
Optimizing Wound Healing in Radial Forearm Donor Sites: A Comparative Study of Ulnar-Based Flap and Split-Thickness Skin Grafting


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
- Patients aged ≥ 18 years.
- Histologically confirmed diagnosis of head and neck cancer requiring RFFF reconstruction.
- No contraindications for microsurgical reconstruction.
- Severe systemic comorbidities contraindicating free flap surgery, including uncontrolled DM or severe peripheral vascular disease.
- Prior surgery or radiotherapy to the forearm affecting flap harvest feasibility.
- Incomplete medical records or lack of postoperative follow-up.
2.2. Biochemical Analysis
2.3. Flap Morbidity Assessment
2.4. Aesthetic Flap Evaluation
2.5. Surgical Technique
2.6. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Biochemical Results Evaluation
3.3. Aesthetic Flap Assessment
3.4. Post-Surgical Complications Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BCC | Basal cell carcinoma |
| CRP | C-reactive protein |
| DM2 | Diabetes mellitus type 2 |
| FGF | Fibroblast growth factor |
| FTSG | Full-thickness skin graft |
| HB | Hemoglobin |
| PDGF | Platelet-derived growth factor |
| PLT | Platelets |
| RFFF | Radial free forearm flap |
| SCC | Squamous cell carcinoma |
| STGS | Split-thickness skin graft |
| UBTF | Ulnar-based transposition flap |
| VEGF | Vascular endothelial growth factor |
| WBC | White blood cells |
References
- Markiewicz-Gospodarek, A.; Kozioł, M.; Tobiasz, M.; Baj, J.; Radzikowska-Büchner, E.; Przekora, A. Burn Wound Healing: Clinical Complications, Medical Care, Treatment, and Dressing Types: The Current State of Knowledge for Clinical Practice. Int. J. Environ. Res. Public Health 2022, 19, 1338. [Google Scholar] [CrossRef]
- Tottoli, E.M.; Dorati, R.; Genta, I.; Chiesa, E.; Pisani, S.; Conti, B. Skin Wound Healing Process and New Emerging Technologies for Skin Wound Care and Regeneration. Pharmaceutics 2020, 12, 735. [Google Scholar] [CrossRef] [PubMed]
- Pang, C.; Ibrahim, A.; Bulstrode, N.W.; Ferretti, P. An overview of the therapeutic potential of regenerative medicine in cutaneous wound healing. Int. Wound J. 2017, 14, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Dutra Alves, N.S.; Reigado, G.R.; Santos, M.; Caldeira, I.D.S.; Hernandes, H.D.S.; Freitas-Marchi, B.L.; Zhivov, E.; Chambergo, F.S.; Nunes, V.A. Advances in regenerative medicine-based approaches for skin regeneration and rejuvenation. Front. Bioeng. Biotechnol. 2025, 13, 1527854. [Google Scholar] [CrossRef]
- Kumar, R.; Kumar, V.; Mohan, A.; Gupta, G.; Kashyap, V. Translational research in the generation of therapeutic medicine for wound healing: A review. Discov. Med. 2024, 1, 158. [Google Scholar] [CrossRef]
