
The Efficacy of a Deproteinized Bovine Bone Mineral Graft for Alveolar Ridge Preservation: A Histologic Study in Humans

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Inclusion Criteria
- Patients with at least two noncontiguous teeth scheduled for extraction without signs of acute infection.
- Patients over 18 years of age.
- Patients who were willing to rehabilitate the extracted teeth with dental implants.
- Patients who were able to attend all the required study visits and undergo necessary evaluations.
- Patients in good general health without systemic diseases (ASA I/II).
2.3. Exclusion Criteria
- Patients currently enrolled in another clinical study.
- Patients with alveolar sockets with healing times of less than 6 months.
- Excessive alcohol consumption (defined as >60 g/day for men and >40 g/day for women, according to World Health Organization criteria).
- Individuals with substance abuse problems.
- The use of any medication or substance that may affect bone metabolism (e.g., bisphosphonates).
- Teeth presenting with acute or chronic infections (e.g., osteomyelitis) at the surgical site.
- Patients with metabolic disorders, including uncontrolled diabetes (HbA1c >6.5%), thyroid disease, osteomalacia, autoimmune diseases, osteoporosis, renal disease, or severe liver disease, or those receiving high-dose corticosteroids.
- Patients with active cancer or receiving chemotherapy or radiotherapy.
- Individuals with known hypersensitivity to antibiotics, analgesics, or anti-inflammatory drugs.
- Pregnant or lactating women.
2.4. Materials
2.4.1. Clinical Examination Instruments
- Oral cavity examination: Sterile intraoral mirror (No. 5, non-magnifying; Hu-Friedy®, Frankfurt, Germany).
- Periodontal assessment: Williams-type periodontal probe (Hu-Friedy®, Frankfurt, Germany).
- Tissue handling: Anatomic stainless steel tweezers (Hu-Friedy®, Frankfurt, Germany).
2.4.2. Surgical Instruments for Tooth Extraction
- Extraction tools:
- ○
- Dental elevators (straight and angled; Hu-Friedy®, Frankfurt, Germany).
- ○
- Extraction forceps (site-specific; Hu-Friedy®, Frankfurt, Germany).
- ○
- Lucas bone curette (Hu-Friedy®).
- Anesthesia: Disposable 27-gauge dental needle and aspirating syringe (Becton Dickinson, Madrid, Spain).
2.4.3. Surgical Instruments for Alveolar Ridge Preservation (ARP)
- Incision and flap elevation:
- ○
- Scalpel handle with No. 15C blade (Swann-Morton®, Sheffield, UK).
- ○
- Periosteal elevators (Buser and Zinghem; Hu-Friedy®, Frankfurt, Germany).
- Bone manipulation:
- ○
- Surgical chisels (Orban and Castroviejo; Hu-Friedy®, Frankfurt, Germany).
- Suturing:
- ○
- Non-resorbable monofilament sutures (Supramid® 4-0; S. Jackson Inc., Alexandria, VA, USA).
- ○
- Sharp/blunt scissors (Hu-Friedy®, Frankfurt, Germany).
2.4.4. Graft Material
- Deproteinized bovine bone mineral (DBBM):
- ○
- techBiomat bone® (0.25–1.68 mm granule size; Technology in Biomaterials S.L., Barcelona, Spain).
- ○
- Note: The manufacturer provided the graft material but had no role in study design, data analysis, or interpretation.
2.4.5. Histological Sample Collection
- Bone core harvesting:
- ○
- Sterile trephine bur (external Ø = 2.0 mm, length ≥ 5.0 mm; MT. Medicon®, Barcelona, Spain).
- Tissue fixation:
- ○
- We used 10% neutral buffered formaldehyde (PanReac AppliChem, Barcelona, Spain).
2.4.6. Dental Implants
- Implant system:
- ○
- Ticare Inhex® (Standard and Quattro designs; Mozo-Grau SA, Valladolid, Spain).
- ○
- Surgical kit (800 rpm drilling protocol under irrigation; 20 Ncm insertion torque).
