

Quantitative Real-Time RT-PCR Verifying Gene Expression Profile of Cavitations Within Human Jaw Bone



Abstract
1. Introduction
2. Materials and Methods
2.1. Collection of the Jawbone Samples
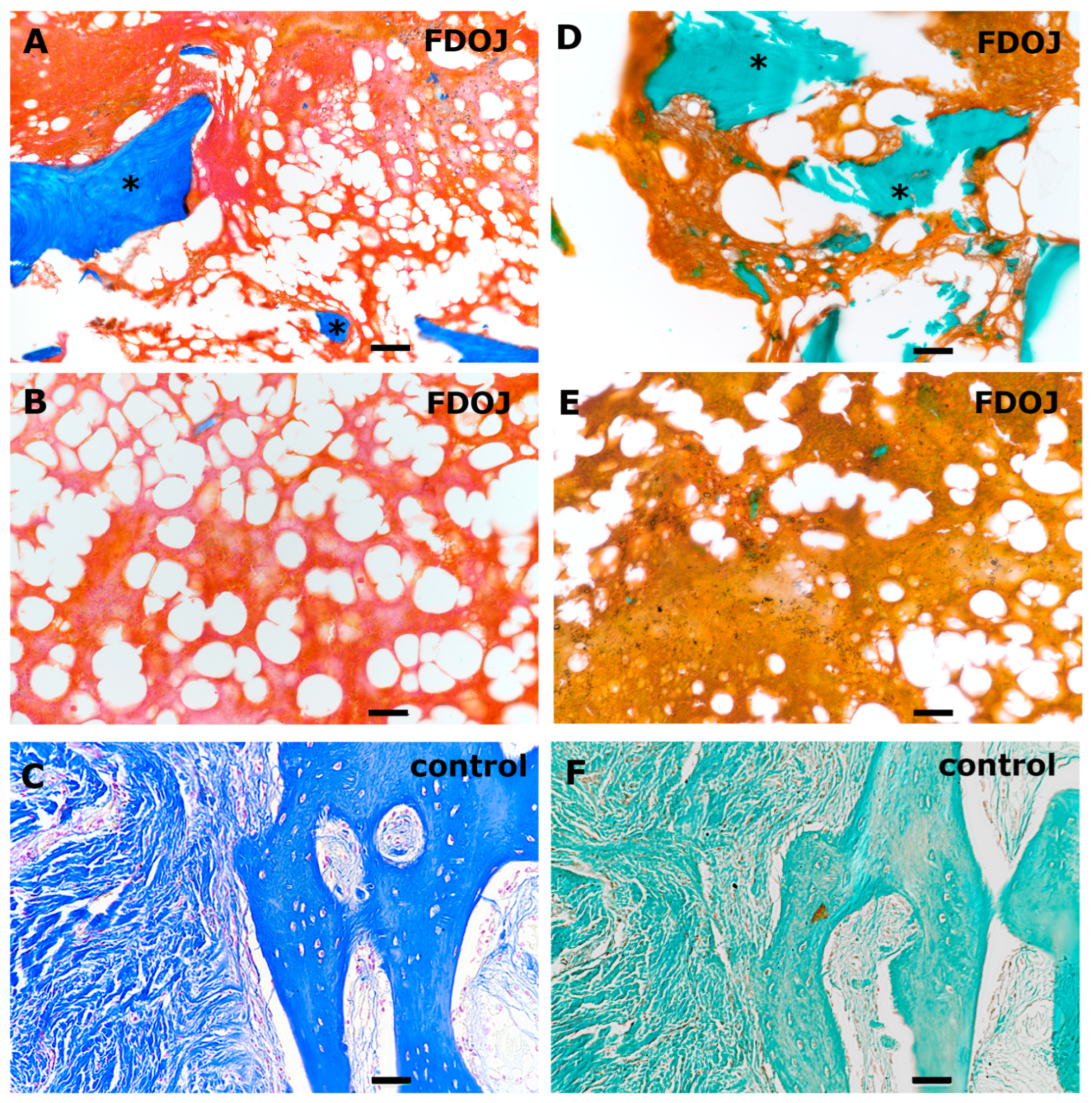
2.2. Histology of FDOJ Tissue Samples
2.3. Isolation of Healthy Human Primary Osteoblasts (pOBs)
2.4. Analysing Gene Expression Profile in BMDJ/FDOJ Tissue Samples
2.4.1. Sample Preparation
2.4.2. Quantitative Real-Time PCR
3. Results
3.1. Histological Evaluation of BMDJ/FDOJ Samples
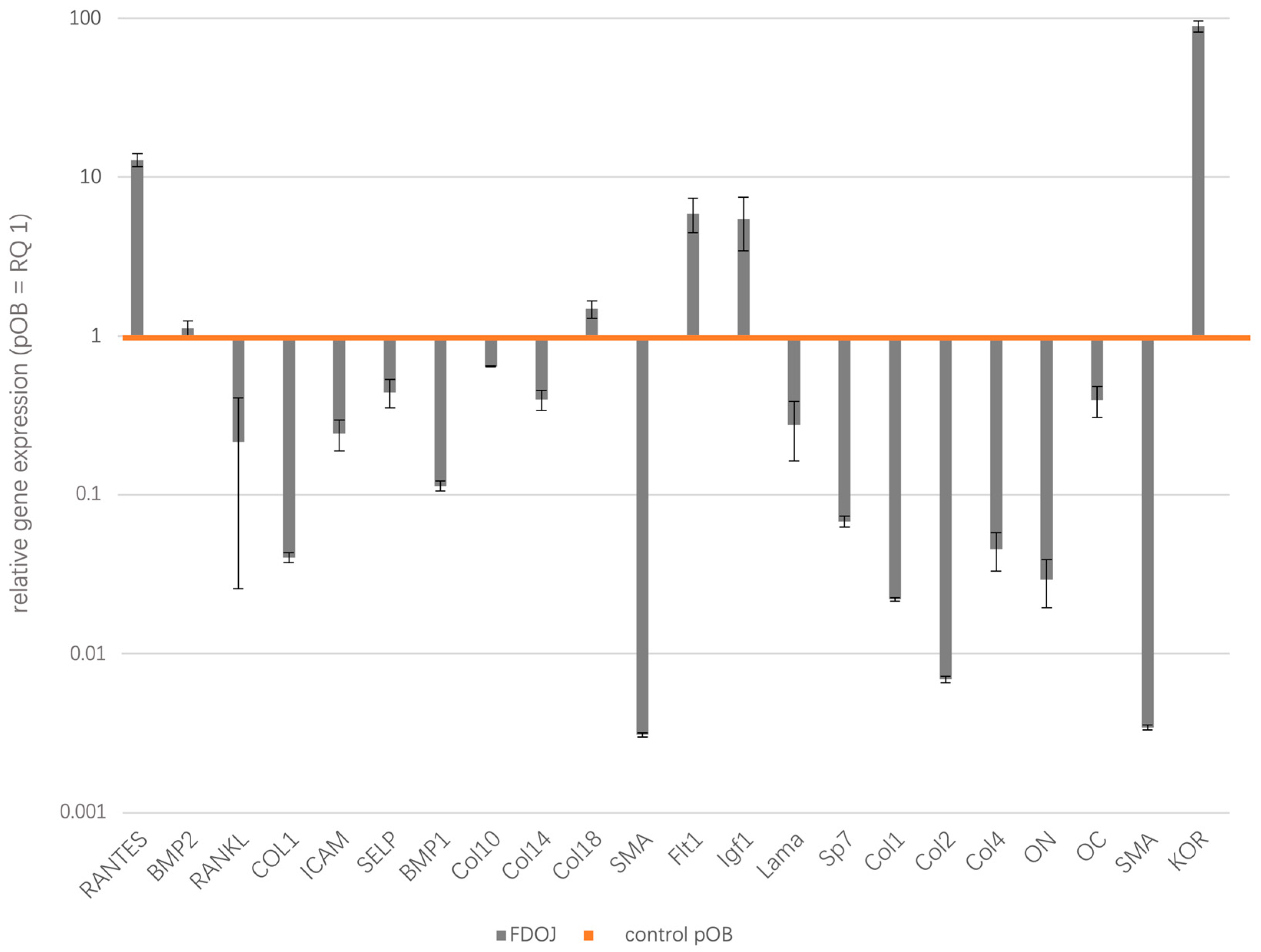
3.2. Relative Gene Expression Profile of BMDJ/FDOJ RNA Versus Healthy pOB RNA
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMDJ | Bone marrow defects of the jaw |
| FDOJ | fatty degenerative osteonecrosis of the jaw |
| pOB | human primary osteoblasts |
| TAU | transalveolar ultrasonography |
| RANTES | Regulated And Normal T cell Expressed and Secreted |
| BMP2 | Bone morphogenic protein 2 |
| RANKL | Receptor Activator of NF-κB Ligand |
| COL1 | Collagen1 |
| ICAM | Intercellular adhesion molecule 1 |
| SELP | P-Selectin |
| BMP1 | Bone morphogenic protein 1 |
| Col10 | Collagen10 |
| Col14 | Collagen14 |
| Col18 | Collagen18 |
| SMA | smooth muscle actin |
| Flt1 | Vascular endothelial growth factor receptor 1 |
| Igf1 | Insulin-like growth factor |
| Lama | Laminin |
| Sp7 | transcription factor Sp7, Osterix |
| Col1 | Collagen 1 |
| Col2 | Collagen 2 |
| Col4 | Collagen 4 |
| ON | Osteonectin |
| OC | Osteonectin |
| KOR | kappa opioid receptor |
References
- Yasuda, H.; Shima, N.; Nakagawa, N.; Yamaguchi, K.; Kinosaki, M.; Goto, M.; Mochizuki, S.I.; Tsuda, E.; Morinaga, T.; Udagawa, N.; et al. A novel molecular mechanism modulating osteoclast differentiation and function. Bone 1999, 25, 109–113. [Google Scholar] [CrossRef]
- Hong, J.; Luo, F.; Du, X.; Xian, F.; Li, X. The immune cells in modulating osteoclast formation and bone metabolism. Int. Immunopharmacol. 2024, 133, 112151. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.C.; Takegahara, N.; Kim, H.; Choi, Y. Updating osteoimmunology: Regulation of bone cells by innate and adaptive immunity. Nat. Rev. Rheumatol. 2018, 14, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Zhu, L. Osteoimmunology: The Crosstalk between T Cells, B Cells, and Osteoclasts in Rheumatoid Arthritis. Int. J. Mol. Sci. 2024, 25, 2688. [Google Scholar] [CrossRef]
