
Heart Failure and Wide QRS: Clinical and Pharmacological Perspectives

 ,
, 
 ,
,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
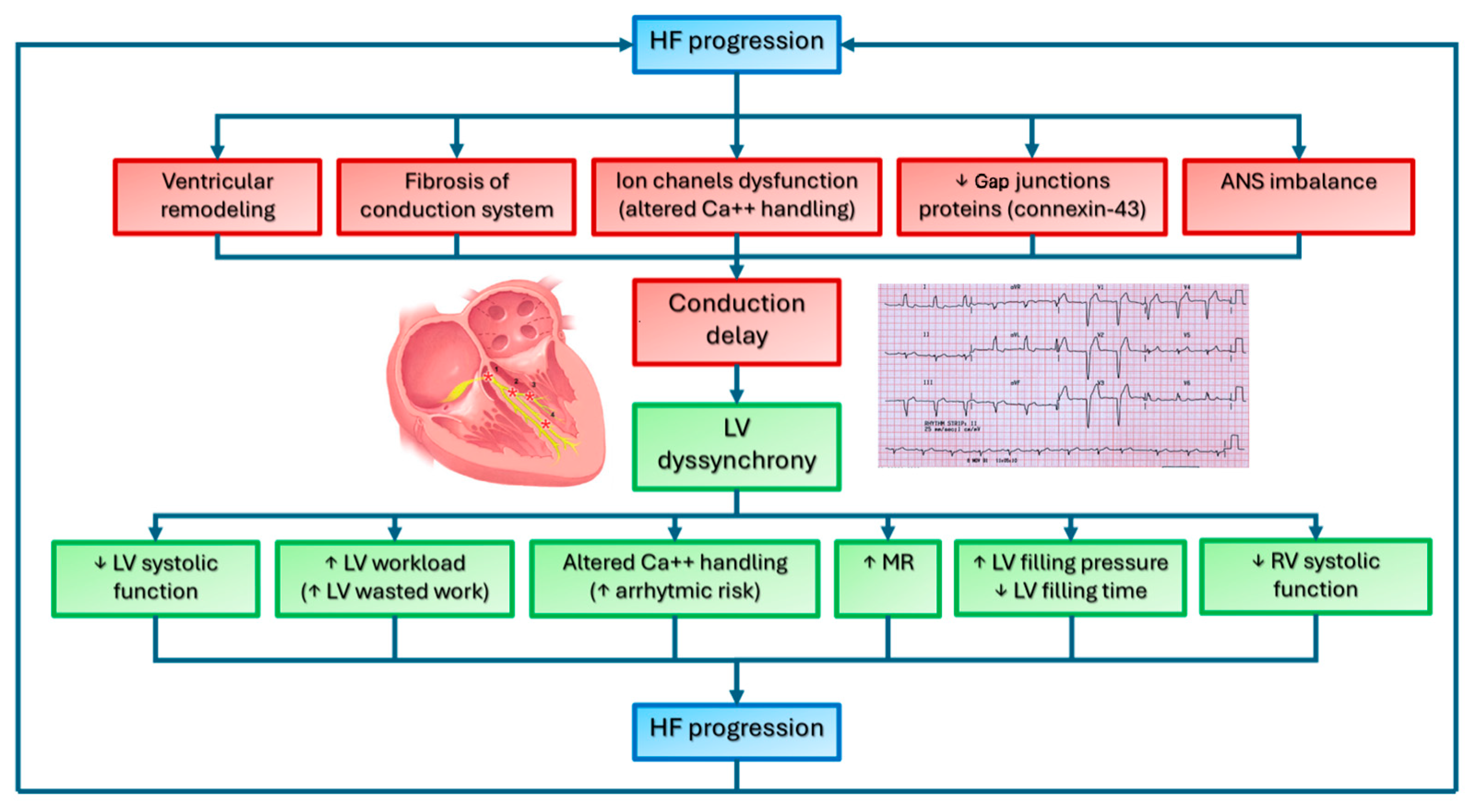
2. Intraventricular Conduction Delay in Heart Failure: Pathophysiological Mechanisms
2.1. Left Bundle Branch Block and Left Ventricle Systolic Function
2.2. Left Bundle Branch Block and Myocardial Metabolism
2.3. Left Bundle Branch Block and Mitral Regurgitation
2.4. Left Bundle Branch Block and Diastolic Function
2.5. Effects of Left Bundle Branch Block on Right Ventricle Function
2.6. Right Bundle Branch Block in Heart Failure
3. Sacubitril/Valsartan
4. SGLT2i
4.1. Role of Dapagliflozin in Wide QRS
4.2. Role of Empagliflozin in Wide QRS
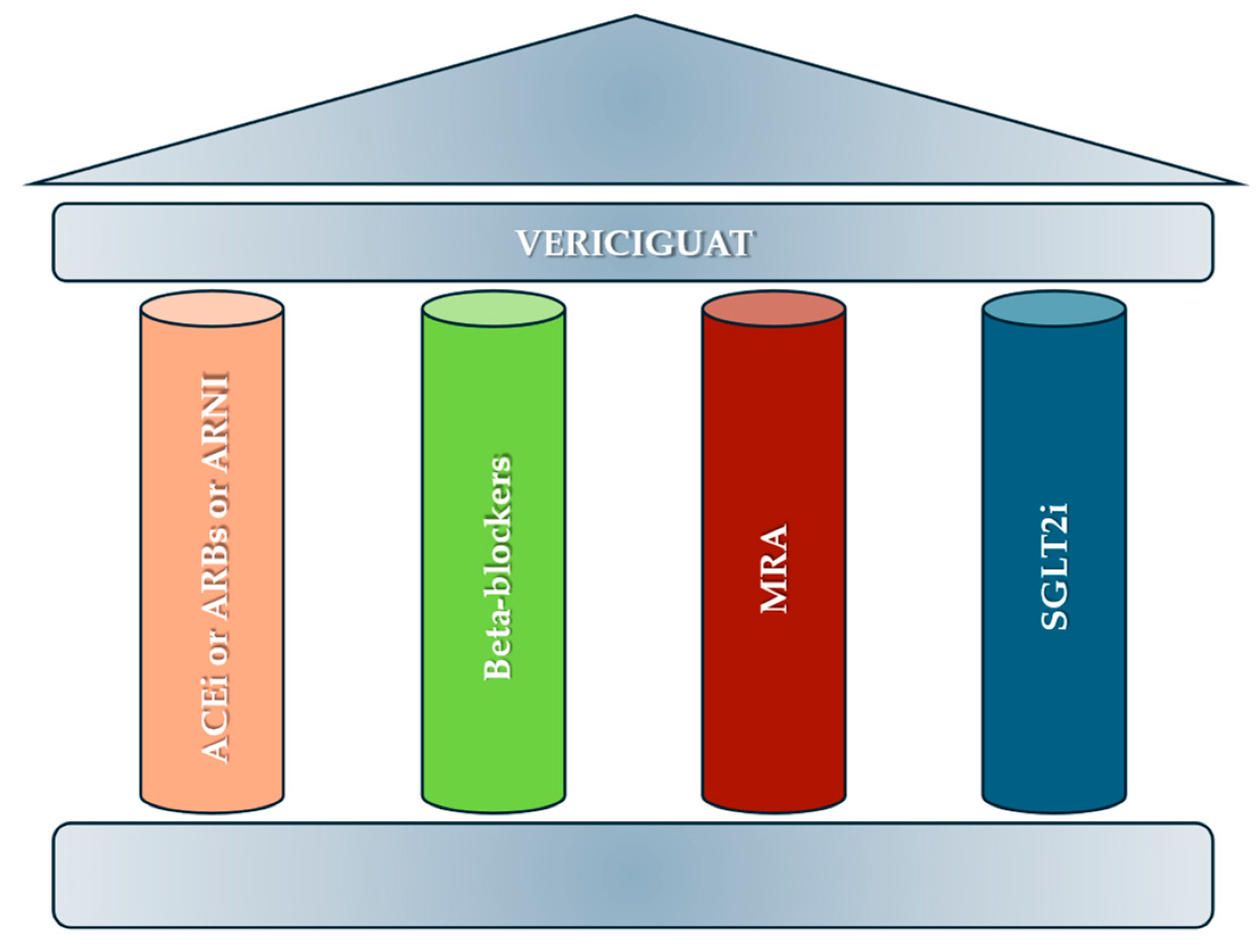
5. Vericiguat
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: Developed by the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC) with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726, Erratum in Eur. Heart J. 2021, 42, 4901. [Google Scholar] [CrossRef] [PubMed]
- Mauriello, A.; Ascrizzi, A.; Roma, A.S.; Molinari, R.; Caturano, A.; Imbalzano, E.; D’Andrea, A.; Russo, V. Effects of Heart Failure Therapies on Atrial Fibrillation: Biological and Clinical Perspectives. Antioxidants 2024, 13, 806. [Google Scholar] [CrossRef]
- Shahim, B.; Kapelios, C.J.; Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure: An Updated Review. Card. Fail. Rev. 2023, 9, e11. [Google Scholar] [CrossRef]
- Kass, D.A. Ventricular Dyssynchrony and Mechanisms of Resynchronization Therapy. Eur. Heart J. Suppl. 2002, 4, D23–D30. [Google Scholar] [CrossRef]
- Hawkins, N.M.; Petrie, M.C.; MacDonald, M.R.; Hogg, K.J.; McMurray, J.J.V. Selecting Patients for Cardiac Resynchronization Therapy: Electrical or Mechanical Dyssynchrony? Eur. Heart J. 2006, 27, 1270–1281. [Google Scholar] [CrossRef] [PubMed]
- Aranda, J.M.; Conti, J.B.; Johnson, J.W.; Petersen-Stejskal, S.; Curtis, A.B. Cardiac Resynchronization Therapy in Patients with Heart Failure and Conduction Abnormalities Other than Left Bundle-branch Block: Analysis of the Multicenter Insync Randomized Clinical Evaluation (MIRACLE). Clin. Cardiol. 2004, 27, 678–682. [Google Scholar] [CrossRef]
- Prinz, C.; Felice, C.D.; Lehmann, R.; Schwarz, M.; Prinz, E.-M.; Bitter, T.; Vogt, J.; Lamp, B.; Faber, L.; Horstkotte, D. Rethinking Cardiac Resynchronization Therapy: The Impact of Ventricular Dyssynchrony on Outcome. Int. J. Cardiol. 2013, 168, 3932–3939. [Google Scholar] [CrossRef]
- Ghio, S. Interventricular and Intraventricular Dyssynchrony Are Common in Heart Failure Patients, Regardless of QRS Duration. Eur. Heart J. 2004, 25, 571–578. [Google Scholar] [CrossRef]
- Bleeker, G.B.; Bax, J.J.; Steendijk, P.; Schalij, M.J.; van der Wall, E.E. Left Ventricular Dyssynchrony in Patients with Heart Failure: Pathophysiology, Diagnosis and Treatment. Nat. Clin. Pract. Cardiovasc. Med. 2006, 3, 213–219. [Google Scholar] [CrossRef]