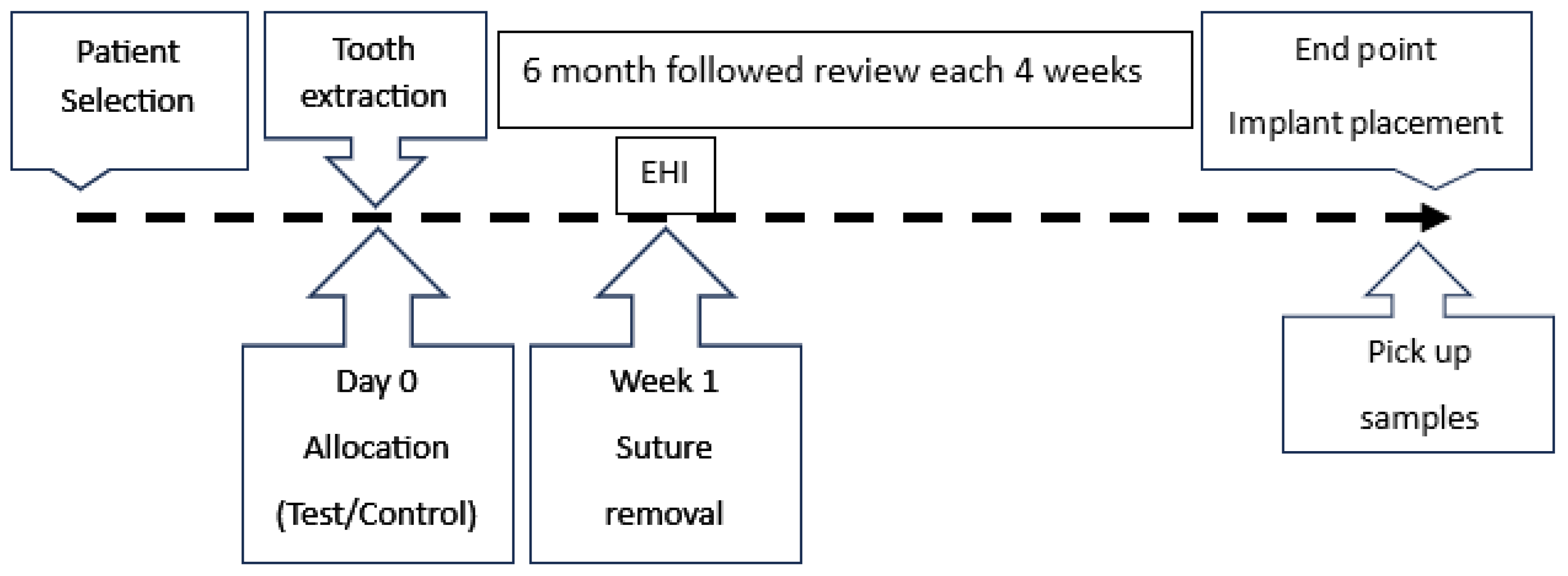
2.5. Methods
- Grade I > 75% (successful result).
- Grade II 50–75%.
- Grade III 25–50%.
- Grade IV < 25%: no new bone formation (failure result).
2.6. Implant Procedure
2.7. Histopathology Procedure
2.8. Duration of This Study
2.9. Statistical Methods
- Descriptive statistics:
- General distribution of the sample: We calculated the values of the means, confidence intervals, and count values for each of the numerical variables considered in this study.
- A frequency analysis of nominal and ordinal variables was conducted.
- Inferential statistics: The Mann–Whitney U test was used to identify statistically significant differences between the test and control groups, in which case the effect size was calculated. A p value < 0.05 was considered statistically significant.
