

Pushing the Limits of Interlimb Connectivity: Neuromodulation and Beyond
 , ,
, ,
Abstract

1. Introduction
2. Methods
3. Cycling to Enhance Proprio-Spinal Connectivity and Improve Walking in Neurological Conditions Affecting Sensorimotor Function
3.1. Leg Cycling Improves Walking Speed, Endurance, and Balance
3.1.1. Leg Cycling Improves Walking Speed
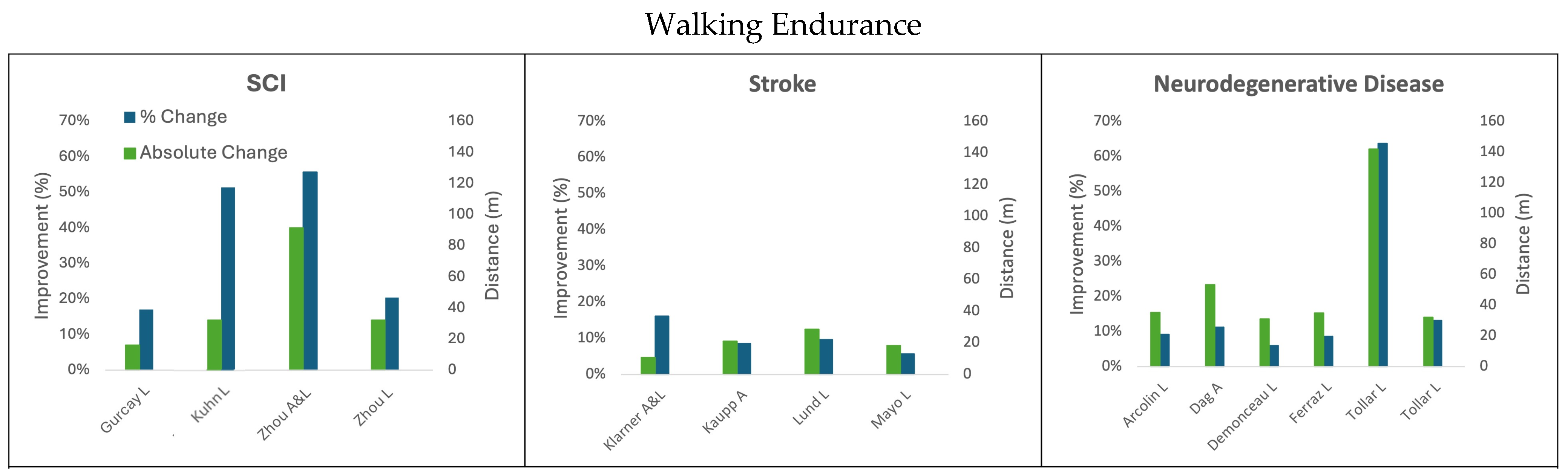
3.1.2. Leg Cycling Improves Walking Endurance Measured with the 6MWT
3.1.3. Leg Cycling Improves Balance on the BBS
3.2. The Addition of the Arms During Cycling Improves Functional Walking, Balance, and Electrophysiological Outcomes Relative to Legs-Only Cycling
3.3. Enhanced Interlimb Coupling After Arm and Leg Cycling
3.4. Arm Cycling Alone Can Improve Walking and Enhance Interlimb Coupling
4. Methods to Further Enhance Proprio-Spinal Connectivity to Improve Walking After Neural Injury
4.1. Functional Electrical Stimulation to Enhance the Effects of Arm and Leg Cycling
4.2. Implementation of Cycling Assisted by Functional Electrical Stimulation in an Acute Care Setting
4.3. High-Intensity Interval Training to Enhance Improvements of Arm and Leg Cycling
4.4. Paired Spinal Cord Stimulation to Improve Walking After Neural Injury
4.4.1. Epidural Spinal Cord Stimulation (eSCS)
4.4.2. Non-Invasive Transcutaneous Spinal Cord Stimulation (tSCS)
4.4.3. Combining Invasive and Non-Invasive Spinal Stimulation
4.5. Development of Coordinated Arm and Leg Rehabilitation Robotics
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruijn, S.M.; Meijer, O.G.; Beek, P.J.; van Dieën, J.H. The effects of arm swing on human gait stability. J. Exp. Biol. 2010, 213, 3945–3952. [Google Scholar] [CrossRef]
- Meyns, P.; Bruijn, S.M.; Duysens, J. The how and why of arm swing during human walking. Gait Posture 2013, 38, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Bernad-Elazari, H.; Nobel, T.; Thaler, A.; Peruzzi, A.; Plotnik, M.; Giladi, N.; Hausdorff, J.M. Effects of Aging on Arm Swing during Gait: The Role of Gait Speed and Dual Tasking. PLoS ONE 2015, 10, e0136043. [Google Scholar] [CrossRef] [PubMed]
- Dietz, V. Do human bipeds use quadrupedal coordination? Trends Neurosci. 2002, 25, 462–467. [Google Scholar] [CrossRef]
- Frigon, A. The neural control of interlimb coordination during mammalian locomotion. J. Neurophysiol. 2017, 117, 2224–2241. [Google Scholar] [CrossRef]
- Zehr, E.P.; Barss, T.S.; Dragert, K.; Frigon, A.; Vasudevan, E.V.; Haridas, C.; Hundza, S.; Kaupp, C.; Klarner, T.; Klimstra, M.; et al. Neuromechanical interactions between the limbs during human locomotion: An evolutionary perspective with translation to rehabilitation. Exp. Brain Res. 2016, 234, 3059–3081. [Google Scholar] [CrossRef] [PubMed]
- Juvin, L.; Simmers, J.; Morin, D. Propriospinal circuitry underlying interlimb coordination in mammalian quadrupedal locomotion. J. Neurosci. 2005, 25, 6025–6035. [Google Scholar] [CrossRef]
- Juvin, L.; Le Gal, J.P.; Simmers, J.; Morin, D. Cervicolumbar coordination in mammalian quadrupedal locomotion: Role of spinal thoracic circuitry and limb sensory inputs. J. Neurosci. 2012, 32, 953–965. [Google Scholar] [CrossRef]
- Yamaguchi, T. Descending pathways eliciting forelimb stepping in the lateral funiculus: Experimental studies with stimulation and lesion of the cervical cord in decerebrate cats. Brain Res. 1986, 379, 125–136. [Google Scholar] [CrossRef]
- Balter, J.E.; Zehr, E.P. Neural coupling between the arms and legs during rhythmic locomotor-like cycling movement. J. Neurophysiol. 2007, 97, 1809–1818. [Google Scholar] [CrossRef]
- Ferris, D.P.; Huang, H.J.; Kao, P.C. Moving the arms to activate the legs. Exerc. Sport Sci. Rev. 2006, 34, 113–120. [Google Scholar] [CrossRef]
- Frigon, A.; Collins, D.F.; Zehr, E.P. Effect of rhythmic arm movement on reflexes in the legs: Modulation of soleus H-reflexes and somatosensory conditioning. J. Neurophysiol. 2004, 91, 1516–1523. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.J.; Ferris, D.P. Upper and lower limb muscle activation is bidirectionally and ipsilaterally coupled. Med. Sci. Sports Exerc. 2009, 41, 1778–1789. [Google Scholar] [CrossRef] [PubMed]
- Luu, J.; Johnsen, J.F.; Passillé, A.M.d.; Rushen, J. Which measures of acceleration best estimate the duration of locomotor play by dairy calves? Appl. Anim. Behav. Sci. 2013, 148, 21–27. [Google Scholar] [CrossRef]
- Zehr, E.P.; Hundza, S.R.; Vasudevan, E.V. The quadrupedal nature of human bipedal locomotion. Exerc. Sport Sci. Rev. 2009, 37, 102–108. [Google Scholar] [CrossRef]