- Soman, P.; Marwick, T.H. Left Ventricular Dyssynchrony. JACC Cardiovasc. Imaging 2019, 12, 1227–1229. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, E895–E1032. [Google Scholar] [CrossRef] [PubMed]
- Hartupee, J.; Mann, D.L. Neurohormonal Activation in Heart Failure with Reduced Ejection Fraction. Nat. Rev. Cardiol. 2017, 14, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Mauriello, A.; Correra, A.; Molinari, R.; Del Vecchio, G.E.; Tessitore, V.; D’Andrea, A.; Russo, V. Mitochondrial Dysfunction in Atrial Fibrillation: The Need for a Strong Pharmacological Approach. Biomedicines 2024, 12, 2720. [Google Scholar] [CrossRef]
- Cohn, J.N.; Ferrari, R.; Sharpe, N. Cardiac Remodeling—Concepts and Clinical Implications: A Consensus Paper from an International Forum on Cardiac Remodeling. Behalf of an International Forum on Cardiac Remodeling. J. Am. Coll. Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef]
- Opie, L.H.; Commerford, P.J.; Gersh, B.J.; Pfeffer, M.A. Controversies in Ventricular Remodelling. Lancet 2006, 367, 356–367. [Google Scholar] [CrossRef]
- González, A.; Schelbert, E.B.; Díez, J.; Butler, J. Myocardial Interstitial Fibrosis in Heart Failure. J. Am. Coll. Cardiol. 2018, 71, 1696–1706. [Google Scholar] [CrossRef] [PubMed]
- Neeland, I.J.; Kontos, M.C.; de Lemos, J.A. Evolving Considerations in the Management of Patients with Left Bundle Branch Block and Suspected Myocardial Infarction. J. Am. Coll. Cardiol. 2012, 60, 96–105. [Google Scholar] [CrossRef]
- Tan, N.Y.; Witt, C.M.; Oh, J.K.; Cha, Y.-M. Left Bundle Branch Block. Circ. Arrhythmia Electrophysiol. 2020, 13, e008239. [Google Scholar] [CrossRef]
- Rohr, S. Role of Gap Junctions in the Propagation of the Cardiac Action Potential. Cardiovasc. Res. 2004, 62, 309–322. [Google Scholar] [CrossRef]
- Prinzen, F.W.; Auricchio, A.; Mullens, W.; Linde, C.; Huizar, J.F. Electrical Management of Heart Failure: From Pathophysiology to Treatment. Eur. Heart J. 2022, 43, 1917–1927. [Google Scholar] [CrossRef]
- Dickstein, K.; Normand, C.; Auricchio, A.; Bogale, N.; Cleland, J.G.; Gitt, A.K.; Stellbrink, C.; Anker, S.D.; Filippatos, G.; Gasparini, M.; et al. CRT Survey II: A European Society of Cardiology Survey of Cardiac Resynchronisation Therapy in 11,088 Patients—Who Is Doing What to Whom and How? Eur. J. Heart Fail. 2018, 20, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Lund, L.H.; Benson, L.; Ståhlberg, M.; Braunschweig, F.; Edner, M.; Dahlström, U.; Linde, C. Age, Prognostic Impact of QRS Prolongation and Left Bundle Branch Block, and Utilization of Cardiac Resynchronization Therapy: Findings from 14,713 Patients in the Swedish Heart Failure Registry. Eur. J. Heart Fail. 2014, 16, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Mauriello, A.; Del Giudice, C.; Del Vecchio, G.E.; Correra, A.; Maratea, A.C.; Grieco, M.; Amata, A.; Quagliariello, V.; Maurea, N.; Proietti, R.; et al. Takotsubo Syndrome and Oxidative Stress: Physiopathological Linkage and Future Perspectives. Antioxidants 2025, 14, 522. [Google Scholar] [CrossRef]