3. Results
3.1. Descriptive Statistics
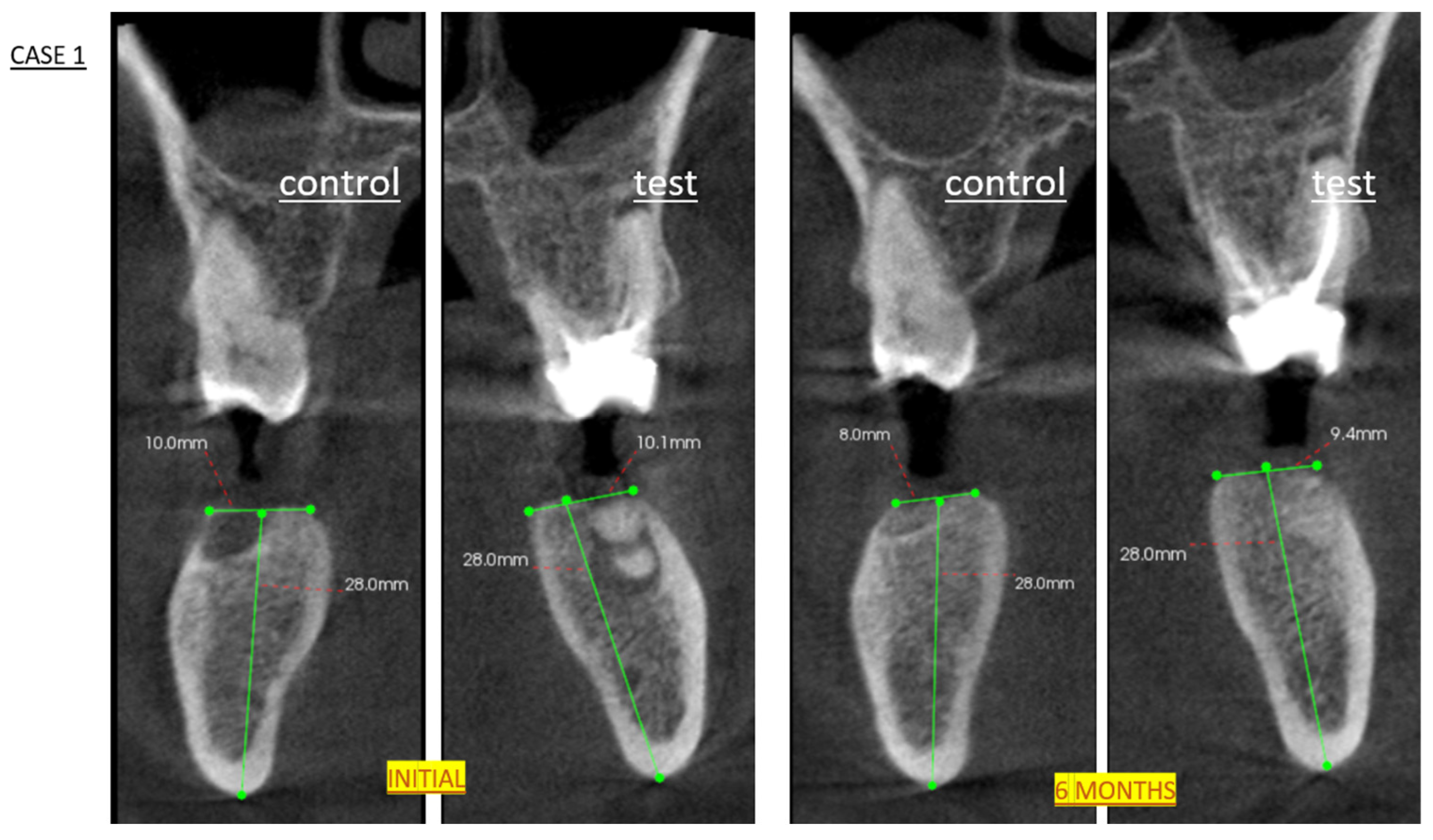
3.1.1. Radiological Results
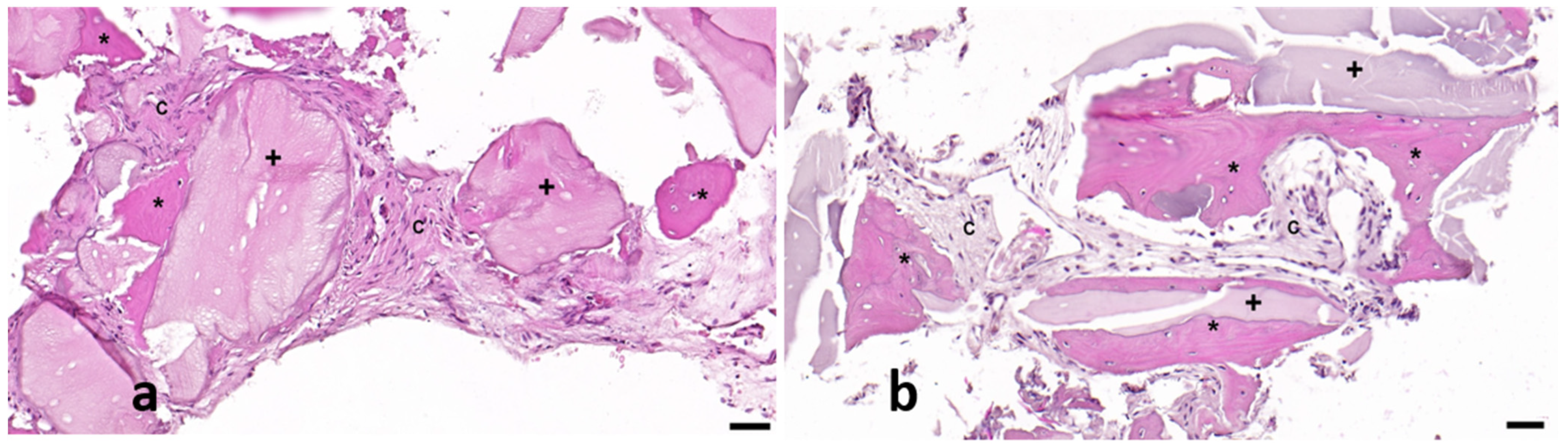
3.1.2. Histological Results
- –
- New Bone Formation
- CONTROL: Normal distribution of new bone formation skewness 0.2, kurtosis 1.1).
- TEST: Left-skewed (−0.7), leptokurtic (3.9) distribution with superior bone formation.
- TEST > CONTROL (42.3% vs. 25.1%).
- –
- Residual Debris
- CONTROL: Right-skewed (0.6), leptokurtic (4.2).
- TEST: Right-skewed (1.1), leptokurtic (3.2) distribution.
- TEST > CONTROL (8.8% vs. 1.8%).
- –
- Connective Tissue Composition
- CONTROL: Approximately normal distribution (skewness −0.3, kurtosis 1.5).
- TEST: Near-normal distribution (skewness −0.006, kurtosis 1.1).
- TEST < CONTROL (48.8% vs. 73.0%).
3.1.3. Clinical Results
3.2. Inferential Analysis of Histological Results
4. Discussion
4.1. Key Findings and Clinical Implications
4.2. Mechanistic Insights
4.3. Clinical and Technical Considerations
4.4. Conclusions
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langer, R.; Tirrell, D.A. Designing materials for biology and medicine. Nature 2004, 428, 487–492. [Google Scholar] [CrossRef]
- Miron, R.J.; Zhang, Y.F. Osteoinduction: A review of old concepts with new standards. J. Dent. Res. 2012, 91, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J. Optimized bone grafting. Periodontology 2000 2024, 94, 143–160. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Vinitha, B.; Fathima, G. Bone grafts in dentistry. J. Pharm. Bioallied Sci. 2013, 5, S125–S127. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Ridge alterations following implant placement in fresh extraction sockets: An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 645–652. [Google Scholar] [CrossRef]
- Cardaropoli, G.; Araújo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Ridge alterations following tooth extraction with and without flap elevation: An experimental study in the dog. Clin. Oral Implant. Res. 2009, 20, 545–549. [Google Scholar] [CrossRef]
- Araújo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontology 2000 2015, 68, 122–134. [Google Scholar] [CrossRef]
- Misawa, M.; Lindhe, J.; Araújo, M.G. The alveolar process following single-tooth extraction: A study of maxillary incisor and premolar sites in man. Clin. Oral Implant. Res. 2016, 27, 884–889. [Google Scholar] [CrossRef]