- Zhou, R.; Parhizi, B.; Assh, J.; Alvarado, L.; Ogilvie, R.; Chong, S.L.; Mushahwar, V.K. Effect of cervicolumbar coupling on spinal reflexes during cycling after incomplete spinal cord injury. J. Neurophysiol. 2018, 120, 3172–3186. [Google Scholar] [CrossRef]
- Lamont, E.V.; Zehr, E.P. Task-specific modulation of cutaneous reflexes expressed at functionally relevant gait cycle phases during level and incline walking and stair climbing. Exp. Brain Res. 2006, 173, 185–192. [Google Scholar] [CrossRef]
- Hodgson, J.A.; Roy, R.R.; de Leon, R.; Dobkin, B.; Edgerton, V.R. Can the mammalian lumbar spinal cord learn a motor task? Med. Sci. Sports Exerc. 1994, 26, 1491–1497. [Google Scholar] [CrossRef]
- Dietz, V.; Colombo, G.; Jensen, L.; Baumgartner, L. Locomotor capacity of spinal cord in paraplegic patients. Ann. Neurol. 1995, 37, 574–582. [Google Scholar] [CrossRef]
- Colombo, G.; Wirz, M.; Dietz, V. Effect of locomotor training related to clinical and electrophysiological examinations in spinal cord injured humans. Ann. N. Y. Acad. Sci. 1998, 860, 536–538. [Google Scholar] [CrossRef]
- Wernig, A.; Müller, S. Laufband locomotion with body weight support improved walking in persons with severe spinal cord injuries. Paraplegia 1992, 30, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Harkema, S.J.; Hurley, S.L.; Patel, U.K.; Requejo, P.S.; Dobkin, B.H.; Edgerton, V.R. Human lumbosacral spinal cord interprets loading during stepping. J. Neurophysiol. 1997, 77, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Barbeau, H.; Norman, K.; Fung, J.; Visintin, M.; Ladouceur, M. Does neurorehabilitation play a role in the recovery of walking in neurological populations? Ann. N. Y. Acad. Sci. 1998, 860, 377–392. [Google Scholar] [CrossRef]
- Harkema, S.J.; Hillyer, J.; Schmidt-Read, M.; Ardolino, E.; Sisto, S.A.; Behrman, A.L. Locomotor training: As a treatment of spinal cord injury and in the progression of neurologic rehabilitation. Arch. Phys. Med. Rehabil. 2012, 93, 1588–1597. [Google Scholar] [CrossRef] [PubMed]
- Field-Fote, E.C.; Roach, K.E. Influence of a locomotor training approach on walking speed and distance in people with chronic spinal cord injury: A randomized clinical trial. Phys. Ther. 2011, 91, 48–60. [Google Scholar] [CrossRef]
- Gama, G.L.; Celestino, M.L.; Barela, J.A.; Forrester, L.; Whitall, J.; Barela, A.M. Effects of Gait Training with Body Weight Support on a Treadmill Versus Overground in Individuals with Stroke. Arch. Phys. Med. Rehabil. 2017, 98, 738–745. [Google Scholar] [CrossRef]
- Zhou, R.; Alvarado, L.; Ogilvie, R.; Chong, S.L.; Shaw, O.; Mushahwar, V.K. Non-gait-specific intervention for the rehabilitation of walking after SCI: Role of the arms. J. Neurophysiol. 2018, 119, 2194–2211. [Google Scholar] [CrossRef]
- Klarner, T.; Barss, T.S.; Sun, Y.; Kaupp, C.; Loadman, P.M.; Zehr, E.P. Long-Term Plasticity in Reflex Excitability Induced by Five Weeks of Arm and Leg Cycling Training after Stroke. Brain Sci. 2016, 6, 54. [Google Scholar] [CrossRef]
- Ambrosini, E.; Parati, M.; Peri, E.; De Marchis, C.; Nava, C.; Pedrocchi, A.; Ferriero, G.; Ferrante, S. Changes in leg cycling muscle synergies after training augmented by functional electrical stimulation in subacute stroke survivors: A pilot study. J. Neuroeng. Rehabil. 2020, 17, 35. [Google Scholar] [CrossRef]
- Arcolin, I.; Pisano, F.; Delconte, C.; Godi, M.; Schieppati, M.; Mezzani, A.; Picco, D.; Grasso, M.; Nardone, A. Intensive cycle ergometer training improves gait speed and endurance in patients with Parkinson’s disease: A comparison with treadmill training. Restor. Neurol. Neurosci. 2016, 34, 125–138. [Google Scholar] [CrossRef]
- Cakt, B.D.; Nacir, B.; Genç, H.; Saraçoğlu, M.; Karagöz, A.; Erdem, H.R.; Ergün, U. Cycling progressive resistance training for people with multiple sclerosis: A randomized controlled study. Am. J. Phys. Med. Rehabil. 2010, 89, 446–457. [Google Scholar] [CrossRef]
- Chang, H.C.; Lu, C.S.; Chiou, W.D.; Chen, C.C.; Weng, Y.H.; Chang, Y.J. An 8-Week Low-Intensity Progressive Cycling Training Improves Motor Functions in Patients with Early-Stage Parkinson’s Disease. J. Clin. Neurol. 2018, 14, 225–233. [Google Scholar] [CrossRef]
- Dağ, F.; Çimen, Ö.B.; Doğu, O. The effects of arm crank training on aerobic capacity, physical performance, quality of life, and health-related disability in patients with Parkinson’s disease. Ir. J. Med. Sci. 2022, 191, 1341–1348. [Google Scholar] [CrossRef]
- Demonceau, M.; Maquet, D.; Jidovtseff, B.; Donneau, A.F.; Bury, T.; Croisier, J.L.; Crielaard, J.M.; Rodriguez de la Cruz, C.; Delvaux, V.; Garraux, G. Effects of twelve weeks of aerobic or strength training in addition to standard care in Parkinson’s disease: A controlled study. Eur. J. Phys. Rehabil. Med. 2017, 53, 184–200. [Google Scholar] [CrossRef]