- Dominiak, M.; Niemczyk, W.; Pitułaj, A.; Świenc, W.; Matys, J. Fatty Degenerative Osteonecrosis of the Jaw: Bridging Molecular Insights and Clinical Practice—A Scoping Review. Int. J. Mol. Sci. 2025, 26, 1853. [Google Scholar] [CrossRef]
- Lechner, J.; Schuett, S.; von Baehr, V. Aseptic-avascular osteonecrosis: Local “silent inflammation” in the jawbone and RANTES/CCL5 overexpression. Clin. Cosmet. Investig. Dent. 2017, 9, 99–109. [Google Scholar] [CrossRef]
- Lechner, J.; Schmidt, M.; von Baehr, V.; Schick, F. Undetected Jawbone Marrow Defects as Inflammatory and Degenerative Signaling Pathways: Chemokine RANTES/CCL5 as a Possible Link Between the Jawbone and Systemic Interactions? J. Inflamm. Res. 2021, 14, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Ghanaati, S.; Śmieszek-Wilczewska, J.; Al-Maawi, S.; Heselich, A.; Sader, R. After Extraction, Upper Premolars Undergo Programmed Socket Collapse with Development of Cavitations Rather than Complete Socket Healing: A Radiological Study. Bioengineering 2025, 12, 128. [Google Scholar] [CrossRef]
- Huber, R.; Choukroun, E.; Fahrenholz, H.; Notter, F. Dental Ultrasonography for Visualizing Osteoimmune Conditions and Assessing Jaw Bone Density: A Narrative Review. Med. Devices 2025, 18, 1–13. [Google Scholar] [CrossRef]
- Lechner, J.; von Baehr, V. RANTES and fibroblast growth factor 2 in jawbone cavitations: Triggers for systemic disease? Int. J. Gen. Med. 2013, 6, 277–290. [Google Scholar] [CrossRef]
- Molfetta, L.; Florian, A.; Saviola, G.; Frediani, B. Bone Marrow Edema: Pathogenetic features. Clin. Ter. 2022, 173, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Lechner, J.; Mayer, W. Immune messengers in Neuralgia Inducing Cavitational Osteonecrosis (NICO) in jaw bone and systemic interference. Eur. J. Integr. Med. 2010, 2, 71–77. [Google Scholar] [CrossRef]
- Atretkhany, K.N.; Drutskaya, M.S.; Nedospasov, S.A.; Grivennikov, S.I.; Kuprash, D.V. Chemokines, cytokines and exosomes help tumors to shape inflammatory microenvironment. Pharmacol. Ther. 2016, 168, 98–112. [Google Scholar] [CrossRef]
- Huang, Y.; Wu, L.; Sun, Y.; Li, J.; Mao, N.; Yang, Y.; Zhao, M.; Ren, S. CCL5 might be a prognostic biomarker and associated with immuno-therapeutic efficacy in cancers: A pan-cancer analysis. Heliyon 2023, 9, e18215. [Google Scholar] [CrossRef]