- Dean, J.; Hoch, C.; Wollenberg, B.; Navidzadeh, J.; Maheta, B.; Mandava, A.; Knoedler, S.; Sherwani, K.; Baecher, H.; Schmitz, A.; et al. Advancements in bioengineered and autologous skin grafting techniques for skin reconstruction: A comprehensive review. Front. Bioeng. Biotechnol. 2025, 12, 1461328. [Google Scholar] [CrossRef]
- Šuca, H.; Čoma, M.; Tomšů, J.; Sabová, J.; Zajíček, R.; Brož, A.; Doubková, M.; Novotný, T.; Bačáková, L.; Jenčová, V.; et al. Current Approaches to Wound Repair in Burns: How far Have we Come from Cover to Close? A Narrative Review. J. Surg. Res. 2024, 296, 383–403. [Google Scholar] [CrossRef]
- Kaur, A.; Midha, S.; Giri, S.; Mohanty, S. Functional Skin Grafts: Where Biomaterials Meet Stem Cells. Stem Cells Int. 2019, 2019, 1286054. [Google Scholar] [CrossRef]
- Motamedi, S.; Esfandpour, A.; Babajani, A.; Jamshidi, E.; Bahrami, S.; Niknejad, H. The Current Challenges on Spray-Based Cell Delivery to the Skin Wounds. Tissue Eng. Part C Methods 2021, 27, 543–558. [Google Scholar] [CrossRef]
- Gerlach, J.C.; Johnen, C.; Ottomann, C.; Bräutigam, K.; Plettig, J.; Belfekroun, C.; Münch, S.; Hartmann, B. Method for autologous single skin cell isolation for regenerative cell spray transplantation with non-cultured cells. Int. J. Artif. Organs 2011, 34, 271–279. [Google Scholar] [CrossRef]
- Carvalho, L.N.; Peres, L.C.; Alonso-Goulart, V.; Santos, B.J.; Braga, M.F.; Campos, F.D.; Palis, G.D.; Quirino, L.S.; Guimarães, L.D.; Lafetá, S.A.; et al. Recent advances in the 3D skin bioprinting for regenerative medicine: Cells, biomaterials, and methods. J. Biomater. Appl. 2024, 39, 421–438. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Park, S.A.; Kim, W.D.; Ha, T.; Xin, Y.-Z.; Lee, J.; Lee, D. Current Advances in 3D Bioprinting Technology and Its Applications for Tissue Engineering. Polymers 2020, 12, 2958. [Google Scholar] [CrossRef]
- Weng, T.; Zhang, W.; Xia, Y.; Wu, P.; Yang, M.; Jin, R.; Xia, S.; Wang, J.; You, C.; Han, C.; et al. 3D bioprinting for skin tissue engineering: Current status and perspectives. J. Tissue Eng. 2021, 12, 20417314211028574. [Google Scholar] [CrossRef]
- Kianian, S.; Zhao, K.; Kaur, J.; Lu, K.W.; Rathi, S.; Ghosh, K.; Rogoff, H.; Hays, T.R.; Park, J.; Rafailovich, M.; et al. Autologous Skin Grafts, versus Tissue-engineered Skin Constructs: A Systematic Review and Meta-analysis. Plast. Reconstr. Surg. Glob. Open 2023, 11, e5100. [Google Scholar] [CrossRef] [PubMed]
- Kozak, G.M.; Hsu, J.Y.; Broach, R.B.; Shakir, S.; Calvert, C.; Stranix, J.T.; Messa C4th Levin, L.S.; Serletti, J.M.; Kovach, S.J.; Fischer, J.P. Comparative Effectiveness Analysis of Complex Lower Extremity Reconstruction: Outcomes and Costs for Biologically Based, Local Tissue Rearrangement, and Free Flap Reconstruction. Plast Reconstr. Surg. 2020, 145, 608e–616e. [Google Scholar] [CrossRef]