- Ferraz, D.D.; Trippo, K.V.; Duarte, G.P.; Neto, M.G.; Bernardes Santos, K.O.; Filho, J.O. The Effects of Functional Training, Bicycle Exercise, and Exergaming on Walking Capacity of Elderly Patients with Parkinson Disease: A Pilot Randomized Controlled Single-blinded Trial. Arch. Phys. Med. Rehabil. 2018, 99, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Gurcay, E.; Karaahmet, O.Z.; Cankurtaran, D.; Nazlı, F.; Umay, E.; Güzel, Ş.; Gurcay, A.G. Functional electrical stimulation cycling in patients with chronic spinal cord injury: A pilot study. Int. J. Neurosci. 2022, 132, 421–427. [Google Scholar] [CrossRef]
- Kaupp, C.; Pearcey, G.E.P.; Klarner, T.; Sun, Y.; Cullen, H.; Barss, T.S.; Zehr, E.P. Rhythmic arm cycling training improves walking and neurophysiological integrity in chronic stroke: The arms can give legs a helping hand in rehabilitation. J. Neurophysiol. 2018, 119, 1095–1112. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, D.; Leichtfried, V.; Schobersberger, W. Four weeks of functional electrical stimulated cycling after spinal cord injury: A clinical cohort study. Int. J. Rehabil. Res. 2014, 37, 243–250. [Google Scholar] [CrossRef]
- Lund, C.; Dalgas, U.; Grønborg, T.K.; Andersen, H.; Severinsen, K.; Riemenschneider, M.; Overgaard, K. Balance and walking performance are improved after resistance and aerobic training in persons with chronic stroke. Disabil. Rehabil. 2018, 40, 2408–2415. [Google Scholar] [CrossRef]
- Mayo, N.E.; MacKay-Lyons, M.J.; Scott, S.C.; Moriello, C.; Brophy, J. A randomized trial of two home-based exercise programmes to improve functional walking post-stroke. Clin. Rehabil. 2013, 27, 659–671. [Google Scholar] [CrossRef]
- McGough, E.L.; Robinson, C.A.; Nelson, M.D.; Houle, R.; Fraser, G.; Handley, L.; Jones, E.R.; Amtmann, D.; Kelly, V.E. A Tandem Cycling Program: Feasibility and Physical Performance Outcomes in People with Parkinson Disease. J. Neurol. Phys. Ther. 2016, 40, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, A.; Lungu, O.; Duchesne, C.; Robillard, M.; Bore, A.; Bobeuf, F.; Plamondon, R.; Lafontaine, A.L.; Gheysen, F.; Bherer, L.; et al. A 12-Week Cycling Training Regimen Improves Gait and Executive Functions Concomitantly in People with Parkinson’s Disease. Front. Hum. Neurosci. 2017, 10, 690. [Google Scholar] [CrossRef] [PubMed]
- Shariat, A.; Nakhostin Ansari, N.; Honarpishe, R.; Moradi, V.; Hakakzadeh, A.; Cleland, J.A.; Kordi, R. Effect of cycling and functional electrical stimulation with linear and interval patterns of timing on gait parameters in patients after stroke: A randomized clinical trial. Disabil. Rehabil. 2021, 43, 1890–1896. [Google Scholar] [CrossRef]
- Tollár, J.; Nagy, F.; Hortobágyi, T. Vastly Different Exercise Programs Similarly Improve Parkinsonian Symptoms: A Randomized Clinical Trial. Gerontology 2019, 65, 120–127. [Google Scholar] [CrossRef]
- Tollár, J.; Nagy, F.; Tóth, B.E.; Török, K.; Szita, K.; Csutorás, B.; Moizs, M.; Hortobágyi, T. Exercise Effects on Multiple Sclerosis Quality of Life and Clinical-Motor Symptoms. Med. Sci. Sports Exerc. 2020, 52, 1007–1014. [Google Scholar] [CrossRef]
- Yaşar, E.; Yılmaz, B.; Göktepe, S.; Kesikburun, S. The effect of functional electrical stimulation cycling on late functional improvement in patients with chronic incomplete spinal cord injury. Spinal Cord 2015, 53, 866–869. [Google Scholar] [CrossRef]
- Zehr, E.P.; Balter, J.E.; Ferris, D.P.; Hundza, S.R.; Loadman, P.M.; Stoloff, R.H. Neural regulation of rhythmic arm and leg movement is conserved across human locomotor tasks. J. Physiol. 2007, 582, 209–227. [Google Scholar] [CrossRef]
- Raasch, C.C.; Zajac, F.E. Locomotor strategy for pedaling: Muscle groups and biomechanical functions. J. Neurophysiol. 1999, 82, 515–525. [Google Scholar] [CrossRef]
- Barbosa, D.; Santos, C.P.; Martins, M. The application of cycling and cycling combined with feedback in the rehabilitation of stroke patients: A review. J. Stroke Cerebrovasc. Dis. 2015, 24, 253–273. [Google Scholar] [CrossRef]
- Musselman, K.E. Clinical significance testing in rehabilitation research: What, why, and how? Phys. Ther. Rev. 2007, 12, 287–296. [Google Scholar] [CrossRef]
- Lam, T.; Noonan, V.K.; Eng, J.J. A systematic review of functional ambulation outcome measures in spinal cord injury. Spinal Cord 2008, 46, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Olmos, L.E.; Freixes, O.; Gatti, M.A.; Cozzo, D.A.; Fernandez, S.A.; Vila, C.J.; Agrati, P.E.; Rubel, I.F. Comparison of gait performance on different environmental settings for patients with chronic spinal cord injury. Spinal Cord 2008, 46, 331–334. [Google Scholar] [CrossRef]