- Vasconcelos, E.C.J.; Notter, F.; Schick, F.; Lechner, J. Comparison of Cytokine RANTES/CCL5 Inflammation in Apical Periodontitis and in Jawbone Cavitations—Retrospective Clinical Study. J. Inflamm. Res. 2024, 17, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Lechner, J.; Zimmermann, B.; Schmidt, M. Focal Bone-Marrow Defects in the Jawbone Determined by Ultrasonography-Validation of New Trans-Alveolar Ultrasound Technique for Measuring Jawbone Density in 210 Participants. Ultrasound Med. Biol. 2021, 47, 3135–3146. [Google Scholar] [CrossRef]
- Lechner, J.; Zimmermann, B.; Schmidt, M.; von Baehr, V. Ultrasound Sonography to Detect Focal Osteoporotic Jawbone Marrow Defects Clinical Comparative Study with Corresponding Hounsfield Units and RANTES/CCL5 Expression. Clin. Cosmet. Investig. Dent. 2020, 12, 205–216. [Google Scholar] [CrossRef]
- Sekundo, C.; Wiltfang, J.; Schliephake, H.; Al-Nawas, B.; Rückschloß, T.; Moratin, J.; Hoffmann, J.; Ristow, O. Neuralgia-inducing cavitational osteonecrosis—A systematic review. Oral. Dis. 2022, 28, 1448–1467. [Google Scholar] [CrossRef]
- Zeng, Z.; Lan, T.; Wei, Y.; Wei, X. CCL5/CCR5 axis in human diseases and related treatments. Genes Dis. 2022, 9, 12–27. [Google Scholar] [CrossRef]
- Appay, V.; Rowland-Jones, S.L. RANTES: A versatile and controversial chemokine. Trends Immunol. 2001, 22, 83–87. [Google Scholar] [CrossRef]
- Struyf, S.; Menten, P.; Lenaerts, J.P.; Put, W.; D’Haese, A.; De Clercq, E.; Schols, D.; Proost, P.; Van Damme, J. Diverging binding capacities of natural LD78beta isoforms of macrophage inflammatory protein-1alpha to the CC chemokine receptors 1, 3 and 5 affect their anti-HIV-1 activity and chemotactic potencies for neutrophils and eosinophils. Eur. J. Immunol. 2001, 31, 2170–2178. [Google Scholar] [CrossRef] [PubMed]
- Schall, T.J.; Jongstra, J.; Dyer, B.J.; Jorgensen, J.; Clayberger, C.; Davis, M.M.; Krensky, A.M. A human T cell-specific molecule is a member of a new gene family. J. Immunol. 1988, 141, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Krensky, A.M.; Ahn, Y.T. Mechanisms of disease: Regulation of RANTES (CCL5) in renal disease. Nat. Clin. Pract. Nephrol. 2007, 3, 164–170. [Google Scholar] [CrossRef]
- Lv, D.; Zhang, Y.; Kim, H.J.; Zhang, L.; Ma, X. CCL5 as a potential immunotherapeutic target in triple-negative breast cancer. Cell. Mol. Immunol. 2013, 10, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Lechner, J.; McMahon, R.E.; Bouquot, J.E.; Notter, F.; Schick, F. Is preexisting inflamed jaw marrow a “hidden” co-morbidity affecting outcomes of COVID-19 infections?—Clinical comparative study. Int. J. Immunopathol. Pharmacol. 2024, 38, 3946320241265265. [Google Scholar] [CrossRef]