- Smiseth, O.A.; Aalen, J.M. Mechanism of Harm from Left Bundle Branch Block. Trends Cardiovasc. Med. 2019, 29, 335–342. [Google Scholar] [CrossRef]
- Vernooy, K.; van Deursen, C.J.M.; Strik, M.; Prinzen, F.W. Strategies to Improve Cardiac Resynchronization Therapy. Nat. Rev. Cardiol. 2014, 11, 481–493. [Google Scholar] [CrossRef]
- Kanawati, J.; Sy, R.W. Contemporary Review of Left Bundle Branch Block in the Failing Heart—Pathogenesis, Prognosis, and Therapy. Heart Lung Circ. 2018, 27, 291–300. [Google Scholar] [CrossRef]
- Strauss, D.G.; Selvester, R.H.; Wagner, G.S. Defining Left Bundle Branch Block in the Era of Cardiac Resynchronization Therapy. Am. J. Cardiol. 2011, 107, 927–934. [Google Scholar] [CrossRef]
- Risum, N.; Strauss, D.; Sogaard, P.; Loring, Z.; Hansen, T.F.; Bruun, N.E.; Wagner, G.; Kisslo, J. Left Bundle-Branch Block: The Relationship between Electrocardiogram Electrical Activation and Echocardiography Mechanical Contraction. Am. Heart J. 2013, 166, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Vecera, J.; Penicka, M.; Eriksen, M.; Russell, K.; Bartunek, J.; Vanderheyden, M.; Smiseth, O.A. Wasted Septal Work in Left Ventricular Dyssynchrony: A Novel Principle to Predict Response to Cardiac Resynchronization Therapy. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 624–632. [Google Scholar] [CrossRef]
- Askenazi, J.; Alexander, J.H.; Koenigsberg, D.I.; Belic, N.; Lesch, M. Alteration of Left Ventricular Performance by Left Bundle Branch Block Simulated with Atrioventricular Sequential Pacing. Am. J. Cardiol. 1984, 53, 99–104. [Google Scholar] [CrossRef]
- Aalen, J.; Storsten, P.; Remme, E.W.; Sirnes, P.A.; Gjesdal, O.; Larsen, C.K.; Kongsgaard, E.; Boe, E.; Skulstad, H.; Hisdal, J.; et al. Afterload Hypersensitivity in Patients with Left Bundle Branch Block. JACC Cardiovasc. Imaging 2019, 12, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Prinzen, F.W.; Hunter, W.C.; Wyman, B.T.; McVeigh, E.R. Mapping of Regional Myocardial Strain and Work during Ventricular Pacing: Experimental Study Using Magnetic Resonance Imaging Tagging. J. Am. Coll. Cardiol. 1999, 33, 1735–1742. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A Novel Clinical Method for Quantification of Regional Left Ventricular Pressure–Strain Loop Area: A Non-Invasive Index of Myocardial Work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Gjesdal, O.; Edvardsen, T.; Smiseth, O.A. Assessment of Wasted Myocardial Work: A Novel Method to Quantify Energy Loss Due to Uncoordinated Left Ventricular Contractions. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H996–H1003. [Google Scholar] [CrossRef] [PubMed]
- Moya, A.; Buytaert, D.; Penicka, M.; Bartunek, J.; Vanderheyden, M. State-of-the-Art: Noninvasive Assessment of Left Ventricular Function Through Myocardial Work. J. Am. Soc. Echocardiogr. 2023, 36, 1027–1042. [Google Scholar] [CrossRef]
- Delhaas, T.; Arts, T.; Prinzen, F.W.; Reneman, R.S. Regional Fibre Stress-fibre Strain Area as an Estimate of Regional Blood Flow and Oxygen Demand in the Canine Heart. J. Physiol. 1994, 477, 481–496. [Google Scholar] [CrossRef]