- Tilson, J.K.; Sullivan, K.J.; Cen, S.Y.; Rose, D.K.; Koradia, C.H.; Azen, S.P.; Duncan, P.W. Meaningful gait speed improvement during the first 60 days poststroke: Minimal clinically important difference. Phys. Ther. 2010, 90, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Hosoi, Y.; Kamimoto, T.; Sakai, K.; Yamada, M.; Kawakami, M. Estimation of minimal detectable change in the 10-meter walking test for patients with stroke: A study stratified by gait speed. Front. Neurol. 2023, 14, 1219505. [Google Scholar] [CrossRef] [PubMed]
- Steffen, T.; Seney, M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified Parkinson disease rating scale in people with parkinsonism. Phys. Ther. 2008, 88, 733–746. [Google Scholar] [CrossRef]
- Lang, J.T.; Kassan, T.O.; Devaney, L.L.; Colon-Semenza, C.; Joseph, M.F. Test-Retest Reliability and Minimal Detectable Change for the 10-Meter Walk Test in Older Adults with Parkinson’s disease. J. Geriatr. Phys. Ther. 2016, 39, 165–170. [Google Scholar] [CrossRef]
- Williams, K.L.; Low Choy, N.L.; Brauer, S.G. Are Changes in Gait and Balance Across the Disease Step Rating Scale in Multiple Sclerosis Statistically Significant and Clinically Meaningful? Arch. Phys. Med. Rehabil. 2016, 97, 1502–1508. [Google Scholar] [CrossRef]
- Forrest, G.F.; Hutchinson, K.; Lorenz, D.J.; Buehner, J.J.; Vanhiel, L.R.; Sisto, S.A.; Basso, D.M. Are the 10 meter and 6 minute walk tests redundant in patients with spinal cord injury? PLoS ONE 2014, 9, e94108. [Google Scholar] [CrossRef]
- Fulk, G.D.; He, Y. Minimal Clinically Important Difference of the 6-Minute Walk Test in People with Stroke. J. Neurol. Phys. Ther. 2018, 42, 235–240. [Google Scholar] [CrossRef]
- Baert, I.; Freeman, J.; Smedal, T.; Dalgas, U.; Romberg, A.; Kalron, A.; Conyers, H.; Elorriaga, I.; Gebara, B.; Gumse, J.; et al. Responsiveness and clinically meaningful improvement, according to disability level, of five walking measures after rehabilitation in multiple sclerosis: A European multicenter study. Neurorehabil. Neural Repair. 2014, 28, 621–631. [Google Scholar] [CrossRef]
- Stevenson, T.J. Detecting change in patients with stroke using the Berg Balance Scale. Aust. J. Physiother. 2001, 47, 29–38. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Al-Eisa, E.S.; Anwer, S.; Sarkar, B. Reliability, validity, and responsiveness of three scales for measuring balance in patients with chronic stroke. BMC Neurol. 2018, 18, 141. [Google Scholar] [CrossRef]
- Hiengkaew, V.; Jitaree, K.; Chaiyawat, P. Minimal detectable changes of the Berg Balance Scale, Fugl-Meyer Assessment Scale, Timed “Up & Go” Test, gait speeds, and 2-minute walk test in individuals with chronic stroke with different degrees of ankle plantarflexor tone. Arch. Phys. Med. Rehabil. 2012, 93, 1201–1208. [Google Scholar] [CrossRef]
- Gervasoni, E.; Jonsdottir, J.; Montesano, A.; Cattaneo, D. Minimal Clinically Important Difference of Berg Balance Scale in People with Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2017, 98, 337–340.e2. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, E.; De Marchis, C.; Pedrocchi, A.; Ferrigno, G.; Monticone, M.; Schmid, M.; D’Alessio, T.; Conforto, S.; Ferrante, S. Neuro-Mechanics of Recumbent Leg Cycling in Post-Acute Stroke Patients. Ann. Biomed. Eng. 2016, 44, 3238–3251. [Google Scholar] [CrossRef] [PubMed]
- Klarner, T.; Barss, T.S.; Sun, Y.; Kaupp, C.; Loadman, P.M.; Zehr, E.P. Exploiting Interlimb Arm and Leg Connections for Walking Rehabilitation: A Training Intervention in Stroke. Neural Plast. 2016, 2016, 1517968. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, T.; Mezzarane, R.A.; Klarner, T.; Barss, T.S.; Hundza, S.R.; Komiyama, T.; Zehr, E.P. Neural mechanisms influencing interlimb coordination during locomotion in humans: Presynaptic modulation of forearm H-reflexes during leg cycling. PLoS ONE 2013, 8, e76313. [Google Scholar] [CrossRef]
- Mezzarane, R.A.; Klimstra, M.; Lewis, A.; Hundza, S.R.; Zehr, E.P. Interlimb coupling from the arms to legs is differentially specified for populations of motor units comprising the compound H-reflex during “reduced” human locomotion. Exp. Brain Res. 2011, 208, 157–168. [Google Scholar] [CrossRef]
- Zehr, E.P.; Haridas, C. Modulation of cutaneous reflexes in arm muscles during walking: Further evidence of similar control mechanisms for rhythmic human arm and leg movements. Exp. Brain Res. 2003, 149, 260–266. [Google Scholar] [CrossRef]