- Gerber, H.P.; Vu, T.H.; Ryan, A.M.; Kowalski, J.; Werb, Z.; Ferrara, N. VEGF couples hypertrophic cartilage remodeling, ossification and angiogenesis during endochondral bone formation. Nat. Med. 1999, 5, 623–628. [Google Scholar] [CrossRef]
- Shaw, P.; Dwivedi, S.K.D.; Bhattacharya, R.; Mukherjee, P.; Rao, G. VEGF signaling: Role in angiogenesis and beyond. Biochim. Biophys. Acta Rev. Cancer 2024, 1879, 189079. [Google Scholar] [CrossRef]
- Hanahan, D.; Folkman, J. Patterns and emerging mechanisms of the angiogenic switch during tumorigenesis. Cell 1996, 86, 353–364. [Google Scholar] [CrossRef]
- Jain, R.K. Normalizing tumor vasculature with anti-angiogenic therapy: A new paradigm for combination therapy. Nat. Med. 2001, 7, 987–989. [Google Scholar] [CrossRef]
- Yang, J.; Yan, J.; Liu, B. Targeting VEGF/VEGFR to Modulate Antitumor Immunity. Front. Immunol. 2018, 9, 978. [Google Scholar] [CrossRef]
- LeRoith, D.; Holly, J.M.P.; Forbes, B.E. Insulin-like growth factors: Ligands, binding proteins, and receptors. Mol. Metab. 2021, 52, 101245. [Google Scholar] [CrossRef] [PubMed]
- Giustina, A.; Mazziotti, G.; Canalis, E. Growth hormone, insulin-like growth factors, and the skeleton. Endocr. Rev. 2008, 29, 535–559. [Google Scholar] [CrossRef]
- Behera, J.; Ison, J.; Tyagi, A.; Mbalaviele, G.; Tyagi, N. Mechanisms of autophagy and mitophagy in skeletal development, diseases and therapeutics. Life Sci. 2022, 301, 120595. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.L.; Sweeney, C.; Wolff, R.; Herrick, J.; Baumgartner, K.; Giuliano, A.; Byers, T. Genetic variation in IGF1, IGFBP3, IRS1, IRS2 and risk of breast cancer in women living in Southwestern United States. Breast Cancer Res. Treat. 2007, 104, 197–209. [Google Scholar] [CrossRef]
- Liu, G.; Zhu, M.; Zhang, M.; Pan, F. Emerging Role of IGF-1 in Prostate Cancer: A Promising Biomarker and Therapeutic Target. Cancers 2023, 15, 1287. [Google Scholar] [CrossRef] [PubMed]
- Denduluri, S.K.; Idowu, O.; Wang, Z.; Liao, Z.; Yan, Z.; Mohammed, M.K.; Ye, J.; Wei, Q.; Wang, J.; Zhao, L.; et al. Insulin-like growth factor (IGF) signaling in tumorigenesis and the development of cancer drug resistance. Genes Dis. 2015, 2, 13–25. [Google Scholar] [CrossRef]
- Hartmann, W.; Koch, A.; Brune, H.; Waha, A.; Schüller, U.; Dani, I.; Denkhaus, D.; Langmann, W.; Bode, U.; Wiestler, O.D.; et al. Insulin-like growth factor II is involved in the proliferation control of medulloblastoma and its cerebellar precursor cells. Am. J. Pathol. 2005, 166, 1153–1162. [Google Scholar] [CrossRef]