- Ono, S.; Nohara, R.; Kambara, H.; Okuda, K.; Kawai, C. Regional Myocardial Perfusion and Glucose Metabolism in Experimental Left Bundle Branch Block. Circulation 1992, 85, 1125–1131. [Google Scholar] [CrossRef]
- Shvilkin, A.; Ellis, E.R.; Gervino, E.V.; Litvak, A.D.; Buxton, A.E.; Josephson, M.E. Painful Left Bundle Branch Block Syndrome: Clinical and Electrocardiographic Features and Further Directions for Evaluation and Treatment. Heart Rhythm. 2016, 13, 226–232. [Google Scholar] [CrossRef]
- Kumar, V.; Venkataraman, R.; Aljaroudi, W.; Osorio, J.; Heo, J.; Iskandrian, A.E.; Hage, F.G. Implications of Left Bundle Branch Block in Patient Treatment. Am. J. Cardiol. 2013, 111, 291–300. [Google Scholar] [CrossRef]
- Spragg, D.D.; Leclercq, C.; Loghmani, M.; Faris, O.P.; Tunin, R.S.; DiSilvestre, D.; McVeigh, E.R.; Tomaselli, G.F.; Kass, D.A. Regional Alterations in Protein Expression in the Dyssynchronous Failing Heart. Circulation 2003, 108, 929–932. [Google Scholar] [CrossRef]
- Nguyên, U.C.; Verzaal, N.J.; van Nieuwenhoven, F.A.; Vernooy, K.; Prinzen, F.W. Pathobiology of Cardiac Dyssynchrony and Resynchronization Therapy. EP Eur. 2018, 20, 1898–1909. [Google Scholar] [CrossRef] [PubMed]
- Kirk, J.A.; Kass, D.A. Electromechanical Dyssynchrony and Resynchronization of the Failing Heart. Circ. Res. 2013, 113, 765–776. [Google Scholar] [CrossRef]
- Aiba, T.; Hesketh, G.G.; Barth, A.S.; Liu, T.; Daya, S.; Chakir, K.; Dimaano, V.L.; Abraham, T.P.; O’Rourke, B.; Akar, F.G.; et al. Electrophysiological Consequences of Dyssynchronous Heart Failure and Its Restoration by Resynchronization Therapy. Circulation 2009, 119, 1220–1230. [Google Scholar] [CrossRef]
- Levine, R.A.; Nagata, Y.; Dal-Bianco, J.P. Left Ventricular Dyssynchrony and the Mitral Valve Apparatus. JACC Cardiovasc. Imaging 2019, 12, 1738–1740. [Google Scholar] [CrossRef] [PubMed]
- Kagiyama, N.; Mondillo, S.; Yoshida, K.; Mandoli, G.E.; Cameli, M. Subtypes of Atrial Functional Mitral Regurgitation. JACC Cardiovasc. Imaging 2020, 13, 820–835. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Huvelle, E.; Dickstein, K.; van Veldhuisen, D.J.; Stellbrink, C.; Køber, L.; Cazeau, S.; Ritter, P.; Maggioni, A.P.; Ferrari, R.; et al. Left Bundle Branch Block as a Risk Factor for Progression to Heart Failure. Eur. J. Heart Fail. 2007, 9, 7–14. [Google Scholar] [CrossRef]
- Regueiro, A.; Abdul-Jawad Altisent, O.; Del Trigo, M.; Campelo-Parada, F.; Puri, R.; Urena, M.; Philippon, F.; Rodés-Cabau, J. Impact of New-Onset Left Bundle Branch Block and Periprocedural Permanent Pacemaker Implantation on Clinical Outcomes in Patients Undergoing Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2016, 9, e003635. [Google Scholar] [CrossRef]
- Liu, L.; Tockman, B.; Girouard, S.; Pastore, J.; Walcott, G.; KenKnight, B.; Spinelli, J. Left Ventricular Resynchronization Therapy in a Canine Model of Left Bundle Branch Block. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H2238–H2244. [Google Scholar] [CrossRef]