- Sarica, Y.; Ertekin, C. Descending lumbosacral cord potentials (DLCP) evoked by stimulation of the median nerve. Brain Res. 1985, 325, 299–301. [Google Scholar] [CrossRef]
- Zehr, E.P.; Kido, A. Neural control of rhythmic, cyclical human arm movement: Task dependency, nerve specificity and phase modulation of cutaneous reflexes. J. Physiol. 2001, 537, 1033–1045. [Google Scholar] [CrossRef]
- Zhou, R.; Alvarado, L.; Kim, S.; Chong, S.L.; Mushahwar, V.K. Modulation of corticospinal input to the legs by arm and leg cycling in people with incomplete spinal cord injury. J. Neurophysiol. 2017, 118, 2507–2519. [Google Scholar] [CrossRef]
- Hundza, S.R.; Zehr, E.P. Suppression of soleus H-reflex amplitude is graded with frequency of rhythmic arm cycling. Exp. Brain Res. 2009, 193, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Loadman, P.M.; Zehr, E.P. Rhythmic arm cycling produces a non-specific signal that suppresses Soleus H-reflex amplitude in stationary legs. Exp. Brain Res. 2007, 179, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Sosnoff, J.J.; Motl, R.W. Effect of acute unloaded arm versus leg cycling exercise on the soleus H-reflex in adults with multiple sclerosis. Neurosci. Lett. 2010, 479, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Zehr, E.P.; Klimstra, M.; Johnson, E.A.; Carroll, T.J. Rhythmic leg cycling modulates forearm muscle H-reflex amplitude and corticospinal tract excitability. Neurosci. Lett. 2007, 419, 10–14. [Google Scholar] [CrossRef]
- Klarner, T.; Zehr, E.P. Sherlock Holmes and the curious case of the human locomotor central pattern generator. J. Neurophysiol. 2018, 120, 53–77. [Google Scholar] [CrossRef]
- Nathan, P.W.; Smith, M.C. Fasciculi proprii of the spinal cord in man. Brain 1959, 82, 610–668. [Google Scholar] [CrossRef]
- Scremin, A.M.; Kurta, L.; Gentili, A.; Wiseman, B.; Perell, K.; Kunkel, C.; Scremin, O.U. Increasing muscle mass in spinal cord injured persons with a functional electrical stimulation exercise program. Arch. Phys. Med. Rehabil. 1999, 80, 1531–1536. [Google Scholar] [CrossRef]
- Faghri, P.D.; Glaser, R.M.; Figoni, S.F. Functional electrical stimulation leg cycle ergometer exercise: Training effects on cardiorespiratory responses of spinal cord injured subjects at rest and during submaximal exercise. Arch. Phys. Med. Rehabil. 1992, 73, 1085–1093. [Google Scholar]
- Martin, R.; Sadowsky, C.; Obst, K.; Meyer, B.; McDonald, J. Functional electrical stimulation in spinal cord injury: From theory to practice. Top. Spinal Cord Inj. Rehabil. 2012, 18, 28–33. [Google Scholar] [CrossRef]
- Poulsen, J.B.; Møller, K.; Jensen, C.V.; Weisdorf, S.; Kehlet, H.; Perner, A. Effect of transcutaneous electrical muscle stimulation on muscle volume in patients with septic shock. Crit. Care Med. 2011, 39, 456–461. [Google Scholar] [CrossRef]
- Mac-Thiong, J.M.; Richard-Denis, A.; Petit, Y.; Bernard, F.; Barthélemy, D.; Dionne, A.; Magnuson, D.S.K. Protocol for rapid onset of mobilisation in patients with traumatic spinal cord injury (PROMPT-SCI) study: A single-arm proof-of-concept trial of early in-bed leg cycling following acute traumatic spinal cord injury. BMJ Open 2021, 11, e049884. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Haldimann, M.; Stocker, N.; Pedrini, B.; Sampaio, A.; Hunt, K.J. Development of a Belt-actuated Robotic Platform for Early Rehabilitation. In Proceedings of the 2022 International Conference on Rehabilitation Robotics (ICORR), Rotterdam, The Netherlands, 25–29 July 2022. [Google Scholar] [CrossRef]
- Jacobs, P.L.; Nash, M.S. Exercise recommendations for individuals with spinal cord injury. Sports Med. 2004, 34, 727–751. [Google Scholar] [CrossRef] [PubMed]
- Duffell, L.D.; Donaldson Nde, N.; Perkins, T.A.; Rushton, D.N.; Hunt, K.J.; Kakebeeke, T.H.; Newham, D.J. Long-term intensive electrically stimulated cycling by spinal cord-injured people: Effect on muscle properties and their relation to power output. Muscle Nerve 2008, 38, 1304–1311. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Poarch, H.J.; Dolbow, D.D.; Castillo, T.; Gater, D.R. Effect of adjusting pulse durations of functional electrical stimulation cycling on energy expenditure and fatigue after spinal cord injury. J. Rehabil. Res. Dev. 2014, 51, 1455–1468. [Google Scholar] [CrossRef] [PubMed]
- Everaert, D.G.; Okuma, Y.; Abdollah, V.; Ho, C. Timing and dosage of FES cycling early after acute spinal cord injury: A case series report. J. Spinal Cord Med. 2021, 44, S250–S255. [Google Scholar] [CrossRef]