- Kalla Singh, S.; Tan, Q.W.; Brito, C.; De León, M.; Garberoglio, C.; De León, D. Differential insulin-like growth factor II (IGF-II) expression: A potential role for breast cancer survival disparity. Growth Horm. IGF Res. 2010, 20, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ma, L.; Sun, F.; Tang, Z.; Chan, P. A Multicenter Study of Multimorbidity in Older Adult Inpatients in China. J. Nutr. Health Aging 2020, 24, 269–276. [Google Scholar] [CrossRef]
- Iqbal, M.J.; Kabeer, A.; Abbas, Z.; Siddiqui, H.A.; Calina, D.; Sharifi-Rad, J.; Cho, W.C. Interplay of oxidative stress, cellular communication and signaling pathways in cancer. Cell Commun. Signal. 2024, 22, 7. [Google Scholar] [CrossRef]
- Mansour, A.; Fox, C.A.; Akil, H.; Watson, S.J. Opioid-receptor mRNA expression in the rat CNS: Anatomical and functional implications. Trends Neurosci. 1995, 18, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Bouquot, J.E.; Roberts, A.M.; Person, P.; Christian, J. Neuralgia-inducing cavitational osteonecrosis (NICO). Osteomyelitis in 224 jawbone samples from patients with facial neuralgia. Oral Surg. Oral Med. Oral Pathol. 1992, 73, 307–319; discussion 319–320. [Google Scholar] [CrossRef] [PubMed]
- Lechner, J.; von Baehr, V. Peripheral Neuropathic Facial/Trigeminal Pain and RANTES/CCL5 in Jawbone Cavitation. Evid. Based Complement. Altern. Med. 2015, 2015, 582520. [Google Scholar] [CrossRef] [PubMed]
- Kuzmin, A.V.; Semenova, S.; Gerrits, M.A.; Zvartau, E.E.; Van Ree, J.M. Kappa-opioid receptor agonist U50,488H modulates cocaine and morphine self-administration in drug-naive rats and mice. Eur. J. Pharmacol. 1997, 321, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Aeschlimann, A.; Reisch, N.; Gay, R.E.; Simmen, B.R.; Michel, B.A.; Gay, S.; Sprott, H. Kappa and delta opioid receptors are expressed but down-regulated in fibroblast-like synoviocytes of patients with rheumatoid arthritis and osteoarthritis. Arthritis Rheum. 2005, 52, 1402–1410. [Google Scholar] [CrossRef]
- Hanada, R.; Hanada, T.; Sigl, V.; Schramek, D.; Penninger, J.M. RANKL/RANK-beyond bones. J. Mol. Med. 2011, 89, 647–656. [Google Scholar] [CrossRef]
- Xiong, J.; Piemontese, M.; Onal, M.; Campbell, J.; Goellner, J.J.; Dusevich, V.; Bonewald, L.; Manolagas, S.C.; O’Brien, C.A. Osteocytes, not Osteoblasts or Lining Cells, are the Main Source of the RANKL Required for Osteoclast Formation in Remodeling Bone. PLoS ONE 2015, 10, e0138189. [Google Scholar] [CrossRef]
