Blocks for Traumatic Brain Injury: A Retrospective Analysis. Biomedicines. 2025; 13(7):1526. https://doi.org/10.3390/biomedicines13071526
Chicago/Turabian StyleMulvaney, Sean W., Sanjay Mahadevan, Roosevelt J. Desronvilles, Jr., Kyle J. Dineen, and Kristine L. Rae Olmsted. 2025. "Three-Month Durability of Bilateral Two-Level Stellate Ganglion Blocks for Traumatic Brain Injury: A Retrospective Analysis" Biomedicines 13, no. 7: 1526. https://doi.org/10.3390/biomedicines13071526
APA StyleMulvaney, S. W., Mahadevan, S., Desronvilles, R. J., Jr., Dineen, K. J., & Rae Olmsted, K. L. (2025). Three-Month Durability of Bilateral Two-Level Stellate Ganglion Blocks for Traumatic Brain Injury: A Retrospective Analysis. Biomedicines, 13(7), 1526. https://doi.org/10.3390/biomedicines13071526