- Kolimi, P.; Narala, S.; Nyavanandi, D.; Youssef, A.A.A.; Dudhipala, N. Innovative Treatment Strategies to Accelerate Wound Healing: Trajectory and Recent Advancements. Cells 2022, 11, 2439. [Google Scholar] [CrossRef]
- Norman, G.; Wong, J.K.; Amin, K.; Dumville, J.C.; Pramod, S. Reconstructive surgery for treating pressure ulcers. Cochrane Database Syst. Rev. 2022, 10, CD012032. [Google Scholar] [PubMed]
- Vindigni, V.; Marena, F.; Zanettin, C.; Bassetto, F. Breast Reconstruction: The Oncoplastic Approach. J. Clin. Med. 2024, 13, 4718. [Google Scholar] [CrossRef]
- Thariat, J.; Carsuzaa, F.; Beddok, A.; Deneuve, S.; Marcy, P.Y.; Merlotti, A.; Dejean, C.; Devauchelle, B. Reconstructive flap surgery in head and neck cancer patients: An interdisciplinary view of the challenges encountered by radiation oncologists in postoperative radiotherapy. Front. Oncol. 2024, 14, 1379861. [Google Scholar] [CrossRef]
- Ibrahim, B.; Rahal, A.; Bissada, E.; Christopoulos, A.; Guertin, L.; Ayad, T. Reconstruction of medium-size defects of the oral cavity: Radial forearm free flap vs facial artery musculo-mucosal flap. J. Otolaryngol. Head Neck Surg. 2021, 50, 67. [Google Scholar] [CrossRef]
- Gałązka, A.; Bieńkowska-Pluta, K.; Kalecińska, Z.; Krupa, Z.; Woźniczko, K. Thumb-up modification of the radial forearm free flap in oral cavity reconstruction: A description of a surgical technique. Pol. Otorhino Rev. 2024, 13, 36–39. [Google Scholar] [CrossRef]
- Wood, J.W.; Broussard, K.C.; Burkey, B. Preoperative Testing for Radial Forearm Free Flaps to Reduce Donor Site Morbidity. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Lee, K.T. Coverage of radial forearm free flap donor site defect using another free flap. Microsurgery 2023, 43, 775–781. [Google Scholar] [CrossRef]
- Wirthmann, A.; Finke, J.C.; Giovanoli, P.; Lindenblatt, N. Long-term follow-up of donor site morbidity after defect coverage with Integra following radial forearm flap elevation. Eur. J. Plast Surg. 2014, 37, 159–166. [Google Scholar] [CrossRef]
- Shah, R.; Rodrigues, R.; Phillips, V.; Khatib, M. The use of artificial dermal substitutes for repair of the donor site following harvesting of a radial forearm free flap: A systematic review. J. Plast Reconstr. Aesthet. Surg. 2024, 88, 501–516. [Google Scholar] [CrossRef]
- Giordano, L.; Bondi, S.; Ferrario, F.; Fabiano, B.; Bussi, M. Radial forearm free flap surgery: A modified skin-closure technique improving donor-site aesthetic appearance. Acta Otorhinolaryngol. Ital. 2012, 32, 158–163. [Google Scholar] [PubMed]