- Özdemir, K.; Altunkeser, B.B.; Daniş, G.; Özdemir, A.; Uluca, Y.; Tokaç, M.; Telli, H.H.; Gök, H. Effect of the Isolated Left Bundle Branch Block on Systolic and Diastolic Functions of Left Ventricle. J. Am. Soc. Echocardiogr. 2001, 14, 1075–1079. [Google Scholar] [CrossRef]
- Xiao, H.B.; Lee, C.H.; Gibson, D.G. Effect of Left Bundle Branch Block on Diastolic Function in Dilated Cardiomyopathy. Heart 1991, 66, 443–447. [Google Scholar] [CrossRef]
- Grines, C.L.; Bashore, T.M.; Boudoulas, H.; Olson, S.; Shafer, P.; Wooley, C.F. Functional Abnormalities in Isolated Left Bundle Branch Block. The Effect of Interventricular Asynchrony. Circulation 1989, 79, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Lumens, J.; Ploux, S.; Strik, M.; Gorcsan, J.; Cochet, H.; Derval, N.; Strom, M.; Ramanathan, C.; Ritter, P.; Haïssaguerre, M.; et al. Comparative Electromechanical and Hemodynamic Effects of Left Ventricular and Biventricular Pacing in Dyssynchronous Heart Failure. J. Am. Coll. Cardiol. 2013, 62, 2395–2403. [Google Scholar] [CrossRef] [PubMed]
- Egoavil, C.A.; Ho, R.T.; Greenspon, A.J.; Pavri, B.B. Cardiac Resynchronization Therapy in Patients with Right Bundle Branch Block: Analysis of Pooled Data from the MIRACLE and Contak CD Trials. Heart Rhythm. 2005, 2, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Bilchick, K.C.; Kamath, S.; DiMarco, J.P.; Stukenborg, G.J. Bundle-Branch Block Morphology and Other Predictors of Outcome after Cardiac Resynchronization Therapy in Medicare Patients. Circulation 2010, 122, 2022–2030. [Google Scholar] [CrossRef]
- Rickard, J.; Kumbhani, D.J.; Gorodeski, E.Z.; Baranowski, B.; Wazni, O.; Martin, D.O.; Grimm, R.; Wilkoff, B.L. Cardiac Resynchronization Therapy in Non-Left Bundle Branch Block Morphologies. Pacing Clin. Electrophysiol. 2010, 33, 590–595. [Google Scholar] [CrossRef]
- McCullough, P.A.; Hassan, S.A.; Pallekonda, V.; Sandberg, K.R.; Nori, D.B.; Soman, S.S.; Bhatt, S.; Hudson, M.P.; Weaver, W.D. Bundle Branch Block Patterns, Age, Renal Dysfunction, and Heart Failure Mortality. Int. J. Cardiol. 2005, 102, 303–308. [Google Scholar] [CrossRef]
- Barsheshet, A.; Goldenberg, I.; Garty, M.; Gottlieb, S.; Sandach, A.; Laish-Farkash, A.; Eldar, M.; Glikson, M. Relation of Bundle Branch Block to Long-Term (Four-Year) Mortality in Hospitalized Patients with Systolic Heart Failure. Am. J. Cardiol. 2011, 107, 540–544. [Google Scholar] [CrossRef]
- Fantoni, C.; Kawabata, M.; Massaro, R.; Regoli, F.; Raffa, S.; Arora, V.; Salerno-Uriarte, J.A.; Klein, H.U.; Auricchio, A. Right and Left Ventricular Activation Sequence in Patients with Heart Failure and Right Bundle Branch Block: A Detailed Analysis Using Three-Dimensional Non-Fluoroscopic Electroanatomic Mapping System. J. Cardiovasc. Electrophysiol. 2005, 16, 112–119. [Google Scholar] [CrossRef]
- Mauriello, A.; Marrazzo, G.; Del Vecchio, G.E.; Ascrizzi, A.; Roma, A.S.; Correra, A.; Sabatella, F.; Gioia, R.; Desiderio, A.; Russo, V.; et al. Echocardiography in Cardiac Arrest: Incremental Diagnostic and Prognostic Role during Resuscitation Care. Diagnostics 2024, 14, 2107. [Google Scholar] [CrossRef]