- Hachmann, J.T.; Yousak, A.; Wallner, J.J.; Gad, P.N.; Edgerton, V.R.; Gorgey, A.S. Epidural spinal cord stimulation as an intervention for motor recovery after motor complete spinal cord injury. J. Neurophysiol. 2021, 126, 1843–1859. [Google Scholar] [CrossRef]
- Courtine, G.; Roy, R.R.; Raven, J.; Hodgson, J.; McKay, H.; Yang, H.; Zhong, H.; Tuszynski, M.H.; Edgerton, V.R. Performance of locomotion and foot grasping following a unilateral thoracic corticospinal tract lesion in monkeys (Macaca mulatta). Brain 2005, 128, 2338–2358. [Google Scholar] [CrossRef]
- Friedli, L.; Rosenzweig, E.S.; Barraud, Q.; Schubert, M.; Dominici, N.; Awai, L.; Nielson, J.L.; Musienko, P.; Nout-Lomas, Y.; Zhong, H.; et al. Pronounced species divergence in corticospinal tract reorganization and functional recovery after lateralized spinal cord injury favors primates. Sci. Transl. Med. 2015, 7, 302ra134. [Google Scholar] [CrossRef]
- Rosenzweig, E.S.; Courtine, G.; Jindrich, D.L.; Brock, J.H.; Ferguson, A.R.; Strand, S.C.; Nout, Y.S.; Roy, R.R.; Miller, D.M.; Beattie, M.S.; et al. Extensive spontaneous plasticity of corticospinal projections after primate spinal cord injury. Nat. Neurosci. 2010, 13, 1505–1510. [Google Scholar] [CrossRef] [PubMed]
- Courtine, G.; Song, B.; Roy, R.R.; Zhong, H.; Herrmann, J.E.; Ao, Y.; Qi, J.; Edgerton, V.R.; Sofroniew, M.V. Recovery of supraspinal control of stepping via indirect propriospinal relay connections after spinal cord injury. Nat. Med. 2008, 14, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Gerasimenko, Y.; Musienko, P.; Bogacheva, I.; Moshonkina, T.; Savochin, A.; Lavrov, I.; Roy, R.R.; Edgerton, V.R. Propriospinal bypass of the serotonergic system that can facilitate stepping. J. Neurosci. 2009, 29, 5681–5689. [Google Scholar] [CrossRef]
- Asboth, L.; Friedli, L.; Beauparlant, J.; Martinez-Gonzalez, C.; Anil, S.; Rey, E.; Baud, L.; Pidpruzhnykova, G.; Anderson, M.A.; Shkorbatova, P.; et al. Cortico-reticulo-spinal circuit reorganization enables functional recovery after severe spinal cord contusion. Nat. Neurosci. 2018, 21, 576–588. [Google Scholar] [CrossRef]
- Harkema, S.; Gerasimenko, Y.; Hodes, J.; Burdick, J.; Angeli, C.; Chen, Y.; Ferreira, C.; Willhite, A.; Rejc, E.; Grossman, R.G.; et al. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: A case study. Lancet 2011, 377, 1938–1947. [Google Scholar] [CrossRef] [PubMed]
- Mayr, W.; Krenn, M.; Dimitrijevic, M.R. Epidural and transcutaneous spinal electrical stimulation for restoration of movement after incomplete and complete spinal cord injury. Curr. Opin. Neurol. 2016, 29, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Formento, E.; Minassian, K.; Wagner, F.; Mignardot, J.B.; Le Goff-Mignardot, C.G.; Rowald, A.; Bloch, J.; Micera, S.; Capogrosso, M.; Courtine, G. Electrical spinal cord stimulation must preserve proprioception to enable locomotion in humans with spinal cord injury. Nat. Neurosci. 2018, 21, 1728–1741. [Google Scholar] [CrossRef]
- Herman, R.; He, J.; D’Luzansky, S.; Willis, W.; Dilli, S. Spinal cord stimulation facilitates functional walking in a chronic, incomplete spinal cord injured. Spinal Cord 2002, 40, 65–68. [Google Scholar] [CrossRef]
- Wagner, F.B.; Mignardot, J.B.; Le Goff-Mignardot, C.G.; Demesmaeker, R.; Komi, S.; Capogrosso, M.; Rowald, A.; Seáñez, I.; Caban, M.; Pirondini, E.; et al. Targeted neurotechnology restores walking in humans with spinal cord injury. Nature 2018, 563, 65–71. [Google Scholar] [CrossRef]
- Kou, J.; Cai, M.; Xie, F.; Wang, Y.; Wang, N.; Xu, M. Complex Electrical Stimulation Systems in Motor Function Rehabilitation after Spinal Cord Injury. Complexity 2021, 2021, 2214762. [Google Scholar] [CrossRef]
- Carhart, M.R.; He, J.; Herman, R.; D’Luzansky, S.; Willis, W.T. Epidural spinal-cord stimulation facilitates recovery of functional walking following incomplete spinal-cord injury. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Courtine, G.; Gerasimenko, Y.; van den Brand, R.; Yew, A.; Musienko, P.; Zhong, H.; Song, B.; Ao, Y.; Ichiyama, R.M.; Lavrov, I.; et al. Transformation of nonfunctional spinal circuits into functional states after the loss of brain input. Nat. Neurosci. 2009, 12, 1333–1342. [Google Scholar] [CrossRef]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of Over-Ground Walking after Chronic Motor Complete Spinal Cord Injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Gill, M.L.; Grahn, P.J.; Calvert, J.S.; Linde, M.B.; Lavrov, I.A.; Strommen, J.A.; Beck, L.A.; Sayenko, D.G.; Van Straaten, M.G.; Drubach, D.I.; et al. Neuromodulation of lumbosacral spinal networks enables independent stepping after complete paraplegia. Nat. Med. 2018, 24, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Angeli, C.A.; Edgerton, V.R.; Gerasimenko, Y.P.; Harkema, S.J. Altering spinal cord excitability enables voluntary movements after chronic complete paralysis in humans. Brain 2014, 137, 1394–1409. [Google Scholar] [CrossRef]