- Ho, T.; Couch, M.; Carson, K.; Schimberg, A.; Manley, K.; Byrne, P.J. Radial forearm free flap donor site outcomes comparison by closure methods. Otolaryngol. Head Neck Surg. 2006, 134, 309–315. [Google Scholar] [CrossRef]
- Hong, S. Risk Factors for Postoperative Donor Site Complications in Radial Forearm Free Flaps. Medicina 2024, 60, 1487. [Google Scholar] [CrossRef]
- Zhang, C.; Pandya, S.; Alessandri Bonetti, M.; Costantino, A.; Egro, F.M. Comparison of split thickness skin graft versus full thickness skin graft for radial forearm flap donor site closure: A systematic review and Meta-analysis. Am. J. Otolaryngol. 2024, 45, 104156. [Google Scholar] [CrossRef]
- Al-Aroomi, M.A.; Mashrah, M.A.; Al-Worafi, N.A.; Zhou, W.; Sun, C.; Pan, C. Biomechanical and aesthetic outcomes following radial forearm free flap transfer: Comparison of ipsilateral full-thickness skin graft and traditional split-thickness skin graft. Int. J. Oral Maxillofac. Surg. 2024, 53, 109–116. [Google Scholar] [CrossRef]
- Mashrah, M.A.; Lingjian, Y.; Handley, T.P.; Pan, C.; Weiliang, C. Novel technique for the direct closure of the radial forearm flap donor site defect with a local bilobed flap. Head Neck 2019, 41, 3282–3289. [Google Scholar] [CrossRef] [PubMed]
- Jaquet, Y.; Enepekides, D.J.; Torgerson, C.; Higgins, K.M. Radial forearm free flap donor site morbidity: Ulnar-based transposition flap vs split-thickness skin graft. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 38–43. [Google Scholar] [CrossRef]
- Marchesi, A.; Gatto, A.; Cavalli, E.M.; Del Bene, M. Free-style propeller ulnar artery perforator flaps for radial forearm flap donor site repair. Microsurgery 2024, 44, e31074. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, G.K.; Martinez-Rodriguez, S.; Md Fadilah, N.I.; Looi Qi Hao, D.; Markey, G.; Shukla, P.; Fauzi, M.B.; Panetsos, F. Progress in Wound-Healing Products Based on Natural Compounds, Stem Cells, and MicroRNA-Based Biopolymers in the European, USA, and Asian Markets: Opportunities, Barriers, and Regulatory Issues. Polymers 2024, 16, 1280. [Google Scholar] [CrossRef] [PubMed]
- Olteanu, G.; Neacșu, S.M.; Joița, F.A.; Musuc, A.M.; Lupu, E.C.; Ioniță-Mîndrican, C.-B.; Lupuliasa, D.; Mititelu, M. Advancements in Regenerative Hydrogels in Skin Wound Treatment: A Comprehensive Review. Int. J. Mol. Sci. 2024, 25, 3849. [Google Scholar] [CrossRef]
- Velikic, G.; Maric, D.M.; Maric, D.L.; Supic, G.; Puletic, M.; Dulic, O.; Vojvodic, D. Harnessing the Stem Cell Niche in Regenerative Medicine: Innovative Avenue to Combat Neurodegenerative Diseases. Int. J. Mol. Sci. 2024, 25, 993. [Google Scholar] [CrossRef]