- Russo, V.; Falco, L.; Tessitore, V.; Mauriello, A.; Catapano, D.; Napolitano, N.; Tariq, M.; Caturano, A.; Ciccarelli, G.; D’Andrea, A.; et al. Anti-Inflammatory and Anticancer Effects of Anticoagulant Therapy in Patients with Malignancy. Life 2023, 13, 1888. [Google Scholar] [CrossRef]
- Zhang, Q.; Xue, M.; Li, Z.; Wang, H.; Zhu, L.; Liu, X.; Meng, H.; Hou, Y. Effects of an Isolated Complete Right Bundle Branch Block on Mechanical Ventricular Function. J. Ultrasound Med. 2015, 34, 2171–2177. [Google Scholar] [CrossRef] [PubMed]
- Sillanmäki, S.; Aapro, S.; Lipponen, J.A.; Tarvainen, M.P.; Laitinen, T.; Hedman, M.; Hämäläinen, H.; Laitinen, T. Electrical and Mechanical Dyssynchrony in Patients with Right Bundle Branch Block. J. Nucl. Cardiol. 2020, 27, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Seçkin Göbüt, Ö.; Sezenöz, B.; Küçükbardaslı, M.; Yamak, B.A.; Ünlü, S. Evaluation of Right and Left Ventricular Deformation Analysis in İdiopathic Right Bundle Branch Block by Speckle Tracking Echocardiography. Echocardiography 2025, 42, e70056. [Google Scholar] [CrossRef]
- Vardeny, O.; Claggett, B.; Packer, M.; Zile, M.R.; Rouleau, J.; Swedberg, K.; Teerlink, J.R.; Desai, A.S.; Lefkowitz, M.; Shi, V.; et al. Efficacy of Sacubitril/Valsartan vs. Enalapril at Lower than Target Doses in Heart Failure with Reduced Ejection Fraction: The PARADIGM-HF Trial. Eur. J. Heart Fail. 2016, 18, 1228–1234. [Google Scholar] [CrossRef]
- Abudan, A.; Parimi, N.; Sami, F.; Mahmood, U.; Schwarz, C.; Pierpoline, M.; Mohammed, M.; Dendi, R.; Pimentel, R.C.; Berenbom, L.D.; et al. Abstract 16271: Resolution of Left Bundle Branch Block with Sacubitril/Valsartan in Patients with Heart Failure with Reduced Ejection Fraction. Circulation 2020, 142 (Suppl. S3), A16271. [Google Scholar] [CrossRef]
- Allam, L.E.; Abdelmotteleb, A.A.; Eldamanhoury, H.M.; Hassan, H.S. Unlocking the Potential of Sacubitril/Valsartan Therapy in Improving ECG and Echocardiographic Parameters in Heart Failure Patients with Reduced Ejection Fraction (HErEF). Egypt. Heart J. 2024, 76, 41. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Huang, J.; Lin, P.; Lee, Y.; Hsu, C.; Chung, F.; Liao, C.; Chiou, W.; Lin, W.; Liang, H.; et al. Clinical Impacts of Sacubitril/Valsartan on Patients Eligible for Cardiac Resynchronization Therapy. ESC Heart Fail. 2022, 9, 3825–3835. [Google Scholar] [CrossRef]
- Russo, V.; Ammendola, E.; Gasperetti, A.; Bottino, R.; Schiavone, M.; Masarone, D.; Pacileo, G.; Nigro, G.; Golino, P.; Lip, G.Y.H.; et al. Add-on Therapy with Sacubitril/Valsartan and Clinical Outcomes in CRT-D Nonresponder Patients. J. Cardiovasc. Pharmacol. 2022, 79, 472–478. [Google Scholar] [CrossRef]
- Khan, M.S.; Felker, G.M.; Piña, I.L.; Camacho, A.; Bapat, D.; Ibrahim, N.E.; Maisel, A.S.; Prescott, M.F.; Ward, J.H.; Solomon, S.D.; et al. Reverse Cardiac Remodeling Following Initiation of Sacubitril/Valsartan in Patients with Heart Failure with and Without Diabetes. JACC Heart Fail. 2021, 9, 137–145. [Google Scholar] [CrossRef]