- Huber, F.; Schnauß, J.; Rönicke, S.; Rauch, P.; Müller, K.; Fütterer, C.; Käs, J. Emergent complexity of the cytoskeleton: From single filaments to tissue. Adv. Phys. 2013, 62, 1–112. [Google Scholar] [CrossRef]
- Grummt, I. Actin and myosin as transcription factors. Curr. Opin. Genet. Dev. 2006, 16, 191–196. [Google Scholar] [CrossRef]
- Chen, D.; Zhao, M.; Mundy, G.R. Bone morphogenetic proteins. Growth Factors 2004, 22, 233–241. [Google Scholar] [CrossRef]
- Sinha, K.M.; Zhou, X. Genetic and molecular control of osterix in skeletal formation. J. Cell. Biochem. 2013, 114, 975–984. [Google Scholar] [CrossRef] [PubMed]
- Tu, Q.; Valverde, P.; Chen, J. Osterix enhances proliferation and osteogenic potential of bone marrow stromal cells. Biochem. Biophys. Res. Commun. 2006, 341, 1257–1265. [Google Scholar] [CrossRef]
- Lim, J.; Grafe, I.; Alexander, S.; Lee, B. Genetic causes and mechanisms of Osteogenesis Imperfecta. Bone 2017, 102, 40–49. [Google Scholar] [CrossRef]
- Xu, B.; Zhang, J.; Brewer, E.; Tu, Q.; Yu, L.; Tang, J.; Krebsbach, P.; Wieland, M.; Chen, J. Osterix enhances BMSC-associated osseointegration of implants. J. Dent. Res. 2009, 88, 1003–1007. [Google Scholar] [CrossRef]
- Lechner, J.; von Baehr, V.; Notter, F.; Schick, F. Osseointegration and osteoimmunology in implantology: Assessment of the immune sustainability of dental implants using advanced sonographic diagnostics: Research and case reports. J. Int. Med. Res. 2024, 52, 3000605231224161. [Google Scholar] [CrossRef]
- Park, K.S.; Park, M.J.; Cho, M.L.; Kwok, S.K.; Ju, J.H.; Ko, H.J.; Park, S.H.; Kim, H.Y. Type II collagen oral tolerance; mechanism and role in collagen-induced arthritis and rheumatoid arthritis. Mod. Rheumatol. 2009, 19, 581–589. [Google Scholar] [CrossRef]
- Bowcock, A.M.; Hebert, J.M.; Christiano, A.M.; Wijsman, E.; Cavalli-Sforza, L.L.; Boyd, C.D. The pro alpha 1 (IV) collagen gene is linked to the D13S3 locus at the distal end of human chromosome 13q. Cytogenet. Cell Genet. 1987, 45, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Soininen, R.; Huotari, M.; Hostikka, S.L.; Prockop, D.J.; Tryggvason, K. The structural genes for alpha 1 and alpha 2 chains of human type IV collagen are divergently encoded on opposite DNA strands and have an overlapping promoter region. J. Biol. Chem. 1988, 263, 17217–17220. [Google Scholar] [CrossRef] [PubMed]