- Hussen, B.M.; Taheri, M.; Yashooa, R.K.; Abdullah, G.H.; Abdullah, S.R.; Kheder, R.K.; Mustafa, S.A. Revolutionizing medicine: Recent developments and future prospects in stem-cell therapy. Int. J. Surg. 2024, 110, 8002–8024. [Google Scholar] [CrossRef]
- Urciuolo, F.; Casale, C.; Imparato, G.; Netti, P.A. Bioengineered Skin Substitutes: The Role of Extracellular Matrix and Vascularization in the Healing of Deep Wounds. J. Clin. Med. 2019, 8, 2083. [Google Scholar] [CrossRef]
- Vecin, N.M.; Kirsner, R.S. Skin substitutes as treatment for chronic wounds: Current and future directions. Front. Med. 2023, 10, 1154567. [Google Scholar] [CrossRef]
- Zhang, M.; Xing, J.; Zhong, Y.; Zhang, T.; Liu, X.; Xing, D. Advanced function, design and application of skin substitutes for skin regeneration. Mater. Today Bio 2023, 24, 100918. [Google Scholar] [CrossRef]
- Saleki, M.; Noor, M.A.; Hurt, P.; Abul, A. Full-Thickness Skin Graft Versus Split-Thickness Skin Graft for Radial Forearm Free Flap Transfer in Oral Cavity Reconstruction: A Systematic Review and Meta-Analysis. Cureus 2023, 15, e49279. [Google Scholar] [CrossRef] [PubMed]
- Niederstätter, I.M.; Schiefer, J.L.; Fuchs, P.C. Surgical Strategies to Promote Cutaneous Healing. Med. Sci. 2021, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Mulvey, C.L.; Brant, J.A.; Bur, A.M.; Chen, J.; Fischer, J.P.; Cannady, S.B.; Newman, J.G. Complications Associated with Mortality after Head and Neck Surgery. Otolaryngol. Head Neck Surg. 2017, 156, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Zuidam, J.M.; Coert, J.H.; Hofer, S.O. Closure of the donor site of the free radial forearm flap: A comparison of full-thickness graft and split-thickness skin graft. Ann. Plast Surg. 2005, 55, 612–616. [Google Scholar] [CrossRef]
- Manek, Y.B.; Jajoo, S.; Mahakalkar, C. A Comprehensive Review of Evaluating Donor Site Morbidity and Scar Outcomes in Skin Transfer Techniques. Cureus 2024, 16, e53433. [Google Scholar] [CrossRef]
- Benanti, E.; De Santis, G.; Leti Acciaro, A.; Colzani, G.; Baccarani, A.; Starnoni, M. Soft tissue coverage of the upper limb: A flap reconstruction overview. Ann. Med. Surg. 2020, 60, 338–343. [Google Scholar] [CrossRef]
- Patel, R. Reducing morbidity in radial forearm free flap donor site: A review of closure techniques. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 363–367. [Google Scholar] [CrossRef]
- Converse, J.M.; Uhlschmid, G.K.; Ballantyne, D.L. “Plasmatic circulation” in skin grafts. The phase of serum imbibition. Plast Reconstr. Surg. 1969, 43, 495–499. [Google Scholar] [CrossRef]
- Converse, J.M.; Smahel, J.; Ballantyne, D.L.; Harper, A.D. Inosculation of vessels of skin graft and host bed: A fortuitous encounter. Br. J. Plast Surg. 1975, 28, 274–282. [Google Scholar] [CrossRef]