- Abdin, A.; Kondo, T.; Böhm, M.; Jhund, P.S.; Claggett, B.L.; Vaduganathan, M.; Hernandez, A.F.; Lam, C.S.P.; Inzucchi, S.E.; Martinez, F.A.; et al. Effects of Dapagliflozin According to QRS Duration across the Spectrum of Left Ventricular Ejection Fraction: An Analysis of DAPA-HF and DELIVER. Eur. J. Heart Fail. 2024, 26, 1952–1963. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Mauriello, A.; Correra, A.; Ascrizzi, A.; Del Vecchio, G.E.; Benfari, G.; Ilardi, F.; Lisi, M.; Malagoli, A.; Mandoli, G.E.; Pastore, M.C.; et al. Relationship Between Left Atrial Strain and Atrial Fibrillation: The Role of Stress Echocardiography. Diagnostics 2024, 15, 7. [Google Scholar] [CrossRef]
- Mauriello, A.; Correra, A.; Maratea, A.C.; Caturano, A.; Liccardo, B.; Perrone, M.A.; Giordano, A.; Nigro, G.; D’Andrea, A.; Russo, V. Serum Lipids, Inflammation, and the Risk of Atrial Fibrillation: Pathophysiological Links and Clinical Evidence. J. Clin. Med. 2025, 14, 1652. [Google Scholar] [CrossRef] [PubMed]
- Antwi-Amoabeng, D.; Sathappan, S.; Beutler, B.D.; Ulanja, M.B.; Awad, M.; Gullapalli, N.; Duncan, P.; Gbadebo, T.D. Association between Empagliflozin Use and Electrocardiographic Changes. Clin. Pract. 2022, 12, 557–564. [Google Scholar] [CrossRef]
- Yang, Z.; Li, T.; Xian, J.; Chen, J.; Huang, Y.; Zhang, Q.; Lin, X.; Lu, H.; Lin, Y. SGLT2 Inhibitor Dapagliflozin Attenuates Cardiac Fibrosis and Inflammation by Reverting the HIF-2α Signaling Pathway in Arrhythmogenic Cardiomyopathy. FASEB J. 2022, 36, e22410. [Google Scholar] [CrossRef]
- Lee, S.-G.; Kim, D.; Lee, J.-J.; Lee, H.-J.; Moon, R.; Lee, Y.-J.; Lee, S.-J.; Lee, O.-H.; Kim, C.; Oh, J.; et al. Dapagliflozin Attenuates Diabetes-Induced Diastolic Dysfunction and Cardiac Fibrosis by Regulating SGK1 Signaling. BMC Med. 2022, 20, 309. [Google Scholar] [CrossRef]
- Wang, M.; Liu, X.; Ding, B.; Lu, Q.; Ma, J. SGLT2 Inhibitor Dapagliflozin Alleviates Cardiac Dysfunction and Fibrosis after Myocardial Infarction by Activating PXR and Promoting Angiogenesis. Biomed. Pharmacother. 2024, 177, 116994. [Google Scholar] [CrossRef]
- Tian, J.; Zhang, M.; Suo, M.; Liu, D.; Wang, X.; Liu, M.; Pan, J.; Jin, T.; An, F. Dapagliflozin Alleviates Cardiac Fibrosis through Suppressing EndMT and Fibroblast Activation via AMPKα/TGF-β/Smad Signalling in Type 2 Diabetic Rats. J. Cell. Mol. Med. 2021, 25, 7642–7659. [Google Scholar] [CrossRef]
- Chatur, S.; Churchill, T.W. Dapagliflozin and Cardiac Reverse Remodeling: New Insights in the Mechanistic Puzzle of SGLT2 Inhibitors. J. Am. Soc. Echocardiogr. 2025, 38, 404–408. [Google Scholar] [CrossRef]
- Savage, P.; Watson, C.; Coburn, J.; Cox, B.; Shahmohammadi, M.; Grieve, D.; Dixon, L. Impact of SGLT2 Inhibition on Markers of Reverse Cardiac Remodelling in Heart Failure: Systematic Review and Meta-analysis. ESC Heart Fail. 2024, 11, 3636–3648. [Google Scholar] [CrossRef] [PubMed]