- Tomasi, C.; Sanz, M.; Cecchinato, D.; Pjetursson, B.; Ferrus, J.; Lang, N.P.; Lindhe, J. Bone dimensional variations at implants placed in fresh extraction sockets: A multilevel multivariate analysis. Clin. Oral Implant. Res. 2010, 21, 30–36. [Google Scholar] [CrossRef]
- Couso-Queiruga, E.; Stuhr, S.; Tattan, M.; Chambrone, L.; Avila-Ortiz, G. Post-extraction dimensional changes: A systematic review and meta-analysis. J. Clin. Periodontol. 2021, 48, 126–144. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Moya-Villaescusa, M.J.; Sánchez-Pérez, A. Measurement of ridge alterations following tooth removal: A radiographic study in humans. Clin. Oral Implant. Res. 2010, 21, 237–242. [Google Scholar] [CrossRef]
- Pommer, B.; Zechner, W.; Watzek, G.; Palmer, R. Chapter 11: To graft or not to graft? Evidence-based guide to decision making in oral bone graft surgery. In Bone Grafting; Alessandro, Z., Batista, D.M.J., Eds.; InTech: Rijeka, Croatia, 2012. [Google Scholar]
- Abdelhamid, A. Alveolar bone preservation. Biological basis and techniques. Int. J. Dent. Sci. Res. 2017, 5, 56–68. [Google Scholar] [CrossRef]
- Keith, J.D.; Salama, M.A. Ridge preservation and augmentation using regenerative materials to enhance implant predictability and esthetics. Compend. Contin. Educ. Dent. 2007, 28, 614–621. [Google Scholar]
- Gargallo, M.G.; García, S.Y.; Martínez, A.B. Técnicas de preservación de alveolo y de aumento del reborde alveolar: Revisión de la literatura. Av. Periodoncia Implantol. Oral 2016, 28, 71–81. [Google Scholar]
- Afrashtehfar, K.I.; Kurtzman, G.M.; Mahesh, L. Improving oral rehabilitation through the preservation of the tissues through alveolar preservation. J. Adv. Prosthodont. 2012, 4, 174–178. [Google Scholar] [CrossRef]
- Hämmerle, C.H.F.; Araújo, M.G.; Simion, M. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin. Oral Implant. Res. 2012, 23, 80–82. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone grafts and substitutes in dentistry: A review of current trends and developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef]
- Norton, M.R.; Odell, E.W.; Thompson, I.D.; Cook, R.J. Efficacy of bovine bone mineral for alveolar augmentation: A human histologic study. Clin. Oral Implant. Res. 2003, 14, 775–783. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Wachtel, H.C.; Langford, A.; Bernimoulin, J.P.; Reichart, P. Guided bone regeneration next to osseointegrated implants in humans. Int. J. Oral Maxillofac. Implant. 1991, 6, 127–135. [Google Scholar]