- Williams, Z.J.; Pezzanite, L.M.; Hendrickson, D.A. Review of skin grafting in equine wounds: Indications and techniques. Equine Vet. Educ. 2024, 36, 484–493. [Google Scholar] [CrossRef]
- Kanapathy, M.; Hachach-Haram, N.; Bystrzonowski, N.; Connelly, J.T.; O’Toole, E.A.; Becker, D.L.; Mosahebi, A.; Richards, T. Epidermal grafting for wound healing: A review on the harvesting systems, the ultrastructure of the graft and the mechanism of wound healing. Int. Wound J. 2017, 14, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Loeffelbein, D.J.; Al-Benna, S.; Steinsträßer, L.; Satanovskij, R.M.; Rohleder, N.H.; Mücke, T.; Wolff, K.D.; Kesting, M.R. Reduction of donor site morbidity of free radial forearm flaps: What level of evidence is available? Eplasty 2012, 12, e9. [Google Scholar] [PubMed]
- Locatelli, L.; Colciago, A.; Castiglioni, S.; Maier, J.A. Platelets in Wound Healing: What Happens in Space? Front. Bioeng. Biotechnol. 2021, 9, 716184. [Google Scholar] [CrossRef]
- Lacci, K.M.; Dardik, A. Platelet-rich plasma: Support for its use in wound healing. Yale J. Biol. Med. 2010, 83, 1–9. [Google Scholar] [PubMed]
- Margolis, D.J.; Kantor, K.; Santanna, J.; Strom, B.L.; Berlin, J.A. Effectiveness of platelet releasate for the treatment of diabetic neuropathic foot ulcers. Diabetes Care 2001, 24, 483–488. [Google Scholar] [CrossRef]
- Aleman Paredes, K.; Selaya Rojas, J.C.; Flores Valdés, J.R.; Castillo, J.L.; Montelongo Quevedo, M.; Mijangos Delgado, F.J.; de la Cruz Durán, H.A.; Nolasco Mendoza, C.L.; Nuñez Vazquez, E.J. A Comparative Analysis of the Outcomes of Various Graft Types in Burn Reconstruction Over the Past 24 Years: A Systematic Review. Cureus 2024, 16, e54277. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | UBTF (n = 10) | STGS (n = 14) | p-Value |
|---|---|---|---|
| Gender | 0.338 a | ||
| Male | 6 (60%) | 12 (85.7%) | |
| Female | 4 (40%) | 2 (14.3%) | |
| Age (mean ± SD) | 57.8 ± 14.1 | 63.2 ± 13.8 | 4.521 b |
| Primary tumor location | 0.238 a | ||
| Tongue | 5 (50%) | 4 (28.6%) | |
| Cheek mucosa | 2 (20%) | 2 (14.3%) | |
| Floor of the mouth | 0 | 3 (21.4%) | |
| Gum | 1 (10%) | 2 (14.3%) | |
| Upper lip | 2 (20%) | 0 | |
| Lower lip | 0 | 2 (14.3%) | |
| Cheek skin | 0 | 1 (7.15%) | |
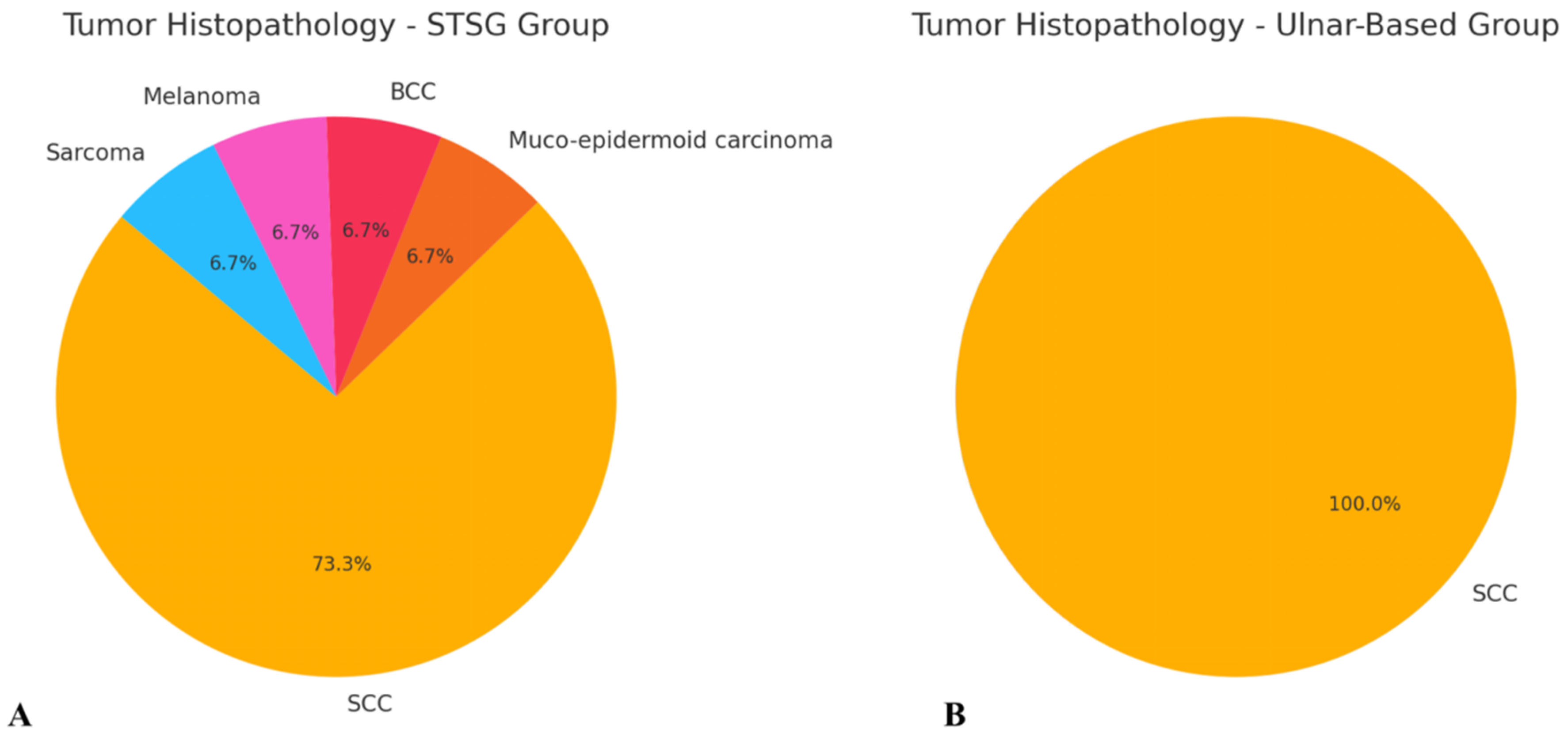
| Histopathological Type | 0.416 a | ||
| SCC | 9 (90%) | 12 (85.8%) | |
| BCC | 0 | 1 (7.1%) | |
| Sarcoma | 1 (10%) | 0 | |
| Melanoma | 0 | 1 (7.1%) | |
| Smoking history | 5 (50%) | 11 (78.6%) | 0.305 a |
| DM2 | 1 (10%) | 3 (21.4%) | 0.853 a |
| Atherosclerosis | 5 (50%) | 8 (57.1%) | 1.0 a |
| RFFF size (cm2) | 41.4 ± 3.503 (mean ± SD) | 41.3 ± 2.225 (mean ± SD) | 0.933 |