- Villarreal, X.C.; Mann, K.G.; Long, G.L. Structure of human osteonectin based upon analysis of cDNA and genomic sequences. Biochemistry 1989, 28, 6483–6491. [Google Scholar] [CrossRef]
- Young, M.F.; Kerr, J.M.; Ibaraki, K.; Heegaard, A.M.; Robey, P.G. Structure, expression, and regulation of the major noncollagenous matrix proteins of bone. Clin. Orthop. Relat. Res. 1992, 281, 275–294. [Google Scholar] [CrossRef]
- Guweidhi, A.; Kleeff, J.; Adwan, H.; Giese, N.A.; Wente, M.N.; Giese, T.; Büchler, M.W.; Berger, M.R.; Friess, H. Osteonectin influences growth and invasion of pancreatic cancer cells. Ann. Surg. 2005, 242, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Bouquot, J.E.; McMahon, R.E.; Glueck, C.J. Bone marrow edema: Mild or nascent variant of ischemic bone disease. J. Oral Maxillofac. Surg. 2008, 66, 205–208. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Gene | FDOJ | Control | Gene | FDOJ | Control |
|---|---|---|---|---|---|
| RANTES | 12.79 ± 1.2 | 1 | Flt1 | 5.89 ± 1.44 | 1 |
| BMP2 | 1.11 ± 0.13 | 1 | Igf1 | 5.43 ± 2.01 | 1 |
| RANKL | 0.21 ± 0.19 | 1 | Lama | 0.27 ± 0.112 | 1 |
| COL1 | 0.04 ± 0.003 | 1 | Sp7 | 0.06 ± 0.0054 | 1 |
| ICAM | 0.24 ± 0.054 | 1 | Col1 | 0.02 ± 0.0006 | 1 |
| SELP | 0.44 ± 0.09 | 1 | Col2 | 0.00 ± 0.00032 | 1 |
| BMP1 | 0.11 ± 0.008 | 1 | Col4 | 0.04 ± 0.0125 | 1 |
| Col10 | 0.64 ± 0.004 | 1 | ON | 0.02 ± 0.0098 | 1 |
| Col14 | 0.39 ± 0.057 | 1 | OC | 0.39 ± 0.087 | 1 |
| Col18 | 1.47 ± 0.187 | 1 | SMA | 0.00 ± 0.00012 | 1 |
| SMA | 0.00 ± 0.00009 | 1 | KOR | 89.01 ± 7.12 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghanaati, S.; Dohle, E.; Schick, F.; Lechner, J. Quantitative Real-Time RT-PCR Verifying Gene Expression Profile of Cavitations Within Human Jaw Bone. Biomedicines 2025, 13, 1144. https://doi.org/10.3390/biomedicines13051144
Ghanaati S, Dohle E, Schick F, Lechner J. Quantitative Real-Time RT-PCR Verifying Gene Expression Profile of Cavitations Within Human Jaw Bone. Biomedicines. 2025; 13(5):1144. https://doi.org/10.3390/biomedicines13051144
Chicago/Turabian StyleGhanaati, Shahram, Eva Dohle, Fabian Schick, and Johann Lechner. 2025. "Quantitative Real-Time RT-PCR Verifying Gene Expression Profile of Cavitations Within Human Jaw Bone" Biomedicines 13, no. 5: 1144. https://doi.org/10.3390/biomedicines13051144
APA StyleGhanaati, S., Dohle, E., Schick, F., & Lechner, J. (2025). Quantitative Real-Time RT-PCR Verifying Gene Expression Profile of Cavitations Within Human Jaw Bone. Biomedicines, 13(5), 1144. https://doi.org/10.3390/biomedicines13051144