- Barss, T.S.; Parhizi, B.; Porter, J.; Mushahwar, V.K. Neural Substrates of Transcutaneous Spinal Cord Stimulation: Neuromodulation across Multiple Segments of the Spinal Cord. J. Clin. Med. 2022, 11, 639. [Google Scholar] [CrossRef]
- Gerasimenko, Y.P.; Lu, D.C.; Modaber, M.; Zdunowski, S.; Gad, P.; Sayenko, D.G.; Morikawa, E.; Haakana, P.; Ferguson, A.R.; Roy, R.R.; et al. Noninvasive Reactivation of Motor Descending Control after Paralysis. J. Neurotrauma 2015, 32, 1968–1980. [Google Scholar] [CrossRef]
- Balykin, M.V.; Yakupov, R.N.; Mashin, V.V.; Kotova, E.Y.; Balykin, Y.M.; Gerasimenko, Y.P. The influence of non-invasive electrical stimulation of the spinal cord on the locomotor function of patients presenting with movement disorders of central genesis. Vopr. Kurortol. Fizioter. Lech. Fiz. Kult. 2017, 94, 4–9. [Google Scholar] [CrossRef]
- Solopova, I.A.; Sukhotina, I.A.; Zhvansky, D.S.; Ikoeva, G.A.; Vissarionov, S.V.; Baindurashvili, A.G.; Edgerton, V.R.; Gerasimenko, Y.P.; Moshonkina, T.R. Effects of spinal cord stimulation on motor functions in children with cerebral palsy. Neurosci. Lett. 2017, 639, 192–198. [Google Scholar] [CrossRef]
- Gerasimenko, Y.; Gorodnichev, R.; Moshonkina, T.; Sayenko, D.; Gad, P.; Reggie Edgerton, V. Transcutaneous electrical spinal-cord stimulation in humans. Ann. Phys. Rehabil. Med. 2015, 58, 225–231. [Google Scholar] [CrossRef]
- McHugh, L.V.; Miller, A.A.; Leech, K.A.; Salorio, C.; Martin, R.H. Feasibility and utility of transcutaneous spinal cord stimulation combined with walking-based therapy for people with motor incomplete spinal cord injury. Spinal Cord Ser. Cases 2020, 6, 104. [Google Scholar] [CrossRef]
- Angeli, C.A.; Gerasimenko, Y. Combined cervical transcutaneous with lumbosacral epidural stimulation improves voluntary control of stepping movements in spinal cord injured individuals. Front. Bioeng. Biotechnol. 2023, 11, 1073716. [Google Scholar] [CrossRef] [PubMed]
- Homma, K.; Hashino, S.; Arai, T. An upper limb motion assist system: Experiments with arm models. In Proceedings of the 1998 IEEE/RSJ International Conference on Intelligent Robots and Systems. Innovations in Theory, Practice and Applications (Cat. No.98CH36190), Victoria, BC, Canada, 17 October 1998; Volume 2, pp. 758–763. [Google Scholar] [CrossRef]
- Mao, Y.; Jin, X.; Gera Dutta, G.; Scholz, J.P.; Agrawal, S.K. Human movement training with a cable driven ARm EXoskeleton (CAREX). IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Hornby, T.G.; Landry, J.M.; Roth, H.; Schmit, B.D. A cable-driven locomotor training system for restoration of gait in human SCI. Gait Posture 2011, 33, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Alamdari, A.; Krovi, V. Robotic Physical Exercise and System (ROPES): A Cable-Driven Robotic Rehabilitation System for Lower-Extremity Motor Therapy. In Proceedings of the ASME 2015 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Boston, MA, USA, 2–5 August 2015. [Google Scholar]
- Chu, C.Y.; Patterson, R.M. Soft robotic devices for hand rehabilitation and assistance: A narrative review. J. Neuroeng. Rehabil. 2018, 15, 9. [Google Scholar] [CrossRef]
- Wernig, A.; Müller, S.; Nanassy, A.; Cagol, E. Laufband therapy based on ‘rules of spinal locomotion’ is effective in spinal cord injured persons. Eur. J. Neurosci. 1995, 7, 823–829. [Google Scholar] [CrossRef]
- Hornby, G.; Campbell, D.; Zemon, D.; Kahn, J. Clinical and quantitative evaluation of robotic-assisted treadmill walking to retrain ambulation after spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2005, 11, 1–17. [Google Scholar] [CrossRef]
- Dobkin, B.; Apple, D.; Barbeau, H.; Basso, M.; Behrman, A.; Deforge, D.; Ditunno, J.; Dudley, G.; Elashoff, R.; Fugate, L.; et al. Weight-supported treadmill vs over-ground training for walking after acute incomplete SCI. Neurology 2006, 66, 484–493. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Name [Reference #] | Number of Participants | Clinical Group | Training Mode | Training Frequency | Type of Cycling |
|---|---|---|---|---|---|
| Ambrosini et al., 2020 [29] | 9 | Stroke | 25 min sessions | 5× per week for 3 weeks | FES Leg Cycling |