| Parameter | STSG Pre-Mean ± SD | STSG Post-Mean ± SD | UBTF Pre-Mean ± SD | UBTF Post-Mean ± SD | p-Value (Pre-Op) | p-Value (Post-Op) |
|---|---|---|---|---|---|---|
| HB (g/dL) | 13.6 ± 1.89 | 10.4 ± 1.41 | 14.5 ± 1.04 | 11.0 ± 1.42 | 0.140 | 0.296 |
| WBC (×10⁹/L) | 7.05 ± 2.32 | 11.6 ± 4.53 | 8.05 ± 3.77 | 11.9 ± 4.24 | 0.468 | 0.838 |
| PLT (×10⁹/L) | 190.2 ± 54.56 | 175.6 ± 55.78 | 280.0 ± 62.51 | 217.9 ± 38.60 | 0.001 | 0.0438 |
| Albumin (mg/dL) | 42.9 ± 2.87 | 37.1 ± 7.13 | 41.5 ± 2.18 | 34.3 ± 4.59 | 0.205 | 0.258 |
| Variable | UBTF (Mean ± SD) | STGS (Mean ± SD) | p-Value a |
|---|---|---|---|
| Skin color | 3.00 ± 0.00 | 1.40 ± 0.507 | p = 0.000021 |
| Skin texture | 3.00 ± 0.00 | 1.67 ± 0.487 | p = 0.000018 |
| Flap stability | 2.56 ± 0.527 | 1.93 ± 0.703 | p = 0.0398 |
| Complication | UBTF Group (n = 10) | STSG Group (n = 14) | p-Value a |
|---|---|---|---|
| Edema | 5 (50%) | 10 (71.4%) | 0.521 |
| Hematoma | 1 (10%) | 0 | 0.862 |
| Infection | 3 (30%) | 6 (42.8%) | 0.830 |
| Wound dehiscence | 2 (20%) | 6 (42.8%) | 0.464 |
| Healing time (days) | 15.7 ± 3.354 (mean ± SD) | 21.6 ± 2.261 (mean ± SD) | 0.0004 |
| Comorbidity | Complication | p-Value a |
|---|---|---|
| DM2 | Edema | 1 |
| Hematoma | 1 | |
| Infection | 1 | |
| Wound dehiscence | 0.654 | |
| Smoking | Edema | 1 |
| Hematoma | 1 | |
| Infection | 0.654 | |
| Wound dehiscence | 1 | |
| Atherosclerosis | Edema | 1 |
| Hematoma | 0.931 | |
| Infection | 0.750 | |
| Wound dehiscence | 0.222 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galazka, A.; Stawarz, K.; Bienkowska-Pluta, K.; Paszkowska, M.; Misiak-Galazka, M. Optimizing Wound Healing in Radial Forearm Donor Sites: A Comparative Study of Ulnar-Based Flap and Split-Thickness Skin Grafting. Biomedicines 2025, 13, 1131. https://doi.org/10.3390/biomedicines13051131
Galazka A, Stawarz K, Bienkowska-Pluta K, Paszkowska M, Misiak-Galazka M. Optimizing Wound Healing in Radial Forearm Donor Sites: A Comparative Study of Ulnar-Based Flap and Split-Thickness Skin Grafting. Biomedicines. 2025; 13(5):1131. https://doi.org/10.3390/biomedicines13051131
Chicago/Turabian StyleGalazka, Adam, Katarzyna Stawarz, Karolina Bienkowska-Pluta, Monika Paszkowska, and Magdalena Misiak-Galazka. 2025. "Optimizing Wound Healing in Radial Forearm Donor Sites: A Comparative Study of Ulnar-Based Flap and Split-Thickness Skin Grafting" Biomedicines 13, no. 5: 1131. https://doi.org/10.3390/biomedicines13051131
APA StyleGalazka, A., Stawarz, K., Bienkowska-Pluta, K., Paszkowska, M., & Misiak-Galazka, M. (2025). Optimizing Wound Healing in Radial Forearm Donor Sites: A Comparative Study of Ulnar-Based Flap and Split-Thickness Skin Grafting. Biomedicines, 13(5), 1131. https://doi.org/10.3390/biomedicines13051131