- Böttcher, M.; Düngen, H.-D.; Corcea, V.; Donath, F.; Fuhr, R.; Gal, P.; Mikus, G.; Trenk, D.; Coenen, M.; Pires, P.V.; et al. Vericiguat: A Randomized, Phase Ib, Placebo-Controlled, Double-Blind, QTc Interval Study in Patients with Chronic Coronary Syndromes. Am. J. Cardiovasc. Drugs 2023, 23, 145–155. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Authors | Patients | Outcome | Results |
|---|---|---|---|
| Huang et al. [67] 2021 | 1168 | Investigate the prescription patterns of sacubitril/valsartan among Taiwanese patients with heart failure with reduced ejection fraction | Multivariate analyses showed that wide QRS durations were negatively associated with the reverse cardiac remodeling |
| Allam et al. [66] 2024 | 100 | Effects of sacubitril/valsartan on electrocardiogram indices and how those parameters relate to echocardiographic parameters | QRS width was reduced from 123.7 ± 20.3 to 117.1 ± 18.8 ms (p < 0.001) |
| Abudan et al. [65] 2022 | 368 | The clinical impacts of sacubitril/valsartan on reverse cardiac remodeling in patients di HFrEF with different QRS durations | During a median follow-up of 9.1 months, five resolved LBBB to normal conduction (p = 0.11), and two improved to non-specific intraventricular conduction delay (p = 0.08) |
| Abdin et al. [70] 2024 | 9824 | The effect of dapagliflozin according to QRS duration across the spectrum of left-ventricular ejection fraction | The risk of the primary outcome consistently across the QRS duration subgroups (HR [95% CI] 0.75 [0.67–0.85], 0.79 [0.65–0.96], and 0.89 [0.70–1.13] in the <120, 120–149, and ≥150 ms groups, respectively; p for interaction = 0.28) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauriello, A.; Correra, A.; Del Vecchio, G.E.; Grieco, M.; Amata, A.; Di Micco, P.; Imbalzano, E.; Paternoster, M.; Ascrizzi, A.; Quagliariello, V.; et al. Heart Failure and Wide QRS: Clinical and Pharmacological Perspectives. Biomedicines 2025, 13, 1462. https://doi.org/10.3390/biomedicines13061462
Mauriello A, Correra A, Del Vecchio GE, Grieco M, Amata A, Di Micco P, Imbalzano E, Paternoster M, Ascrizzi A, Quagliariello V, et al. Heart Failure and Wide QRS: Clinical and Pharmacological Perspectives. Biomedicines. 2025; 13(6):1462. https://doi.org/10.3390/biomedicines13061462
Chicago/Turabian StyleMauriello, Alfredo, Adriana Correra, Gerardo Elia Del Vecchio, Martina Grieco, Arianna Amata, Pierpaolo Di Micco, Egidio Imbalzano, Mariano Paternoster, Antonia Ascrizzi, Vincenzo Quagliariello, and et al. 2025. "Heart Failure and Wide QRS: Clinical and Pharmacological Perspectives" Biomedicines 13, no. 6: 1462. https://doi.org/10.3390/biomedicines13061462
APA StyleMauriello, A., Correra, A., Del Vecchio, G. E., Grieco, M., Amata, A., Di Micco, P., Imbalzano, E., Paternoster, M., Ascrizzi, A., Quagliariello, V., Maurea, N., Giallauria, F., D’Andrea, A., & Russo, V. (2025). Heart Failure and Wide QRS: Clinical and Pharmacological Perspectives. Biomedicines, 13(6), 1462. https://doi.org/10.3390/biomedicines13061462