- Wachtel, H.; Schenk, G.; Böhm, S.; Weng, D.; Zuhr, O.; Hürzeler, M.B. Microsurgical access flap and enamel matrix derivative for the treatment of periodontal intrabony defects: A controlled clinical study. J. Clin. Periodontol. 2003, 30, 496–504. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Deflorian, M.; Testori, T.; Mandelli, F.; Nagursky, H.; Vinci, R. Alveolar socket preservation with demineralised bovine bone mineral and a collagen matrix. J. Periodontal Implant Sci. 2017, 47, 194–210. [Google Scholar] [CrossRef]
- Artzi, Z.; Nemcovsky, C.E. The application of deproteinized bovine bone mineral for ridge preservation prior to implantation. Clinical and histological observations in a case report. J. Periodontol. 1998, 69, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.E.; Lang, N.P. Ridge preservation after tooth extraction. Clin. Oral Implant. Res. 2012, 23, 147–156. [Google Scholar] [CrossRef]
- De Angelis, P.; De Rosa, G.; Manicone, P.F.; De Giorgi, A.; Cavalcanti, C.; Speranza, A.; Grassi, R.; D’Addona, A. Hard and soft tissue evaluation of alveolar ridge preservation compared to spontaneous healing: A retrospective clinical and volumetric analysis. Int. J. Implant Dent. 2022, 8, 62. [Google Scholar] [CrossRef]
- Fischer, K.R.; Solderer, A.; Arlt, K.; Heumann, C.; Liu, C.C.; Schmidlin, P.R. Bone envelope for implant placement after alveolar ridge preservation: A systematic review and meta-analysis. Int. J. Implant Dent. 2022, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.S.; Bosshardt, D.D.; Gruber, R.; Buser, D. Long-term stability of contour augmentation in the esthetic zone: Histologic and histomorphometric evaluation of 12 human biopsies 14 to 80 months after augmentation. J. Periodontol. 2014, 85, 1549–1556. [Google Scholar] [CrossRef]
- Busenlechner, D.; Tangl, S.; Arnhart, C.; Redl, H.; Schuh, C.; Watzek, G.; Gruber, R. Resorption of deproteinized bovine bone mineral in a porcine calvaria augmentation model. Clin. Oral Implant. Res. 2012, 23, 95–99. [Google Scholar] [CrossRef]
- Mealey, B.L.; Keeling, F.; Palaiologou, A.A. Histologic wound healing in studies using different ridge preservation protocols: A review. Clin. Adv. Periodontics 2024, 14, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.; Linder, E.; Lindhe, J. Effect of a xenograft on early bone formation in extraction sockets: An experimental study in dog. Clin. Oral Implant. Res. 2009, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.; Linder, E.; Wennström, J.; Lindhe, J. The influence of bio-oss collagen on healing of an extraction socket: An experimental study in the dog. Int. J. Periodontics Restor. Dent. 2008, 28, 123–135. [Google Scholar]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.O.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wachtel 2003 EHI at 1 Week | ||