| Arcolin et al., 2016 [30] | 16 | Parkinson’s Disease (PD) | 30 min twice per day and 60 min of stretching, strengthening, and balance exercises | 5× per week for 3 weeks | Leg Cycling |
| Cakt et al., 2010 [31] | 14 | Multiple Sclerosis (MS) | 15 sets of 4 min of cycling (2 min on high resistance followed by 2 min on low resistance or 2 min of rest) | 2× per week (non-consecutive days for 8 weeks | Leg Cycling |
| Chang et al., 2018 [32] | 13 | PD | Session 1 = 15 min Session 2 = 20 min Session 3 = 25 min Session 4–8 = 30 min Session 9–12 = 35 min Session 13–16 = 40 min | 2× per week for 8 weeks | Leg Cycling |
| Dağ et al., 2021 [33] | 13 | PD | 60 min | 3× per week for 8 weeks | Arm Cycling |
| Demonceau et al., 2017 [34] | 16 | PD | At least one 30–45 min of cycling at 50–60% of their peak workload (PWL)(continuous session) per week AND At least one interval cycling training session 16–24 min long plus warm up and cool down at 40–50% peak workload for 10 min each | 2–3× per week for 12 weeks with at least one rest day between sessions | Leg Cycling |
| Ferraz et al., 2018 [35] | 20 | PD | 50 min physiotherapy sessions with 30 min of leg cycling, 10 min of stretching, 5 min of calisthenics, and 5 min of respiration exercises | 3× per week for 8 weeks | Leg Cycling |
| Gurcay et al., 2022 [36] | 15 | Chronic spinal cord injury (SCI) | 30 min sessions with 20 min of cycling, a warm up (5 min), and a cool down (5 min) | 3× per week for 6 weeks | FES leg cycling |
| Kaupp et al., 2018 [37] | 19 | Stroke | 30 min | 3× per week for 5 weeks | Arm Cycling |
| Klarner et al., 2016 [28] | 19 | Stroke | 30 min | 3× per week for 5 weeks | Arm and Leg Cycling |
| Kuhn et al., 2014 [38] | 5 | Incomplete SCI (AIS C/D) | 20 min | 2× per week for 4 weeks | FES Leg Cycling |
| Lund et al., 2018 [39] | 13 | Stroke | 3 sets of 12 min at 75% heart rate reserve intensity with 5–10 min rest breaks in between | 3× per week for 12 weeks | Leg Cycling |
| Mayo et al., 2013 [40] | 28 | Stroke | Starting at a minimum of 15 min and building up to 30 min of training. Advised to exercise on the 6–20 scale Borg scale at an 11–15 intensity. | Daily for one year | Leg Cycling |
| McGough et al., 2016 [41] | 38 | PD | 60 min | 3× per week for 10 weeks | Leg Cycling |
| Nadeau et al., 2017 [42] | 19 | PD | Initially at 20 min at 60% exertion building to 40 min at 80% exertion over the 12 weeks | 3× per week for 12 weeks | Leg Cycling |
| Shariat et al., 2021 [43] Linear | 14 | Stroke | 28 min (8 without FES stimulation and 20 with stim) continuously | 3× per week for 4 weeks | FES Leg Cycling |
| Shariat et al., 2021 [43] Interval | 16 | Stroke | 28 min (8 without FES stimulation and 20 with stim) 20 min with stimulation are split into 4 × 5 min intervals | 3× per week for 4 weeks | FES Leg Cycling |
| Tollár et al., 2019 [44] | 25 | PD | 60 min including 5 min warm up and 5 min cool down | 5× per week for 5 weeks | Leg Cycling |
| Tollár et al., 2020 [45] | 14 | MS | 60 min | 5× per week for 5 weeks | Leg Cycling |
| Yaşar et al., 2015 [46] | 15 | Incomplete SCI (AIS C/D) | 60 min | 3× per week for 16 weeks | FES Leg Cycling |
| Zhou et al., 2018 [27] Arm and leg cycling | 7 | Incomplete SCI (AIS C/D) | 60 min | 5× per week for 12 weeks | Arm and FES Leg Cycling |
| Zhou et al., 2018 [27] Legs-only cycling | 8 | Incomplete SCI (AIS C/D) | 60 min | 5× per week for 12 weeks | FES Leg Cycling |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porter, J.A.; Barss, T.S.; Mann, D.J.; Karamzadeh, Z.; Okusanya, D.O.; Hemakumara, S.G.; Zehr, E.P.; Klarner, T.; Mushahwar, V.K. Pushing the Limits of Interlimb Connectivity: Neuromodulation and Beyond. Biomedicines 2025, 13, 1228. https://doi.org/10.3390/biomedicines13051228
Porter JA, Barss TS, Mann DJ, Karamzadeh Z, Okusanya DO, Hemakumara SG, Zehr EP, Klarner T, Mushahwar VK. Pushing the Limits of Interlimb Connectivity: Neuromodulation and Beyond. Biomedicines. 2025; 13(5):1228. https://doi.org/10.3390/biomedicines13051228
Chicago/Turabian StylePorter, Jane A., Trevor S. Barss, Darren J. Mann, Zahra Karamzadeh, Deborah O. Okusanya, Sisuri G. Hemakumara, E. Paul Zehr, Taryn Klarner, and Vivian K. Mushahwar. 2025. "Pushing the Limits of Interlimb Connectivity: Neuromodulation and Beyond" Biomedicines 13, no. 5: 1228. https://doi.org/10.3390/biomedicines13051228
APA StylePorter, J. A., Barss, T. S., Mann, D. J., Karamzadeh, Z., Okusanya, D. O., Hemakumara, S. G., Zehr, E. P., Klarner, T., & Mushahwar, V. K. (2025). Pushing the Limits of Interlimb Connectivity: Neuromodulation and Beyond. Biomedicines, 13(5), 1228. https://doi.org/10.3390/biomedicines13051228