|---|---|---|
| Full closure | Without fibrin | 0 |
| Fibrin line | 1 | |
| Fibrin clot | 2 | |
| Incomplete closure | Partial necrosis | 3 |
| Total necrosis | 4 | |
| Category | No Graft | Graft |
|---|---|---|
| >75% | 1 (6.7%) | 13 (86.7%) |
| 75–50% | 11 (73.3%) | 2 (13.3%) |
| 50–25% | 3 (20%) | 0 (0%) |
| <25% | 0 (0%) | 0 (0%) |
| Mean | SE | SD | IQR | LCI | UCI | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|---|---|
| % New bone | ||||||||
| Test | 42.3 | 2.3 | 8.9 | 5.9 | 37.3 | 47.2 | −0.7 | 3.9 |
| Control | 25.1 | 2.1 | 8.4 | 7.9 | 20.4 | 29.8 | 0.2 | 1.1 |
| Residual bone | ||||||||
| Test | 8.8 | 0.7 | 2.7 | 0.7 | 7.2 | 10.3 | 1.1 | 3.2 |
| Control | 1.8 | 0.2 | 0.8 | 4.1 | 1.3 | 2.2 | 0.6 | 4.2 |
| Connective tissue | ||||||||
| Test | 48.8 | 2.5 | 10.0 | 43.2 | 54.4 | 5.93 | −0.006 | 1.1 |
| Control | 73.0 | 2.0 | 8.0 | 8.0 | 68.5 | 77.5 | −0.3 | 1.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Pérez, A.; Rodríguez-Sánchez, M.; Martínez-Cáceres, C.M.; Jornet-García, A.; Moya-Villaescusa, M.J. The Efficacy of a Deproteinized Bovine Bone Mineral Graft for Alveolar Ridge Preservation: A Histologic Study in Humans. Biomedicines 2025, 13, 1358. https://doi.org/10.3390/biomedicines13061358
Sánchez-Pérez A, Rodríguez-Sánchez M, Martínez-Cáceres CM, Jornet-García A, Moya-Villaescusa MJ. The Efficacy of a Deproteinized Bovine Bone Mineral Graft for Alveolar Ridge Preservation: A Histologic Study in Humans. Biomedicines. 2025; 13(6):1358. https://doi.org/10.3390/biomedicines13061358
Chicago/Turabian StyleSánchez-Pérez, Arturo, Marcos Rodríguez-Sánchez, Carlos Manuel Martínez-Cáceres, Alfonso Jornet-García, and María José Moya-Villaescusa. 2025. "The Efficacy of a Deproteinized Bovine Bone Mineral Graft for Alveolar Ridge Preservation: A Histologic Study in Humans" Biomedicines 13, no. 6: 1358. https://doi.org/10.3390/biomedicines13061358
APA StyleSánchez-Pérez, A., Rodríguez-Sánchez, M., Martínez-Cáceres, C. M., Jornet-García, A., & Moya-Villaescusa, M. J. (2025). The Efficacy of a Deproteinized Bovine Bone Mineral Graft for Alveolar Ridge Preservation: A Histologic Study in Humans. Biomedicines, 13(6), 1358. https://doi.org/10.3390/biomedicines13061358